Chest Pain: New Methods Chest Pain: New Methods Applied to an Old ProblemApplied to an Old Problem
Amad Zineldine, MD, FACCAmad Zineldine, MD, FACC
March 10, 2012March 10, 2012
Chest PainChest Pain
• 2 million hospitalizations annually with cost of 2 million hospitalizations annually with cost of more than $8 billionmore than $8 billion
• Cardiac etiology found in less than one thirdCardiac etiology found in less than one third
• 2% of patients with acute MI are unrecognized and 2% of patients with acute MI are unrecognized and discharged from the EDdischarged from the ED
Chest Pain in the Emergency Chest Pain in the Emergency DepartmentDepartment
• 5 million annual ED visits for chest pain5 million annual ED visits for chest pain
• Treatments for ACS are time sensitiveTreatments for ACS are time sensitive
• About 2-4% of acute MIs are missed in the EDAbout 2-4% of acute MIs are missed in the ED
• Number one cause of ED related malpracticeNumber one cause of ED related malpractice
• Strong bias for admissionStrong bias for admission

GoalsGoals
1.1. Rapid recognition of management of true ACSRapid recognition of management of true ACS
2.2. Recognition of other life-threatening causes of chest Recognition of other life-threatening causes of chest painpain
• Aortic dissectionAortic dissection• Pulmonary embolismPulmonary embolism• Tension pneumothoraxTension pneumothorax
3.3. Minimize cost and hospitalization in patients with Minimize cost and hospitalization in patients with chest pain of benign etiology.chest pain of benign etiology.

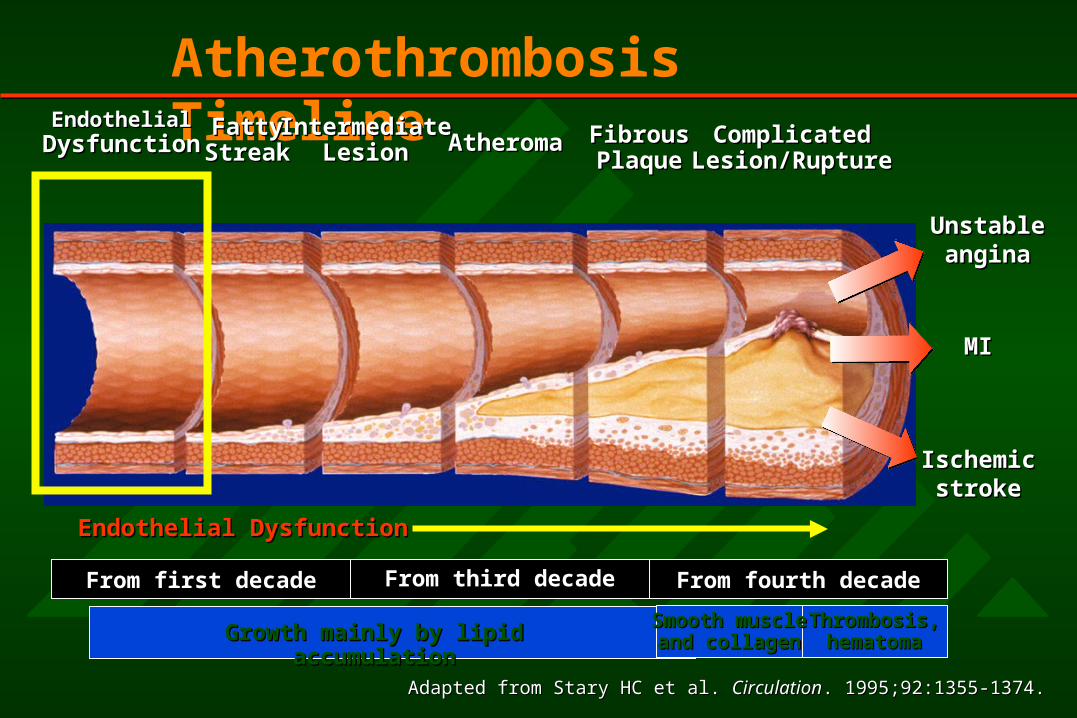
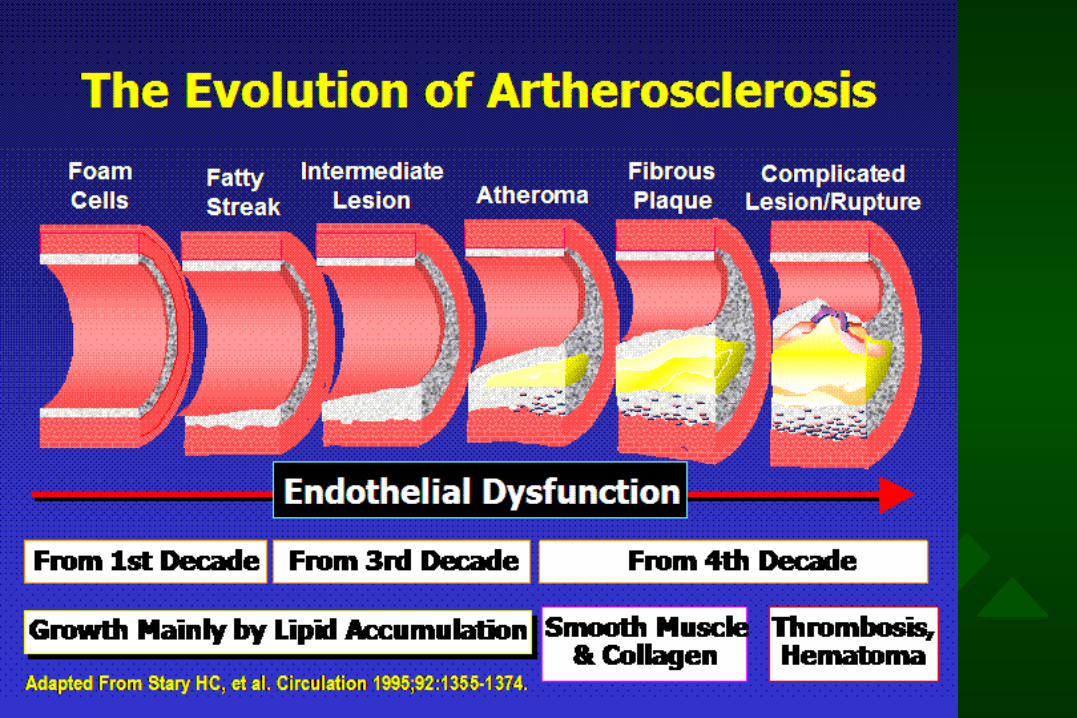
Atherothrombosis Timeline
Endothelial DysfunctionEndothelial Dysfunction
From first decade From third decade From fourth decade
Growth mainly by lipid accumulationGrowth mainly by lipid accumulation Thrombosis,Thrombosis,hematomahematoma
Adapted from Stary HC et al. Adapted from Stary HC et al. CirculationCirculation. 1995;92:1355-1374.. 1995;92:1355-1374.
EndothelialEndothelialDysfunctionDysfunction
FattyFattyStreakStreak
IntermediateIntermediateLesionLesion AtheromaAtheroma FibrousFibrous
PlaquePlaqueComplicatedComplicated
Lesion/RuptureLesion/Rupture
MIMI
IschemicIschemicstrokestroke
UnstableUnstableanginaangina
Smooth muscleSmooth muscleand collagenand collagen
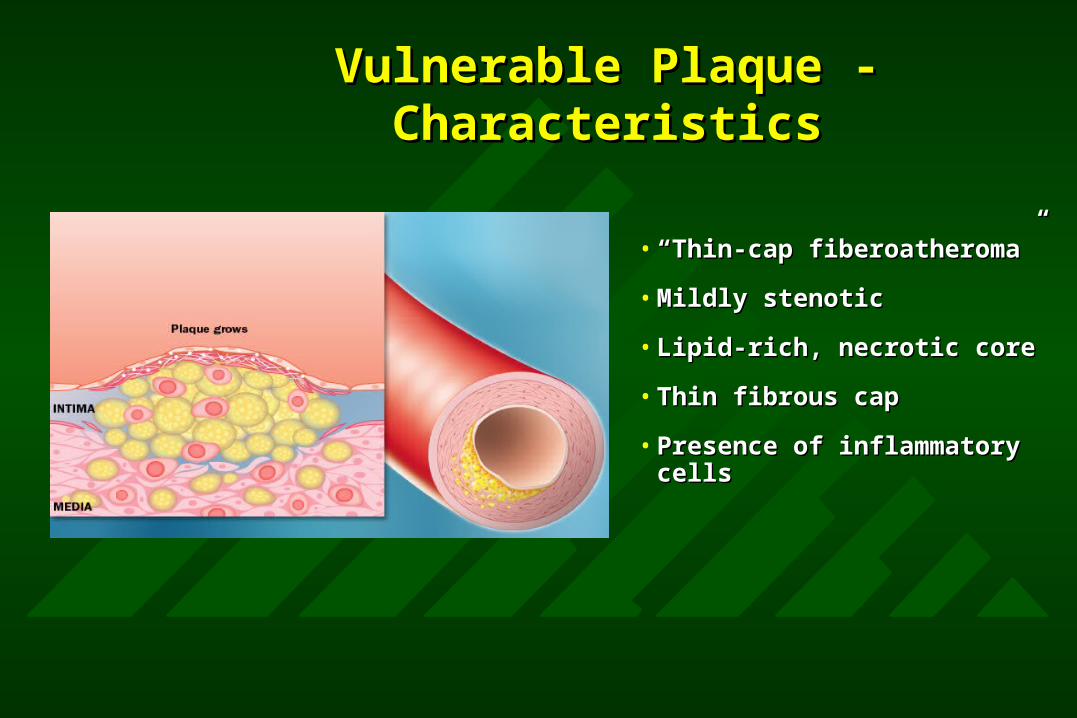
Vulnerable Plaque - Vulnerable Plaque - CharacteristicsCharacteristics
• ““Thin-cap fiberoatheroma”Thin-cap fiberoatheroma”
• Mildly stenoticMildly stenotic
• Lipid-rich, necrotic coreLipid-rich, necrotic core
• Thin fibrous capThin fibrous cap
• Presence of inflammatory Presence of inflammatory cellscells
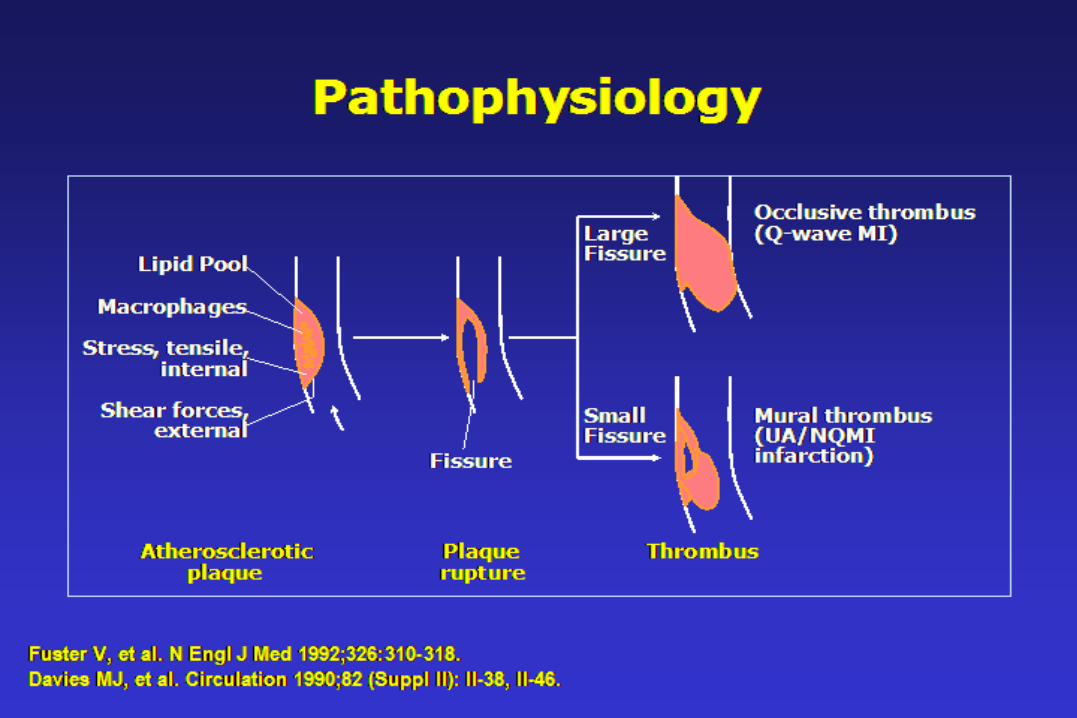

