CHAPTER ONE
1.0 INTRODUCTION
1.1 BACKGROUND OF THE STUDY
Various health centres, for example Koforidua regional hospital, St Joseph hospital,
Adweso clinic ect, have made considerable efforts to improve access to health services.
However, public health resources have been so stretched that the quality of services has
sturdily declined over the last decade. As a result of this, the public is becoming attracted
to private providers than to public hospitals and clinics. Many reasons, such as lack of
infrastructure, hygienic nature of the facilities ect, has led to further declines in the
quality and efficiency of public sector health services. It remains a challenge to find
proper approaches that improve the quality of health service delivery. National Quality
Assurance Programmes are one way to improve standards, but strategies to implement
Quality Assurance at district and sub-district level are sometimes ill conceived or may
not exist at all. This is surprising in view of the fact that health sector reform policies
usually include quality as an explicit priority. Whilst greater decentralisation of
responsibility and resources might allow enthusiastic districts to remedy this situation,
staffs need models of good practice to boost morale and, indeed, improve their quality of
care. Over the last ten years, there has been a dramatic increase in the references to and
interest in quality assurance as it applies to health care. A World Health working group.
1

Quality Assurance discerned four sets of reasons: economic, social, political, and
professional (WHO, 1985).Demand for health care is increasing. Not only are people
living longer and requiring care over a long period and an extended old age but also
expectations are rising through education and general interest. There is therefore an
increasing emphasis on value for money and cost efficient solution. As resources become
more over used, there is a commensurate need to ensure that standard that is quality; are
upheld. So Quality Assurance is advanced as a way of ensuring that standards are
maintained and that resources are used as effectively as possible. The demand for health-
for cure or alleviation of undesirable conditions and for longer life is a social variable and
reflects the values preoccupations of the western world in the late twentieth century.
Another social pressure is the customer movement. Patients expect to be told what is
being provided foe them and to have redress if the service falls below standards. In the
US particularly, one reason for Quality Assurance is the need for medical practitioners to
ensure quality to avoid litigation. In order to achieve patient orientation and to improve
cost effectiveness, approaches are imported from business and commerce. It is suggested
that whiles Health Care may not be a business; it should be run in a business-like way. It
is important that this dive for efficiency should not be seen as just cost-cutting.
2

1.1 STATEMENT OF THE PROBLEM
Improvement of the quality of service provided in the health institutions has been the
main theme of Ministry of Health trust since 1989. At the regional level in Ghana, the
Regional Director of Health service and Deputy Director of nursing services at various
meetings thought critically and produce different views of what quality of service should
be. In the late1990 and early 1991, key aspects of various services were incorporated into
a “Quality of Health Checklist”.
In the “checklist” quality of care is evaluated by variables including:
- the sanitary state of Health facility
- the state of repair of infrastructure
- availability of essential drugs and a smooth flow of patients at Out –Patients
Department.
Since 1989, a lot has gone on such as the completion of the essential drug list, supply of
input examples gloves, linen, cotton ect, in the improvement of drug supply by the “cash
and carry system” and the creation of incentives such as best nurse award. Service
3

providers (supervision) feel that due to the number of measures in place in Health
Institutions, a change for the better has occurred, but patients are not satisfied with the
effort being made by the providers. Based on comments from the media, individuals and
analysis of Hospitals returns patient satisfaction is still observed to be low. It is possible
that there are differences of perception of quality of service between the service providers
and patients. The latter needs to be considered if Ministry of Health wants to improve its
services. Hence the need to find patients perception of quality of care to supplement the
checklist and improve service delivery.
1.2 OBJECTIVES OF THE STUDY
General Objectives
To determine factors contributing to patient’s dissatisfaction with service in Government
Health Facilities on the Koforidua Central Hospital as a basis for taking measures to
improve these services.
Specific Objectives
To identify service provider factors that influence patient’s satisfaction.
4

To identify structural and environmental factors that influence patient’s
satisfaction.
To develop a comprehensive checklist for monitoring level of quality of care to meet
patients expectation.
1.4 SIGNIFICANCE OF THE STUDY
The study is carried out for the following reasons:
Firstly, the study is the major work aimed at knowing patients views about treatment
received at Government Health Institutions in the New Juabeng Municipality and how
they feel in general concerning the whole environment of these institutions. The outcome
of the survey is going to help the medical officer together with their team to identify were
there are lapses and make sure that attention is paid to those areas.
Secondly, the survey is going to enlighten patients on what is expected of a good health
institution so they would know which health institution to visit in the district in order to
receive quality care.
Finally, all staffs of health institutions in the districts are going to perform their duties
promptly and with care because they are now aware patients would be interviewed
regularly regarding treatments they receive.
5

1.5 SCOPE OF THE STUDY
This project or research work will cover young men and women together with the elderly
ones who fall within the ages 15 years and above in the New Juabeng Municipality of
Koforidua in the eastern region of Ghana.
1.6 LIMITATION OF THE STUDY
There are some limitations and problems which must be kept in mind in interpreting the
results. These range from technical limitations to socio-cultural problems. Some
limitations of this study of user satisfaction was time constraint, financial constraint, and
also the problem of illiteracy on the part of young men and women who find it difficult to
provide the necessary information.
1.8 ORGANIZATION OF THE STUDY
The research report has been divided into five chapters and these are as follows:
Chapter One: - This presents the background of the study, statement of the problem,
objectives of the study, significance of the study, and the scope of the study.
Chapter Two: - This discusses related literature on Quality Assurance in general.
Chapter Three: - This discusses the research design, the population and sample base on
which analysis was made. It also discusses the research instrument that was used in the
6

data collection, the procedure used in the data collection process and method used for
analysing the data.
Chapter Four: - This comprises of hypothesis, limitations, findings and analysis of data
obtained.
Chapter Five: - This covers conclusion and underlying recommendations for the project.
7

CHAPTER TWO
2.0.0 LITERATURE REVIEW
2.1.0 INTRODUCTION
Studies of practitioner-patient relationships have demonstrated the importance of
understanding the patient’s point of view. Emphasis should therefore be put on
customer’s opinion in the assessment to extend that they are into account in policy
formulation. This is an indirect form of customer participation, a much desired ingredient
in the primary health care strategy. It has been realised that satisfaction with care is an
important influence determining whether a person seeks medical advice, compiles with
treatment and maintains a continuing relationship with the practitioner.
A study conducted by Castowny T. R et al reveal that:
A causal relationship between patient satisfaction and the use of health service
exit.
It is bi-directional and reciprocal in nature.
It is highly related to the provider from which patients seek care.
In some providers, achievement of satisfaction has been positive whiles others have been
negative. Currently, there is little information available to indicate the extent to which
patients are satisfied with the quality of care they receive. Available information indicates
8

that patient satisfaction is influenced by provider- patient interaction, service
characteristics and patient characteristics. Provider- patient interaction is the key
determinant of patient satisfaction. In a summary of the major studies, Inus and Cater
concluded that patient satisfaction is maximized when the physician with the patient
expectation and concerns, communicates with warmth and interest and when the
physician provide information to the patient. Background characteristics of patients
including health status, age, gender, social class
are related to user satisfaction in different ways DiMatteo M. et al male inpatients and
older patients were satisfied with the care received.
Consumer satisfaction studies can be used for three related but distinct purposes:
As evaluation of quality of care
As indicators of which aspects of service need to be changed to improve patient
response.
Finally, satisfaction studies can function to give providers of health care some idea of
how they would have to satisfy their client’s. In order to be used in this way, studies
should be based on consumers’ actual experiences with these and be sufficiently detailed
to provide clear guides as to which areas require modifications in service delivery to
people.
Definition of Quality: The Oxford Advanced Learner’s Dictionary defines “quality” as
“how good or bad a thing is”. Thus we can refer to a good quality thing or poor quality
9

