ShoemakerCertificationDianeParks,APRN-NPMay4,2020
1
ChronicInflammatoryResponseSyndrome(CIRS)Understanding,DiagnosingandTreating
DianeM.Parks,APRN-NPTheWellforHealth,PLLC
575DavidsonGatewayDrive,Suite100Davidson,NC28036
704-799-5433

ShoemakerCertificationDianeParks,APRN-NPMay4,2020
2
Chronic Inflammatory Response Syndrome (CIRS)
Understanding, Diagnosing and Treating History ChronicInflammatoryResponseSyndrome(CIRS)isamulti-system,multi-symptomillnessassociatedwithexposuretobiotoxinsorneurotoxins.Itisusuallypresentinasubsetofthepopulationwithgeneticsusceptibilitycharacterizedbyagroupingofsymptoms,proteometrics,genomicabnormalities,specificbrainchangesandabnormalvisualcontrastsensitivity.(1)Thisisnotonlyaninflammatorydisorder,butalsoanimmunemechanismdysfunctioncausedbytoxins,anddependingongeneticprofile,canaffectupto24%ofthepopulation.Thesepatientsareoftenseenmultiplepractitionerspresentingwithalonglistofmisdiagnoseshavingspentthousandsofdollarsresultinginlittleornosymptomaticimprovement.Thelistofdiagnosesmayinclude-butnotlimitedto-dementia,autoimmunedisease,chronicfatigue,fibromyalgia,ADD/ADHD,depression,panicdisorder,generalanxietydisorder,bipolardisorder,insomnia,cardiovascular/respiratorydisease,asthma,exerciseintolerance,obesity(suggestiveofindifferencetotheconsequences),allergies,irritableboweldisorder,andsomatization.Typically,theirqualityoflifeisgreatlydiminishedastheyexperiencedysfunctionwithintheneurological,immune,endocrine,circulatory,respiratory,muscularskeletalandpsychologicalsystems.Mostofthecreditfortherecognition,evaluation,andtreatmentofCIRSbelongstoDr.RitchieShoemaker,whoin1997asafamilypractitionerinPocomoke,Marylandfirstnotedthesignsandsymptomsofthissyndromeinlocalfishermen.ThesefishermenbeganpresentingwithstrikingphysicalandneurologicsymptomsafterexposuretoenvironmentalfactorsthatwerealsocausingfishtodieinlargenumbersinconjunctionwithPfiesteriabloomoutbreaksinthePocomokeRiver.Focusedinvestigationbyhim,incollaborationwithothernotedcolleagues,ledtotheevolvingfoundation,research,andformulationoftheShoemakerProtocolformanagementofthispreviouslyunrecognizedsyndrome.Withtime,Dr.Shoemakerandhiscolleaguesbegantorecognizestrikingsimilaritiesinotherpatientswithsimilarsymptomsexposedtoothertoxins,suchasmoldfromwaterdamagedbuildings(WDB),tickbornemicrobes(BorreliaburgdoferiandBabesiamicroti),reclusespiders(brownandMediterranean),ciguaterafromingestionofcontaminatedfish,andinhalationorcontactwithalgaebloomscontainingcyanobacteria.Sincetheinitialrecognitionofachronicimmuneresponsesyndrome,researchbasedstrategiesdevelopedbyDr.Shoemakerhasresultedinthediagnosisandtreatmentofover10,000patientsworldwide. InflammatoryandImmuneCascade Inahealthy,non-geneticallysusceptibleperson,theremovaloftoxinsisaccomplishedbytheinterplaybetweentheinnateandadaptiveimmunesystems.Theinnatesystemistheprimary

ShoemakerCertificationDianeParks,APRN-NPMay4,2020
3
andfirstrespondertoinvadingantigens.ByactivationofcytokinesandTGF(TransformingGrowthFactor)Beta-1fortherecruitmentofimmunecellstotheareaofinsult,itinitiatesactivationofthecomplementsystemtoassistinremovingtheinvadingantigens.Theinnatesystemthencommunicateswiththeadaptiveimmunesystem(orsecondlineofdefense)todestroythetoxinsbypresentingthemtoinflammatoryTcelllymphocytesbywhichinductionofantibodiesbyBcellsoccurs.NaturalkillerTcellsarealsoactivatedtoproduce,amongotherfactors,cytokines,includingIL-2andTNF-alpha,andlendsupporttoBcellantibodyproduction.Whentheadaptivesystemisintactandworkingappropriately,(i.e.withoutadefectiveHLAsystem),itprovideslong-lastingimmunityandreturntohomeostasis.Thesetwosystemsarequiteeffectiveinprovidinganadequatedefensefromforeigntoxinsinapproximately75%ofthepopulationwithanormalhistocompatibilitygenegroup,anentitythatprovidesinstructionformakingHumanLeukocyteAntigens.TheHLAcomplexhelpstheimmunesystemdistinguishthebody’sownproteinsfromotherforeigninvaderproteinssuchasthosemadebyvirusesandbacteria.Inbiotoxinillness,theHLAchallengedindividualisincapableofmountinganadequateresponseandthusunabletoclearthetoxin.Thisleadstochronicactivationoftheinnatesysteminwhichinflammatorycytokinesareleftinplaceresultingindysregulationofmultiplebodysystems.(2)IfthisindividualisnotproperlyevaluatedforprompttreatmentbyoneexperiencedinCIRSmanagement,toxinscanremaininthebodyformonthsandyearsleadingtoextraordinarydamage,expensivemisdiagnosesbyprovidersnotawareoftheetiology,andultimatelyamajorinterferenceinthepatient’squalityoflife. INSTIGATORSOFCIRSListedbelowareexamplesofknownsourcesofbiotoxinsfoundtoinitiateCIRS.Theyareresponsiblefortriggeringtheinnateandadaptiveimmunesystemscausingsystemicinflammation.
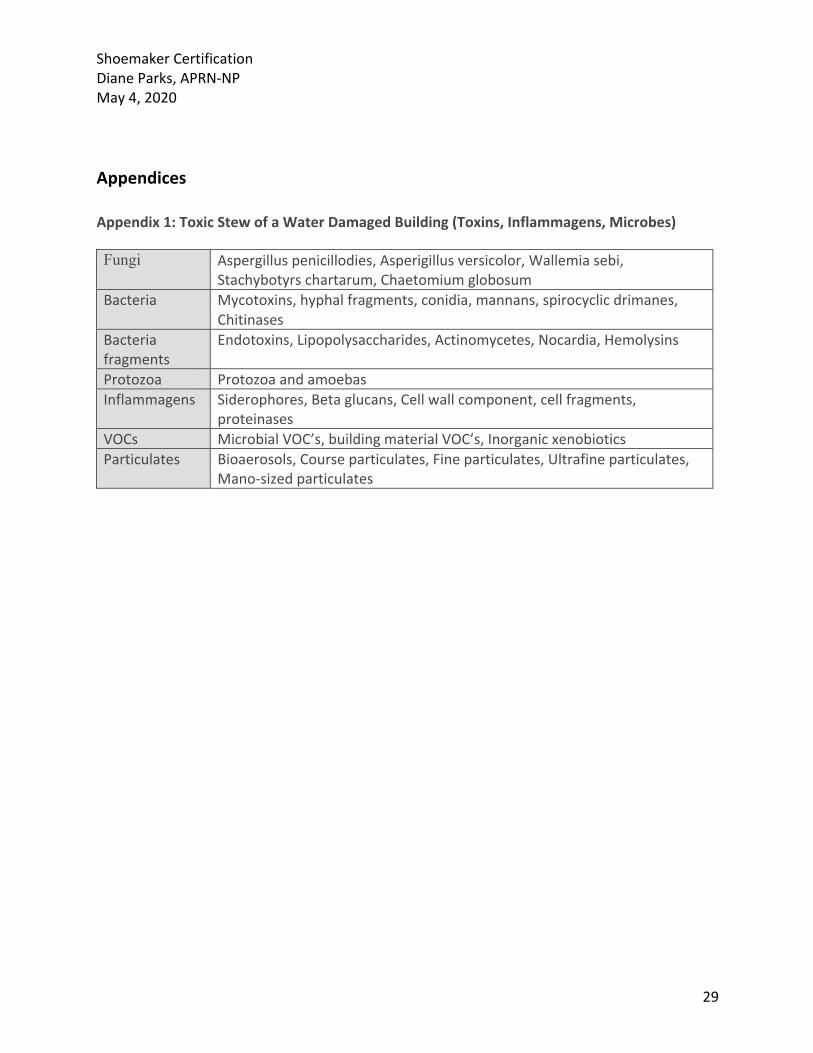
• CIRS-WDB(WaterDamagedBuilding):Examples-Chaetomiumglobosum,Aspergilluspenicillioides,Aspergillusversicolor,Stachybotryschartarum,Wallemiasebi,Actinomycetes,bacteriaandinflammagens.AWDBhasbeencalleda“toxicstew”asatleast30potentiallytoxicentitieshavebeenidentifiedandallcansetoffaninnateimmuneresponse.(Appendix1)
• CIRS-PostLymeSyndrome(PLS):Borreliaspecies• CIRS-possibleestuarineassociatedsyndrome(PEAS):Pfiesteria(dinoflagellate)• CIRS-Ciguateria:Gambierdiscus(dinoflagellate)• CIRS-Arachnids:Reclusespiders(brownandMediterranean)• CIRS-Apicomplexans:BabesiaSpp.,Sarcocystis• CIRS-Cyanobacteria:Microcystis,Lyngbya,Cylindrospermopsis,Anabaenopsis
DiagnosisofCIRS AnaccuratediagnosisofCIRSrequiresadetailedassessmentofthemanysignsandsymptoms

