Cholera and other Vibrio Infections
Sung Chul Hwang, M.D.
Dept. of Pulmonary and Critical Care Medicine
Ajou University School of Medicine
Vibrios
• Coma shaped gram negative rods with flagella
• The most common organism in the surface water in the world
• Halophilic organism• Grows well in alkaline media• Main pathogens are cholerae , parahemoly
ticus, vulnificus
Cholera• Acute diarrheal disease caused by enterot
oxin from V. cholerae in small intestine
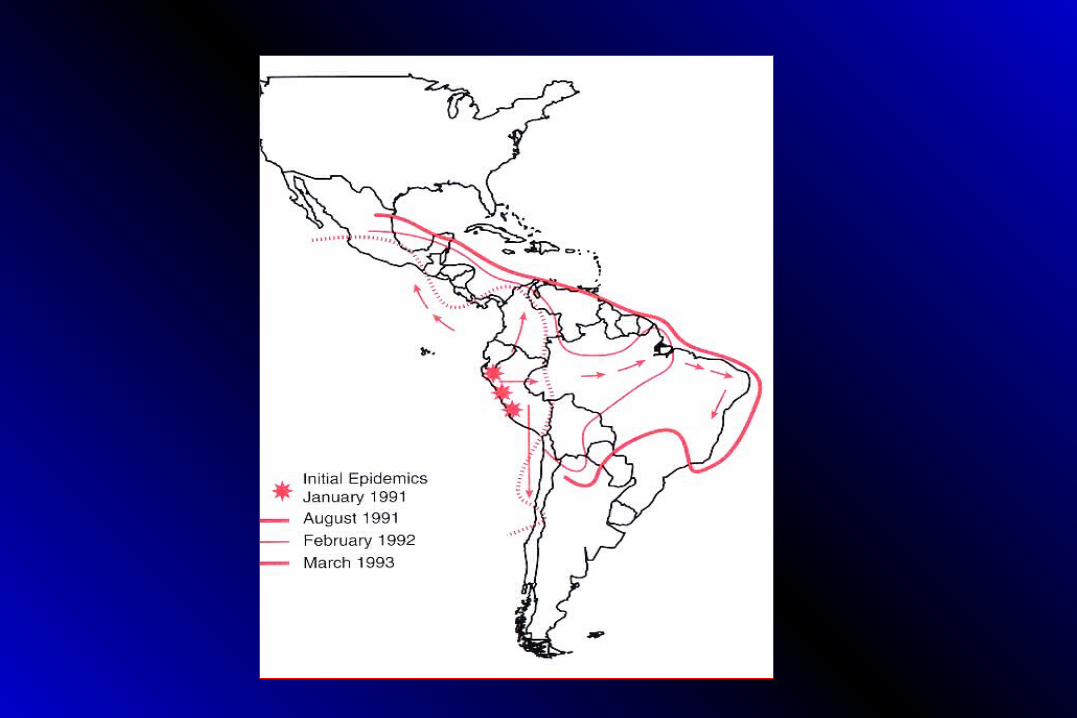
• Epidemic or endemic in occurrence : South & Central America, Africa, Southeast Asia, Middle East
• May produce massive GI fluid loss acidosis & shock
Etiology• Short , slightly curved, sausage shaped gram n
egative rod
• Rapidly motile with the use of polar flagellum
• More than 140 serotypes determined by O Ag on cell surface LPS