thing. This thing may be a product or service. Another definition in the same says quality
is the extent to which customers or clients fill that product or service perceives their
needs or expectations or it is basically a simple ideal standard set for a product or service;
production is organised so that these standards are met consistently. Patients would be
assured that they would receive quality care when everything is managed to ensure set
down standards are met. Standards must then be checked regularly to make sure that they
are indeed being met. If they are not, then steps must be taken to put things right and try
to that shortfalls do not occur in the future.
Avedis Donabedian defined quality as, the extent to which the care provided is expected
to achieve the most favourable balance of risks and benefits.
(Avedis Donabedian, M.D., 19802)
2.2.0 DIMENSIONS OF QUALITY
These dimensions of quality are a useful framework that helps health teams to define and
analyze their problems and to measure the extent to which they are meeting program
standards. The eight dimensions discussed in detail in this section have been developed
from the technical literature on quality, and synthesize ideas from various Quality
Assurance experts. We feel that these dimensions are relevant to LDC settings; however,
not all eight deserve equal weight in every program. Each should be considered in the
light of specific programs and should be defined according to the local context.
10

These dimensions of quality are as appropriate for clinical care as for management
services that support service delivery.
Technical Competence
Technical competence refers to the skills, capability, and actual performance of health
providers, managers, and support staff. For example, to provide technically competent
services, a Rural/Urban health worker must have the skills and knowledge (capability) to
carry out specific tasks and to do so consistently and accurately (actual performance).
Technical competence relates to how well providers execute practice guidelines and
standards in terms of dependability, accuracy, reliability, and consistency. This
dimension is relevant for both clinical and no clinical services. For health providers, it
includes clinical skills related to preventive care, diagnosis, treatment, and health
counselling. Competence in health management requires skills in supervision, training,
and problem solving. The requisite skills of support staff depend on individual job
descriptions. For instance, a technically competent receptionist must be able to respond to
information requests, while a pharmacist might be expected to possess competence in
logistics and inventory management. Technical competence can also refer to material
resources: for example, an X-ray machine must produce radiation that consistently meets
accepted standards. A lack of technical competence can range from minor deviations
from standard procedures to major errors that decrease effectiveness or jeopardize patient
safety.
11

Access to Services
Access means that health care services are unrestricted by geographic, economic, social,
cultural, organizational, or linguistic barriers. Geographic access may be measured by
modes of transportation, distance, travel time, and any other physical barriers that could
keep the client from receiving care. Economic access refers to the affordability of
products and services for clients. Social or cultural access relates to service acceptability
within the context of the clients cultural values, beliefs, and attitudes. For example,
family planning services may not be accepted if they are offered in a way that is
inconsistent with the local culture. Organizational access refers to the extent to which
services are conveniently organized for prospective clients, and encompasses issues such
as clinic hours and appointment systems, waiting time, and the mode of service delivery.
For example, the lack of evening clinics may reduce organizational access for day
labourers. Where travel is difficult, lack of home visits or Village-based services may
create an access problem. Linguistic access means that the services are available in the
local language or a dialect in which the client is fluent.
Effectiveness
The quality of health services depends on the effectiveness of service delivery norms and
clinical guidelines. Assessing the dimension of effectiveness answers the questions, does
the procedure or treatment, when correctly applied, lead to the desired results?
12

And is the recommended treatment the most technologically appropriate for the setting in
which it is norms and specifications are defined. Effectiveness issues should also be
considered at the local level, where managers decide how to carry out norms and how to
adapt them to local conditions. When selecting standards, relative risks should be
considered. For example, more frequent use of caesarean section might be warranted in a
population with many high risk pregnancies, despite the associated risks. To determine
this strategy,
effectiveness, the procedures potential harm must be compared with its potential net
benefits.
Interpersonal Relations
The dimension of interpersonal relations refers to the interaction between providers and
clients, managers and health care providers, and the health team and the community.
Good interpersonal relations establish trust and credibility through demonstrations of
respect, confidentiality, courtesy, responsiveness, and empathy. Effective listening and
communication are also important. Sound interpersonal relations contribute to effective
health counselling and to a positive rapport with patients. Inadequate interpersonal
relations can reduce the effectiveness of a technically competent health service. Patients
who are poorly treated may be less likely to heed the health care provider,
recommendations, or may avoid seeking care.
13

Efficiency
The efficiency of health services is an important dimension of quality because it affects
product and service affordability and because health care resources are usually limited.
Efficient services provide optimal rather than maximum care to the patient and
community; they provide the greatest benefit within the resources available. Efficiency
demands that necessary or appropriate care is provided. Poor care resulting from
ineffective norms or incorrect delivery should be minimized or eliminated. In this way,
quality can be improved while reducing costs. Harmful care, besides causing unnecessary
risk and patient discomfort, is often expensive and time-consuming to correct. It would
be misleading, however, to imply that quality improvements never require additional
resources. But by analyzing efficiency, health program managers may select the most
cost-effective intervention.
Continuity
Continuity means that the client receives the complete range of health services that they
need, without interruption, cessation, or unnecessary repetition of diagnosis or treatment.
Services must be offered on an ongoing basis. The client must have access to routine and
preventive care provided by a health worker who knows his or her medical history. A
client must also have access to timely referral for specialized services and to complete
follow-up care.
14

Continuity is sometimes achieved by ensuring that the client always sees the same
primary care provider; in other situations, it is achieved by keeping
accurate medical records so that a new provider knows the patients history and can build
upon and complement the diagnosis and treatment of previous providers. The absence of
continuity can compromise effectiveness, decrease efficiency, and reduce the quality of
interpersonal relations.
Safety
As a dimension of quality, safety means minimizing the risks of injury, infection, harmful
side effects, or other dangers related to service delivery. Safety involves the provider as
well as the patient. For example, safety is an important dimension of quality for blood
transfusions, especially since the advent of AIDS. Patients must be protected from
infection, and health workers who handle blood and needles must be protected by safety
procedures. Additional safety issues related to blood transfusions include maintaining
aseptic conditions and using proper techniques for transfusing blood. While safety may
seem most important when complex clinical services are provided, there are safety
concerns in the provision of basic health services as well. For example, health centre
waiting rooms can put clients at risk of infection from other patients if risk-reducing
measures are not taken. If a health worker does not provide proper instruction on the
preparation of oral rehydration solution (ORS), a mother may administer to her child
ORS containing a dangerously high concentration of salt.
15

Amenities
Amenities refer to the features of health services that do not directly relate to clinical
effectiveness but may enhance the client’s satisfaction and willingness to return to the
facility for subsequent health care needs. Amenities are also important because they may
affect the client’s expectations about and confidence in other aspects of the service or
product. Where cost recovery is a consideration, amenities may enhance the client’s
willingness to pay for services. Amenities relate to the physical appearance of facilities,
personnel, and materials; as well as to comfort, cleanliness, and privacy. Other amenities
may include features that make the wait more pleasant such as music, educational or
recreational videos, and reading materials. While some amenities -- clean, accessible
restrooms; and privacy curtains in examination rooms -- are considered luxuries in most
LDC health care settings, they are nevertheless important for attracting and retaining
clients and for ensuring continuity and coverage.
2.3.0 PERSPECTIVES ON THE MEANING OF QUALITY
The definitions and dimensions outlined above constitute a broad conceptual framework
that includes almost every aspect of the health system performance. All these dimensions
come into play as clients, health providers, and health care managers try to define quality
of care from their unique perspectives.
16