Plaque RupturePlaque Rupture

Chest Pain: Clinical Chest Pain: Clinical DiagnosisDiagnosis

Chest Pain PresentationChest Pain Presentation
Recurrent Recurrent EpisodicEpisodic
AcuteAcute PersisitentPersisitent
MultipleMultiple
EpisodesEpisodes
One One episodeepisode
One One episodeepisode
Minutes Minutes
Pain-freePain-free
Minute-Minute-HoursHours
Pain-freePain-free
Days-WeeksDays-Weeks
Pain-ongoingPain-ongoing

Recurrent Episodic Chest PainRecurrent Episodic Chest PainDifferent DiagnosisDifferent Diagnosis
• AnginaAngina• PericarditisPericarditis• Pulmonary embolism or Pulmonary embolism or
hypertensionhypertension• PleuritisPleuritis• Esophageal reflux, ulcer or spasm Esophageal reflux, ulcer or spasm
cholecystitis, pancreatitischolecystitis, pancreatitis• Cervical disk disease athritisCervical disk disease athritis• CostochondritisCostochondritis• Intercostal muscle crampsIntercostal muscle cramps• Breast diseaseBreast disease• Anxiety attacks Anxiety attacks
Cardiac Cardiac
{{Pulmonary Pulmonary
{{Gastrointestinal Gastrointestinal
{{ Musculoskeletal Musculoskeletal
{{Other Other {{
Cardio Vascular Risk FactorsCardio Vascular Risk Factors
• HypertentionHypertention
• SmokingSmoking
• ObesityObesity
• Physical InactivityPhysical Inactivity
• DyslipidemiaDyslipidemia
• Microalbuminuria or GFR <60 Microalbuminuria or GFR <60
• Age Age
• Family History of Premature CVDFamily History of Premature CVD
Cardiovascular Chest PainCardiovascular Chest Pain
• Coronary Heart DiseaseCoronary Heart Disease– Stable angina pectorisStable angina pectoris– Unstable anginaUnstable angina– Myocardial infarctionMyocardial infarction
• Coronary Vasomotor Coronary Vasomotor DiseaseDisease– Variant anginaVariant angina– Microvascular anginaMicrovascular angina
• PericarditisPericarditis
• MyocarditisMyocarditis
• Valvular Heart DiseaseValvular Heart Disease– Aortic stenosisAortic stenosis– Mitral stenosisMitral stenosis– Hypertrophic Hypertrophic
cardiomyopathycardiomyopathy
• Aortic DissectionAortic Dissection
• Post-pericardiotomyPost-pericardiotomy

Recurrent Episodic Chest PainRecurrent Episodic Chest Pain
LocationLocation QualityQuality DurationDurationAggravating & Aggravating &
Relieving FactorsRelieving FactorsAssociated Associated
Signs/SymptonsSigns/Symptons
Stable AnginaStable Angina SubsternalSubsternal Pressure Pressure SqueezingSqueezing
2-20”2-20” ↑ExerciseExercise
↓Rest/NTGRest/NTG
S4,MR,SOBS4,MR,SOB
PericarditisPericarditis Sternal or ApicalSternal or Apical Sharp Sharp stabbingstabbing
Minutes- DaysMinutes- Days ↑Breathing,supineBreathing,supine
↓Sitting upSitting up
Pericardial rubPericardial rub
Pulmonary Pulmonary EmbolismEmbolism
Substernal or over Substernal or over infarctioninfarction
Angina like or Angina like or pleurticpleurtic
Sudden onsetSudden onset<60”<60”
↑+/- Breathing+/- Breathing SOB, RR, HR, pleural SOB, RR, HR, pleural rub, hemoptysisrub, hemoptysis
PleuritisPleuritis Localized over Localized over involved areainvolved area
pleurticpleurtic Minutes- DaysMinutes- Days ↑BreathingBreathing SOB,cough, fever, SOB,cough, fever, pleural rubpleural rub
RefluxReflux Substernal Substernal epigastricepigastric
BurningBurning 10-60”10-60” ↑<60” after meal<60” after meal
↑Sitting anti acidSitting anti acid
Bitter, sour tasteBitter, sour taste
CholecystitisCholecystitis Epigastric RUQEpigastric RUQ Aching Aching colickycolicky
Minutes- HoursMinutes- Hours ↑60-90” after meal60-90” after meal Abdominal tendernessAbdominal tenderness
MussculoskelatalMussculoskelatal VariableVariable AchingAching VariableVariable ↑movementmovement h/o muscular h/o muscular exertion,injuryexertion,injury
AnxietyAnxiety Often apicalOften apical variablevariable Variable fleetingVariable fleeting situationalsituational Chest wall tendernessChest wall tenderness
• Chest Pain May Be Dangerous or BenignChest Pain May Be Dangerous or Benign– angina Vs strained muscle angina Vs strained muscle
• Severity of Pain Severity of Disease Severity of Pain Severity of Disease – angina can be mild angina can be mild – costochondritis can be severecostochondritis can be severe
• Anatomy PainAnatomy Pain– hiatus hernia refluxhiatus hernia reflux– CAD anginaCAD angina
• Two condition often coexistTwo condition often coexist– reflux esophagitis and anginareflux esophagitis and angina– anxiety and arthritisanxiety and arthritis
Chest PainChest PainScope of the ProblemScope of the Problem
Chest PainChest PainScope of the ProblemScope of the Problem
• Chest pain is commonChest pain is common
• Angina is common +/- lethalAngina is common +/- lethal
• But …But …
……Most chest pain is not anginaMost chest pain is not angina

