-
Colon Cancer: State of the Art
Heinz-Josef Lenz
Professor of Medicine and Preventive Medicine
Associate Director, Clinical Research
J Terrence Lanni Chair in Cancer Research
Co-Director, USC Center for Molecular Pathways and Drug
Discovery
USC/Norris Comprehensive Cancer Center
Los Angeles, California
-
HEINZ-JOSEF LENZ COLORECTAL CANCER: STATE OF THE ART
ADVISORY BOARDS: BAYER, BOEHRINGER-INGELHEIM, MERCKSERONO,
ROCHE, GENENTECH, BMS
CLINICAL TRIAL SUPPORT: ROCHE, BAYER, TAIHO, DAICHI, INCYTE,
BOEHRINGER-INGELHEIM, BMS, PFIZER,
MERCK, MERCKSERONO, SWOG, NCI, NIH
THE SPEAKER WILL DIRECTLY DISCLOSURE THE USE OF PRODUCTS FOR
WHICH ARE NOT LABELED (E.G., OFF LABEL USE) OR IF THE
PRODUCT IS STILL INVESTIGATIONAL.
14th Annual California Cancer Conference Consortium
August 10-12, 2018
-
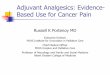
The Colorectal Cancer Subtyping Consortium
(CRCSC) identifies a network of molecular subtypes
Dienstmann R, et al. ASCO 2014 (Abstract No. 3511)
Group A
Group B
Group C
Group D
Group E
Group F
Subtype 1.3
D
E CCS3
Subtype 1.1
C4 Stem-like
C_score
CMS4
C2
C
Inflammatory
CCS2 A_score
Subtype 1.2 CMS1
Subtype 2.1
C3
Goblet-like
A
CMS3
CMS2
CCS1
Enterocyte
B_score
B
C5
TA
C1
Subtype 2.2
-
Presented by: Heinz Josef Lenz
0 12 24 36 48 60 72
Months From Randomization
0.00
0.25
0.50
0.75
1.00P
ro
po
rtio
n W
ith
ou
t E
ve
nt
0 12 24 36 48 60 72
Months From Randomization
0.00
0.25
0.50
0.75
1.00P
ro
po
rtio
n W
ith
ou
t E
ve
nt
Logrank P-value:
-
Presented by: Heinz Josef Lenz
0 12 24 36 48 60 72
Months From Randomization
0.00
0.25
0.50
0.75
1.00P
ro
po
rtio
n W
ith
ou
t E
ve
nt
0 12 24 36 48 60 72
Months From Randomization
0.00
0.25
0.50
0.75
1.00P
ro
po
rtio
n W
ith
ou
t E
ve
nt
Logrank P-value: 0.0290
11.7 (10.9-18.0)49/55Cetuximab
22.5 (15.9-32.6)36/49Bevacizumab
Median (95% CI)Events/TotalArm
OS – CMS1 Patients by Arm
-
Presented by: Heinz Josef Lenz
0 12 24 36 48 60 72
Months From Randomization
0.00
0.25
0.50
0.75
1.00P
ro
po
rtio
n W
ith
ou
t E
ve
nt
0 12 24 36 48 60 72
Months From Randomization
0.00
0.25
0.50
0.75
1.00P
ro
po
rtio
n W
ith
ou
t E
ve
nt
Logrank P-value: 0.0484
42.0 (39.3-54.4)79/119Cetuximab
36.0 (33.5-42.3)94/123Bevacizumab
Median (95% CI)Events/TotalArm
OS – CMS2 Patients by Arm
-
● Ding et al., Nature 2010
● Mutations present in 5–90% of
sequencing reads from one tumor
● Navin et al., Nature 2011
● Independent subclones coexisting
in a single anatomic site in breast
● Gerlinger et al., NEJM 2012
● Two-thirds of mutations in single
biopsies were not uniformly
detectable throughout all sampled
regions
● Both sensitive and resistant RNA
expression patterns
Heterogeneity also exists within
individual tumors
-
Intra-tumor copy number heterogeneity in CRC at the single gland
level
C. Curtis & colleagues
-