ShoemakerCertificationDianeParks,APRN-NPMay4,2020
4
presentedbythepatient.Byitsverynature,CIRSisacomplexconglomerationofmanydysfunctionalprocessesthatcanmimicmanyotherdiseases;therefore,itishelpfultoformulateaconcertedplantodifferentiateitfromtheseotherthesediseases.AdetailedlongtermhistoryisrequiredwhichwouldincludeaspecificCIRSclusterofsymptomsquestionnaire(seebelow).Inaddition,visualcontrastsensitivitytestingandacomprehensivephysicalexamarenecessaryelementsoftheinitialassessment.(3)Atwo-tieredsystemcasedefinitionwasintroducedbyDr.Shoemakerin2005tomoredefinitivelyestablishthediagnosis.Itsfocuswastomakeanobjectivemodeltoallowatoolforaccuratediagnosis.AstandardizedprocesswasthenimplementedinwhichallofthecriteriaforTierOnehadtobemetandthreeoutofsixmeasuresinTierTwohadtobemettomakethediagnosis.Furthermore,in2008,theGovernmentAccountabilityOffice(GAO)reviewing54studiesfromUSagenciesinvolvedwithconsequencestoexposuretoWDB,notednosignificantcoordinationwiththeseagencies,andasaresult,proposedafederalcasedefinitionrequiringtheinclusionofcriteriaforCIRS-WDB.(4)Subsequently,athirdtierwasaddedfortheevaluationofsuccessoftreatment.Incoordinationwiththisreview,theelementsfordiagnosisofCIRSwasexpanded.ThefollowingliststherequirementsofTierOne,TierTwo,andTierThreecriteria: Tier1(Allofthefollowingcriteriamustbemet)1) Potentialforexposuretotoxinsinawaterdamage/dampindoorspace.Thisincludes
visualmoldgrowth,mustysmellsorabnormalERMItest(MSQPCR),tickorspiderbite,eatingfishthatfeedsonabarrierreef,exposuretoPfiesteriaorCyanobacteria
2) Presenceofamultisystem,multi-symptomillnesswithspecificsymptomsmirroringthoseoutlinedinpublishedstudies.AClusterofSymptomsQuestionnairehasbeendevelopedforeaseinidentifyingthesesymptoms.Ascoreof8of13symptomsindicates92%likelyhoodofCIRS,6of13issuspicious.Inchildren,5of13issignificantandwarrantsfurtherevaluation.(Appendix2)
3) Absenceofpertinentdifferentialdiagnosesafterathoroughevaluation(3)Tier2-(Atleast3of6criteria)
• FailedVisualContrastSensitivityTest(VCS)–Neurotoxicillness• HLADR/DQMutations–Geneticsusceptibility• Increaseinatleast1of3inflammatorymarkers:MatrixMetalloproteinase-9(MMP-9),
TransformingGrowthFactorBeta-1(TGF-beta1),C4a-Cytokineactivation• DecreasedalphaMelanocyteStimulatingHormone(MSH)–Hypothalamicimpairment• DysregulationADHorCopeptin/Osmolality–Pituitaryandperipheralendocrine
dysregulation• DysregulationofACTH/Cortisol–Pituitaryandperipheralendocrinedysregulation(7)
Tier3–(Improvementinatleast2of3markers)
• CholestyramineorWelchol/Colesevelam–resolutionofsymptoms

ShoemakerCertificationDianeParks,APRN-NPMay4,2020
5
• ReducedLeptin,ifincreasedpriortotreatment• ReducedMMP-9,ifincreasedpriortotreatment(3,6,30)
TheBiotoxinPathway Forabetterunderstandingofchronicinflammatoryresponsesyndrome,Dr.Shoemakerhasprovidedapathwaychartdepictingtheeffectsofbiotoxinsongeneticallysusceptiblepeopleandthevariedresponsesthebodymayengendertocombattheinsult.Inthispopulation,thenormalresponseoftheimmunesystemforremovingtheinsultisaltered;therefore,unregulatedandexaggerateddefensemechanismsareleftunchecked.Thisleadstoacascadeofdetrimentalsymptomsandpathology.Exposurestriggeringthepathwayinclude,butarenotlimitedto,toxinsfromWDB,infectedtickbornebacteria/parasites(Borrelia,Babesia,Ehrlichia),inhaled,ingested,orskinabsorbeddinoflagellates(Pfiesteria,Ciguatera),locallyinjectedvenom(Loxoscelesspecies),andinhaledorabsorbedCyanobacteriatoxin.Thedegreeofsymptomandsystemresponsetoanyoftheseinsultsmaydependontheamountofexposureandthetoxininvolved.(5)
ShoemakerCertificationDianeParks,APRN-NPMay4,2020
6
ConfirmingDiagnosisofCIRS AftermeetingthesystemcriteriainTierOneoutlinedpreviously,thenextstepistoconfirmthediagnosis.ManytestshavebeenlistedinTierTwoandaredescribedbelowinfurtherdetail.ItisimportanttonotetherearemanyteststhatwillmostlikelynotbeabnormalincludingCBC,metabolicprofile,ESR,CRP,TSH,ANA,ImmunoglobulinsIgG,IgM,IgE),Lipidprofiles,Antibodyprofiles,allcomplementexceptforanaphylatoxins,allgenetictestingexceptforHLADR/DQ,LH,FSH,SHBG,estradiol,estrone,prolactin,normalEKG,viralstudies.(3,6)1) VCStest–PositivetestmeansdeficiencyincontrastingabilityVisualcontrastisameasureofneurologicalfunctionbytheabilitytodifferentiatebetweenvisualpatternsofgrey,black,andwhite.Dr.KenHudnell,aneurotoxicologistfortheEPA,wasthefirsttouseVCStestingforbiotoxinillness.Chemicals,toxins,andmedicationshaveallbeenimplicatedinnegativelyaffectingthevisualnervoussystem.Specifically,capillaryhypo-perfusioncausedbyinflammationfromtoxinscompromisetheopticnerveandretinasuchthatthevisualcontrastdelineationisdecreasedasopposedtovisualacuity(thesharpnessofretinalfocus)whichisleftlargelyunaffected.AccordingtoDr.Shoemaker,92%ofCIRSpatientswillfailVCStesting:however,8%willfalselypassiftheypossessoutstandingvisualacuitydespitesevereinflammation.IfthepatientfailstheVCStestandsymptomclustersarepositive,thelikelihoodofCIRSexceeds98.5%.(7)TherearetwomethodsoftakingaVCStest:1)anonlineversionfoundonthehomepageofwww.survivingmold.comand2)arecommendedhandheldversionpurchasedathttps://www.survivingmold.com/store1/vcs-aptitude-handheld-kits.Carefuladherencetodirectionsisnecessaryforaccurateassessment.Determinationofapassingscoreoccurswhenapatient,usingoneeyeatatime,isabletoseebeyondrow6incolumnCandbeyondrow5inColumnD.ColumnEisusedtomonitortreatmentsuccessaswellasmonitorpossibleintensificationreactioninpatternswithLymedisease.(3)Inregardstoimprovement,Dr.Shoemakerstates,“ariseinoneblockinonecolumnisnotsignificant,butariseofoneblockfromeachoffivecolumnsissignificant.Ariseoftwoblocks(orafallintwoblocks)foranyonecolumnissignificant.(8)2) HLADR/DQTest(HumanLeukocyteAntigen)–(LabCorptest#167120)ThistestdeterminesifapatientisgeneticallysusceptibleforthedevelopmentofCIRS.Inthesusceptiblepopulation,theinnateimmunesystemrecognizesthebiotoxinssendingsignalstotheadaptiveimmunesystemtorespond.Unfortunately,theadaptiveimmunesystemdoesnotrecognizethebiotoxinsandthereforecannotmakeantibodiesagainstthem.Withoutthehelpoftheadaptiveimmunesystem,theinnatesystemisconstantlytriggered(upregulated)creatinghighlevelsofinflammation.Thisincitesamulti-system,multi-symptomillnessknownasCIRS.

ShoemakerCertificationDianeParks,APRN-NPMay4,2020
7
Dr.Shoemakerhasconductedanextensivegeneregistryandfoundthatapproximately24%ofthepopulationis“mold”susceptibleand21%isLymesusceptible.(9)LymesusceptiblepatientsdonotalwaysrespondwelltoantibioticsandmayneedCIRStreatmenttohelpenableclearanceofthetoxin.LymepatientsalsotendtohaveanincreasedriskofdevelopingCIRS-WDB.(4)Dr.ShoemakerdevelopedtheRosettaStoneIndexwhichwasdesignedasascoringmethodbaseduponacompilationofHLAhaplotypestoassesstheriskofsusceptibilitytoseveraltoxins.(10)Acaveat:Notallonlineautomaticinterpretationofresultsiscompletelyaccurate,therefore,thereistheneedforprovideradeptnessforaccurateinterpretation.(Appendix3)3) aMSH(alphamelanocytestimulatinghormone)(LabCorptest#10421)Referencerange:35-81pg/mLAlphaMSHisaneuro-regulatoryhormoneinstrumentalinensuringoptimalimmunesystemresponse.Italsohaspowerfulanti-inflammatoryactions.(7)InCIRSpatients,MSHisusuallylowcausingabnormalregulationofcytokines,endorphins,melatonin,sexhormones,cortisol,andACTH.Contributingsymptomsincludechronicfatigue,unusualpainfeatures,sleepdisturbance,headaches,temperatureinstability,muscleaches,anddecreasedconcentration.Inaddition,physiologicdisturbanceswithglutenintolerance,ADH/osmolalityimbalance,andleptinresistantweightgainhavebeendemonstrated.4) MARCoNS(multipleantibioticresistantcoagulasenegativestaph)(MycobiologyDX)ReferenceRange:PositivewithorwithoutbiofilmsorNegativeMARCoNSisfounddeepwithinthenasalpassagesandisextremelycommoninthosewithCIRS-WDBaswellaspatientswithpostLymeSyndromewhohavebeentreatedwithantibioticsforaprolongedperiodoftime.Inthepast,MARCoNSwaspresumedtobebenigncolonizersofthenoseandskin,butwiththeincreaseuseofantibiotics,thesebacteriahaveshownresistancetotwoormoreantibiotics.Theyhavenowbecomepathogensabletoproducebiofilmsallowingthebacteriatoliveundetectedandactlikemulticellularorganisms.Thebiofilmhinderspenetrationofantibioticsfortreatment.MSHandMARCoNShaveabidirectionalrelationship.NasalmembranesareprotectedfromcolonizationbyadequateMSHlevels;however,withdecliningMSH,theprotectivelayerisreducedleadingtothedevelopmentofMARCoNS.Ithasbeenshownthat80%ofMSH-deficientpatientswillhaveMARCoNSandwiththispresence,MSHcontinuestodecline.Initially,itwasthoughtMARCoNSwasconfinedtothenose,butrecentlyMARCoNShasbeenculturedfromdentalcavities.MostpatientswithMARCoNSdonotexperiencenasalcongestion,rhinitis,orsinusitis,butdohavecognitiveconcernsdescribingsymptomsas“brainfog”,declineinmemory,attentionandconcentration.
ShoemakerCertificationDianeParks,APRN-NPMay4,2020
8
AMARCoNStestshouldbepartoftheinitialwork-upforCIRS.ItisdonewithaAPI-STAPHnasalcultureobtainedfromthenasopharynx.Onlyonesideofthenoseneedsbetestedinsertingtheswabdeepwithinthenasalpathwayorapproximately3-4inches.Itisimportanttogoslowly,takingcaretofollowingtheangleofthepassageandonceinthecorrectarea,twirltheswabfor3-5seconds.MicobiologyDXprovidestestkitsandsampling:http://www.microbiologydx.com.(3)5) MMP-9(matrixmetalloproteinase-9)(LabCorptest#500124)Referencerange:0-322ng/mL–PerDr.ShoemakerLabCorpcurrentreferencerangeof85-332isincorrectastheystilluseEsoterixrangethatcombinescontrolsandcases(6)MMP-9isanenzymeoftheinnateimmunesystemproducedbybloodvesselendothelium.ExpressionofMMP-9istriggeredbyhighlevelsofcytokines.Onceelevated,increasedvascularpermeabilityoccursthusdeliveringinflammatoryproductstolocaltissuesincludingthelungs,nervousandmuscularsystems.Symptomsincludeheadaches,musclepain,cognitiveissues,alteredlungfunction,staticshocks,andneurologicalissues.(11)6) C4a(complement4a)(NationalJewishONLY)Referencerange:<2830ng/mL-NOTE:BecauseJewishNationalistheonlyreliablesourceoftesting,itmaybeverydifficultforpatientstoobtainthistest.ThismarkerisofgreatsignificanceinCIRS-WDBdiagnosisandisalsousuallyelevatedwithexposuretodinoflagellates,cyanobacteria,andpersistentLymedisease.Itisacomplementsplitanaphylatoxinwhichmediateschemotaxis,contractionofsmoothmuscle,histaminereleasefrommastcells,capillaryhypoperfusionandincreasesvascularpermeability.Exposuretoabiotoxinactivatesthemannosebindinglectinassociatedenzymes(MASP-1andMASP-2)producingC4a.SymptomsrelatedtoanelevatedC4aincludefatigue,respiratoryconcernsandcanalsoplayaroleinchangesofsixexecutivefunctions:decreasedconcentration,difficultywithwordfinding,decreasedassimilationofnewknowledge,confusion,anddisorientation.ItpotentiallyplaysaroleinAlzheimer’sdiseaseasadecreaseinC4aseemstobeassociatedwithimprovedsymptoms.Thistestisnotonlyusedforassessmentofcurrentexposure,butalsoforre-exposureinthatanincreaseinC4acanoccurwithin10minutesofexposure.Itisthereforeagoodscreeningtoolforbothcurrentandrecurrentexposuretrials.ClinicalseverityoftencorrelateswithhigherlevelsofC4a.Itisthereforeagoodscreeningtoolforbothcurrentexposureandre-exposuretrials.Oftentimes,clinicalseveritycorrelateswithhigherlevelsofC4a.(6)7)C3a(NationalJewishONLY)Referencerange:<940ng/mL-NOTE:Thistestisalsoverydifficulttoobtain.C3aisananaphylatoxinwhichstimulateshistaminereleasefrommastcellscausingcontractionofsmoothmuscle,capillaryhypoperfusion,andincreasedvascularpermeability.C3astimulates