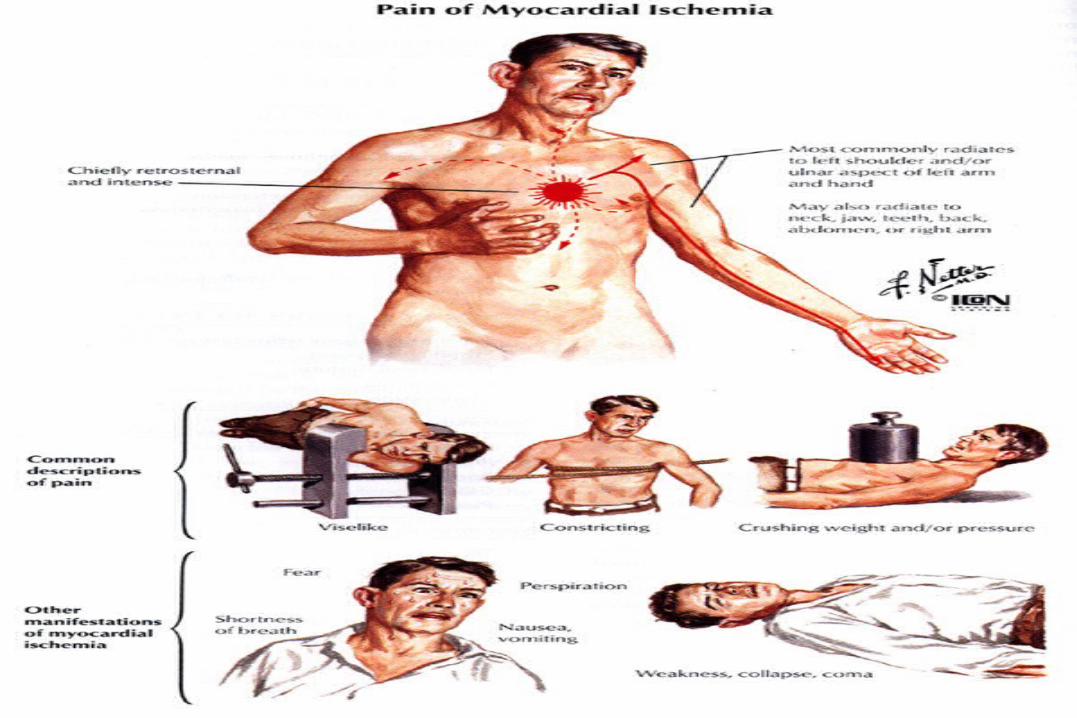
““Classic” AnginaClassic” Angina
• Location: central chestLocation: central chest
• Quality: squeezing, pressure, heavinessQuality: squeezing, pressure, heaviness
• Radiation: arm(s), neck, jawRadiation: arm(s), neck, jaw
• Associated symptoms: dyspnea, diaphoresis, nauseaAssociated symptoms: dyspnea, diaphoresis, nausea
• Eliciting factors: exertionEliciting factors: exertion
• Relieving factors: rest, nitroglycerinRelieving factors: rest, nitroglycerin
Recurrent Episodic Chest PainRecurrent Episodic Chest Pain
Typically …Typically …
Angina is not typicalAngina is not typical
Recurrent Episodic Chest PainRecurrent Episodic Chest PainProbability (Bayesian) AnalysisProbability (Bayesian) Analysis
• Chest Pain TypeChest Pain Type
• Age, GenderAge, Gender
• Risk FactorsRisk Factors– DM, lipids, HTN, family history, smokingDM, lipids, HTN, family history, smoking
• ECGECG
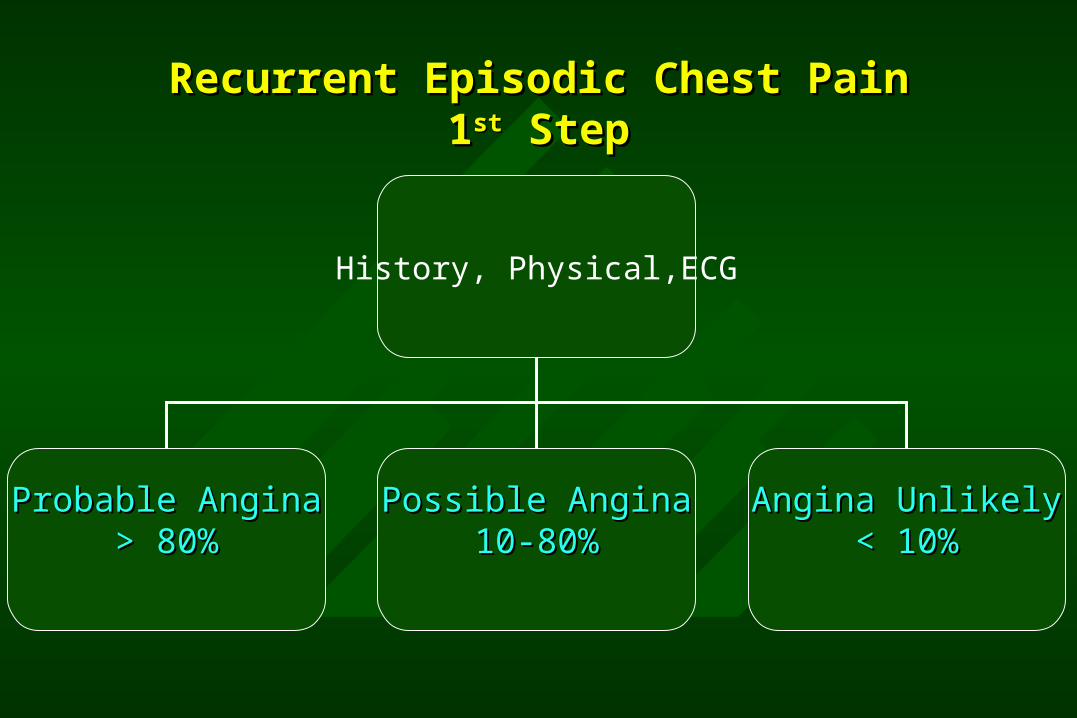
Recurrent Episodic Chest PainRecurrent Episodic Chest Pain11stst Step Step
History, Physical,ECG
Probable AnginaProbable Angina> 80%> 80%
Possible AnginaPossible Angina10-80%10-80%
Angina UnlikelyAngina Unlikely< 10%< 10%
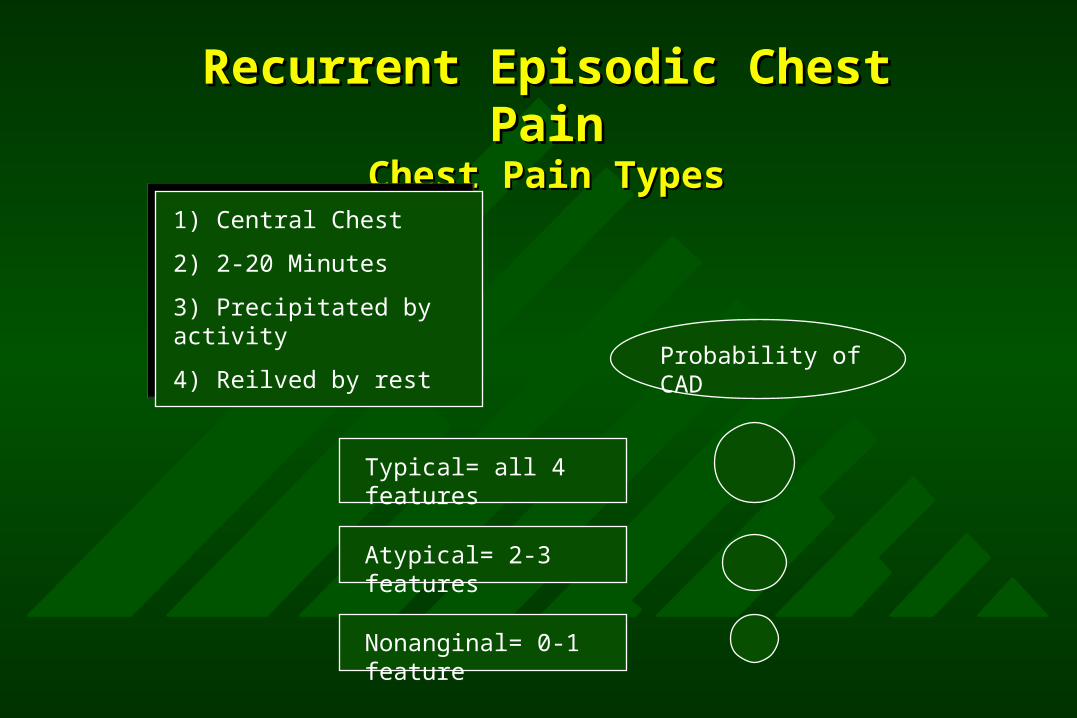
Recurrent Episodic Chest PainRecurrent Episodic Chest PainChest Pain TypesChest Pain Types
1) Central Chest
2) 2-20 Minutes
3) Precipitated by activity
4) Reilved by rest
Typical= all 4 features
Atypical= 2-3 features
Nonanginal= 0-1 feature