Liquid Biopsies
Circulating
Tumor
Cells (CTC)
http://www.inostics.com/
Tumor specific change (e.g. Mutation)
Tumor
Tumor cell
release DNA and RNA Circulating
tumor DNA
Normal DNA
CTC
Blood Vessel
Circulating
tumor RNA
-
MGH GI Cancer Center Liquid Biopsy Program
Routine liquid biopsy
assessment can effectively
identify mechanisms of
resistance across different
tumor types and treatments
Mechanism of resistance identified in 80%
36% with multiple resistance mechanisms
(range 2-12; median 3)
In patients with matched tumor biopsies, ctDNA
identified additional resistance mechanisms in 64%
RAS WT CRC (n=21)
54%
BRAF mCRC (n=5) 13%
FGFR2 biliary (n=8) 21%
FGFR2 gastric (n=1)
2%
MET amp gastric (n=2)
5%
HER2 amp CRC (n=2)
5%
N=39
no mechanism identified (n=8)
21%
multiple mechansims identified (n=14)
36%
single mechanism identifed (n=17)
43%
-
EGFR antibodies in RAS-WT CRC
Anti-EGFR antibodies
RAS
CRAF
ARAF
BRAF
ERK
MEK
PROLIFERATION AND SURVIVAL
KRAS
NRAS
HRAS
EGFR RTK
• 10 distinct resistance alterations
identified across 21 patients
• KRAS mutations
• KRAS amplification
• EGFR ECD mutations
• MET amplification
• ERBB2 amplification
• Novel MEK1 mutation
• Some patients with 5 or more
alterations present in ctDNA
-
A Bertotti et al. Nature 000, 1-5 (2015)
doi:10.1038/nature14969
Therapeutic intervention in preclinical trials to
overcomeresistance to anti-EGFR antibody
blockade.
-
Interesting Findings
14
1. In a small series of 10 patients who all had mt ras in
tissue
and liquid biopsy treated with bev based chemotherapy.
5/10 changed to wt Ras under chemotherapy ) Gazzaniga
et al Annals of Oncology (2017) 28 (suppl_5): v573-v594)
2. Case report in JCO Precision Oncology from same group
reported PR in one of this patient treated with cetuximab
-
CALGB/SWOG 80405
Chemo + Cetuximab
Chemo + Bevacizumab
1ST LINE
MET / ADVANCED
COLORECTAL
KRAS wt Codons 12 & 13
FOLFIRI or
FOLFOX
MD choice
ASCO, JUNE, 2014 Chemo + Cetuximab
OS = 29.9 mos
PFS = 10.4 mos
Chemo + Bevacizumab
OS = 29.0 mos
PFS = 10.8 mos N = 1137
: NO DIFFERENCE
All RAS
wt
OS = 32.0 mos
PFS =11.4 mos
OS = 31.2 mos
PFS = 11.3 mos
ESMO, SEP, 2014
N = 526
ESMO, 2016
N = 474 *
OS = 32.5 mos
OS = 31.2 mos
* Right or left-sided primary
Included in sidedness analysis
-
80405: Overall Survival by Sidedness (all RAS wt)
Side N
(Events)
Median
(95% CI)
HR
(95% CI) p
Left 325
(238)
35.2
(32.1-39.0) 0.72
(0.56-0.92) 0.009
Right 149
(114)
21.9
(16.3-29.0)
-
80405: OS by Sidedness (Bevacizumab)
Side
N
(Events)
Median
(95% CI)
HR
(95% CI)
Adjusted
p
Left 152
(119)
32.6
(28.3-36.2) 0.88
(0.62-1.25) .50
Right 78
(58)
29.2
(22.4-36.9)
-
80405: OS by Sidedness (Cetuximab)
Side N
(Events)
Median
(95% CI)
HR
(95% CI)
Adjuste
d P
Left 173
(119)
39.3
(32.9-42.9) 0.55
(0.39-0.79) 0.001
Right 71
(56)
13.6
(11.3-19.0)