What does quality of health care mean for the Communities and clients that depend on it,
the clinicians who provide it and the managers and administrators who oversee it?
The Client
For the clients and communities served by health care facilities, quality care meets their
perceived needs, and is delivered courteously and on time. In sum, the client wants
services that effectively relieve symptoms and prevent illness. The client’s perspective is
very important because satisfied clients often are more likely to comply with treatment
and to continue to use primary health services. Thus, the dimensions of quality that relate
to client satisfaction affect the health and well-being of the community. Patients and
communities often focus on effectiveness, accessibility, interpersonal relations,
continuity, and amenities as the most important dimensions of quality. However, it is
important to note that communities do not always fully understand their
health service needs--especially for preventive services--and cannot adequately assess
technical competence. Health providers must learn about their community’s health status
and health service needs, educate the community about basic health services, and involve
it in defining how care is to be most effectively delivered. Which decisions should be
made by health professionals and which should be made by the community? Where does
the technical domain begin and end? This is a subjective and value-laden area that
requires an ongoing dialogue between health workers and the community. Answering
these questions requires a relationship of trust and two way communication between the
parties.
17

The Health Service Provider
From the provider’s perspective, quality care implies that he or she has the skills,
resources, and conditions necessary to improve the health status of the patient and the
community, according to current technical standards and available resources. The
provider’s commitment and motivation depend on the ability to carry out his or her duties
in an ideal or optimal way. Providers tend to focus on technical competence,
effectiveness, and safety. Key questions for providers may be: How many patients are
providers expected to see per hour? What laboratory services are available to them, and
how accurate, efficient, and reliable are they? What referral systems are in place when
specialty services or higher technologies are needed? Are the physical working
conditions adequate and sanitary, ensuring the privacy of patients and a professional
environment? Does the pharmacy have a reliable supply of all the needed medicines? Are
there opportunities for continuing medical education? Just as the health care system must
respond to the patient’s perspectives and demands, it must also respond to the needs and
requirements of the health care provider. In this sense, health care providers can be
thought of as the health care systems, internal clients. They need and
expect effective and efficient technical, administrative, and support services in providing
high-quality care.
18

The Health Care Manager
Quality care requires that managers are rarely involved in delivering patient care,
although the quality of patient care is central to everything they do. The varied demands
of supervision and financial and logistic management present many unexpected
challenges and crises. This can leave a manager without a clear sense of priorities or
purpose. Focusing on the
various dimensions of quality can help to set administrative priorities. Health care
managers must provide for the needs and demands of both providers and patients. Also,
they must be responsible stewards of the resources entrusted to them by the government,
private entities, and the community. Health care managers must consider the needs of
multiple clients in addressing questions about resource allocation, fee schedules, staffing
patterns, and management practices. The multidimensional concept of quality presented
here is particularly helpful to managers who tend to feel that access, effectiveness,
technical competence, and efficiency are the most important dimensions of quality.
2.4.0 THE HEALTH SECTER REFORM RESEARCH WORK PROGRAMM
2.4.1 Why is Quality Assurance important?
However, public health resources have been so stretched that the quality of services has
declined markedly over the last decade. Policy makers have realised that health services
of inferior quality do not promote equity or maximise health gain.
19

As a result of this, the public is becoming attracted more to private providers than to
public hospitals and clinics. For many reasons, such as low staff morale and reduced
income, this has led to further declines in the quality and efficiency of public sector
health services. It remains a challenge to find innovative approaches that improve the
quality of health service delivery. National Quality Assurance Programmes are one way
to improve standards, but strategies to implement Quality Assurance at district and sub-
district level are sometimes ill conceived or may not exist at all. This is surprising in view
of the fact that health sector reform policies usually include quality as an explicit priority.
Whilst greater decentralisation of responsibility and resources might allow enthusiastic
districts to remedy this situation, staffs need models of good practice to bolster morale
and, indeed, improve their quality of care. This briefing paper proposes Quality
Assurance (QA) as an approach that governments and health managers should consider in
their attempts to systematically monitor and improves service delivery. We ask:
1. What is Quality Assurance in health care?
2. What kind of QA policy is needed to ensure good quality of care?
3. Can governments introduce an "off the shelf" QA package?
4. How can a QA policy be put into practice?
20

The answers we provide are based on experiences and results from Quality Assurance
programmes in India, Ghana, Honduras, Costa Rica and Panama. No answers apply
equally to all situations; we welcome dialogue and ask readers to share their experiences
in implementing quality assurance programmes. In exchange we offer to assist those
involved in the lengthy and difficult process of improving quality in the health sector.
Broad Definition: Quality Assurance (QA) is a planned and systematic approach to
monitoring, assessing and improving the quality of health services on a continuous basis
within the existing resources. As the Quality Assurance field has evolved and developed,
various definitions of quality assurance have emerged. Dr. Donabedian broadly defines it
as .all the arrangements and activities that are meant to safeguard, maintain, and promote
the quality of care. Drs. Ruelas and Frenk, who have conducted extensive Quality
Assurance work in Mexico, define it as .a systematic process for closing the gap between
actual performance and the desirable outcomes. According to Dr. Heather Palmer, a
Quality Assurance expert in U.S. ambulatory care, it is a .process of measuring quality,
analyzing the deficiencies discovered, and taking action to improve performance
followed by measuring quality again to determine whether improvement has been
achieved. It is a systematic, cyclic activity using standards of measurement. Dr. Donald
Berwick, a U.S.-based clinician, is working to apply principles of continuous quality
improvement (CQI) to health services.
21

This approach to Quality Assurance is an integrated organizational approach for meeting
client needs and expectations involving both management and staff while improving
processes and services using quantitative techniques and analytical tools. According to
Berwick, it is a systematic managerial transformation designed to address the needs and
opportunities of all organizations as they try to cope with increasing change, complexity
and tension within their environments. All these definitions of Quality Assurance share
several characteristics. Each, for example, refers to a systematic, ongoing process that is
oriented toward improving performance and using data in the process, either implicitly or
explicitly. In essence, quality assurance is that set of activities that are carried out to set
standards and to monitor and improve performance so that the care provided is as
effective and as safe as possible. Quality assurance is not a new .magic bullet, but has
been a part of health care for the past100 years. It was introduced into modern medicine
by a British nurse, Florence Nightingale, who assessed the quality of care in military
hospitals during the Crimean War. She introduced the first standards in nursing care;
these resulted in dramatic reductions of mortality rates in hospitals. Until recently, quality
assurance was primarily used by hospitals in developed countries and relied heavily on
standards of care developed by accrediting agencies. In the 1980s, quality assurance
expanded to primary health care in the United States and Europe. Simultaneously,
internationally accepted standards of care were introduced by diarrhoea and acute
respiratory infection (ARI) case management algorithms developed by ‘WHO’.
22

After 1985, WHO and several projects such as PRICOR and CCCD began using systems
analysis and facility assessments to assess the quality of care. There has recently been a
revolution in quality assurance approaches and an explosion of interest in developing
national Quality Assurance programs for several reasons Democratization movements
have led politicians to consider more carefully the demands of citizens for better quality
cares Economic problems in all countries have limited their ability to improve quality by
Spending more. Countries have realized that improvements in quality must come by
improving the efficiency and effectiveness of current resources Managers see the need for
more cost recovery, but realize that it will be difficult to charge for services unless the
quality is improved The success of quality management approaches employed by
industry in Japan, and recently in the United States and Europe, has inspired health care
organizations to apply these same methods to their quality assurance programs. After
only five years, there are dramatic examples of the improvements in quality and
efficiency that can be achieved. Recent experience in applying quality management to
health care systems suggests that four tenets should be adhered to in an ideal quality
assurance program:
2.4.2 What kind of QA policy ensures good Quality of care?
It has become fashionable for the government health policy around the world to include
statements on the quality of their services. Such Quality Assurance statements usually
reflected a responsive to public needs. Examples of National Policy Statements;
23