Probability of CAD
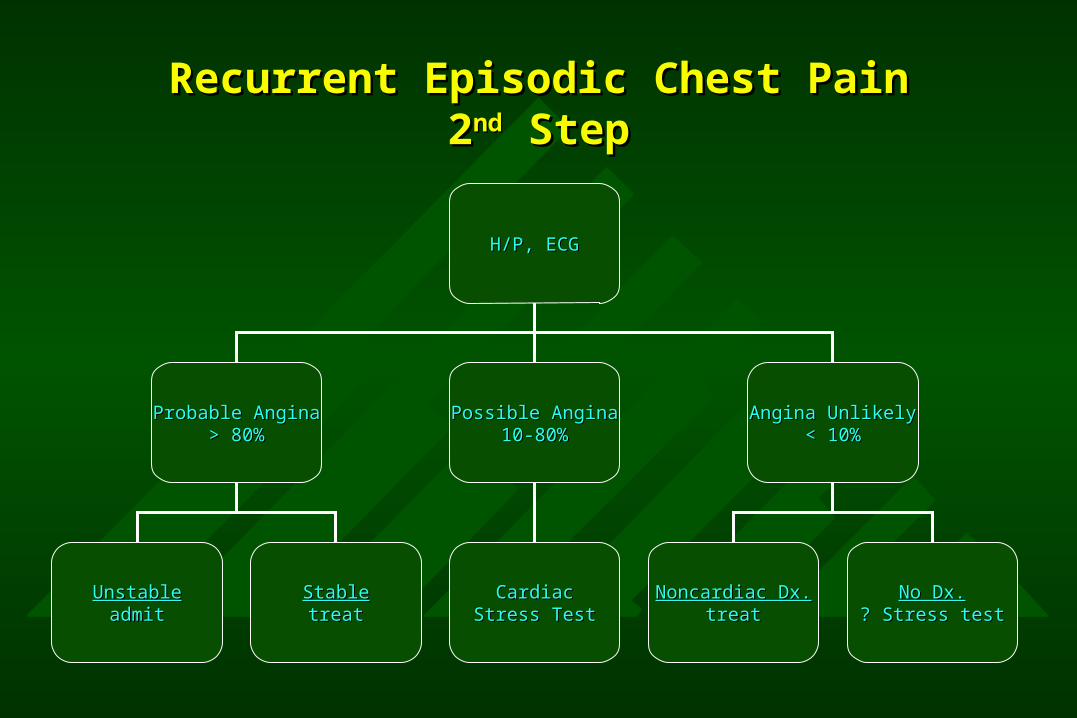
Recurrent Episodic Chest PainRecurrent Episodic Chest Pain22ndnd Step Step
H/P, ECGH/P, ECG
Probable AnginaProbable Angina> 80%> 80%
Possible AnginaPossible Angina10-80%10-80%
Angina UnlikelyAngina Unlikely< 10%< 10%
Noncardiac Dx.Noncardiac Dx.treattreat
No Dx.No Dx.? Stress test? Stress test
CardiacCardiacStress TestStress Test
UnstableUnstableadmitadmit
StableStabletreattreat
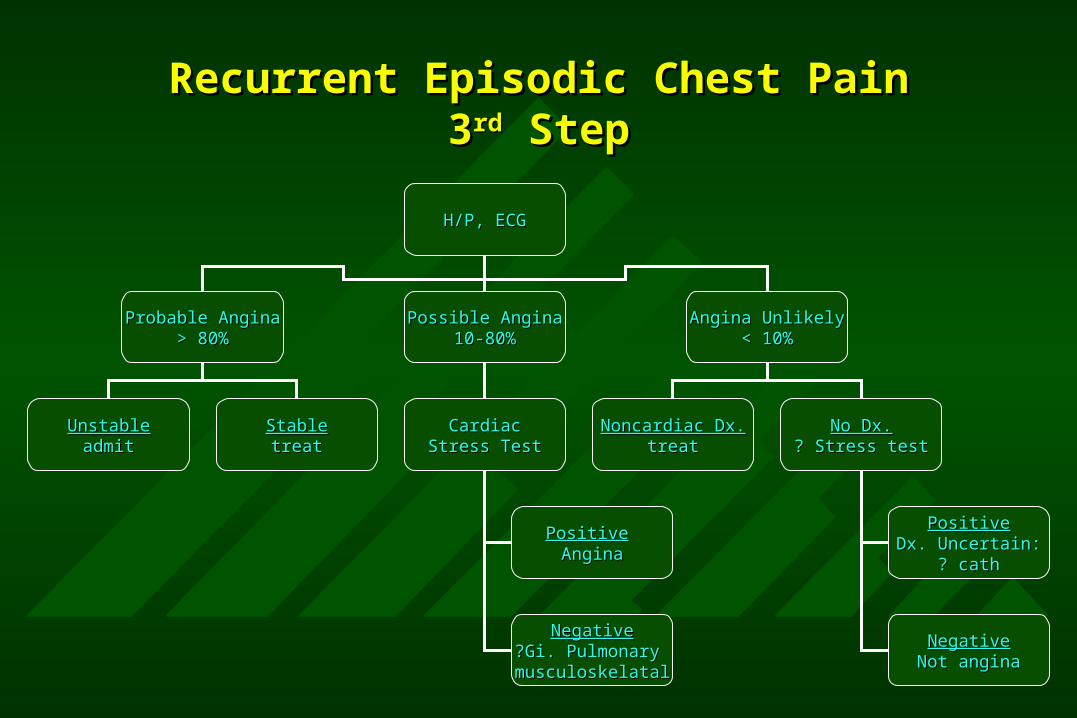
Recurrent Episodic Chest PainRecurrent Episodic Chest Pain33rdrd Step Step
H/P, ECGH/P, ECG
Probable AnginaProbable Angina> 80%> 80%
Possible AnginaPossible Angina10-80%10-80%
Angina UnlikelyAngina Unlikely< 10%< 10%
Noncardiac Dx.Noncardiac Dx.treattreat
No Dx.No Dx.? Stress test? Stress test
CardiacCardiacStress TestStress Test
UnstableUnstableadmitadmit
StableStabletreattreat
PositivePositiveDx. Uncertain:Dx. Uncertain:
? cath? cath
NegativeNegativeNot anginaNot angina
PositivePositive AnginaAngina
NegativeNegative?Gi. Pulmonary ?Gi. Pulmonary musculoskelatalmusculoskelatal
Audience QuestionAudience Question
What feature best predicts a cardiac etiology to chest What feature best predicts a cardiac etiology to chest pain?pain?
A.A. Location in chestLocation in chest
B.B. Character or quality of discomfortCharacter or quality of discomfort
C.C. Response to NitroglycerinResponse to Nitroglycerin
D.D. Relationship to exertionRelationship to exertion