-
80405: Sidedness Predictive for Biologics
Biologic by 1° Side Interaction BIOLOGIC SIDE OF PRIMARY HAZARD
RATIO
95% CI
P (adjusted*)
Any biologic
OS
Cetux v Bev; left
Cetux v Bev; right
1.81
(1.15, 2.84)
Pint = 0.009
PFS 1.94
(1.28, 2.95)
Pint = 0.001
Cetux v Bev
OS
Left 0.77
(0.59, 0.99)
0.04
PFS 0.84
(0.66, 1.06)
0.15
Cetux v Bev
OS
Right 1.36
(0.93, 1.99)
0.10
PFS 1.64
(1.15, 2.36)
0.006
*Adjusted for biologic, protocol chemotherapy, prior adjuvant
therapy, prior RT, age, sex, synchronous disease, in place
primary,
liver metastases
-
Numbers at
Risk
Cetuximab + FOLFIRI
38
10 0 0
0 0 0
Bevacizumab +
FOLFIRI
5
0
16 1 0 0 0 0
Cetuximab + FOLFIRI
38
24 10 4 1 1 0
Bevacizumab +
FOLFIRI
50
37 16 7 1 0 0
Progression-free survival
Overall survival
FIRE-3: Right-sided tumors
0.0
0.2
0.4
0.6
0.8
1.0
Pro
ba
bil
ity o
f P
FS
7.6
9.0
HR = 1.44 (95% CI: 0.92–
2.26)
p = 0.11
Right-sided mCRC
Bevacizumab + FOLFIRI (n=50)
0 12 60 72 24 36
48
Months
Numbers at Risk
0.0
0.2
0.4
0.6
0.8
1.0 Right-sided mCRC
Pro
ba
bil
ity o
f O
S
HR = 1.31 (95% CI:
0.81–2.11)
p = 0.28
Cetuximab + FOLFIRI (n=38)
Bevacizumab + FOLFIRI (n=50)
18.3 23.0
0 12 60 72 24 36 48
Months
Cetuximab + FOLFIRI (n=38)
-
Numbers at
Risk
Cetuximab + FOLFIRI
157
60 17 10 6 4 0
Bevacizumab +
FOLFIRI
149
56 13 7 2 0 0
0.0
0.2
0.4
0.6
0.8
1.0 Left-sided mCRC
Pro
ba
bil
ity o
f P
FS
10.7
10.7
HR = 0.90 (95% CI:
0.71–1.14)
p=.38
Cetuximab + FOLFIRI (n=157)
Bevacizumab + FOLFIRI (n=149)
0 12 24 36
Months
60 72 48
A
0.0
0.2
0.4
0.6
0.8
1.0 Left-sided mCRC
Pro
ba
bil
ity o
f O
S
0 12
HR = 0.63 (95% CI:
0.48–0.85)
p = 0.002
Cetuximab + FOLFIRI (n=157)
Bevacizumab + FOLFIRI (n=149)
60 72
24 36 48
Months
B
Cetuximab + FOLFIRI
157
131 77 38 23 6 0
Bevacizumab +
FOLFIRI
149
120 76 31 11 3 0
Progression-free survival
Overall survival
FIRE-3: Left-sided tumors
28.0 38.3
Numbers at
Risk
-
BRAF mut
MSI
KRAS
PIK3CA
Mucinous
differentiation
Right
Left
18q loss
20q Gain
EREG expression
EGFR gain
HER2 gain
Poor
Prognosis
Sensitive to
Cetuximab
Good
Prognosis
High mutation
Frequency
Distinct Biology of R v. L CRC
Analysis of PETACC-3 samples (n=2849)
Missiaglia, ASCO 2013
-
LEFTy Organization
-
LEFTy Organization
-
HR for OS According to Primary Tumor Location
Loree JM,.... Kopetz S; Clin Cancer Res 2018
-
T + EGFR-i
if ORR is a
primary goal
D + Bev
if EGFR-i are not
accepted/tolerated
RAS wt
Left-sided
Treatment options based on Location: My Take
D + EGFR-i
if OS is a
primary goal
Right-sided
D/T + Bev
if OS is a
primary goal
default
recommendation
default
recommendation D: chemo doublet
T: chemo triplet
-
Microsatellite Instability
-
3 6 5 7 3 0
-1 2 5
-1 0 0
-7 5
-5 0
-2 5
0
2 5
5 0
7 5
1 0 0
1 2 5
%C
ha
ng
e fro
m B
as
elin
e S
LD
M M R -d e fic ie n t C R C
M M R -p ro fic ie n t C R C
Le DT, et al.