ShoemakerCertificationDianeParks,APRN-NPMay4,2020
9
theadaptiveimmunesystem,inducesandmodulatesTandBcellproductionandproliferation.Itisfoundinthelung,kidney,andbrain.ThepresenceofbacterialmembranesmayelevateC3aexemplifiedbyactivationinmanyactiveLymepatients.(3)8)Leptin(QuestTest#90367orLabCorpTest#146712)Referencerange:Male:0.5-13.8ng/mL;Female:1.1-27.5ng/mLLeptinisproducedinadipocytesandlinkstheneuroendocrineandimmunesystemsactingasbothahormoneandcytokine.CytokinessuchasTNFalpha,IL-6,andIL-1areunregulatedresultinginheightenedinflammationandinsomepatients,elevatedplasminogenactivatorinhibitor-1(PAI),abnormalvonWillebrandfactor’s(VWF),andFactorVIIIresultingincoagulopathies.Theseinflammatorycytokinesblockleptinhypothalamicreceptorscreatingleptinresistance.Leptinresistancedecreasesthebody’sabilitytousefatstoresasenergygivingrisetodramaticweightgaindespitecalorierestrictionandexercise.LeptinlinksthehormonesystembyaffectingMSH,ACTH,andendorphinproduction.Forinstance,symptomsassociatedwithalowerMSHmightincludetemperatureinstability,headaches,muscleaches,anddecreasedabilitytoconcentrate.(7) 9)TransformingGrowthFactorbeta-1(TEGbeta-1)(Questonly–Test#91238:performedatCambridgeMedical)Referencerange:<2382pg/mLTGFbeta-1isaproteinplayinganimportantroleintheregulatorypropertiesoftheimmunesystemespeciallyinregardtotissuerepairandfibrosis.Itisproducedbylymphocytes,macrophages,anddendriticcellsandcontrolsgrowth,differentiation,activation,anddeathofimmunecells.IthasbeenassociatedwithautoimmunediseasesspecificallySLE,rheumatoidarthritis,dermatomyositis,scleroderma,ulcerativecolitis.Inaddition,lungfibrosis,vocalcordpolyps,GIdysfunctionandanincreasedincidenceofopportunisticinfectionhasbeenlinkedtoelevatedlevelsofTGFbeta-1.Oneexampleofitseffectsisonlungperformancenotedbyanincreasedincidenceofpulmonarysystolicpressureandpossibleprogressiontopulmonaryhypertension.InconjunctionwithelevatedproductionofMMP-9andVEGF,TGFbeta-1hasalsobeenimplicatedwithincreasedbloodbrainbarrierpermeabilityresultingininflammatoryconsequencessuchaslearningdisabilitiesandcognitivedysfunction.(3)10)VascularEndothelialGrowthFactor(VEGF-plasma)(Quest–Test#14512orLabCorp–Test#117006)Referencerange:31-86pm/mLVEGFisagrowthfactor,whichinhealthpeople,dilatesbloodvesselsinresponsetohypoxiainduciblefactor(HIF).Hypoxiaoccurswheninflammatorycytokineboundtotheendotheliumreleasechemicalsnarrowingthecapillaries.RegulatorycellsthenproduceHIFwhichinducesanincreaseVEGF.LowVEGFmaybeanindicatorofcapillaryhypoperfusionleadingtofatigueand
ShoemakerCertificationDianeParks,APRN-NPMay4,2020
10
cognitivedecline,andifpresentinskeletalmuscle,decreasedmuscleendurance.Treatmentisnecessaryforlevels<31;however,inCIRSpatients,levelscanbeover100indicatingactivationoftheinnateimmuneresponseasthebodycompensatesforlowoxygendelivery.VeryhighVEGFcanalsooccurwithrenalfailureandrarelycancer.(2,6)11)Anti-GliadinAntibody(AGA–IgG,IgA)(Quest–Test#8889orLabcorp–Test#161646/161647)Referencerange:0-19UThoughelevatedAGAdoesnotnecessarilyindicateceliacdisease,itdoesstronglysuggestaninflammatoryresponsetogluten.Inglutensensitivepatients,theadaptiveimmuneresponsemediatedbytheantigen-specificTregulatorylymphocytesincitesautoimmunedysregulation.InCIRSpatients,whooftenhavelowMSHlevels,thisdysregulationcanbeenhanced.AGAIgGandIgAareantibodiesagainstgliadinfoundingluten,aproteinpresentinwheat,barley,andrye.Oats,too,canbeaninstigatoroftheresponseifcrosscontaminationoccursinprocessingwithgliadincontainingfoods.NOTE:Ifapatientisstrictlyglutenfree,itisstillnecessarytotestAGA.(2)12)AndrogenDeficiency–TotaltestosteroneandDHEA-sulfate(QuestorLabCorp)Referencerange:VariesbysexandageNOTE:Optimally,amoresensitiveassayisperformedinmenopausalwomentoassurethemostaccurateresult.
• Testosterone(Female:sensitive)–QuestTest#15983,LabCorpTest#500159• Testosterone(Male:regular)–QuestTest#36170,LabCorpTest#4226• DHEA-sulfate–QuestTest#402,LabCorpTest#4020• Estrone–QuestTest#23244,LabcorpTest#4564• Estradiol–sensitive(menopausewomenandmen)–QuestTest#30289,LabCorpTest
#140244• Estradiol–regular(Non-menopausalwomen)–QuestTest#4021,LabCorpTest#4515
Androgenlevelscanbecomeabnormallylowduetoupregulationinthearomataseenzyme.DHEA-smayalsobelow.Inflammationcausesmorerapidconversionoftestosteroneintoestrogenresultinginhighestrogenandlowtestosterone.Testosteronetherapyiscontraindicatedinthesepatients.DHEA-smaybeusedinitsplace,butitnecessitatesmonitoringestrogenlevelssotheyarenotelevatedasopposedtotheintendednormalizationoftestosterone.Forthisreason,bothestroneandestradiolshouldbetestedtoinsureproperconversion.Symptomsofhormonaldysregulationincludefatigue,musclewasting,lowlibidoandsexualdysfunction,highhematocrit/hemoglobin,midabdominalweightgain,gynecomastia,waterretention,PMScomplaintssuchasanxietyandirritability.(12)13)vonWillebrand’sComprehensivePanel(Questonly–Test#19790)