• Only Serotype O1 and O139 are responsible for the epidemic cholera
• Other non-O1 strains cause sporadic cases
Microbiology
• V. cholerae is divideed into two biotypes, Classical and El Tor based on on biochemical traits and susceptibility to specific phages
• Both are subdivided into ogawa( A, B), inaba(A,C), Hikojima (A,B, C)
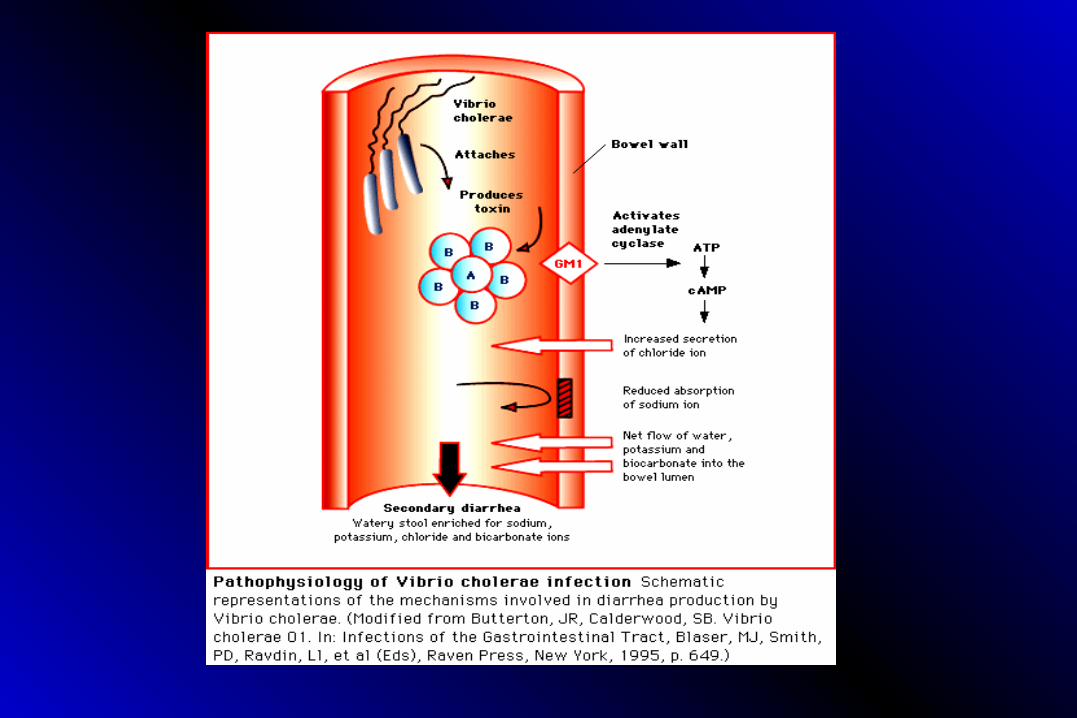
• Major virulence factor for O1 and O 139 serotype is cholera toxin, multimeric protein with one A subunit and 5 B subunits. (ADP ribosylation factor)
Pathogenesis • Ingestion of viable organisms : 10 11
• Attach to mucosa by the pili(TCP)• Production of enterotoxin(CTX):• (A1~A2) + (5 B) : ADP Ribosylation • CTX stimulates adenyl cyclase in intestin
al epithelial cells• Increase in cAMP • Secretion of isotonic fluids
Clinical Features
• Increase in peristalsis ( 1st Sx)