NEJM 2015
and ASCO
2016
-1 0 0
-5 0
0
5 0
1 0 0
M M R -p ro fic ie n t C R C
M M R -d e fic ie n t C R C
% C
ha
ng
e fro
m B
as
elin
e S
LD
MMR-deficient CRC, N=28
MMR-proficient CRC, N=25
Response Rate 57% 0%
Disease Control Rate 89% 16%
Pembrolizumab
-
MSI-high CRC: Nivolumab Monotherapy
Overman et al. Lancet Oncology 2017
a
0 1 2 2 4 3 6 4 8 6 0 7 2 8 4 9 6 1 0 8 1 2 0
- 1 0 0
- 7 5
- 5 0
- 2 5
0
2 5
5 0
7 5
1 0 0
W e e k s
Ch
an
ge
in
S
um
o
f T
ar
ge
t L
es
io
ns
S
iz
e (%
)
O n
T r e a t m e n tO f f T r e a t m e n t
C o m p l e t e o r P a r t i a l
R e s o p o n s eF i r s t O c c u r r e n c e o f N e w L e s
io n
C h a n g e T r u n c a t e d t o 1 0 0 %
On treatment
Off treatment
CR or PR
First occurrence of new lesion
Disease Control ≥12weeks in 69%
RR 31% SD 39% PD 24%
-
Reduction in Target Lesions Regardless of PD-L1 Expression, BRAF
or Lynch History
≥ 1% < 1% + Confirmed CR/PR
Inve
stig
ato
r-A
sses
sed
Be
st C
han
ge in
Tar
get
Lesi
on
Siz
e (
%)
Tumor PD-L1 Expression
100
-50
-100
50
0
BRAF Mutation Status 100
-50
-100
50
0
Inve
stig
ato
r-A
sses
sed
Bes
t C
han
ge in
Tar
get
Lesi
on
Si
ze (
%)
Mutant Wild type + Confirmed CR/PR
Clinical History of Lynch Syndrome 100
-50
-100
50
0
Inve
stig
ato
r-A
sses
sed
Bes
t C
han
ge in
Tar
get
Lesi
on
Si
ze (
%)
Yes No + Confirmed CR/PR
Overman et al. Lancet Oncology 2017
-
World Congress On Gastrointestinal Cancer, 2018 Bendell J, et
al. IMblaze370
IMblaze370: randomised, Phase III, multicentre, open-label study
in mCRC
Atezo, atezolizumab; cobi, cobimetinib; INV, investigator; rego,
regorafenib. a Two-sided type I error rate of 0.05 was controlled
by hierarchical testing (testing atezo vs rego only if atezo + cobi
vs rego
was positive). NCT02788279.
32
• Unresectable locally
advanced or metastatic
CRC
• Received ≥ 2 prior
regimens of cytotoxic
chemotherapy for
metastatic disease
• ECOG PS 0-1
• MSI-H capped at 5%
Regorafenib 160 mg oral 21/7 days
Atezolizumab 840 mg IV q2w
+ cobimetinib 60 mg oral 21/7 days
Atezolizumab 1200 mg IV q3w R
2:1:1
N=363 Lo
ss o
f
clin
ical
ben
efi
t
Primary endpoint
• OSa
– Atezo + cobi vs rego
– Atezo vs rego
INV-assessed key secondary endpoints
• PFS
• ORR
• DOR
Stratification
• Extended RAS mutation status (≥ 50% patients in each arm)
• Time since diagnosis of first metastasis (< 18 months vs ≥
18 months)
• Data cutoff date: March 9, 2018
-
World Congress On Gastrointestinal Cancer, 2018 Bendell J, et
al. IMblaze370
Overall survival
N/A, not applicable. HRs are from stratified log-rank tests.