Objective: To provide universal access to primary health services and to improve the
quality of services.
Strategy: Institute a process for quality assurance and develop a framework for
monitoring and regulation of services – this will about through the establishment of
standards of practice, intensive training and supervision, the use of sanctions and rewards
and strengthening of supervisory and regulatory mechanisms.
(Medium Term Health Strategy, Ghana, 1995)
The new agenda commits to delivering the highest quality health care; therefore
improving quality of health services in the search for efficiency and equity constitutes a
fundamental health policy for the next four years.
(The New Health Agenda, Honduras, 1998).
These statements seek to promote quality of care in general terms, and this recognition at
a Central level is important. But such statements are fairly nebulous, and if they merely
reflect government lip service to an ideal, they are meaningless. Quality statements that
apply to particular aspects of health service delivery are much more manageable, and
specific quality objectives are far more useful. Here are two examples:
Targets for waiting time for acute hospital services.
“80% of in-patient admissions to be within 6 months of diagnosis”
24

Targets for compliance for TB control programmes.
“90% of patient receiving TB treatment completes the full treatment”
In addition to setting specific objectives for policy statements, outline strategies for
implementation should be made clear at Central level. Detailed implementation plans
are best left to service providers at the local level.
2.4.3 Is there a ‘Universal Quality Assurance package’?
Is there a model Quality Assurance programme that will secure quality improvements in
all countries and settings? Agencies involved in the development of Quality of Care
models offer a variety of blueprints which governments of developing countries might
find attractive in providing a ‘quick fix’ solution to improve health service quality.
However, experience shows that changes in health service culture are a prerequisite for
achieving quality improvements. Ownership of the Quality Assurance programme by the
health personnel themselves is part and parcel of this culture change. This would argue
against the notion of a universal Quality Assurance package. Adopting an off-the-shelf
package might be evidence of a government’s response to public demand for better
services.
25

But improving quality of services demands a response from the service providers
themselves. This is unlikely to happen with the top-down imposition of a bolt-on system
for quality improvement. In Ghana the Quality Assurance process began with an initial
focus on patients’ perceptions of outpatient department services. The main tool used for
monitoring quality was a locally developed exit interview. Quality Assurance teams used
the information from these patient perceptions to develop low-cost interventions for
improving service quality. The next step was to extend this monitoring and improvement
of quality to primary health-care facilities. Now that Quality Assurance has become more
institutionalised in Ghana the emphasis is moving towards clinical and management
quality issues. If there is no genuine commitment from the top, Quality Assurance
initiatives can develop in a piecemeal way. Different geographical areas may develop at a
different rate, and they may use different approaches. This can fragment the drive for
quality. A more systematic approach to Quality Assurance development has been taken in
a project in Central America. Development of a Regional Quality Assurance system in
Costa Rica, Panama and Honduras involved four different stages.
2.4.4 How can a Quality Assurance Policy be put into Practice?
Implementing Quality Assurance systems is as much a 'people' issue as a 'technical' one.
Providers implementing Quality Assurance should guard against over-ambition. They
26

may wish to start by focusing on a single issue, then, as a quality culture develops in the
health service, add additional elements to the Quality Assurance programme. Districts
should be encouraged to develop their own Quality Assurance initiatives that should be
part of the annual work plan with their own budgets. Care should be taken to ensure that
these initiatives are guided by national policies with nationally agreed standards and
indicators of quality of care. Menus of practical options for Quality Assurance strategies
should be collected centrally and actively promoted to support weaker districts where
Quality Assurance development is not taking place. However, ownership by local service
providers remains the secret to success in turning policy on quality of care into practice.
Interdisciplinary Quality Assurance teams represent the best mechanism for driving the
Quality Assurance process and at least some of the team members should have
managerial responsibility to take decisions that can directly influence service quality.
However, for long-term sustainability Quality Assurance must be integrated into the
existing roles and responsibilities of all staff. Quality Assurance must be driven from
both the bottom and top of the health system if it is become an integral part of the health
delivery system. Resource people are required at national, regional and district level to
support the Quality Assurance process. External technical assistance can act as a catalyst
for getting things started, especially if there is limited country expertise.
27

The role of National level is to advocate the importance of quality improvements
strategies, and facilitate them locally by:
providing resources,
co-ordinating training
co-ordinating standards of care.
A national Quality Assurance committee would be an appropriate body to have this
responsibility. The committee could also support district development by requiring
quality of care to be included in the training curriculum of all health service workers, so
that a culture of quality is fostered in the health service community, both public and
private.
At Regional level a quality strategy group should monitor quality and provide supportive
supervision to districts. A regional training programme should reflect the national
strategy with quality indicators and standards based on regional priorities.
At District level a quality steering team should support facility-level quality
improvements. To support consistent goals for quality across the district, this quality
steering team should facilitate effective communications between primary and secondary
level facilities.
At Facility level an interdisciplinary Quality Assurance team should be responsible for
continuously monitoring, assessing and improving quality. Each facility should have
28

targets for its services in line with regional standards. Teams should be able to re-allocate
resources according to priorities and planned interventions
2.5.0 The Four Tenets of Quality Assurance
Quality Assurance is oriented toward meeting the needs and expectations of the
patient and the community.
Quality assurance focuses on systems and processes.
Quality assurance uses data to analyze service delivery processes.
Quality assurance encourages a team approach to problem solving and quality
improvement.
Quality assurance is oriented toward meeting the needs and expectations of the patient
and the community. Quality assurance requires a commitment to finding out what
patients and the community need, want, and expect from the health services. The health
team must work with communities to meet service demand and to promote acceptance of
needed preventive services. Subsequent program planning and quality improvement
efforts should be evaluated according to these needs and expectations.
29

Quality assurance also requires that health workers, Professional needs and expectations
be met.
Quality assurance focuses on systems and processes. By focusing on the analysis of
service delivery processes, activities, and tasks as well as outcomes, quality assurance
approaches allow health care providers and managers to develop an in-depth
understanding of a problem and to address its root causes.
Rather than merely treating the symptoms of a quality-related problem, quality assurance
seeks to find a cure. In the advanced stages of a Quality Assurance program, the health
centre team can go even further by analyzing processes to prevent problems before they
occur.
Quality assurance uses data to analyze service delivery processes. Simple quantitative
approaches to problem analysis and monitoring are another important aspect of quality
improvement. Data-oriented methods allow the Quality Assurance team to test its
theories about root causes; effective problem solving should be based on facts, not
assumptions.
Quality assurance encourages a team approach to problem solving and quality
improvement. Participatory approaches offer two advantages. First, the technical product
is likely to be of higher quality because each team member brings unique perspective and
insight to the quality improvement effort. Collaboration facilitates a thorough problem
analysis and makes development of a feasible solution more likely. Second, staff
members are more likely to accept and support changes that they helped to develop.
30