ShoemakerCertificationDianeParks,APRN-NPMay4,2020
11
ReferenceRange:<50or>150IUforFactorVIII,vonWillebrand’santigen,orRistocetinassociatedcofactorVonWillebrand’sDiseaseistypicallyaninheriteddisordercharacterizedbyexcessiveorprolongedbleeding.InCIRSpatients,however,theconditioncanbeacquiredasaresultofincreasedC4awhichmayparadoxicallyresultinbothbleedingtendenciesandhyper-coagulation.Symptomsrelatedtobleedingtendenciesincluderecurrent,sometimesprofusenosebleeds,generalizedbleeding,andheavymenstrualperiods.Conversely,otherswiththeacquireddisordermaybeatsignificantriskforintravascularclottingresultinginpulmonaryembolism,deepveinthrombosisormicro-emboliinthebrain.Ifhyper-coagulationoccurs,cognitivedeclinemaybeapresentingsymptomduetothedecreasedoxygendeliverydistaltoembolithoughpatientsoftenareasymptomatictotheincitingevent.IfacquiredvonWillebrand’sdiseaseispresent,otherpertinentlabstoconsiderinclude:PT,PTT,Sedrate,D-dimer,fibrinogen.Otherthanavoidanceofexposuretoincitingfactors,treatmentwithdesmopressin(DDAVP)maybewarrantedforepisodesofprofusebleeding.(2)14)PlasminogenActivatorInhibitor-1(PAI-1)(QuestTest#36555,LabCorp#146787)(ReferenceRange:4-43ng/mL)PAI-1isanacutephasereactantthatcanbecomeelevatedwithinfection,pregnancy,inflammationandtrauma.Itcanincreaseriskofhypercoagulation.(3)15)AnticardiolipinAntibodies(IgA,IgG,IgM)(QuestTest#,LabcCorpTest#161950)Referencerange:Negative=ACAIgA<11APL;ACAIgG<14GPL;ACAIgM<12MPLAnticardiolipinantibodiesattackthecardiolipincellularmembraneandcancauseabnormalbleedingtendenciesincludingincreasedbloodclotting.Theseantibodiesarefoundinpatientswithlupus,sclerodermaautoimmunethrombocytopenia,pulmonaryembolism,deepveinthrombosis,andendocarditisfromclotformationonheartvalves.Inpregnancy,theymayalsoincreasetheriskofspontaneousabortion.16)AntidiureticHormone(ADH)(LabCorponly,Test#10447)(QuestnowSubstitutesCopeptininitsplace,Test#37740)QuestmakestheassumptionthatCopeptinisamorereliablemarker.(13)CurrentlyareviewofresultsisunderwayintheCIRSprofessionalcommunitytodetermineanoptimalCIRSreferencerange.CIRScompetentprovidershavereportedanormalrangebetween3-4pmol/LasanequalcorrelationtoanormalrangeofADH<0.8pg/ml.SerumOsmolality(QuestTest#677,LabCorpTest#2071)Referencerange:280-300mOsm/L

ShoemakerCertificationDianeParks,APRN-NPMay4,2020
12
Antidiuretichormone(ADH),alsoknownasvasopressin(AVP),isahormonesecretedbythepituitaryglandinresponsetoextracelluarfluidhypertonicity.Itregulatesfluidbalancebyincreasingsolute-freewaterreabsorptionbackintocirculationfromthekidneyandsecondlycausesconstrictionofarteriolesincreasingperipheralvascularresistance.Bythesemechanisms,ithelpstomaintainbloodpressure,bloodvolume,andtissuewatercontent.Osmolalityisameasureoftheconcentrationofdissolvedsolutessuchassodium,potassium,chloride,andglucose.(9)ADH/osmolalitydysregulationoccursin60%ofCIRSpatientscontributingtosymptomsoffrequenturination,dehydration,excessivethirst,andheadaches.Excessivesaltontheskinactsaconduitforelectricalstaticshocks.(3)17)AdrenocorticotropinHormone(ACTH)/Cortisol(ACTH:QuestTest#211,LabCorp#4440)(Cortisol:QuestTest#4212,LabCorp#4051)NormalReferenceRange:ACTH:8-77pg/mL(Mustbedrawnbetween7-10am)Cortisol:AM4.3-22.4ncg//dL(drawnbetween7-9am)PM3.1-16.7ncg/dL(drawnbetween4-5pm)(9)ACTHDysregulation:
1) Absolutehigh:ACTH>45orCortisol>212) Absolutelow:ACTH<5orCortisol<43) Relative:ACTHwas<10whencortisolwas<74) Relative:ACTHwas>15whencortisolwas>16(2)
Thehypothalamic-pituitary-adrenal(HPA)axisisafeedbackresponsetoincomingstressfrommanybodysystems.ACTHisreleasedbythepituitaryglandandsignalstheadrenalglandtoproducecortisol.Cortisolhasmanyfunctionsamongwhichincludestimulatinggluconeogenesis,regulatingglycogenstoresintheliver,immuneregulation,andthephysiologicalresponseof“flightorfight”.Inthebody’sreactiontoacuteillness,stress,inflammation,fever,bacterialorviralinfections,cortisolsecretioninitiallyrises(iftheadrenalgland’scapabilityisintact)tomodulatethestressresponse;however,withchronicexposuretoadversestimuli,typicalinCIRSpatients,cortisollevelsmaydecreaseduetoadrenalglanddiminutioninitsabilitytomaintainanadequateresponse.Asaresultofthisdiminishedresponse,ACTHproductionisadjustedbythehypothalamicsensitivitytothesesignalsresultinginasubsequent“instruction”tothepituitaryglandforthereleaseoftheappropriatesecretionofACTH.Unfortunately,inCIRSpatients,thecapacitytoperformthisfunctionmaynotbeadequateandsymptomssuchasdaytimefatigue,sleepdisturbance,insomnia,dizziness,andfluctuatingbloodsugarlevelsmayresult.(9)Dr.Shoemakerhasalsoreportedthat60%ofCIRSpatientswithlowMSHwillexperiencelossofcortisolregulation.(7)18)VasoactiveIntestinalPeptide(VIP)–importantbutnolongermeasuredastestinghasbeenfoundtobeunnecessary