Data cutoff: March 9, 2018. a For descriptive purposes only.
33
Atezo + cobi
(n = 183)
Atezo
(n = 90)
Rego
(n = 90)
Median OS, mo
(95% CI)
8.9
(7.00, 10.61)
7.1
(6.05, 10.05)
8.5
(6.41, 10.71)
HR vs rego
(95% CI)
1.00
(0.73, 1.38)
1.19
(0.83, 1.71) N/A
P value 0.9871 0.3360a N/A
12-mo OS, % 38.5% 27.2% 36.6%
-
HER2 Overexpression
HER2/neu 3+ (2+)
-
Trastuzumab + Lapatinib in HER2+ / KRAS-wt pts refractory to
ani-EGFR AK
Siena, et al. ASCO 2015
HERACLES Trial
849 patients screened, 46 patients (5.4%) HER2+ (2+/3+); 23
patients evaluable for response
ORR 35%, DCR 78%
-
Optimal treatment of mCRC in
the presence of braf
-
Clinical Efforts in BRAFmut
37
BRAFi+ EGFRi
BRAFi+ EGFRi
+ PI3Ki
BRAFi+ EGFRi
+ MEKi
Roche/Genentech
GSK Novartis
BRAFi+ EGFRi
+ chemo
US Cooperative Groups
-
Study Design
Presented by: Scott Kopetz, MD, PhD
R
E
G
I
S
T
R
A
T
I
O
N
Local
BRAF
testing
No local
BRAF
testing
BRAF
V600E
Mutation
Central
Testing
Performed
Wild-type
(off study)
R
A
N
D
O
M
I
Z
A
T
I
O
N
ARM 1:
Cetuximab +
Irinotecan
ARM 2:
Vemurafenib +
Cetuximab +
Irinotecan
STEP 3: Cross-
over to add
Vemurafenib
Progression
Off Study
Progression Off Study
Vemurafenib 960mg PO bid continuous
Cetuximab 500mg/m2 IV q2weeks
Irinotecan 180mg/m2 IV q2weeks
-
Primary Endpoint: Progression-free survival
Presented by: Scott Kopetz, MD, PhD
N Events Median 95% Conf Int
Cetuximab + Irinotecan 50 46 2.0 (1.8 – 2.1)
Vemurafenib + Cetuximab 49 36 4.3 (3.6 – 5.7)
+ Irinotecan
HR = 0.48 (95% CI 0.31 – 0.75)
P=0.001
0 3 6 8 10 12 14
Months after randomization
80%
100%
60%
40%
20%
0%
April 18. 2017 data cutoff
-
Response Rate
Cetuxim
ab +
Irinotec
an
(n=45)a
Vemurafe
nib
+
Cetuxima
b +
Irinotecan
(n=43)a
P-valuec
Partial
response 4% 16%
P=0.001 Stable
disease 18% 48%
Progressionb 56% 12%
Disease
Control 22% 67%
Rate
a93 patients had measurable disease; b Including symptomatic
deterioration; c Chi-squared
Presented by: Scott Kopetz, MD, PhD
Cetuximab + Irinotecan
Vemurafenib + Cetuximab + Irinotecan
April 18. 2017 data cutoff
100%
20%
-100%
0%
-30%
100%
20%
-100%
0%
-30%
-
BEACON CRC Phase 3 Study Design1
Safety Lead-in Completed Phase 3 Currently Enrolling
ENCO 300 mg QD
+
BINI 45 mg BID
+
CETUX 400 mg/m2 (initial),
then 250 mg/m2 QW
Triplet therapy
ENCO + BINI + CETUX
n=205
Doublet Therapy
ENCO + CETUX
n=205
Control Arm
FOLFIRI + CETUX, or
IRI + CETUX
n=205
Disease
progression
Disease
progression
Disease
progression
Continued
follow-up
for
evaluation
of OS
R
1:1:1
1. Clinicaltrials.gov/ct2/show/NCT02928224;
https://clinicaltrials.gov/ct2/show/NCT02928224 (February
2018).