Clinical Diagnosis of Chest PainClinical Diagnosis of Chest Pain
• Location, quality of pain generally not predictive of Location, quality of pain generally not predictive of cardiac causecardiac cause
• Response to nitroglycerine not a reliable predictorResponse to nitroglycerine not a reliable predictor
• While radiation and associated symptoms may be While radiation and associated symptoms may be predictive, their sensitivity and specificity are quite predictive, their sensitivity and specificity are quite lowlow
• More than a history and physical are needed!More than a history and physical are needed!

Noninvasive TestingNoninvasive Testing
StressorStressor
• ExerciseExercise
• DipyridamoleDipyridamole
• AdenosineAdenosine
• LexiscanLexiscan
• DobutamineDobutamine
Measure of IschemiaMeasure of Ischemia
• AnginaAngina
• ECG ST-segment changeECG ST-segment change
• Nuclear perfusion defectNuclear perfusion defect
• Echo wall motion abnormalityEcho wall motion abnormality
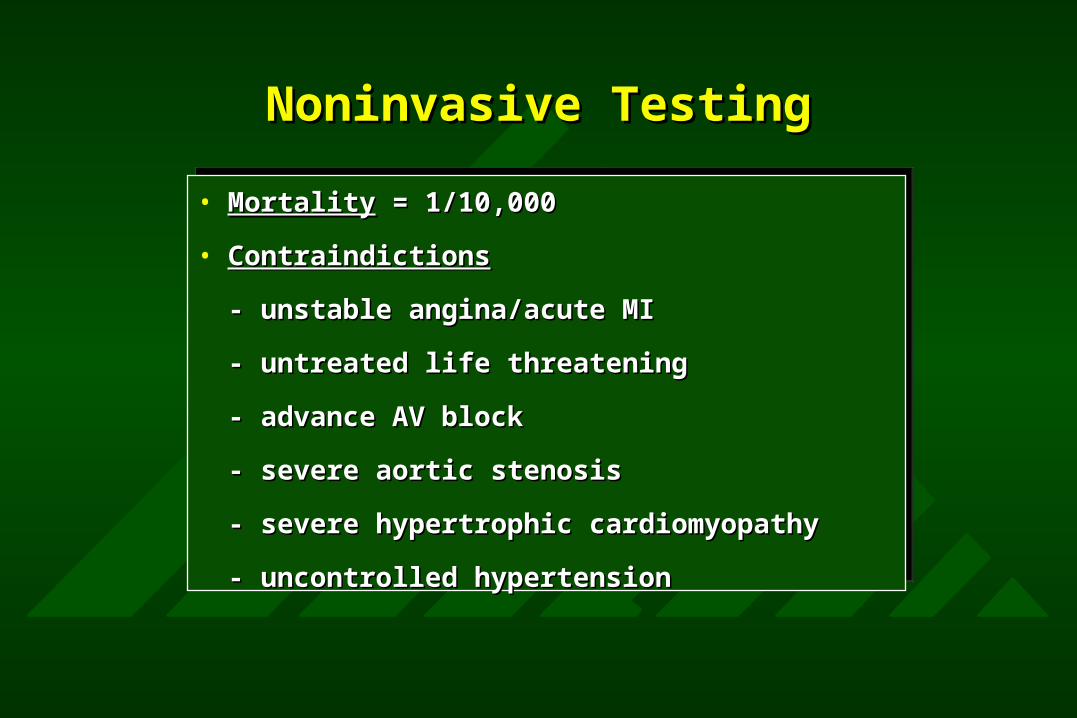
Noninvasive TestingNoninvasive Testing
• MortalityMortality = 1/10,000 = 1/10,000
• ContraindictionsContraindictions
- unstable angina/acute MI- unstable angina/acute MI
- untreated life threatening- untreated life threatening
- advance AV block- advance AV block
- severe aortic stenosis- severe aortic stenosis
- severe hypertrophic cardiomyopathy- severe hypertrophic cardiomyopathy
- uncontrolled hypertension- uncontrolled hypertension
Noninvasive TestingNoninvasive TestingExercise TerminationExercise Termination
Symptom Symptom LimitedLimited
Physician Physician LimitedLimited
DyspneaDyspnea
FatigueFatigue
DizzinessDizziness
Chest PainChest Pain
ST-changeST-change
ArrhythmiaArrhythmia
Hypotension Hypotension
Noninvasive TestingNoninvasive TestingExercise Test InterpretationExercise Test Interpretation
• ST-segment changeST-segment change
• AnginaAngina
IntesityIntesity
work-ratework-rate
HRHR
Noninvasive TestingNoninvasive TestingExercise Electrocardiography LimitationsExercise Electrocardiography Limitations
• False PositivesFalse Positives
- digoxin- digoxin
- LVH- LVH
- rest ST-depression- rest ST-depression •UninterpretablUninterpretablee
- LBBB- LBBB
- Ventrical - Ventrical PacingPacing
• False False NegativesNegatives

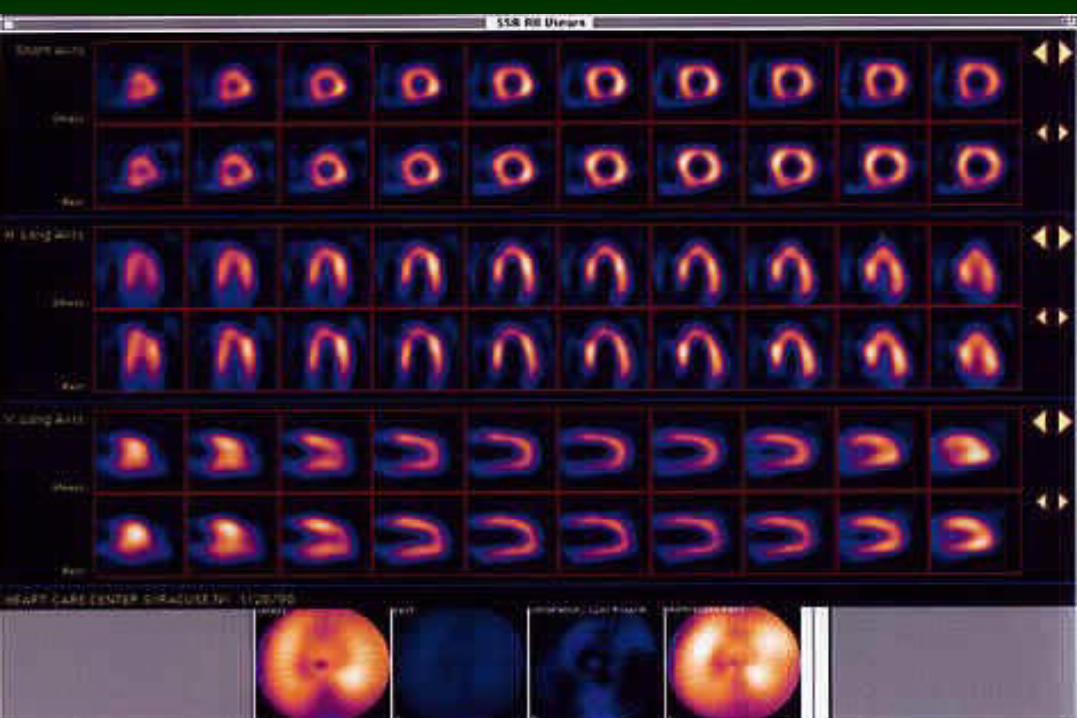
Noninvasive TestingNoninvasive TestingExercise Myocardial Perfusion ImagingExercise Myocardial Perfusion Imaging
RadionuclidesRadionuclides
ThalliumThallium
SestamibiSestamibi
Tetrofosmin Tetrofosmin
Uptake & Blood Uptake & Blood FlowFlow
Perfusion Perfusion agentsagents