Thus, participation in quality improvement builds consensus and reduces resistance to
change. It is important to note that the definition of Quality Assurance can be extremely
broad and can include all program management activities. Quality Assurance can include
everything from applied research to comprehensive management assessments and
interventions. In practice, the scope of a Quality Assurance effort depends on the needs
and capacities of the health service organization.
Usually, the Quality Assurance effort will be developed as a limited activity that is
integrated into the existing management system. However if an organization desires a
comprehensive approach, a Quality Assurance initiative can be developed as a
component of a general management improvement effort or a total quality management
system. Quality Assurance comes in many guises, and may be known as Total Quality
Management, Continuous Quality Improvement, Clinical Audit or Quality Circles.
Quality of care has different meanings to different stakeholders, for example, doctors and
patients. All Quality Assurance systems should encompass three perspectives on quality:
Clinical standard
Performance management
Client satisfaction
Hence there are usually several elements within the Quality Assurance system, such as
clinical audit, quality control of laboratory services, standards setting and client
satisfaction surveys. These components do not have to be introduced simultaneously, but
can be introduced as distinct packages.
31

CHAPTER THREE
METHODOLOGY
3.0 INTRODUCTION
This chapter describes methods employed in carrying out the study. It involves
description of the study area, population of the study, source of data, research instrument
and data collection method, sampling technique and sample size, and methods of data
analysis.
3.1 DESCRIPTION OF THE RESEARCH OR STUDY AREA
The research project was made to cover the people of the New Juabeng Municipality.
The New Juabeng Municipality covers a geographical area of approximately 110km2 and
consists of 57% of the total area of the Eastern Region.
New Juabeng Municipality is made up of 46 communities which we would like to
mention a few of them and they are Adweso, Efiduase, Asokore, Okorase, Akwadum,
Jumapo, Koforidua, Oyoko, ect.
According to the1984 population Census, the total population of the New Juabeng
Municipality, then district was 124,482 and that of 2000 was 136,768 which constitute
48.5% males and 51.5% females and the population growth rate is 2%.
The reason for selecting Koforidua central hospital as the targeted area was that, almost
75%of the inhibiters in new Juaben attend the Koforidua regional hospital.
32

3.2 POPULATION OF THE STUDY
The study population was defined as:
Adult users of and adults who accompanied children to the government health institutions
in the New Juabeng Municipality(Koforidua Regional Hospital). However, from the
study
we defined adults as being between the ages 15 to 60 years and above.
3.3 RESEARCH INSTRUMENT AND DATA COLLECTION METHOD DATA
Data was collected using semi-structured questionnaires to interview the respondents.
It was under two sections:
Out-patients satisfaction
Inpatient satisfaction
The questionnaires consist of a series of structured questions and were administered in
the form of interview by the researchers and one assistant to collect the information since
the majority of the respondents were illiterate. In view of this, questions which are
simple, clear, opened ended, and closed ended were used. These questions could
translate research objectives into specific questions to be answered by the respondent.
33

3.4 SAMPLING TECHNIQUE AND SAMPLE SIZE
Data was collected using convenience sampling method, whereby exit interviews were
performed, using the most readily available people willing to participate as respondents
in the study. In all, (100) hundred sample size was used for the various satisfaction-level
categories namely Out- patient, and Inpatient
3.5 METHOD OF DATA ANALYSIS
This chapter is more technical due to the nature of the research work, as it explains the
exact nature of the statistical test that the researcher intends to conduct. It was designed to
tabulate and make qualitative and quantitative analysis from the survey data. All
information collected were from primary source and we sorted out, edited, and collated
with the aid of simple tables to enable the overall data to be determined quickly and
easily as well as drawing conclusions. Graphs and Charts were also used.
34

CHAPTER FOUR
DATA PRESENTATION, ANALYSIS AND INTERPRETATION
4.0 INTRODUCTION
This chapter deals with presentation, analysis and interpretation of the data obtained in
the course of the research, questionnaires which were administered to obtain the views of
patients towards quality assurance they receive in government health facilities in the New
Juabeng Municipality in the Eastern Region of Ghana. The case study was the Eastern
regional hospital. Interviews were conducted where applicable, and a summary of the
questionnaires and the findings have been summarised below.
Table 4.1 Questionnaires administered and responds obtained
Number of questionnaire administered
Number returned
percentage(%)
Total 100 100 100
As indicated in table 4.1 above, out of hundred (100) questionnaires which were
administered, the number that returned were 100, representing 100% of the total number
of questionnaires administered.
35

4.2 DEMOGRAPHIC DISTRIBUTION OF RESPONDENTS
The questionnaires covered background of respondents with variables such as Gender
distribution, Age distribution, Educational level and the Occupational level.
Table 4.1.2 Gender distribution of respondents
Gender Frequency Percentage (%)
Male 62.0 62.0
Female 38.0 38.0
Total 100.0 100.0
From table 4.1.2, the analysis of data revealed that out of hundred (100) respondents
interviewed, sixty two (62) represents 62.0% were male, while thirty eight (38) represents
38.0% were female.
Table 4.1.3 Age distribution of respondents
Age Frequency Percentage (%)
18-27 37.0 37.0
28-37 38.0 38.0
38-47 15.0 15.0
48 and above 10.0 10.0
Total 100.0 100.0
Table 4.1.3 shows the Age distribution of respondents, out of the 100 questionnaires
36

administered, the largest age group who responded were 28-37 representing 38.0%,
followed by 18-27 representing 37.0%, followed by 38-47 representing 15.0% and the
least group interviewed were 48 and above with 10 respondents representing 10%.
Table 4.1.4 Educational distribution of respondents
Educational Level Frequency Percentage (%)
Basic school 17.0 17.0
Secondary school 23.0 23.0
post secondary school 27.0 27.0
Tertiary school 27.0 27.0
Others 4.0 4.0
No education 2.0 2.0
Total 100.0 100.0
Table 4.1.4 shows the educational distribution of respondents, out the 100 questionnaires
administered; groups of interviewers who responded largely were people from post-
secondary and tertiary school, which is they all responded to 27 questionnaires
representing 27.0%, followed by 23 from secondary school representing 23.0%, followed
by 17 people who had their basic formal education representing 17.0%, followed by 4
people who had education in other educational level representing 4.0% and for the No
education we had 2 people who responded representing 2.0%
37

Table 4.2.0 Occupational distribution of respondents
Occupation Frequency Percentage (%)Teachers 12.0 12.0
Students 42.0 42.0
Traders 14.0 14.0
Farmers 13.0 13.0
Business men 8.0 8.0
Dressmakers 5.0 5.0
Others 6.0 6.0
Total 100.0 100.0
From table 4.2.0, analysis of the data revealed that out of the 100 questionnaires
administered, 42 representing 42.0% were students who responded, 14 were traders who
responded representing 14.0%, followed by farmers 13 representing 13.0%, followed by
teachers 12 representing 12.0% and the least number of people who responded to the
questionnaire were dressmakers, they were 2 representing 2.0%.
38

Table 4.2.1 Category of user (respondents)
Category Frequency Percentage (%)
out patient 56.0 56.0
inpatient 44.0 44.0
Total 100.0 100.0
Table 4.2.1 shows the category of users which consist of out-patient and inpatient, out of
the 100 questionnaires administered, 56.0% who responded were out-patient and the
remaining 44.0% were inpatient.
Table 4.2.2 Satisfaction level of respondents
Satisfaction
Frequency
Percentage (%)
very satisfied 22.0 22.0
satisfied 58.0 58.0
dissatisfied 19.0 19.0
very dissatisfied 1.0 1.0
Total 100.0 100.0
Table 4.2.2 shows the satisfaction level of respondent, out of the 100 questionnaires that
were administered 58 respondents said they were satisfied with the service they received
39

representing 58.0%, 22 said they were very satisfied representing 22.0%, followed by 19
respondents who said they were dissatisfied representing 19.0% and 1 person was very
dissatisfied.
Table 4.2.3 Behaviour of staffs towards clients
Behaviour Frequency Percentage (%)
very good 16.0 16.0
good 48.0 48.0
poor 32.0 32.0
very poor 4.0 4.0
Total 100.0 100.0
Table 4.2.3 shows the behaviour of staffs towards clients, out of the 100 questionnaires
administered, 48 responded that the staffs were good to them representing 48.0%, 32
responded that the performance of the staffs was poor representing 32.0%, followed by
16 who said the staffs were very good to them representing 16.0% and 4 said their
behaviour towards them was very poor representing 4.0%.
40