ShoemakerCertificationDianeParks,APRN-NPMay4,2020
13
VIPisaneuro/endocrinepeptidepossessingdiversecardiovasculareffectsthatincludevasodilatationofthecerebralandcoronaryarteries,stimulationofmyocardialcontractility,relaxationofsmoothmuscleinthetrachea,stomach,andgallbladder.Itisproducedbyimmunoreactivenervefibersoriginatingfrommanytissuesincludingthegut,pancreas,andhypothalamus.OftendiminishedinCIRSpatients,resultingsymptomsincludeshortnessofbreath(especiallywithexercise),increasedinflammatorycytokinerelease,androgendeficiency,andcognitiveimpairment.IntranasaladministrationofVIPhasbeenshowntosignificantlyimprovealloftheabovesymptomsandinaddition,helpcorrectproteomics,transcriptomics,andgreymatternuclearatrophy.(7)
19)Transcriptomics–GeneExpression:InflammationExplained(GENIE)GENIEisarelativelynewtestthatisrevolutionizingdiagnosisandtreatmentinCIRSpatients.Itcontains175reportergenescoveringareassuchasmitochondrialATPsynthase,tolllikereceptors,apoptosis,caspases,andmore.Firstconceived10yearsago,followedbymorethan3yearsofdevelopmentandvalidation,thetestbecameavailable.CIRSpatientsareinastateofhypometabolismmanifestedbypathologicsuppressionofribosomalandnuclearencodedmitochondrialgenes.(15)In2016,Dr.ShoemakerandJamesRyanPhDpublishedresearchshowingthesequencingofRNAinpatientswithCIRStreatedwithVIP.TheresultsshowedVIPdownregulatedgeneexpressionwhichcorrelatedwithresolutionofsymptoms(3,31)Thesefindingssuggestapowerfulpotentialfortreatmentinpatientswithchronicfatigue,fibromyalgia,andtheillnesseswithunknownetiologies.(15)GENIEcanbeorderedbypatientorprovider:www.survivingmold.com/store1/progene-dx.20)Otherimportanttests/procedurestoconsider
• PulmonaryFunctionTests–Baselineoneveryoneandthenasneeded(Asthmaisassociatedwithobstructive,butifrestrictiveconsiderinterstitiallungchangesassociatedwithCIRS.
• EKG–baselineoneveryoneandthenasneeded• Pulmonaryarterysystolicpressure(PASP)–Considerthistestonanypatientwho
becomesshortofbreathwithexerciseorwalkingupstepsthatresolveswithrest.Inquireiftherewasadiagnosisofasthma,coronaryarterydisease,labeledasoverweightandoutofshape”.Echocardiogramisdonetoevaluatepulmonaryarterysystolicpressure(tricuspidregurgitation),whichshouldnotrisemorethan8Hgduringexercise.ElevatedPASP,oftenfoundinCIRS,cancausepalpitationsanddyspneawhichdoesnotrespondtobeta2antagonists.(3)
• VO2max–consideriffatiguetakesdaystorecover.This“push-crash”syndromeiscausedfromcapillaryhypoperfusionandabnormalnuclearencodedmitochondrialgenes.LowVO2maxwillmostlikelyshowdecreasedabilitytoperformmaximumexerciseformorethanonetotwominutes.(32)
ShoemakerCertificationDianeParks,APRN-NPMay4,2020
14
21)MRIofthebrainwithoutcontrastwithNeuroQuantNeuroQuantisanadditiontoanMRItodeterminethevolumeof11regionsofthebrainandstratifiedtoage.ItwasdevelopedbyCorTechsLabsandclearedbytheFDAin2007.NeuroQuanthasbeenusedtoevaluateAlzheimer’s,epilepsy,traumaticbraininjuryandPTSD.Additionally,duetohighrateofneurocognitivedeficitsinCIRSpatients,studieshavedemonstratedbrainchangesandpatternsspecifictoCIRSusingNeuroQuant.(3)Thesepatternsinclude:CIRS-WBD(mold)
• Increasedforebrainparenchyma• Increasedcorticalgray• Decreasedcaudate
CIRS-PLS
• Increasedthalamus• Decreasedputamen
Dr.ShoemakerhasdevelopedonlinesoftwareanalysisasascoringsystemofNeuroQuant(GeneralMorphometryReport)specifictoareasofatrophy,asymmetryaswellasdeterminingmoldvsLyme.Thisreportisveryhelpfulindeterminingtreatmentstrategies.Thisonlineanalysiscanbefoundathttps://www.survivingmold.com/store1/online-neuroquant-test(16) Shoemaker12-stepProtocolforCIRS TheShoemakerprotocolinvolves12stepsdoneinspecificorderandbeginswiththemostimportantstep,removalofexposure.Ingeneticallysusceptibleindividuals,simplyremovingtheexposurewilloftennotbesufficienttocorrectotherassociatedmaladiessuchasimmunedysregulation,neuroendocrineandhormonalabnormalities,inflammation,brainatrophy,coagulationdisorders,allcontributorstothismulti-system,multi-symptomillness.Removalfromexposureisthefirstandmostimportantsteplayingthefoundationforfuturetreatmentsuccess.Indeterminingthesource,thepractitionermustfocusonadeliberate,painstaking,sometimesexpensiveprocesswhichrequiresextensiveknowledgeforallconditionsinthedifferentialdiagnosesthatmaycontributetotheillness.WhileWDBandPLSarefrontrunnersinCIRSillness,dinoflagellate(Pfiesteria),foodpoisoning,Ciguatera,Cyanobacteria,Babesiaandspiderbitepoisonhavetobeconsidered.Oncethesource(s)ofdiseaseareidentified,aggressivemeasuresmustbeimplementedtoremovethissourceofexposure.
ShoemakerCertificationDianeParks,APRN-NPMay4,2020
15
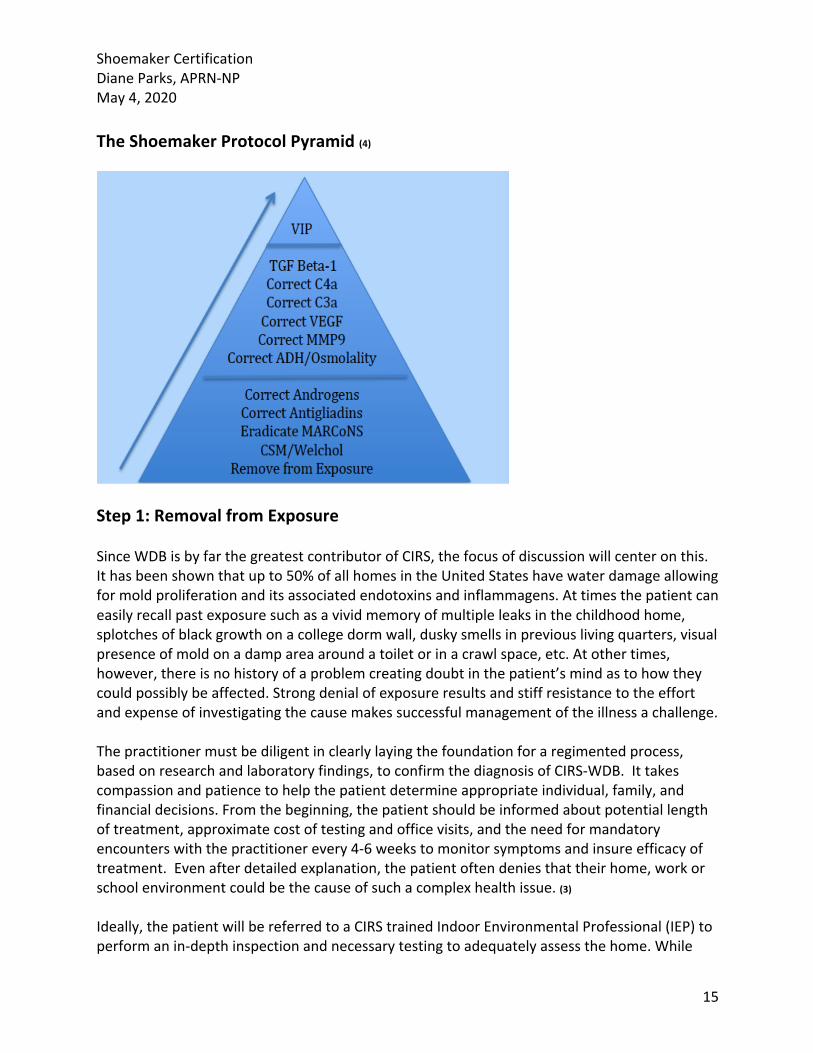
TheShoemakerProtocolPyramid(4)
Step1:RemovalfromExposureSinceWDBisbyfarthegreatestcontributorofCIRS,thefocusofdiscussionwillcenteronthis.Ithasbeenshownthatupto50%ofallhomesintheUnitedStateshavewaterdamageallowingformoldproliferationanditsassociatedendotoxinsandinflammagens.Attimesthepatientcaneasilyrecallpastexposuresuchasavividmemoryofmultipleleaksinthechildhoodhome,splotchesofblackgrowthonacollegedormwall,duskysmellsinpreviouslivingquarters,visualpresenceofmoldonadampareaaroundatoiletorinacrawlspace,etc.Atothertimes,however,thereisnohistoryofaproblemcreatingdoubtinthepatient’smindastohowtheycouldpossiblybeaffected.Strongdenialofexposureresultsandstiffresistancetotheeffortandexpenseofinvestigatingthecausemakessuccessfulmanagementoftheillnessachallenge.Thepractitionermustbediligentinclearlylayingthefoundationforaregimentedprocess,basedonresearchandlaboratoryfindings,toconfirmthediagnosisofCIRS-WDB.Ittakescompassionandpatiencetohelpthepatientdetermineappropriateindividual,family,andfinancialdecisions.Fromthebeginning,thepatientshouldbeinformedaboutpotentiallengthoftreatment,approximatecostoftestingandofficevisits,andtheneedformandatoryencounterswiththepractitionerevery4-6weekstomonitorsymptomsandinsureefficacyoftreatment.Evenafterdetailedexplanation,thepatientoftendeniesthattheirhome,workorschoolenvironmentcouldbethecauseofsuchacomplexhealthissue.(3)Ideally,thepatientwillbereferredtoaCIRStrainedIndoorEnvironmentalProfessional(IEP)toperformanin-depthinspectionandnecessarytestingtoadequatelyassessthehome.While
ShoemakerCertificationDianeParks,APRN-NPMay4,2020
16
maylocationsintheUSdonothaveavailabilityofIEPinspectors,manynowhaveremoteinspectionandtestingavailable,atremendousadvantageforthosewithlimitedresources.Butincaseswhenthisassessmentisnotpossible,thepatientcantesttheirhomeusingaMSQPCR(MoldSpecificQuantitativePolymeraseChainReaction)alsoknownasEnvironmentalRelativeMoldIndextest(ERMI)andHealthEffectsRosterofType-SpecificFormersofMycotoxinsandInflammagenstest(HERTSMI-2),bothofwhichofferpredictorsofwhetherabuildingissafefromsignificantharmfulmoldexposure.SurfaceratherthanairsamplesareobtainedbecausesurfacedustprovideshistoricaldataastotoxinconcentrationassociatedwithWDBandairsamplesonlygiveasnapshotofa10-15minutewindow.(4)ERMIandHERTSMI-2canbeobtainedthroughMycometricsatwww.mycometrics.com.ERMI,HERTMI-2,Actinomycetes,andEndotoxinscanallbeobtainedthroughEnvironmetricsatwww.environmetrics.com.Bothprovidedetailedinstructionforcollectionofsamples.TheguidelinesbelowforERMIshouldbefollowedifanindividualhasgeneticsusceptibility:
• WhentheERMIscoreis<2andtheMSH<35withaC4a<20,000,thepatientismostlikelyabletotoleratetheenvironment:however,iftheMSHscoreis<35andtheC4ais>20,000,thenanERMIof<1isrequired.(3,17)
AHERTSMI-2scorecanbederivedeitherindividuallyorcalculatedfromtheERMIreport.Ittestsforfivetoxicmoldspeciesassociatedwithindoorair:Aspergilluspenicilloides,Aspergillusversicolor,Chaetomiumglobosum,StachybotyrschartarumandWallemiasebi.
• AHERTSMI-2≤10isgenerallyconsidersafeforall,butthemostsensitivepatientsmayrequireascore≤8forittobeconsideredasafeenvironment.(3,17)
Oncethepresenceofelevatedtoxigenicmoldspecieshasbeenidentified,remediationbyahighlyskilledprofessionalwithaclearunderstandingoftheintricaciesofbiotoxinremediationshouldbeused.Afterremediation,thisshouldbefollowedbysmallparticlecleaningagainbyaskilledprofessional.Thisstepismostoftenomitted,acostlyerrorbecausecontinuedmoldexposurefrompre-remediateddustmaystillbepresent.Assumingremediationandpost-remediationsmallparticlecleaninghavebeensuccessful,arepeatHERTSMI-2willverifysafeentrywithascore≤10. Once this confirmation has been achieved, proceeding to Step2ispermissible. Step2:ReducingBiotoxinCarriagewithCholestyramine(CSM)orWelcholCSMisanon-absorbablemedicationusedtotreatelevatedcholesterolfirstapprovedbytheFDAin1973.IthasalsobeenusedofflabeltotreatsecretorydiarrheacausebyClostridiumdifficile.(4,18)In1997,Dr.ShoemakerdiscovereditsbenefitinmitigatingsymptomsassociatedwithaPfiesteriaoutbreakinMaryland.Itssuccessinalleviatingbiotoxin-relatedsymptomsinPfiesteriaexposureledtoofflabeluseinotherbiotoxinillnessesandthedevelopmentofthe
ShoemakerCertificationDianeParks,APRN-NPMay4,2020
17
Shoemakerprotocol.(4,19,20)BecauseCSMhasstrongtoxinbindingproperties,isnon-absorbableandeliminatedinthestool,itisanidealvehicleforremovalofthesebiotoxins.Itisthereforeconsideredafirstlinetherapy.SideeffectsaremostlyrelatedtoGIsymptomssuchasconstipation,nausea,reflux,andbloating.CSMcanbeprescribedthroughtraditionalpharmaciesreadilyavailableunderthetradename,QuestranorQuestranLight.Thelattercontainsaspartame,acomponentthatshouldnotbeusedinpatientswithahistoryofdepression,anxiety,orheightenedsensitivitiestochemicals,dyes,fillers,orsucrose.AnalternativemightbethecompoundedversionmixedwithStevia.(4,18,21)
CSMisprescribedfourtimesadaywithtimingtoavoidbindingnutrientsinfood,vitamins,orothermedications.Itisrecommendedtobeginatalowdose,slowlytitratingtofulldosingastolerated.Attimes,onemightexperiencean“intensificationreaction”,sometimesconfusedwiththeJarisch-Herxheimerreactiontoantibiotics.TheintensityofthereactioncanbemanagedbypreloadingwithhighdoseOmega3FattyAcids(EPA2.4gandDHA1.8g/day)aweekortwopriortothefirstdoseofCSM.Inaddition,alowamylosedietisrecommended.(Appendix4)WhenCSMisnottolerated,Welchol,takenwithmeals,maybeasatisfactoryalternative.Unfortunately,ithasonly25%bindingcapacityascomparedtoCSM.Ahybridtherapyhasalsobeenproposed:CSMtakenpriortobreakfastandatbedtimeandWelcholtakenwithlunchanddinner. DosingandtimingofMedication(Appendix5)1) CholestyraminedosingAdults:>120lbsor>18Questran:9grams(1scoop)mixedin6ozofwateruptofourtimesdaily,followingguidelinesAppendix5.CompoundingCholestyramine(CSM):4gramsmixedwith6ozwateruptofourtimesdaily,followingguidelinesinTable6Pediatrics:<120or<18QuestranorCompoundedCSM:60mg/kg/dosemixedwith6ozofwater,uptothreetimesdaily,followingguidelinesAppendix5.2) WelcholdosingAdults:Welchol625mg:Take2tabletsupto3timesdailywithmealsPediatrics:Welchol625mg:Take1tabletupto3timesdailywithmeals
ShoemakerCertificationDianeParks,APRN-NPMay4,2020
18
Guidelinesoncetreatmentbegins:
• RepeatVCStestevery30daysafterstartingCSM• ConsiderGENIEtestingpriortoinitiatingCSMandthenatleastevery6months• Baselinelabshavealreadybeenobtainedandarerepeatedwitheachstepofthe
protocoloratthediscretionofpractitioner:TGF-beta1,MMP-9,VEGF,MSH,ADH/osmolalityandACTH/Cortisol,Testosterone,DHEA-s,Leptin
• OnceVCStesthasbeenpassedandconfirmationisobtainedthathome/school/workisfreefromexposure,discontinueCSMandbeginmaintenancedoseofWelchol625mg1tablettwicedaily
• Shouldre-exposureoccur,havethepatienttakeaVCStest,increaseWelchol625mg2tabletsthreetimesperdaywithmealsorpreferablyCSM4gthreetofourtimesperdayorastoleratedperguidelinesandcontinueforaminimumof3daystodecreasebiotoxinburdenandinflammation
• Treatmentfailureoccursfromcontinuedornewexposure,poorcomplianceorfailuretoeradicateMARCoNS.(3)
Step3:EradicateMARCoNS IfMARCoNStestingispositive,begintreatment30daysafterinitiationofCSM/WelcholwiththecompoundedmedicationEDTA.MARCoNScanberesistanttotreatment,sometimesrequiringuptooneyear.Dr.Shoemakerreportsthesurgeofoveruseofantifungalmedicationshascausedincreasedresistancetomultipleantibioticsmakingeradicationmoredifficult.Typically,CIRSimprovementwillnotoccuruntilMARCoNSiseradicated.(22)MedicationAdults:EDTA0.2%-Instill2sprayseachnostrilthreetimesdaily.BlownosefirstPediatrics:EDTA0.2%-Instill1sprayalternatenostrilthreetimesdaily–RarelyneededGuidelinesoncetreatmentbegins:
• Initialtreatmentmaycausethepatienttofeelworsedueto“dieoff”,butwhenstartingatalowdoseandslowlytitratingup,inconjunctionwithalowamylosedietandhighdoseOmega3FattyAcids,theincidenceofthisshoulddecline.
• If“dieoff”symptomspersist,considerre-exposureandcheckaVCStest.RowDandEwillfallandMMP-9willincrease.
• Retestafter1month,butrarelyisMARCoNSeradicatedsoquickly.Ifpositive,continuetreatingfor2additionalmonthsandthenretest.Mayneed6-12monthsoftreatment.(2)
• GENIEcanbeaninvaluabletooltoguidelengthoftreatmentastwoweeksofEDTAhasbeenshowntoimproveribosomalsuppression.(23,24)VIPcanbeinitiatedafter2weeksonEDTAnasalspray.
ShoemakerCertificationDianeParks,APRN-NPMay4,2020
19
Step4:EliminateGluteninAGAPositivePatients AGAisnotceliacdisease,butdoesindicateaninflammatoryresponsetogluten.Ifpositive,initiateastrictglutenfreedietfor3months.ThiswillreduceGIinflammation.Guidelinesoncetreatmentbegins:
• IfanoamylosedietwasinitiatedduringthefirststepofCIRStreatment,continueforanadditional3months.
• After3months,retestAGAandifnegative,slowlyreinitiateglutenandmonitorforsymptoms
• Ifsymptomsreturnorapatientfeelsbetteroffgluten,removeforlife.(2) Step5:CorrectAndrogens:Testosterone/DHEA-s Androgens(TestosteroneandDHEA)maybecomeabnormalduetoupregulationinaromataseenzyme.Inflammationcausesmorerapidconversionoftestosteroneintoestrogenresultinginhighestrogenandlowtestosterone.Itiscontraindicatedtotreatwithtestosteroneinthesepatients.Instead,treatingwithDHEAwillslowlyincreasetestosteroneaswellasDHEA,withlessriskofincreasingestradiol,estrone,hematocritandhemoglobinasoftenseenintestosteronetherapy.(12)MedicationAdults:Men–DHEA25-75mgdaily,Women5-25mgdailyPediatrics:NotindicatedGuidelinesoncetreatmentbegins:
• Obtainpre-treatmentDHEA-s,TotalandFreeTestosterone,Estradiol,Estrone,CBC,CMPandatleastevery2-3months
• DonotusearomataseinhibitorswithaaMSH<35,asthiscouldcausedeterioration• DHEAcanbereducedordiscontinuedonceDHEA-sandTestosteronelevelsnormalize
Step6:CorrectADH/Osmolality ADH/Osmolalitydysregulationoccursin80%ofCIRSpatient’scontributingtosymptomsoffrequenturination,dehydration,excessivethirst,headaches.Excessivesaltontheskinactsasaconduitforelectricitycontributingtostaticshocks.DesmopressinAcetate(DDAVP)isanexogenousreplacementforADHandisstartedwhenosmolalityishigh>295.(2)
ShoemakerCertificationDianeParks,APRN-NPMay4,2020
20
MedicationAdults:Initiallyone0.2mgtableteveryothernightfor10nights.Monitorcarefullyforsideeffects,specificallyweightgainandedema.(2,4,26)Pediatrics:1-4sprayspernightbasedonweightandageGuidelinesoncetreatmentbegins:
• After5dosescheckADH,osmolality,electrolytestoensurenormalsodiumandpotassium
• Ifon“offdays”symptomspersist,considerDDVAP0.2mgdailyandcheckelectrolytesADHandosmolalityafter10days.
• MedicationtaperisrequiredonceADH/Osmolalityhavenormalized• ForpatientswithPOTS,dailyDDVAPmaybebeneficialonalong-termbasis,takingcare
toregularlymonitorelectrolytes,ADHandosmolality• MaycorrectacquiredvonWillebrand’ssyndromeandreduceMMP-9.Patient’sneedto
carryDDAVPtostophemorrhage.• DDVAPisofflabeluseforthispurpose(2)
Step7:CorrectionofMMP-9 Aspreviouslymentioned,elevatedMMP-9isoftencorrectedwithhighdoseOmega3FattyAcids–EPA2.4gandDHA1.8gdaily,whichmayhavebeeninitiatedpriortostartingCSM/Welcholtopreventintensificationreaction.Actos45mgdailyisrarelyusedincurrenttreatmentprotocolsduetoblackboxwarningforbladdercancer. Step8:CorrectionofVEGF VEGFisagrowthfactorwhichinhealthypeopledilatesbloodvesselsinresponsetohypoxiainduciblefactor(HIF).Hypoxiaoccurswheninflammatorycytokinesboundtotheendotheliumreleasechemicalsnarrowingthecapillaries.Hypoxiacausessymptomsofdecreasedmuscleendurance,poorendurance,fatigueandcognitivedecline.OftenSteps1-7willhavecorrectedVEGF,butexercisecanbeaddedtooptimizelevels.VEGFissecretedinresponsetoexercise;however,thisisadouble-edgedswordasmanypatientsarenoncompliantwithexerciserecommendationsduetosignificantlossofenduranceexperiencedduringexercise.Startwithhighintensityexerciselastingfromsecondstoseveralminutesandwithtimetransitioningtoanerobicconditioningforoptimalresponse.(26)ConsistencyiskeytoprovideongoingsignalingforthebodytoproduceVEGF.OnceVEGFhasnormalized,treatcapillaryhypoperfusion,lowV02andpostexercisemalaise.Dr.Shoemakerrecommendsgradedexercisestartedinthefollowingway:
ShoemakerCertificationDianeParks,APRN-NPMay4,2020
21
• Startwithcardioexercisesfor5mindailyworkingupto15minutesdaily• Thenaddfloorexercises5minutesdailyworkingupto15minutesdaily• Thenaddfreeweights5minutesdailyworkingupto15minutesdaily• Afteronemonth,gobacktoeachexerciseandaddintensity(27)
Step9:CorrectionofC3a C3aisananaphylatoxinwhichstimulateshistaminereleasefrommastcells,causescontractionofsmoothmuscle,capillaryhypoperfusionandincreasedvascularpermeability.ThepresenceofbacterialmembraneselevatesC3aandanexampleofactivationofC3awouldbeactiveLymedisease.(4)MedicationAdults:HighdoseStatins80mgdailytoreduceC3a.(26)Guidelinesoncetreatmentbegins:
• Obtainpre-treatmentliverenzymesandmonthlywhileontreatment• StatinslowerCoQ10soadd100-150mgdailywhileontreatment
Step10:CorrectionofC4a ThismarkerisofgreatsignificancetoCIRS-WDBandwillalsobeelevatedwithexposuretodinoflagellates,cyanobacteriaandpersistentLymedisease.Additionally,increasedC4acanplayaroleinchangesofsixexecutivefunctions:decreasedconcentration,difficultywithwordfinding,decreasedassimilationofnewknowledge,confusionanddisorientation.ItpotentiallyalsoplaysaroleinAlzheimer’sdiseaseandwithadecreaseinC4acognitivesymptomscanimprove.(3)MedicationAdults:VIPNasalspray50mcg/ml–4spraysdaily(26)Guidelinesoncetreatmentbegins:
• Rarelyneedtotreatif<5000,butif>10,000willcauseadverseeffects(25)• Obtainpre-treatmentC4a,liverenzymes,lipase,amylaseandmonthlywhileon
treatment• Thistestisnotonlyusedforassessmentofcurrentexposurebutalsore-exposureas
wellasanincreaseinC4acanoccurwithin10minutesofexposure• Procritwaspreviouslyusedbutnolongerrecommendedduetoblackboxwarningfor
riskofbloodclotting(3)
ShoemakerCertificationDianeParks,APRN-NPMay4,2020
22
Step11:ReductionofTGFbeta-1TGFbeta-1isaveryimportantproteinplayinganimportantroleintheregulatorypropertiesoftheimmunesystemespeciallywithregardtotissuerepairandfibrosis.MedicationAdults:Losartan1-2timesdailyfor30days(26)ForpatientwithlowbloodpressureorunabletotolerateLosartan,useVIP50mcg/mlintranasally4spaysdaily(3)Pediatrics:Losartan0.6/0.7mg/kg/dayindivideddosestwicedailyGuidelinesoncetreatmentbegins:
• Monitorbloodpressuretwicedailyduringfirstmonthoftreatment• Obtainpre-treatmentlipase,GGTP,TGFbeta-1andthenmonthlywhileontreatment
Step12:VIP(VasoactiveIntestinalPolypeptide)
Thisfinalstepiswithoutadoubtthemostimpressiveandbeneficialforthosewithsustainedorsevereillness.ExogenousVIPgivenintranasallycanreverseSOBwithexercise,downregulatingcytokines(decreaseinflammation),normalizeTGFbeta-1,androgendeficiency,improvecognition,correctproteomics,transcriptomicsandimprovegreymatternuclearatrophyinCIRS.(7)
Adults:FullstrengthVIP500mcg/ml–Instill1spray(50mcg)intransallyfourtimesdaily–alternatingnostrilswitheachapplication.Higherdoseshavebeenuseddependingonseverityofsymptomsandatrophy.Pediatrics:VIPhasnotbeenwellestablishedinpediatricpatientsGuidelinesbeforeinitiatingVIP:(2,3,23,28,29)
• Thoroughlyeducatepatientandfamilyregardingrisks,benefits,alternative,sideeffects,importanceoffollowingprotocolandconsiderwrittenconsent.
• Proofoflackofexposuretobiotoxins(ERMI<2orHERTSMI-2≤10.• MustpassVCStest.• NegativeMARCoNS–thisisoftenverydifficulttoachieveduetopersistentnatureof
MARCoNS;however,withtheincreaseduseofGENIE,thereissomeindicationthatthegenesassociatedwithMARCoNSaredownregulatedwithintwoweeks.Inthefuture,thismaybecomepartoftheVIPprotocolasmoredataisobtained.
• Normallipase,GGTP