• Abd. Fullness
• Loose stool
• “ Rice water ” appearance
• Hypotensive within hours
• Death within 18 hours to several days
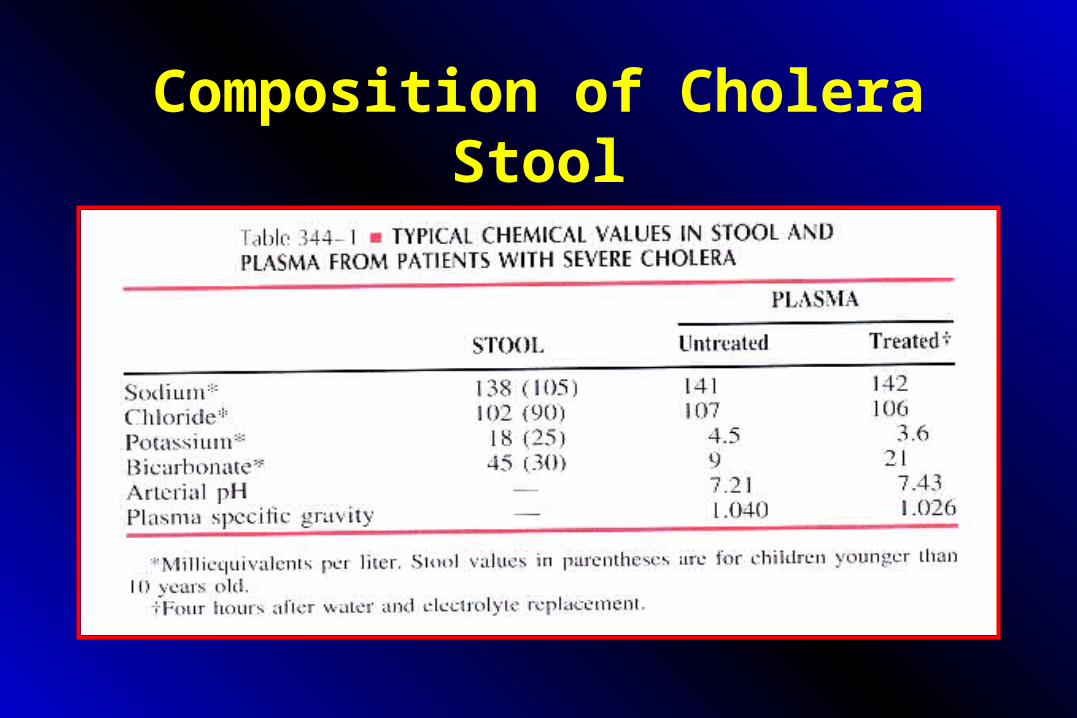
Composition of Cholera Stool
Diagnosis
• History of acute onset with watery diarrhea in the absence of fever or abdominal cramp
• Darkfield or phase contrast microscopy : most effective and rapid diagnostic test
• Cultures from stool or rectal swab (Gelatin, Meat extract, MacConkey, TCBS, Monsur)
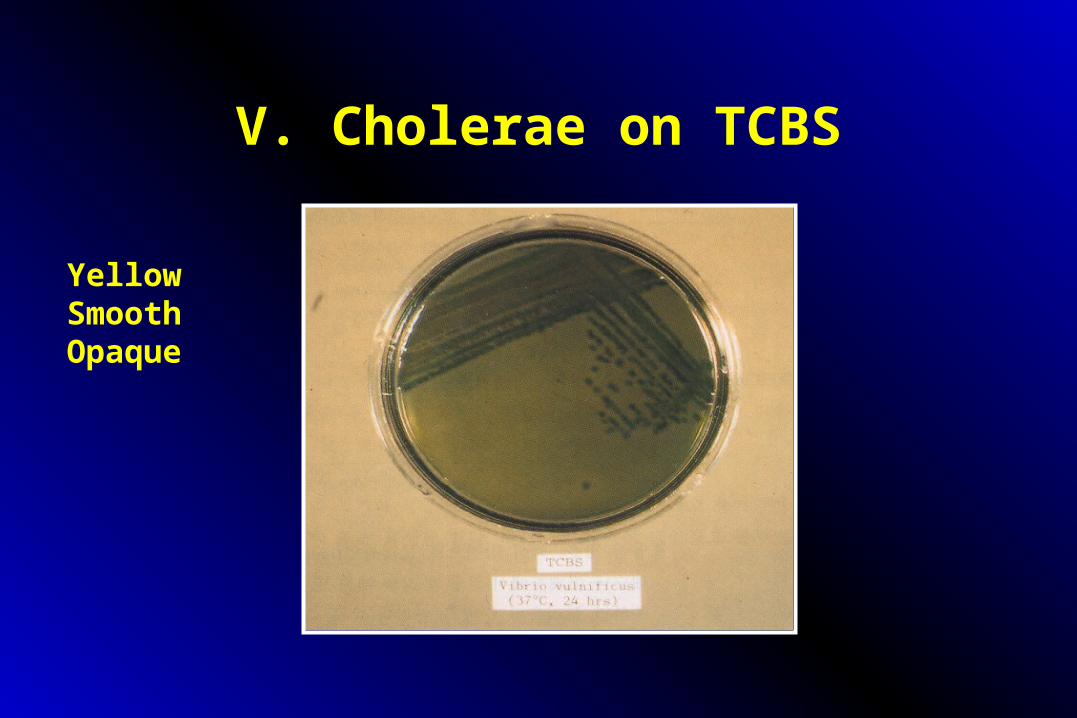
V. Cholerae on TCBS
YellowSmooth Opaque
Complications
• Altered consciousness or convulsions : especially due to hypoglycemia in children
• Electrolyte imbalance : Hypokalemia ( in children)
• Renal failure
• Aspiration in depressed consciousness and vomiting
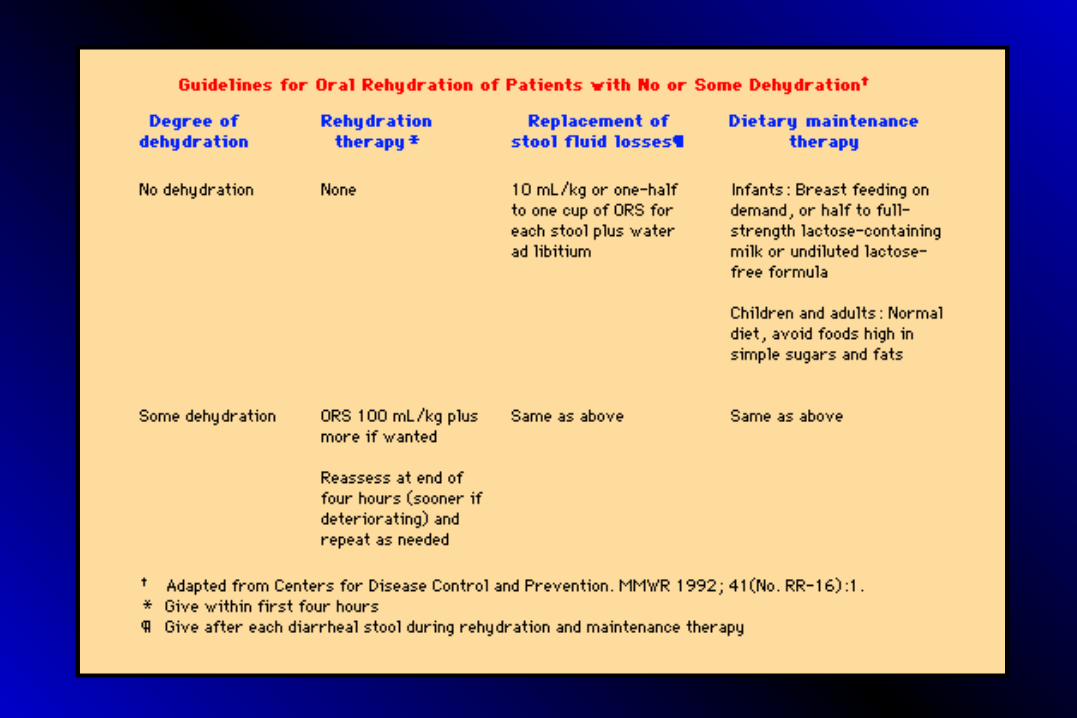
Treatment (1)