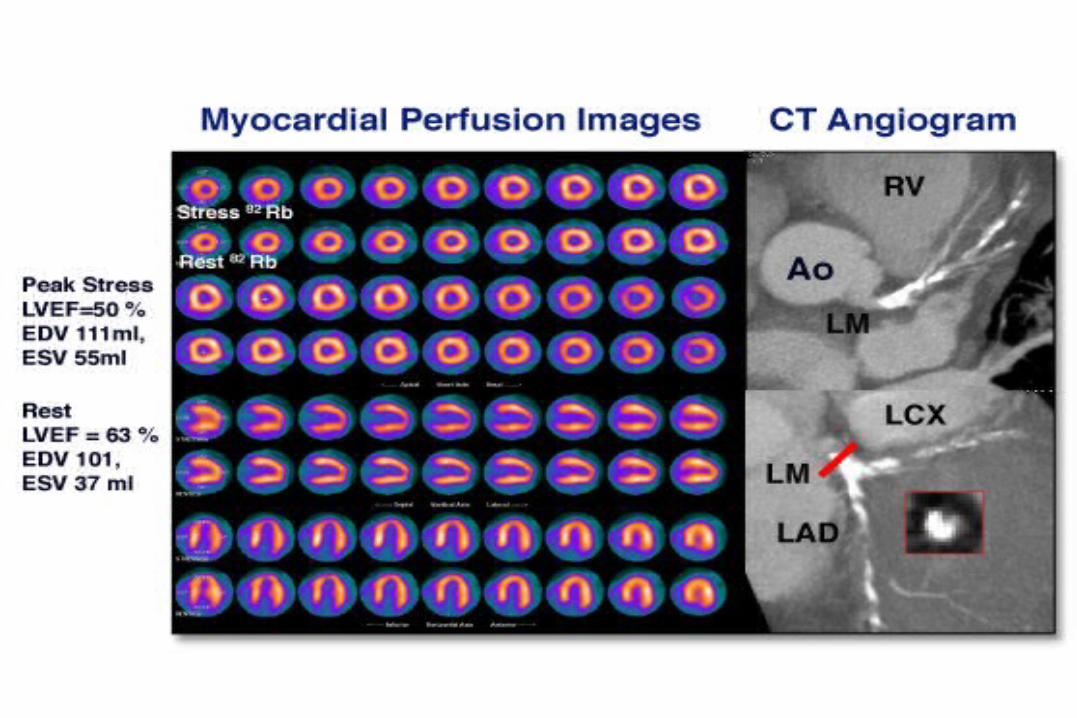
Noninvasive TestingNoninvasive TestingExercise Myocardial Perfusion ImagingExercise Myocardial Perfusion Imaging
with ECG Gatingwith ECG Gating
perfusionperfusion
Normal
Ischemia
infarct
fuction
EF
wall motion
thickening
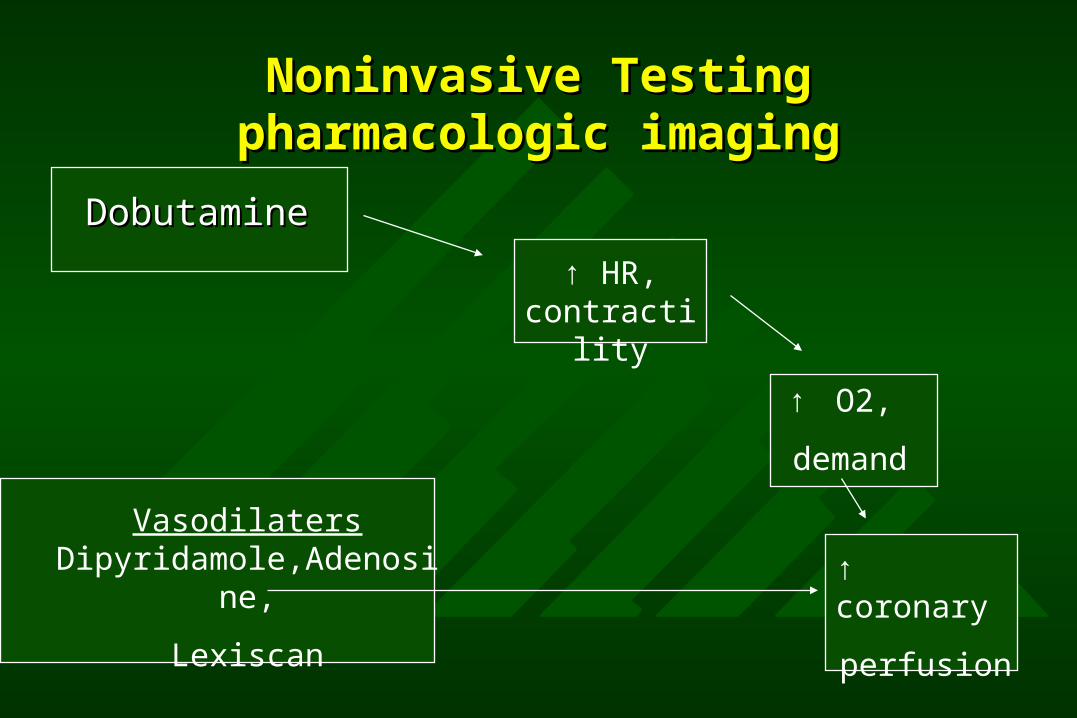
Noninvasive TestingNoninvasive Testingpharmacologic imagingpharmacologic imaging
DobutamineDobutamine
↑ HR, contractility
↑ O2,
demand
↑ coronary
perfusion
Vasodilaters Dipyridamole,Adenosine,
Lexiscan

Noninvasive TestingNoninvasive Testingpharmacologic imagingpharmacologic imaging
ContraindicationsContraindications
Bronchospasm
advanced AV block
theophylline
Arrhythmias
Severe HCM
dipyridamole/adenosine
Dobutamine Dobutamine

Noninvasive TestingNoninvasive TestingIschemic Heart DiseaseIschemic Heart Disease
What is the Probability of CAD?