ShoemakerCertificationDianeParks,APRN-NPMay4,2020
23
• Considerobtainingastressechocardiogramtoevaluatepulmonaryarterysystolic
pressure(tricuspidregurgitation),whichshouldnotrisemorethan8Hgduringexercise.ElevatedPASPoftenfoundinCIRScancausepalpitationsanddyspneawhichdoesnotrespondtobeta2antagonists.(3)
• OfficevisitforPre-VIPVitalSignsandphysicalexam:(BP,pulse),examinationofskinandabdomen.Havepatientinstill1sprayinonenostril.ThencheckVSQ5minutesX3andassessforoccurrenceofrashes.Askpatientifbreathingorjointpainhasimprovedorifthereisthepresenceofabdominalpain.
• IdeallyTGFbeta-1andC4awouldbedoneatbaselineandagain15-minutespostVIP.Ifatwo-foldincrease,considercontinuedexposure.Thisisdifficultforpracticeswithoutlabfacilities.(2)
Guidelinesoncetreatmentbegins:
• Monthlylipase,GGTPandabdominalexam.VIPmustbediscontinuedwithelevatedlipase,considergallbladderdiseaseand/orpancreatitis,orwithabdominalpainorrash.
• VIPdurationrangesfrom6monthsto18months.• Regularlyassesssymptomimprovement,CIRSbiomarkers,VCStest,cognition,and
whennormalconsidertaperingdownto2spraysdailyfor30days,followedby1spraydailyfor30days,andthendiscontinue.(3)
• RepeatNeuroQuantMRIafter9-12monthsofVIP.VIPhasbeenshowntocorrectCIRS-WDBandimproveorreverseCIRS-WDBrelatedatrophynotedonNeuroQuantMRI.(30)
• Followupat6-monthspostVIPtoensurestability,VCSandlabsremainnormal(3) Re-exposureinstructions ItisalmostinevitableaCIRSpatientwillexperiencere-exposureanditisimperativethataplanisinplacetoquicklymitigatedamagetopreventfullblownCIRSrelapse.ThefollowingareguidelinesforSequentialActivationofInnateImmuneElements–SAIIE)
• TreatwithCSMorWelcholtore-establishcontrollabvalues• Patientmuststayinasafeenvironmentandstopallbiotoxinmedication• After3days,measureVCS,C4a,Leptin,MMP-9,TGFbeta-1,VEGF,FactorVIIi• Patientcontinuestostayoffallbiotoxinmeds• Re-exposepatienttotheproblematicbuildingfor8hours• Retestlabsthemorningafter,thenre-exposepatienttothebuildingforanother8hours• Retestlabsthemorningafterandhavepatientstayinthebuildingforanother8hours
(3rdexposuretoproblematicbuilding)• Retestlabsforthe3rdtimesincebaseline• Afterlabs,restartCSMorWelcholifpatientisexperiencingsymptomsofCIRS(3,18)