Water and salt replacement • 1) oral replacement in most cases – three finger
pinch of salts plus handful scoop of sugar, in half liter or one pint of drinking water
• 2) Intravenous replacement therapy – in severe cases, when the volume exceeds 100 l/kg/24hours or 7 L/day in 70 kg person
• Antibiotics Shortens the duration of diarrhea and reduce fluid loss
• Tetracycline : Drug of choice 250 mg q 6 hrs or others such as Ampicillin, CM, TMP/SFX, Doxycycline
Treatment (2)
Prophylaxis
• Cholera vaccines : 50% effective Primary immunization Booster immunization• Antibiotics : prevents transmission in
close contacts tetracycline or CM• Improve standard of living , public
health, and sanitation
Oral Rehydration Solution (ORS)
• 3.5 g Sodium Chloride
• 2.9 g Trisodium Citrate or 2.5 g Sodium Bicarbonate
• 1.5 g Potassium Chloride
• 20 g Glucose or 40 g Sucrose
Mortality
• 50 to 70 % in untreated patients
• Children mortality is higher ( ten times)
• Pregnant woman : 50 % chance of fetal death during third trimester
• Death may happen in 2-3 hours of illness but usually after 18hours to several days
Vibrio parahemolyticus
• Major cause of acute diarrheal disease in Japan and Korea
• Ingestion of contaminated sea food
• Production of enterotoxin and inflammation in small bowel mucosa
• Incubation : 23 hrs ( 5 to 92 hrs)
Symptoms and Signs
• Acute onset of explosive diarrhea
• Abdominal pain, low grade fever, mild chills, headache, vomiting, and electrolyte loss
• Very high attack rate
Lab Findings
• Diarrheal fluid : Watery, sometimes mucoid, less often bloody ( < 15%) with a few leukocytes 10 – 20 WBCs/HPF)
• Stool Culture : TCBS agar
• Positive Kanagawa test :- hemolysis