Table 4.2.4 Hours spent at each service points
Hours spent at each service points
Frequency Percentage (%)
Within 30
minutes
Up to 1 hour
2 hours and
aboveRecords 9 7 3 19 19.0
waiting to
see doctor
31 13 5 49 49.0
dispensary 7 5 1 13 13.0
lab/x-ray 2 1 0 3 3.0
revenue 5 2 0 7 7.0
NHIS 3 5 1 9 9.0
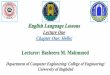
Total 57 33 10 100 100.0
Table 4.2.4 shows the hours spent at each service point, out of 100 questionnaires that
were administered, 49% responded that they spent much hours waiting to see the doctor,
from which 31 said they waited within 30 min,13 said up to 1 hour and 5 said 2 hours and
above, 19% indicated that they spend much time at the records from which 9 waited
within 30 min, 7 up to 1 hour, and 3 said 2 and above, 13% at dispensary from which 7
said they spent within 30 min, 5 up to 1 hour and 1, 2hrs and above, 9% NHIS, out of
which 3 said within 30 min, 5 up to 1hr and 1, 2hrs and above, 7% revenue, out of which
5 said within 30 min and 2 up to 1hr, and 3% from lab/X-ray, out of which 2 waited
within 30 min and 1 up to 1hr.
41

Figure 1.0 The graph below shows the service points were patients spend most of
their time.
Table 4.2.5 Cleanliness of the whole Hospital Premises/Clinic (Surroundings)
Cleanliness Frequency Percentage (%)
very clean 24.0 24.0
clean 61.0 61.0
dirty 15.0 15.0
Total100.0 100.0
Table 4.2.5 shows the cleanliness of the environment together with the health facilities,
42

out of the 100 questionnaires administered, 61 of the respondents expressed their
sentiments that it was clean which represent 64.0%, whereas 24 said it was very clean
which represent 24.0% and 15 responded that it was dirty representing 15.0%. Most of
the patients interviewed indicated that the clients of the hospital were those who made the
surrounding unclean.
Table 4.2.5 Cost of services to clients
Cos
t Frequency Percentage (%)
very expensive 6.0 6.0
expensive26.0 26.0
normal 33.0 33.0
Not expensive because of
NHIS35.0 35.0
Total 100.0 100.0
Table 4.2.5 shows the cost of service to clients, out of 100 questionnaires
administered, 35 of the respondents expressed their sentiment that it was not expensive
because of NHIS which is introduced into the system representing 35.0%, whereas 33said
it was normal which represent 33.0%, 26 said it was expensive representing 26.0% and 6
said it was very expensive representing 6.0%.
43

Table 4.2.6 Reception at the wards
Reception Frequency Percentage (%)
very good 28.0 28.0
good 60.0 60.0
poor 11.0 11.0
very poor 1.0 1.0
Total100.0 100.0
Table 4.2.6 shows reception given to clients at the various wards, out of the 100
questionnaires that were administered, 60 respondents said reception accorded them was
good representing, 28 said it was very good representing 28.0%, 11 said reception
accorded them was poor representing 11.0%, 1 said it was very poor which represent
1.0%.
44
Table 4.2.7 Cleanliness of the various facilities

Facilities cleanliness Frequency Percentage (%)
Very clean
clean dirty
Bathroom 4 15 1 20 20.0
Toilet 4 9 5 18 18.0
Floor 8 15 5 28 28.0
Wards in general
22 8 4 34 34.0
Total 38 47 15 100 100.0
Table 4.2.7 shows the cleanliness of the wards. About 4 expressed their sentiments that
bathrooms were very clean whereas said it was clean and 1 think it was dirty representing
20%. Also 4 of the respondents who have used the toilet facility said very clean, 9 said it
was clean and 5 said it was dirty representing 18%. 8 said the floor was very clean, 15
said it was clean, 5 said it was dirty representing 28%. Also, majority of the respondents
attested to the fact that wards in general was clean representing 34%, out of which 22
said it was very clean, 8 said it was clean and 4 said it was dirty. Most of the patients
interviewed indicated that clients of the hospital were those who made the place unclean.
45
Figure 2.0 Cleanliness of the various facilities

46
Table 4.2.7 Dispensing of drugs

Drugs Frequency Percentage (%)
All 61.0 61.0
Most 37.0 37.0
Non 2.0 2.0
Total100.0 100.0
Table 4.2.7 shows that out of the 100 questionnaires that were administered, 61%
responded that they received all drugs that were prescribed to them, 37% said not all
drugs were prescribed to them, 2% said they received non.
47
Table 4.2.8 SPSS Output of Test Statistics (Chi – Square)

Satisfaction level of
respondents
Behaviour of staffs towards clients
Time spent at
each service point
Cost of services
Reception at the
various wards
Drugs received
from dispensary
Computed value of
Chi-Square
68.400 44.000 68.720 21.040 77.840 52.820
Degree of Freedom
(df) 3 3 5 3 3 2
Asymp. Sig. 0.000 0.000 0.000 0.000 0.000 0.000
Level of significant 0.05 0.05 0.05 0.05 0.05 0.05
Critical value of
Chi - Square
7.815 7.815 11.071 7.815 7.815 5.99
4.3 HYPOTHESIS OF THE STUDY
State the Null and Alternate Hypothesis
Select the level of significance
Select the test statistics
Formulate the decision rule
Make a decision
48

4.3.1 THE RELATIONSHIP BETWEEN PATIENT PERCEPTION OF QUALITY
ASSURANCE AND THE SATISFACTION LEVEL IN GOVERNMENT HEALTH
FACILITIES.
Step 1: Hypothesis
Null Hypothesis (Ho)
There is no relationship between patient perception of Quality Assurance and the
satisfaction level in Government Health facilities.
Alternative Hypothesis (H1)
There is relationship between patient perception of Quality Assurance and the
satisfaction level in Government Health facilities.
Step 2: Level of significant is α=0.05
Step 3: The Test statistic chosen is 68.400
Step 4: The decision rule is that do not reject the null hypothesis if, Computed value of
Chi-Square less than Critical value of Chi – Square.
Critical value of Chi – Square (0.05, 3) =7.815
Step 5: From the ANOVA table above, Computed value of Chi-Square =68.400
The purpose for using 0.05 significance is to test the strong evidence that (Ho) is
not true, Since Computed value of Chi-Square is greater than the Critical value of
Chi–Square (68.400>7.815), we fail to accept the Null Hypothesis (Ho) per the
decision rule.
49

We therefore conclude that the relationship between patient perception of Quality
Assurance in Government Health facilities and the satisfaction level is significant.
4.3.2 RELATIONSHIP BETWEEN PATIENT PERCEPTION OF QUALITY
ASSURANCE AND BEHAVIOR OF STAFFS TOWARDS CLIENTS IN
GOVERNMENT HEALTH FACILITIES.
Null Hypothesis (Ho)
There is no relationship between patient perception of Quality Assurance and
Behaviour of staffs towards clients in Government Health facilities.
Alternative Hypothesis (H1)
There is relationship between patient perception of Quality Assurance and the
Behaviour of staffs towards clients in Government Health facilities.
Step 3: The Test statistic chosen is 44.000
Step 4: The decision rule is that do not reject the null hypothesis if, Computed value of
Chi-Square less than Critical value of Chi – Square.
Critical value of Chi – Square (0.05, 3) =7.815
Step 5: From the ANOVA table above, Computed value of Chi-Square =44.000
Since Computed value of Chi-Square is greater than the Critical value of Chi –
Square (44.000>7.815), we fail to accept the Null Hypothesis per the decision
rule.
50