ShoemakerCertificationDianeParks,APRN-NPMay4,2020
24
Predictivelabchangeswithre-exposure
• C4aincreasesin4hours• Leptinincreasesonday2• MMP-9increasedonday2-3• VEGFincreasesonday1andcrashesday3(6)
Summary Itdoesnotmatterifyourareaofexpertiseisprimarycare,pediatrics,OB/GYN,pulmonology,rheumatologyorendocrinology,apatientexperiencingCIRSwillpresentonaregularbasis.Thesearethemostcomplicated,oftentimesmisunderstoodpatientswhosequalityoflifehasbeenseverelyimpactedbythislittlerecognized,butverydramaticillness.ManyCIRSpatientshaveseen10-15ormorepractitioners,oftengivendiagnosisofchronicfatigue,fibromyalgia,anxiety,depression,bipolardisorderandOCD.Theymayhavespenthundreds,ifnotthousandsofdollarsontheirhealthcarewithoutbenefit.Asapractitioner,becomingproficientinthemanagementofCIRSillness,hasbeenaprofessionalgamechangerandanintellectualchallengelikenootheraspectofmyeducationendeavors.Itistrulyimpossibletoturnablindeyetoanillnessthatoncelearned,smacksyouinthefaceonaregularbasis.Thispatientpopulationisintellectuallyandemotionallychallenging;yettherewardsaregreat.Itishelpfultokeepinmindthatdespitegreateffortsonthepartoftheprovider,notallpatientshavethewill,sheerdeterminationorfinancialmeanstodotheworkittakestogetbetter.IstandinamazementeachandeverydaythatasafamilydocinruralMarylandtreatingastrangeandunforgivingillness,Dr.Shoemakerextrapolatedthisexperienceintoaresearchdriven,self-made“university”mentoringandeducatinghundredsofmedicalpractitionersandprofessionalsthroughouttheworld,andindoingso,savingthousandsoflives.Theprofessionalswhohavesurroundedhimaredetermined,smart,anddedicatedtospreadinginformationaboutCIRS.Thankyou,Dr.Shoemaker.TheamountofresearchandstudythatgoesintothejourneytowardscertificationintheShoemakerprotocolisintense.NotonlydidIrelyonvastresearcharticles,booksandslidepresentations,butthecertificationpapersofotherpractitionersobtainingcertificationwereinvaluabletoorganizingtheprotocolinasuccinctandstraight-forwardmanner.IwouldliketoacknowledgetheexcellentworkbyDrs.Thomas,Smith,Hoffman,Berry,Lawsonandadvancednursepractitioner’sBeshara,Meinhardt.Thankyou!Also,abigthankyoutoDebWaidnerforalways“beingthere”toanswermillionsofquestions,offerencouragementandmotivation.Sheiscounselorextraordinaire,extremelydedicatedandalotoffun!Thankyou,Deb!Finally,mysincerethankstomyphysicianhusbandwhoisintriguedbyCIRSandhaslearnedsomuchasheexpertlyeditedthispapertomakeit“presentable”toothers!
ShoemakerCertificationDianeParks,APRN-NPMay4,2020
25
For all those CIRS professionals, I love this quote: “Those who danced were thought to be quite insane by those who could not hear the music” (Angela Monet). CIRS is the dance and we are the dancers.
ShoemakerCertificationDianeParks,APRN-NPMay4,2020
26
Resources 1. ShoemakerRC,HouseD,RyanJ,VasoactiveIntestinalpolypeptide(VIP)correctschronic
inflammatoryresponsesyndrome(CIRS)acquiredfollowingexposuretowater-damagedbuildings.Health,2013;5(3);396-401
2. HoffmanMD,Bruce-ChronicInflammatoryResponseSyndrome(CIRS)Evaluationand
Treatment(CertificationPaper)3. SmithNMD,Jennifer–ChronicInflammatoryResponseSyndrome:DiagnosisandTreatment
(CertificationPaper)4. ShoemakerRC-ProficiencyPartnersLectureslidepresentation1/2019,Module25. TheBiotoxinPathway,www.survivingmold.com6. SAIIE:AHealthIndexforPeopleRe-exposedtoWaterDamagedBuildings,IAQA10/14/077. ShoemakerRC,etal(2018).DiagnosticProcessforChronicInflammatoryResponse
Syndrome(CIRS):AconsensusStatementReportfotheConsensuscommitteeofSurvivingMold.InternalMedicineReview,4(5),1-47.
8. ShoemakerMD,Ritchie.SurvivingMoldFAQVolume1,29.9. ThomasMD,Natasha–UnderstandingChronicInflammatoryResponseSyndrome(CIRS:
Definition,Diagnosis,andTreatment(CertificationPaper)10. ShoemakerRC.SurvivingMold:LifeintheEraofDangerousBuildings,Appendix2:Rosetta
Stone.11. BesharaMS,APRN,Mary.CIRS–ChronicInflammatoryResponseSyndrome:The
ShoemakerProtocol(CertificationPaper)12. InternationalSocietyfortheStudyofWomen’sSexualHealth(ISSWSH)–AnnualMeeting,
Hormonaldysregulationslides,February201913. QuestDiagnosticswebsite(https://testdirectory.questdiagnostics.com/test/test-
detail/37740/copeptin?p=r&q=37740&cc=)14. SurvivingmoldListserveemailthreadMarch4-5,2020
ShoemakerCertificationDianeParks,APRN-NPMay4,2020
27
15. ShoemakerRC.Transcriptomics:TheFinalFrontierforChronicFatiguingIllnesses.www.survivingmold.com
16. ShoemakerRC,HouseD,RyanJC.Structuralbrainabnormalitiesinpatientswith
inflammatoryillnessacquiredfollowingexposuretowater-damagedbuildings:avolumetricMRIstudyusingNeuroQuant.NeurotoxicologyandTeratology.2014Sept-Oct;45:15-26.
17. Shoemaker,R(2014).StateoftheArtAnswersto500MoldQuestions.Cork:BookBaby.18. Berry,Y.(April3,2014).Physicians’guidetounderstandingandtreatingbiotoxinillness;
BasedontheworkofRitchieShoemaker,MD.http://www.survivingmold.com19. BerndtsonK,McMahonS.,AckerleyM,RapaportS,GuptaS,ShoemakerRC.(2015).
Medicallysoundinvestigationandremediationofwater-damagedbuildingsincasesofCIRS-WDB:ConsensusStatementPart1.CenterforResearchonBiotoxinAssociatedIllness.Pocomoke,MD.
20. Shoemaker,RC.(2001).Desperationmedicine:theinsidestoryofhowanAmericandoctor
discoveredathreateninganewfamilyof“environmentaldiseases”–andhowtostopthem.Baltimore,MD;GatewayPress
21. Shoemaker,R.C.(2014,December).WhatisCIRS,labTestingandtreatmentprotocol.
Retrievedfromhttp://www.survivingmold.com22.ShoemakerRC-ProficiencyPartnersLectureslidepresentation1/2019,Module12-1322. Meinhardt,J.BACKTOBASICS:ChronicInflammatoryResponseSyndrome,CIRSmeeting
January2019.23. Musto,J.,Hrabec,G.,Moin,E.,Katz,D.(2017,November6).ReportoftheEffectivenessof Colloidal Silver in Treating Multiple Antibiotic Resistant Coagulase Negative Staphylococcus (MARCoNS), Other Gram Positive and gram Negative Bacteria, Yeast and Mold in Nares culture. Bedform: Micobiology DX. 25.ShoemakerRC-ProficiencyPartnersLectureslidepresentation1/2019,Module526.LawsonDO,Lynese.TheDiagnosisandTreatmentofChronicInflammatoryResponseSyndrome“CIRS”:CausedbytheEnvironment;FrequentlyOverlookedandMisunderstood.(CertificationPaper)27.ShoemakerRC-ProficiencyPartnersLectureslidepresentation1/2019,Module19