Clinical Course
• Self limited
• Mortality : rare
• Prevention : Adequately cooking sea food
Vibrio vulnificus
• “ vulnificus ” means “wound making”• Gram negative rod in Vibrio family• Causes serious wound infections and septi
cemia• First identified in 1970s• Common in those with liver disease or chr
onic illnesses such as DM
Microbiology• Gram negative curved rods with a polar flagellum• Grows well in Salt water : Halophilic vibrio• Epidemic when the temperature of the sea water r
ises• Exponential growth in the presence of free Iron , t
ranferrin saturation above 70%• Reason for infecting Liver cirrhosis, splenectomy,
hemochromatosis, ESRD

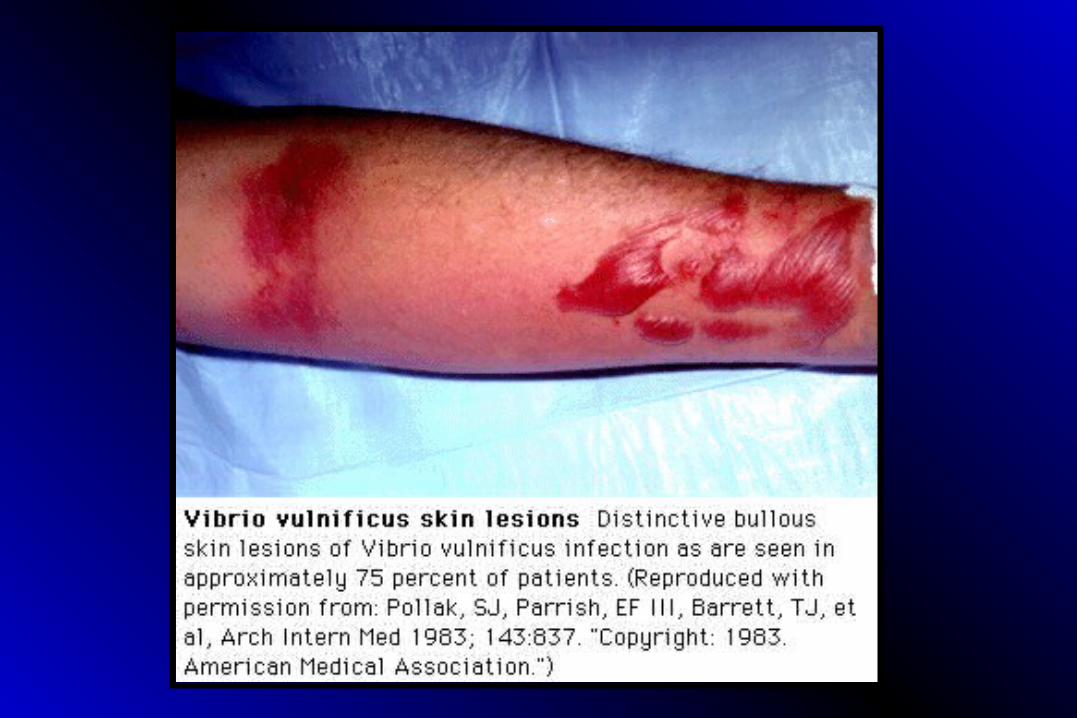
Clinical Types of V. vulnificus Infection
• Localized wound infection – cellulitis
• Acute gastroenteritis
• Septicemia with bullae and gangrene