Noninvasive TestingNoninvasive TestingWhat is the Probability of CAD?
Test
Patient Pre-test Probability
Sensitivity Specify
Post-test Probability
Noninvasive TestingNoninvasive TestingWhat is the Probability of CAD?
Patient Pre Test Probability of Disease
Chest Pain Type
Age, Gender
Risk Factors
Rest ECG
TIMI Risk scoreTIMI Risk score
• Age > 65Age > 65
• Greater than 3 coronary risk factorsGreater than 3 coronary risk factors
• ST-segment deviationST-segment deviation
• Greater than 2 angina events in 24 hrs.Greater than 2 angina events in 24 hrs.
• Use of ASA within 7 daysUse of ASA within 7 days
• Increase in cardiac markersIncrease in cardiac markers
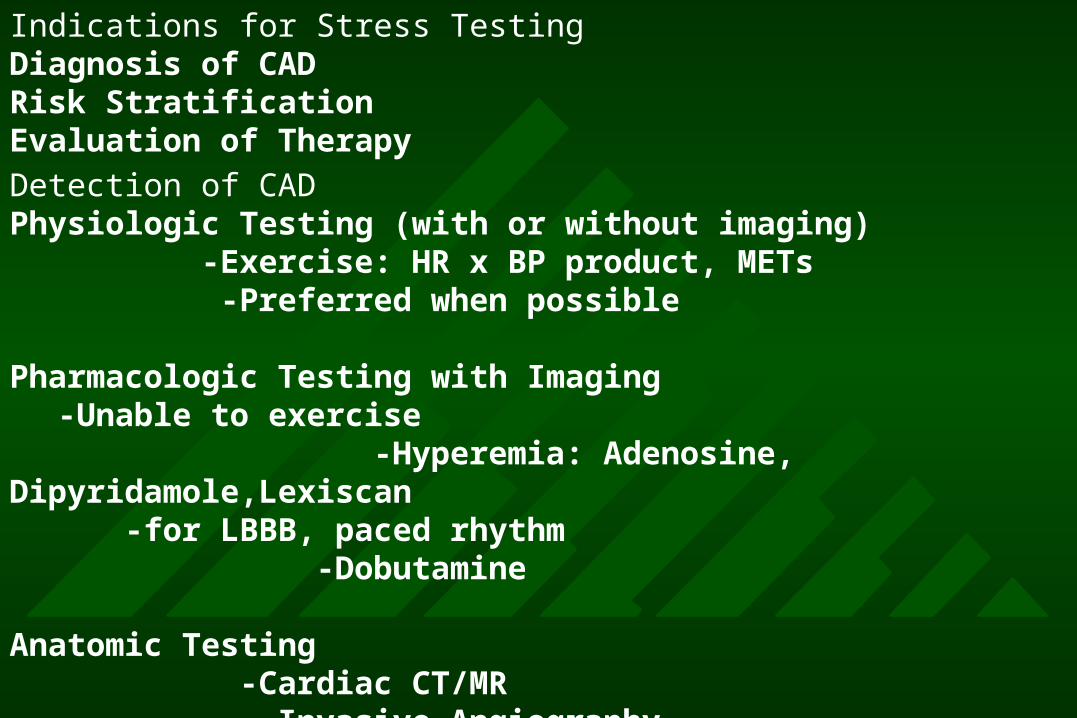
Indications for Stress TestingDiagnosis of CADRisk StratificationEvaluation of Therapy
Detection of CADPhysiologic Testing (with or without imaging) -Exercise: HR x BP product, METs -Preferred when possible
Pharmacologic Testing with Imaging-Unable to exercise
-Hyperemia: Adenosine, Dipyridamole,Lexiscan -for LBBB, paced rhythm -Dobutamine
Anatomic Testing -Cardiac CT/MR -Invasive Angiography
Exercise ECG Testing Without Imaging
Class I:
Intermediate pretest probabilityRBBB → still OK!< 1mm ST ↓ → still OK!
Class IIa
Vasospastic angina
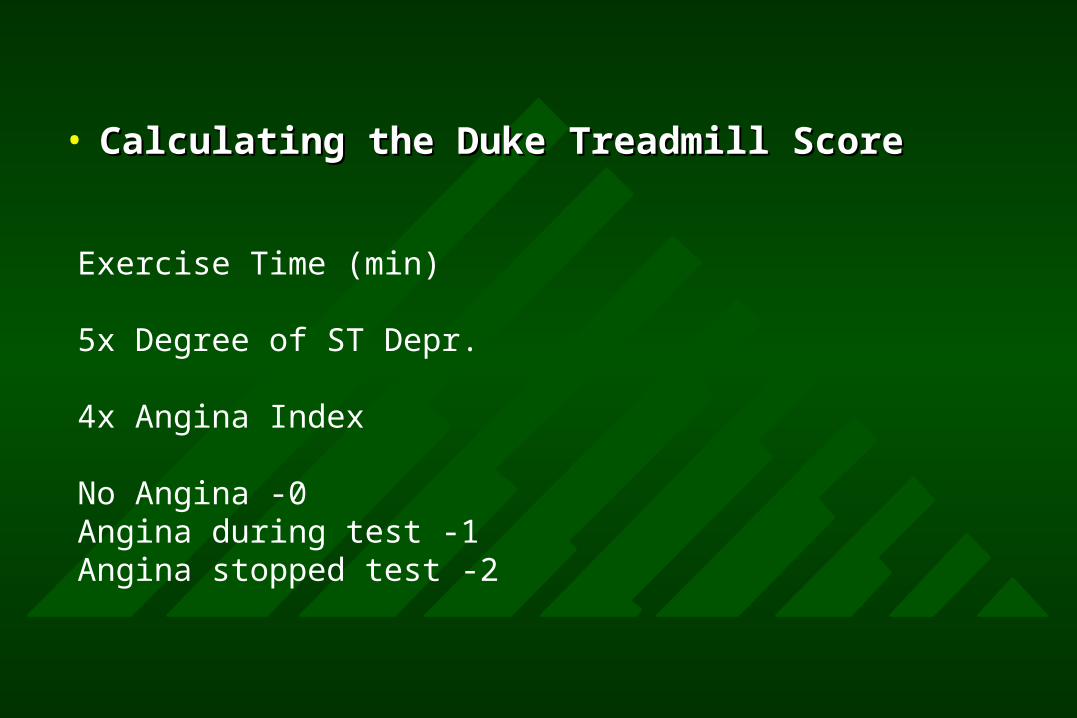
• Calculating the Duke Treadmill ScoreCalculating the Duke Treadmill Score
Exercise Time (min)
5x Degree of ST Depr.
4x Angina Index
No Angina -0Angina during test -1Angina stopped test -2