ShoemakerCertificationDianeParks,APRN-NPMay4,2020
28
28.Shoemaker,R.,Katz,D.,Ackerley,M.,Rapaport,S.,McMahon,S.,Berndtson,K.,Ryan,J.(2017).IntranasalVIPsafelyrestoresvolumeotmultiplegreymatternucleiinpatientswithCIRS.InternalMedicineReview,3(4).Doi:10.18103/imr.v3i4.41229.ShoemakerMD,Ritchie.12/01/2010-Slidepresentation:Theacademicbasisoftreatmentofbiotoxinillnesses:ObjectivePhysiologicMeasuresCharacterizeTreatableDiseaseMeetVIP–Finally,aprovenanswer.CenterforResearchonBiotoxinAssociatedIllnesses,Pocomoke,MDBoston,Massachusetts30.ShoemakerRC.,&HouseDE.(2006).Sickbuildingsyndrome(SBS)andexposuretowater-damagedbuildings;Timeseriesstudy,clinicaltrialandmechanisms.NeurotoxicologyandTeratology,28(5),573-588.31.Ryan,J.,Shoemaker,R.(2016).RNA-Seqonpatientswithchronicinflammatoryresponsesyndrome(CIRS)treatedwithvasoactiveintestinalpeptide(VIP)showsashiftinmetabolicstateandinnateimmunefunctionsthatcoincidewithhealing.MedicalResearchArchives,4(7).32.ShoemakerRC-ProficiencyPartnersLectureslidepresentation1/2019,Module16,17
ShoemakerCertificationDianeParks,APRN-NPMay4,2020
29
AppendicesAppendix1:ToxicStewofaWaterDamagedBuilding(Toxins,Inflammagens,Microbes) Fungi Aspergilluspenicillodies,Asperigillusversicolor,Wallemiasebi,
Stachybotyrschartarum,ChaetomiumglobosumBacteria Mycotoxins,hyphalfragments,conidia,mannans,spirocyclicdrimanes,
ChitinasesBacteriafragments
Endotoxins,Lipopolysaccharides,Actinomycetes,Nocardia,Hemolysins
Protozoa ProtozoaandamoebasInflammagens Siderophores,Betaglucans,Cellwallcomponent,cellfragments,
proteinasesVOCs MicrobialVOC’s,buildingmaterialVOC’s,InorganicxenobioticsParticulates Bioaerosols,Courseparticulates,Fineparticulates,Ultrafineparticulates,
Mano-sizedparticulates

ShoemakerCertificationDianeParks,APRN-NPMay4,2020
30
Appendix2:ClusterofSymptoms(YesorNo)–Highestscore13 DiarrheaAbdominalpainNumbness
ImpairedmemoryDifficultywithwordfinding
DisorientationMetallictasteWateryeyes
UnusualskinsensitivityTinglingTremorsUnusualpain
CongestedsinusesShortnessofbreath
BlurredvisionNightsweatsMoodswingsIce-pickpainRedorbloodshoteyes
MuscleweaknessBodyachesHeadacheSensitivitytolightTroublelearningnewinfo
ExcessivethirstConfusionCough
VertigoStaticshocks
JointpainMorningStiffnessMusclecramps
TroubleregulatingbodytemperatureIncreasedurinaryfrequencyAppetiteswings
Troubleconcentrating
Persistentfatigue Score:/Date:

ShoemakerCertificationDianeParks,APRN-NPMay4,2020
31
Appendix3:RosettaStone(AppendixofSurvivingMold)
DRB1 DQ DRB3 DRB4 DRB5
Multisusceptible 4 3 53 11/12 3 52B 14 5 52B Moldsusceptible 7 2/3 53 13 6 52A,B,C 17 2 52A 18* 4 52A Borrelia,PostLymeSyndrome 15 6 51 16 5 51Dinoflagellates 4 7/8 53 MARCoNS–MultiAntibioticResistantCoagulaseNegativeStaphAureus
11 7 52B
Norecognizedsignificance 8 3,4,6 LowriskMold 7 9 53 12 7 52B 9 9 53
ShoemakerCertificationDianeParks,APRN-NPMay4,2020
32
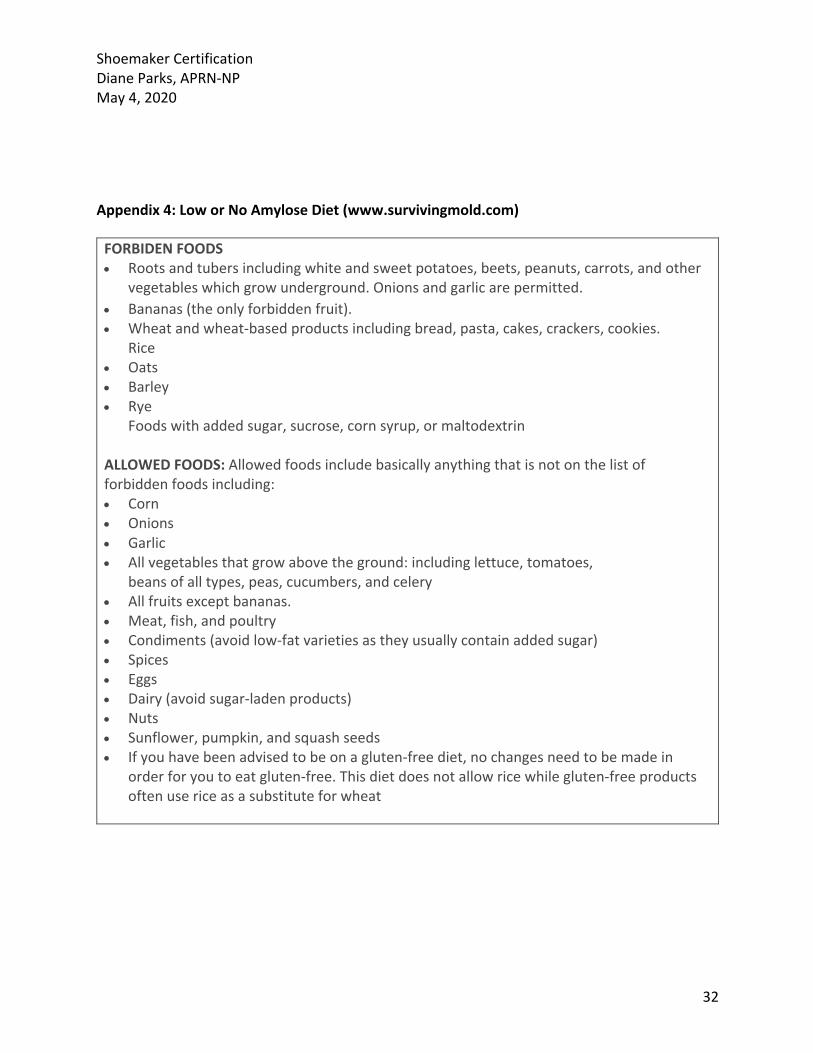
Appendix4:LoworNoAmyloseDiet(www.survivingmold.com) FORBIDENFOODS• Rootsandtubersincludingwhiteandsweetpotatoes,beets,peanuts,carrots,andother
vegetableswhichgrowunderground.Onionsandgarlicarepermitted.• Bananas(theonlyforbiddenfruit).• Wheatandwheat-basedproductsincludingbread,pasta,cakes,crackers,cookies.
Rice• Oats• Barley• Rye
Foodswithaddedsugar,sucrose,cornsyrup,ormaltodextrin
ALLOWEDFOODS:Allowedfoodsincludebasicallyanythingthatisnotonthelistofforbiddenfoodsincluding:• Corn• Onions• Garlic• Allvegetablesthatgrowabovetheground:includinglettuce,tomatoes,
beansofalltypes,peas,cucumbers,andcelery• Allfruitsexceptbananas.• Meat,fish,andpoultry• Condiments(avoidlow-fatvarietiesastheyusuallycontainaddedsugar)• Spices• Eggs• Dairy(avoidsugar-ladenproducts)• Nuts• Sunflower,pumpkin,andsquashseeds• Ifyouhavebeenadvisedtobeonagluten-freediet,nochangesneedtobemadein
orderforyoutoeatgluten-free.Thisdietdoesnotallowricewhilegluten-freeproductsoftenusericeasasubstituteforwheat

ShoemakerCertificationDianeParks,APRN-NPMay4,2020
33
Appendix5:Cholestyramine(CSM)Protocol(www.survivingmold.com) Cholestyramine(CSM)Protocol1. Onanemptystomach,take4gmsofCSMmixedwith4-6oz.water,orjuice.2. Stirwellandswallow.Addmoreliquid,ifnecessary,toconsumefullamountof
powder3. Drinkanextra4-6ozofliquid.4. After30minutes,youmayeatortakemeds(waitatleast2hoursbeforetaking
thyroxine,digitalis,theophylline,Coumadinandothers;askyourdoctorforinformation).
5. TakeCSM4timesaday!6. Ifyoueatfirst,waitatleast60minutesbeforetakingyournextCSM.7. Reflux,constipation,bloatingandboweldistressarenotunusual.8. Useacidblockingmedicationsifneeded.Talktoyourdoctorabout
this.9. UseMiralaxtorelieveconstipation
Recommended

