N=30
Van Cutsem et al., ESMO GI 2018
-
2 6 1 1 7 2 1 6 9 1 4 7 8 1 3 2 8 2 5 2 4 2 3 2 7 1 5 1 2 4 * 2
2 2 1 1 9 2 0 1 8 1 1 6 * 1 0 3 5 *
-1 0 0
-8 0
-6 0
-4 0
-2 0
0
2 0
4 0
6 0
8 0
1 0 0
P a rt ia l R e s p o n s e (n = 1 1 )
C o m p le te R e s p o n s e (n = 3 )
Best Percentage Change in Tumor Measurements from Baseline
*Patients with lymph node disease with decreases in short axis
dimensions consistent with RECIST 1.1 defined Complete Response.
†One patient had no baseline sum of longest diameters and is not
presented.
1. Kopetz S, et al. J Clin Oncol. 2017;35:Abstr 3505, with
permission.
Be
st
% C
ha
ng
e f
rom
Ba
se
lin
e
Patients†
1 Cetuximab + Irinotecan from SWOG S1406
Van Cutsem et al., ESMO GI 2018
-
BEACON SLI: Overall Survival 100
0
10
20
30
40
50
60
70
80
90
0 3 6 9 12 15 18 Time (mo)
Ove
rall
su
rviv
al (%
)
Patients with BRAFV600 mutation (N=29)
Censored patients
1-year OS rate: 62%
29 28 25 22 18 6 0
Survival Rate 1 Prior
Regimen
2 Prior
Regimens
6 mo 88% 85%
12 mo 63% 62%
Patients at risk
Van Cutsem et al., ESMO GI 2018
Median OS: Not reached Data fully mature through 12.6 months
-
Ras and effector dependencies
• KRAS subtype lines:
– depend on the canonical RAS-RAF MAPK pathway
– upregulate genes involved in the maintenance of the epithelial
phenotype
• RSK subtype lines:
– depend on the RSK-MTOR/PI3K axis to drive aerobic metabolism
to supplement glycolysis
– express mesenchymal markers ZEB1, TGFB, TWIST
Tina Yuan, Rachel Bagni, Cyril Benes, Arnaud
Amzallag, Bob Stephens, Ming Yi, FNLCR
Cell Feb 2018
RS
K
KR
AS
-
KRAS suptype: RAF/MEK/ERK dependencies
1. Inhibition of this signaling with MEK inhibitors
such as trametinib, selumetinib alone or in
combination
2. Inhibition of ERK with inhibitors such as MK-
8353, BVD-523
3.Combination of MEK and ERK inhibition to
overcome resistance
4.Pan raf inhibitors LY3009120
5.RAF/MEK inhibitor RO5126766
6.Combination of AKT/MEK PI3K/MEK inhibitors
7.Cdk4/6 and MEK inhibitors
-
MLH1 rs1799977 Outcome Data from KRAS mut mCRC patients in TRIBE
FOLFIRI/bevacizumab arm
HR 3.14 (95%CI 1.37-7.18) Median OS 25.8 vs 18.4 months
-
CCL2 rs4586 Outcome Data from KRAS mut mCRC patients in TRIBE
FOLFIRI/bev Arm
HR 0.51 (95%CI 0.28-0.92) Median PFS 25.8 vs 18.4 months
-
RAS mutated
BRAF mutated, MSS
MSI-High
RAS/BRAF wild type
• “Left Sided”
• “Right Sided”
Current View of mCRC Treatment
FOLFOXIRI + Bev
Vemurafenib/
Cetuximab/Irinotecan
or Clinical Trial
FOLFOX + Bev PD-1 inhibition
FOLFOX + Bev FOLFIRI + Bev
Salvage
Oral
agents:
Rego
TAS-102 FOLFOX + Cet/Pan
(or Bev)
FOLFOX + Bev FOLFIRI + Bev Irinotecan +
Cetuximab/Pantimumab
FOLFIRI + Bev (or
Cet/Pan)
FOLFOX + cetux
-
The one who knows more, may decide better