We therefore conclude that the relationship between patient perceptions of Quality
Assurance in Government Health facilities and the Behaviour of staffs towards clients is
significant.
4.3.3 THE RELATIONSHIP BETWEEN PATIENT PERCEPTION OF QUALITY
ASSURANCE AND THE TIME SPENT AT EACH SERVICE POINT IN
GOVERNMENT HEALTH FACILITIES.
Null Hypothesis (Ho)
There is no relationship between patient perception of Quality Assurance in
Government Health facilities and the Time spent at each service point.
Alternative Hypothesis (H1)
There is relationship between patient perception of Quality Assurance in
Government Health facilities and the Time spent at each service point
Step 3: The Test statistic chosen is 68.720
Step 4: The decision rule is that do not reject the null hypothesis if, Computed value of
Chi-Square is less than Critical value of Chi – Square.
Critical value of Chi – Square (0.05, 5) =11.071
Step 5: From the ANOVA table above, Computed value of Chi-Square=68.720
Since Computed value of Chi-Square is greater than the Critical value of Chi –
Square (68.720>11.071), we fail to accept the Null Hypothesis per the decision
rule.
51

We therefore conclude that the relationship between patient perceptions of Quality
Assurance in Government Health facilities and the Time spent at each service point is
significant.
4.3.4 THE RELATIONSHIP BETWEEN PATIENT PERCEPTION OF QUALITY
ASSURANCE IN GOVERNMENT HEALTH FACILITIES AND COST OF
SERVICES.
Null Hypothesis (Ho)
There is no relationship between patient perception of Quality Assurance in
Government Health facilities and Cost of services.
Alternative Hypothesis (H1)
There is relationship between patient perception of Quality Assurance in
Government Health facilities and Cost of services.
Step 3: The Test statistic chosen is 21.040
Step 4: The decision rule is that do not reject the null hypothesis if, Computed value of
Chi-Square less than Critical value of Chi – Square.
Critical value of Chi – Square (0.05, 3) =7.815
Step 5: From the ANOVA table above, Computed value of Chi-Square=21.040
Since Computed value of Chi-Square is greater than the Critical value of Chi –
Square (21.040>7.815), we fail to accept the Null Hypothesis per the decision
rule.
52

We therefore conclude that the relationship between patient perceptions of Quality
Assurance in Government Health facilities and the Cost of services is significant.
4.3.5 THE RELATIONSHIP BETWEEN PATIENT PERCEPTION OF QUALITY
ASSURANCE IN GOVERNMENT HEALTH FACILITIES AND DRUGS
RECEIVED FROM DISPENSARY.
Null Hypothesis (Ho)
There is no relationship between patient perception of Quality Assurance in
Government Health facilities and Drugs received from dispensary.
Alternative Hypothesis (H1)
There is relationship between patient perception of Quality Assurance in
Government Health facilities and Drugs received from dispensary.
Step 3: The Test statistic chosen is 52.82
Step 4: The decision rule is that do not reject the null hypothesis if, Computed value of
Chi-Square less than critical value of Chi – Square.
Critical value of Chi – Square (0.05, 2.00) =5.99
Step 5: From the ANOVA table above, Computed value of Chi-Square=52.82
Since Computed value of Chi-Square is greater than the Critical value of Chi –
Square (52.82>5.99), we fail to accept the Null Hypothesis per the decision rule.
53

We therefore conclude that the relationship between patient perceptions of Quality
Assurance in Government Health facilities and Drugs received from dispensary is
significant.
In conclusion, all the results of the test that was conducted using Chi-square is showing
that the tests are significant.
54

CHAPTER FIVE
SUMMARY, CONCLUSION AND RECOMMENDATION
5.0 SUMMARY
The main objective of this study was to find out the perceptions of patients towards the
service rendered in the Government health facilities. The services rendered include
- Dispensing of drugs to patients.
- Interaction between Doctors and Patient in the consulting room.
- Reception in the ward or level of tolerance of ward attendants to Patients
- Time spent in the hospital.
The research also looked in to consideration the cleanliness of the various infrastructural
facilities such as –bathroom and toilet
The research was conducted by using sampling procedure
5.1 FINDINGS AND CONCLUSION
From the research findings it found out that 80% of the respondents said they were
satisfied with the service that they received and 20% said that they were dissatisfied with
the service.
With the behaviour of staff towards clients, the research revealed that 64% of the
respondents said staffs were good to them and 36% responded that staffs behaviour
towards them were poor. The findings revealed that 46% spend much time waiting to see
55

the doctor than in all the service points.
With the cleanliness of the environment, 85% expressed their views that it was clean,
whereas the remaining 15% said it was unclean. Most of the patients interviewed
indicated that the clients of the hospital were those who made the surroundings unclean.
Further more, the findings revealed that 35% responded that cost of service to them, was
not expensive because of the NHIS, 33% said it was normal, whereas 32% said it was
expensive. Also for the reception at the wards, 88% expressed their views that it was
good, whereas 12% said it was poor.
5.2 RECOMMENDATION
The aim of the study was to fined out how patients satisfaction are met through the
quality of service that they receive in the health care centre. Based on the findings and
conclusions, the following were recommended.
Long waiting time: caused by inadequate staff strength, increasing number of
clients due to NHIS, delay in starting time of service. Staff should be increase in
their various professions.
Poor staff attitude at the history table and at the NHIS desk: caused by pressure
from workload, lack of patience for clients by the staff. We would like to suggest
that, clients should be admonished to exercise restrain when they visit the
56

hospital, customer care should be organized for the staffs, staffs are encouraged to
treat clients with respect and dignity, and also NHIS staffs should be made to
understand that, they are rendering services to the hospital and are bound by its
ethics and code of conduct.
Admissions without telling the reasons to Patients: caused by staff attrition and
lack of encouragement or reminder. Staff should be reminded of the importance
of informing patients why they are admitted and also educate or orientate new
staff.
Patients not maintaining cleanliness at the various wards: caused by lack of
education and we suggest that health care advert, like posters, magazines should
be provided and also provision of bins on every corridor will help curb this
insanitary situation in the wards.
.
57

APPENDIX: GLOSSARY OF COMMON TERMS
Access: The extent to which user can reach and obtain services
Accreditation: A voluntary process by which a recognized governmental or non-
governmental body assesses and determines whether or not a health facility meets already
agreed standards.
Checklist: A list of items and conditions expected to be present.
Client: User of a product or service, clients may be internal, that is, among the providers
themselves, or external, that is, outside the providers.
Confidentiality: Protection of information from persons who are not expected to have
access to it.
Continuity of services: Ability of the client to receive the complete package of services
that he needs from service provision system over time, without interruption or cessation.
Customer: Used interchangeably with client.
Effectiveness: The ability of a process to produce the anticipated desirable effect(s).
Efficiency: Carrying out an activity or process with the least waste of time, effort and
resources.
Equity: Fairness in the distribution of services.
Evaluation: Assessment of the outcome of a set of processes in relation to set objectives.
Expectation: What is seen as being satisfactory?
Guideline: Direction on how an activity may be carried out.
Indicator: A yardstick used to measure the level of quality.
Input: The set of people and things needed to carry out an activity.
Interpersonal relations: Relationship between users and providers and among providers.
Model of Quality: The different angles from which one can define, monitor, measure
and improve quality.