Predisposing Conditions• Chronic Liver Diseases : Liver cirrhosis, chronic hep
atitis• Alcohol abuse• Hemochromatosis• Gastrectomy• Splenectomy• Immune suppressive therapy• DM, RA, Leukemia, Lymphoma• TBC, ESRD
Contaminated foods
• 조개• 홍합• 맛살• 산낙지• 생굴
Clinical Features in Septicemia
• Incubation Period : 3 – 14 days• Invasion to blood stream through gut mucosa
abrupt onset of fever, chills, hypotension metastatic cutaneous lesion Bacteremia DIC Shock
• GI bleeding• High mortality rate
Clinical Features in Healthy
Wound Infections Open wound contaminations Intense c
ellulitis necrotizing vasculitis ulcer formation occasional bacteremia
Treatment
• Antibiotics : Tetracycline or ciprofloxacin
• Supportive care for the Sepsis
• Early Surgical debridement and wide excision with skin graft
• Prevention : avoid eating raw fish
Non-O1 V. cholerae
• Diarrheal illness from severe watery diarrhea to milder traveller’s diarrhea
• May produce enterotoxin• Small numbers of leukocytes and RBCs in
stool• Stool culture on TCBS agar• Usually no treatment required
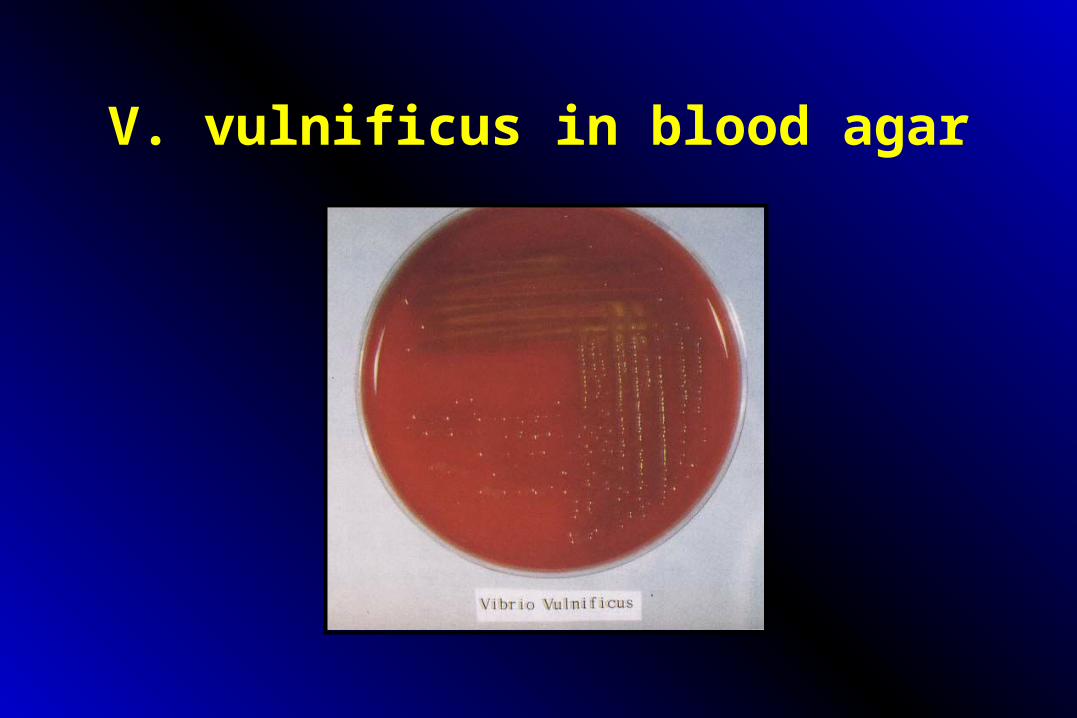
V. vulnificus in blood agar
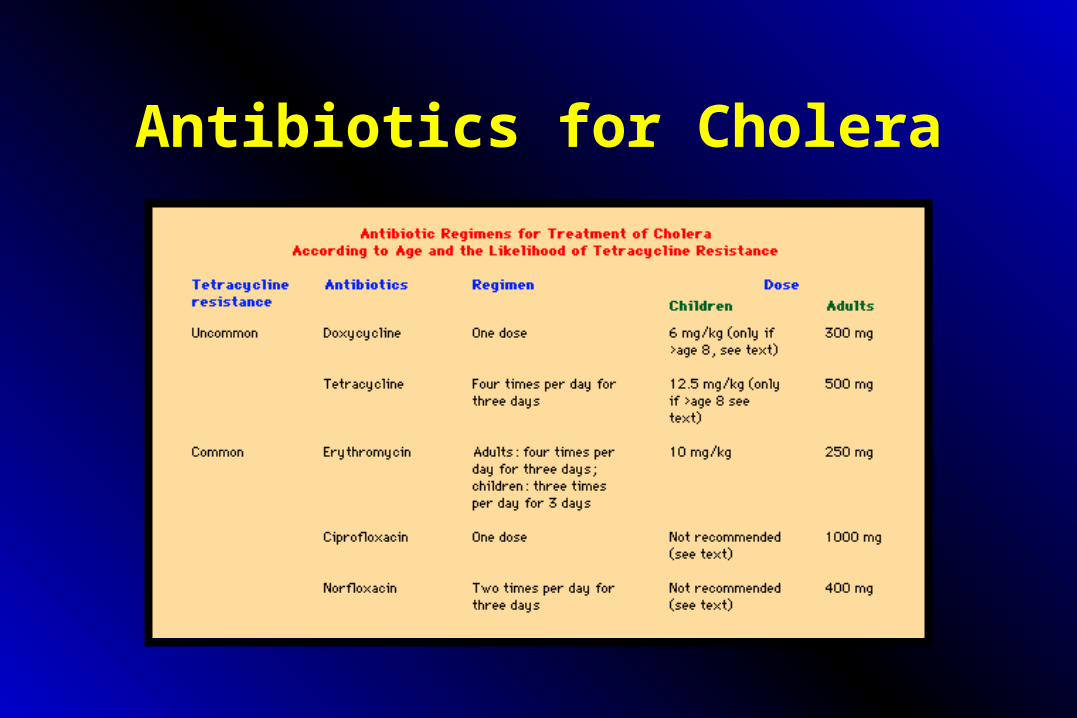
Antibiotics for Cholera

Hemorrhagic Bullae

Necrotic Bullae & Gangrene

Pathology of the Bullae
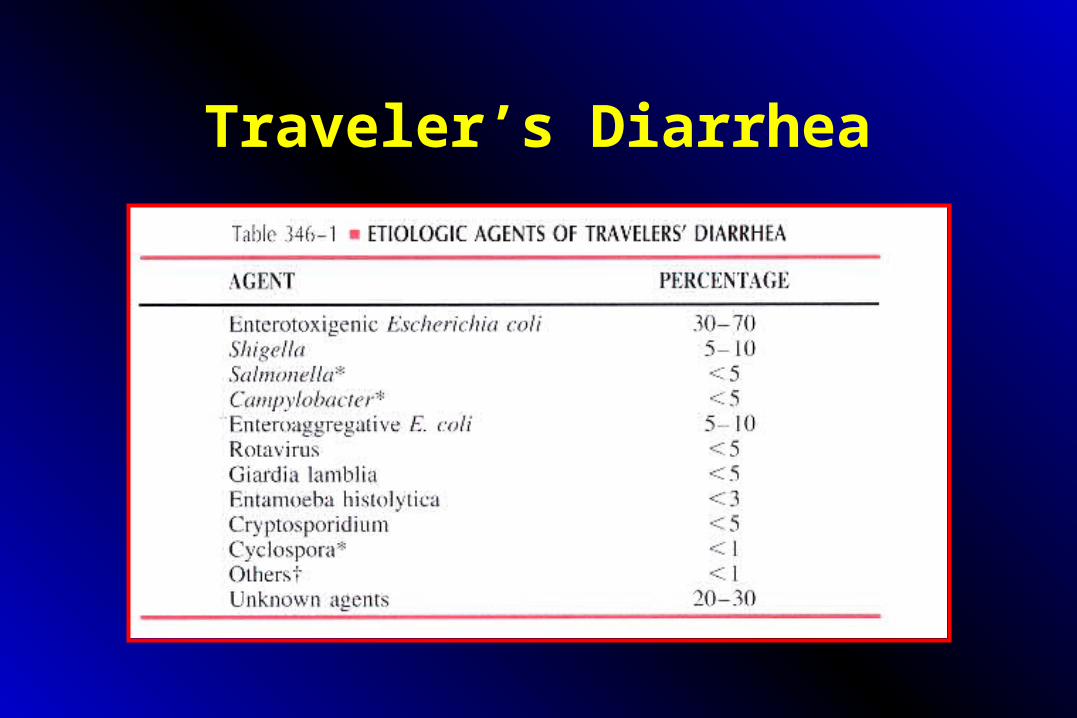
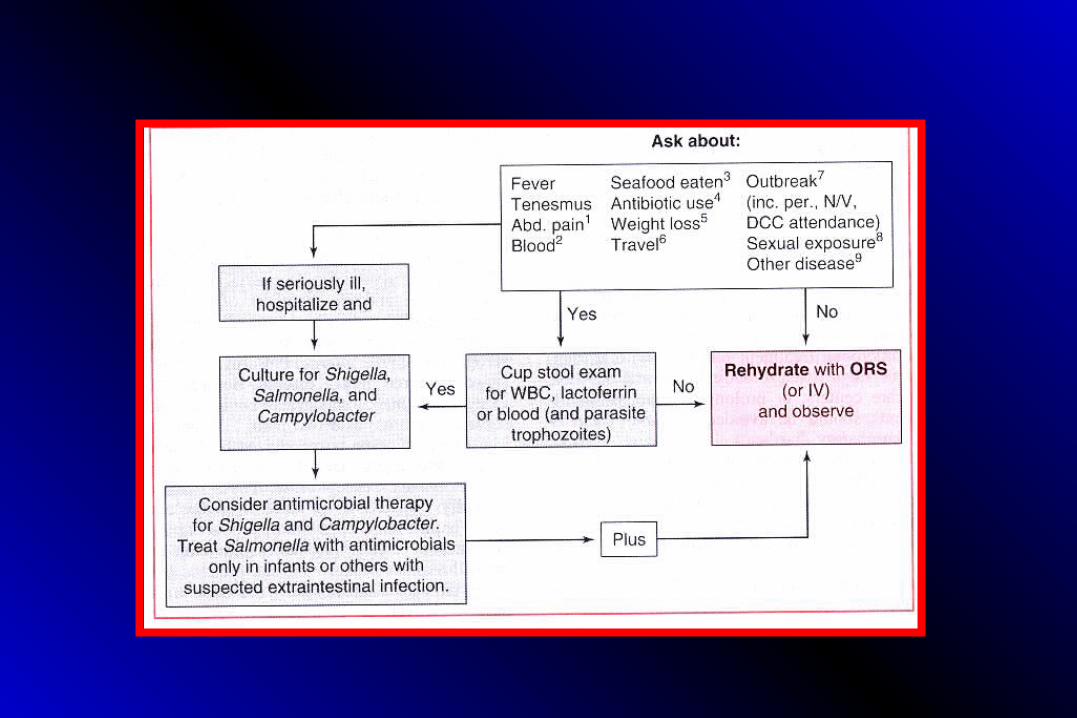
Traveler’s Diarrhea

Vibrio bacilli
Vibrio vulnificus

Vibrio


Vesicles of V. vulnificus Infection

Vesicles of V. vulnificus Infection

Erythema of the V. vulnificus infection

Recommended














![[Ajou Greative 콘서트] 글로벌 sw엔지니어로 성장하기](https://img.pdfslide.net/doc/110x75/58ee8dc91a28ab0f108b45ed/ajou-greative-sw-.jpg)