• Indications for ImagingIndications for Imaging
• Baseline ECG abnormalities LBBB, paced Baseline ECG abnormalities LBBB, paced rhythm, LVH, WPW, digoxinrhythm, LVH, WPW, digoxin
• > 1 mm resting ST depression> 1 mm resting ST depression
• Inability to exerciseInability to exercise
• Intermediate Duke Treadmill ScoreIntermediate Duke Treadmill Score
• Assessment of viabilityAssessment of viability
• Localization of ischemia for PCILocalization of ischemia for PCI
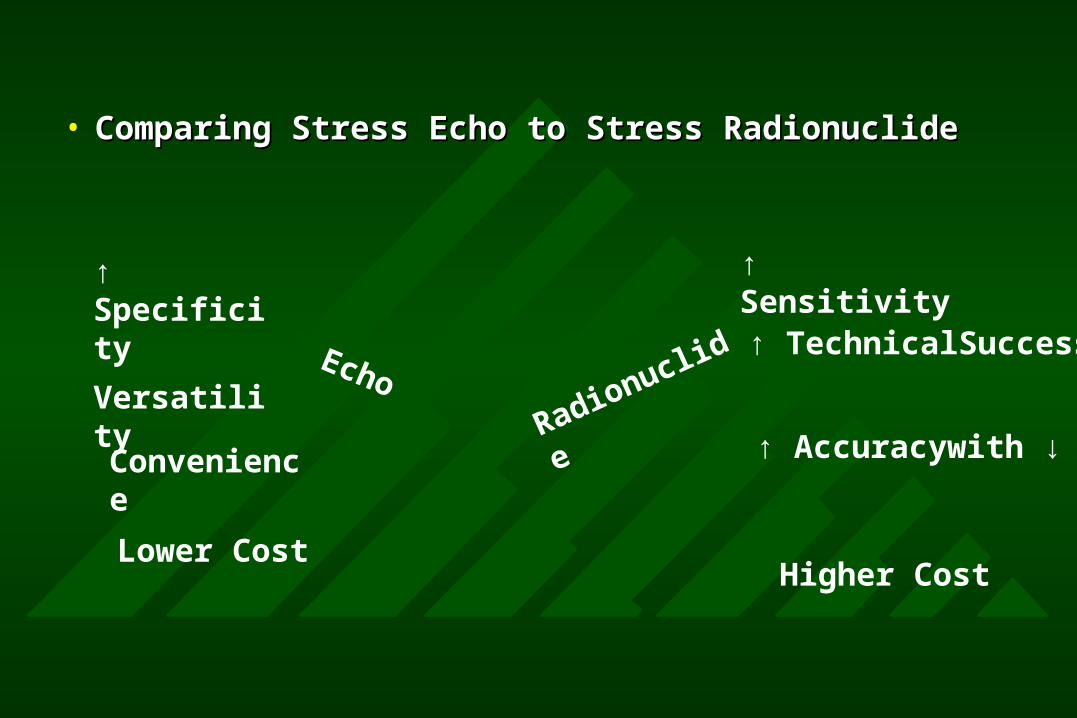
• Comparing Stress Echo to Stress Radionuclide Comparing Stress Echo to Stress Radionuclide
↑ Specificity
Versatility
Convenience
Lower Cost
↑ Sensitivity
Echo
Radionuclide ↑ TechnicalSuccess
↑ Accuracywith ↓ LV
Higher Cost
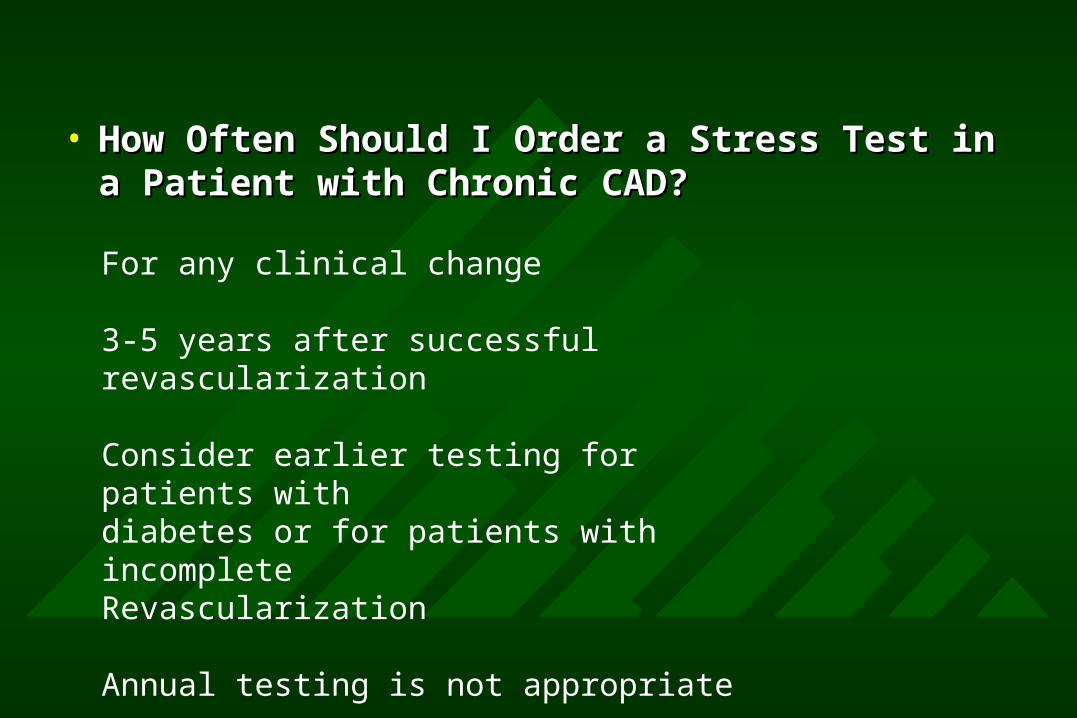
• How Often Should I Order a Stress Test in a How Often Should I Order a Stress Test in a Patient with Chronic CAD?Patient with Chronic CAD?
For any clinical change
3-5 years after successful revascularization
Consider earlier testing for patients withdiabetes or for patients with incompleteRevascularization
Annual testing is not appropriate
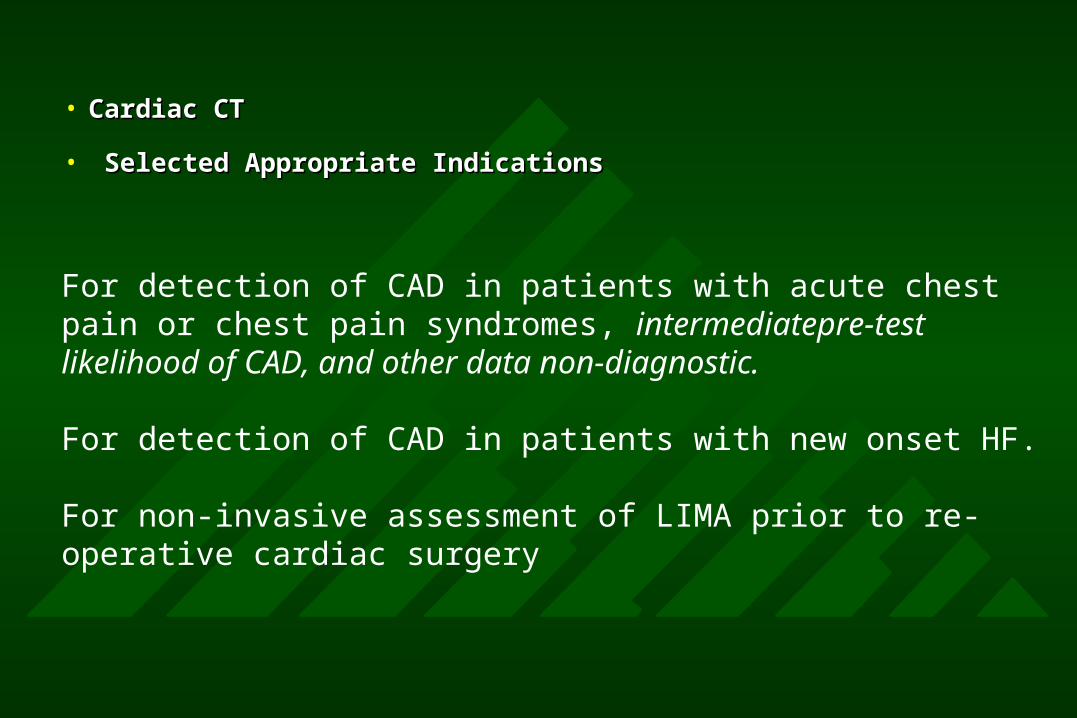
• Cardiac CTCardiac CT
• Selected Appropriate IndicationsSelected Appropriate Indications
For detection of CAD in patients with acute chest pain or chest pain syndromes, intermediatepre-test likelihood of CAD, and other data non-diagnostic.
For detection of CAD in patients with new onset HF.
For non-invasive assessment of LIMA prior to re-operative cardiac surgery
• Calcium scoring for patients with low CHD Calcium scoring for patients with low CHD risk.risk.
• CT angiography for asymptomatic low or CT angiography for asymptomatic low or intermediate CHD risk patients.intermediate CHD risk patients.
• CT angiography for intermediate peri-CT angiography for intermediate peri-operative risk patients.operative risk patients.
• Routine CT angiography after CABG.Routine CT angiography after CABG.

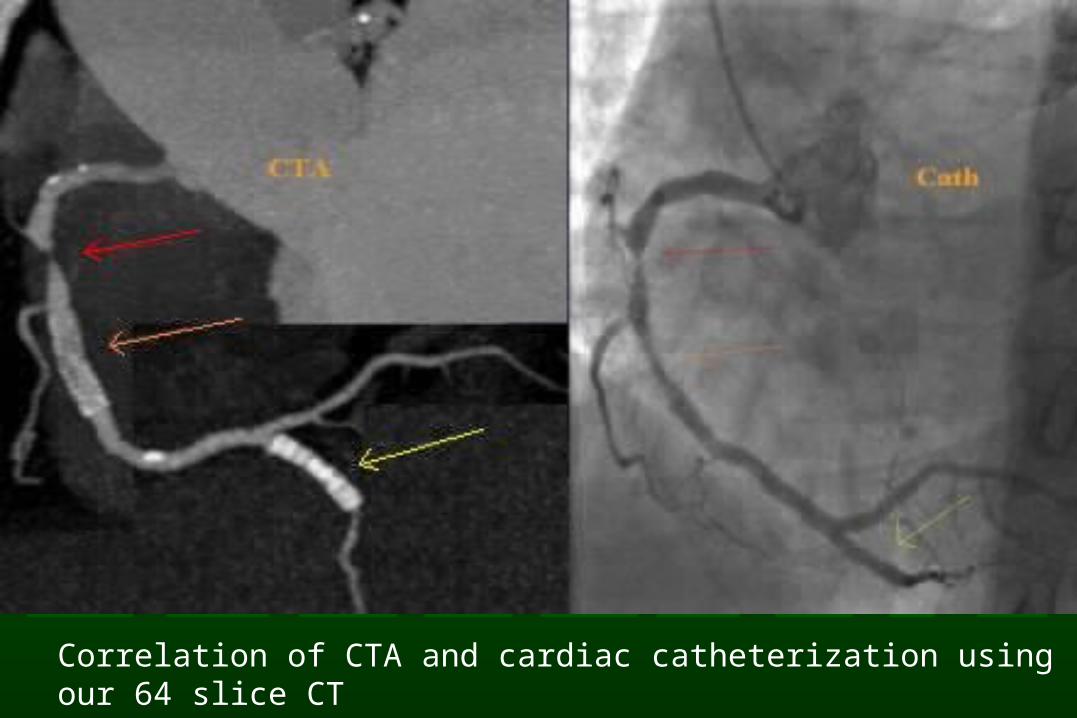
Correlation of CTA and cardiac catheterization using our 64 slice CT
ConclusionsConclusions
• Clinical characteristics are the least accurate Clinical characteristics are the least accurate predictor of the etiology of chest painpredictor of the etiology of chest pain
• Pattern of pain may be most reliablePattern of pain may be most reliable
• Accurate diagnosis and management requires use Accurate diagnosis and management requires use of clinical history, ECG, and other highly specific of clinical history, ECG, and other highly specific marker of ischemia or infarctionmarker of ischemia or infarction
• Rapid Dx &Tx = saved muscle = improved outcomeRapid Dx &Tx = saved muscle = improved outcome
Recommended

