Monitoring: Continuing assessment of the progress made in the implementation of a
plan or activity, with recommendations for modification of methods as appropriate.
Perception: Expression of what is experienced.
Perspective: Approach or point of view.
Privacy: The state of not being seen or head by a person not expected to do so.
Quality: The degree to which a product or service meets the expectations of an
individual or group.
Quality Assurance: A planned systematic approach for continuously monitoring,
measuring and improving quality of health services, with available resources, to meet the
expectations of both users and providers.

REFERENCES
1. Roemer, M.I., and Montoya-Aguilar, C., .Quality Assessment and Assurance in
Primary Health Care, WHO Offset Publication No., 105, World Health
Organization, Geneva, Switzerland, 1988.
2. Adogboba, Kwame; Offei, Aaron; Tweneboa, Nicholas; Acquah, Seth; Arvorke,
Getrud; Ankrah, Victor; March 2000: Towards a unified QA Strategy for Ghana:
Quality Assurance Review 98. Ministry of Health Ghana in Collaboration with
Liverpool School of Tropical Medicine
3. Donabedian, pp. 5-6.
4. Ruelas, Enrique and Frenk, Julio, .Framework for the Analysis of Quality in
Transition: The Case of Mexico,. Australian Clinical Review, 9, 1989, pp. 9-16.
5. Palmer, Heather, Ambulatory Health Care Evaluation Principles and Practice,
Chicago: American Hospital Association, 1983, p. 139.
6. Berwick, Donald, Improving Health Care Quality, Boston: Institute for Healthcare
Improvement, 1991, p. II-3.
7. De Geyndt, Willy, 1995: Managing the Quality of Health Care in Developing
Countries. World Bank Technical Paper.

8. Donabedian , Avedis, 1996: Evaluating the Quality of Medical care. Milbank
Memorial Fund Quarterly 44:166-203.
9. Nicholas, David D., Heiby, James R., and Hatzell, Theresa A., .The Quality
Assurance Project: Introducing Quality Improvement to Primary Health Care in
Less Developed Countries, Quality Assurance in Health Care, 3:3, Great Britain,
1991, pp. 147-165.
10. Doyle, Vicki; 2000 Quality Assurance Training handouts.otes
11. Field, Marilyn J., and Lohr, Kathleen N. (editors), Clinical Practice Guidelines –
Directions for a New Program, Institute of Medicine, National Academy Press,
Washington, D.C., 1990, p. 8.
12. Copies can be obtained by writing to Centre for Human Services, 7200 Wisconsin
Avenue, Suite 600, Bethesda, MD 20814, U.S.A.
13. The comparative analyses summarize the work of PRICOR II:
Burns Jaeger, Janice, Franco, Lynne Miller, and Newman, Jeanne S., .Oral
Rehydration Therapy in Diarrheal Disease Control: A Review of Experience in
Eight Countries,. September 1990.

14. Donabedian, Avedis, Explorations in Quality Assessment and Monitoring, Ann
Arbor, MI: Health Administration Press, 1980, pp. 5-6.
15. Acquah, S.D., 2002: Quality Assurance Training Handouts.
16. Amstrong, M.; 1997: Human Resources Management. Strategy and Action. Kogan
Page
17. Baah-Odoom, Dinah, 2002: Quality Assurance Training handouts
18. Brown, Lori Di Prete: Franco, Lynne M.; Rafeh, Nadwa; Hatzell, Theresa: Quality
Assurance of Health Care in Developing Countries. Bethesda, USA (USAID).

QUESTIONNAIRE ON PATIENTS PERCEPTON OF QUALITY ASSURANCE
IN GOVERNMENT HEALTH FACILITIES
A CASE STUDY IN THE KOFORIDUA REGIONAL HOSPITAL
INTRODUCTION
Please there are observed, opened ended and subjective questions. Tick [√] where
boxes are provided and give reasons where there are necessary.
QUESTIONNAIRE FOR BOTH OUT-PATIENT AND INPATIENT
1.0 BACKGROUND VARIABLES
1. Gender ……….. a) Male [ ] b) Female [ ]
2. Age …………... a) 15-24 [ ] b) 25-34 [ ] c) 35-44 [ ] 45 and above [ ]
3. Educational level:
a) Basic school [ ] b) Secondary school [ ] c) Post Secondary school [ ]
d) Tertiary education [ ] e) Others [ ] f) No education [ ]
4. Occupation ………………………………………………………………………........
5. When was the last time you used the government health facility?
a) 0-2 years [ ] b) 2-4 years [ ] c) 4-6 years [ ] d) 6 years and above [ ]

6. Category of user:
a) Out- patient [ ] b) Inpatient [ ]
7. Type of respondent:
a) Self user [ ] b) Accompanied ward [ ] c) Both [ ]
8. Which type of facility? a) Hospital [ ] b) Health centre/post [ ]
c) Maternal and child health care centre [ ]
9. Were you satisfied with the services you received?
a) Very satisfied [ ] b) Satisfied [ ] c) Dissatisfied [ ]
d) Very dissatisfied [ ]
10. Do you have any difficulty in finding your way around the facility?
a) Yes [ ] b) No [ ]
11. How was the behaviour of the staffs towards you when you last reported sick?
a) Very good [ ] b) Good [ ] c) Poor [ ] d) Very poor [ ]
d) Shorter than expected
12. Can you give details?
………………………………………………………………………………………………
………………………………………………………………………………………………
13. Do you feel comfortable discussing your complaints (sickness) with the nurse/doctor
or at the O.P.D in the presence of the other staffs? a) Yes [ ] b) No [ ]
14. Did you receive all the drugs that were prescribed to you? a) Yes [ ] b) No [ ]

15. Where was the place you spent much time? a) Records [ ]
b) Waiting to see the doctor [ ] c) Dispensary [ ] d) Laboratory/X- rays [ ]
e) Revenue [ ] f) NHIS [ ]
16. Why do you think you spent much time?
……………………………………………………………………………………………
……………………………………………………………………………………………
17. Do you have any suggestion to reduce the time spent?
………………………………………………………………………………………………
………………………………………………………………………………………………
18. What do you think of the cost the service you received?
a) Very expensive [ ] b) Expensive [ ] c) Normal
d) Cheap because of NHIS [ ]
19. How clean is the environment (surrounding)?
a) Very clean [ ] b) Clean [ ] c) Dirty [ ]
FOR INPATIENT ONLY
20. Were you told why you were to be admitted? a) Yes [ ] b) No [ ]
21. How would you describe your reception at the ward? a) Very good [ ]
b) Good [ ] c) Poor [ ] d) Very poor [ ]
22. Were you attended to prompt when you needed help? a) Yes [ ] b) No [ ]

23. What was/is the attitude of the health staffs? a) Very friendly [ ]
b) Friendly [ ] c) Rude [ ]
24. Who maintained your physical hygiene? a) Parent [ ] b) Health staff [ ]
c) Brother [ ] d) Sister [ ]
25. How would you describe the cleanliness of the following areas?
a) Very clean b) Clean c) Dirty
Bathroom
Toilet
Floor
Ward in general
26. How would you describe the following services?
a) Very satisfied b) Satisfied c) Not satisfied
Nursing care
Medicine
Laboratory service
Doctors
Health aids
Laundry service
Any comment:……………………………………………………………………………..
…………………………………………………………………………………………….

Recommended