Critical immunity thresholdsfor measles elimination
Sebastian Funk
Centre for the Mathematical Modelling of Infectious Diseases London School of Hygiene & Tropical Medicine
!"vöå"!(}å!öZ&!u'öZ"u'ü!'o!u},"oo]vP!of!]v("!ü}µê!,]ê"'ê"ê
19 October, 2017
Outline
1.Background • Immunity targets for measles • Age-specific contact patterns
2.Results • Immunity profiles and elimination • Comparison to serological profiles
3.Conclusions and recommendations
1. Background

Background
- When the number of secondary infections generated by each infective person is less than 1, transmission will stop.
- To achieve this for measles, the population immune needs to be 93-95%, the herd immunity threshold.
- This is based on two assumptions: 1. homogeneous mixing among individuals 2. stationary, uniform immunity (through vaccination)
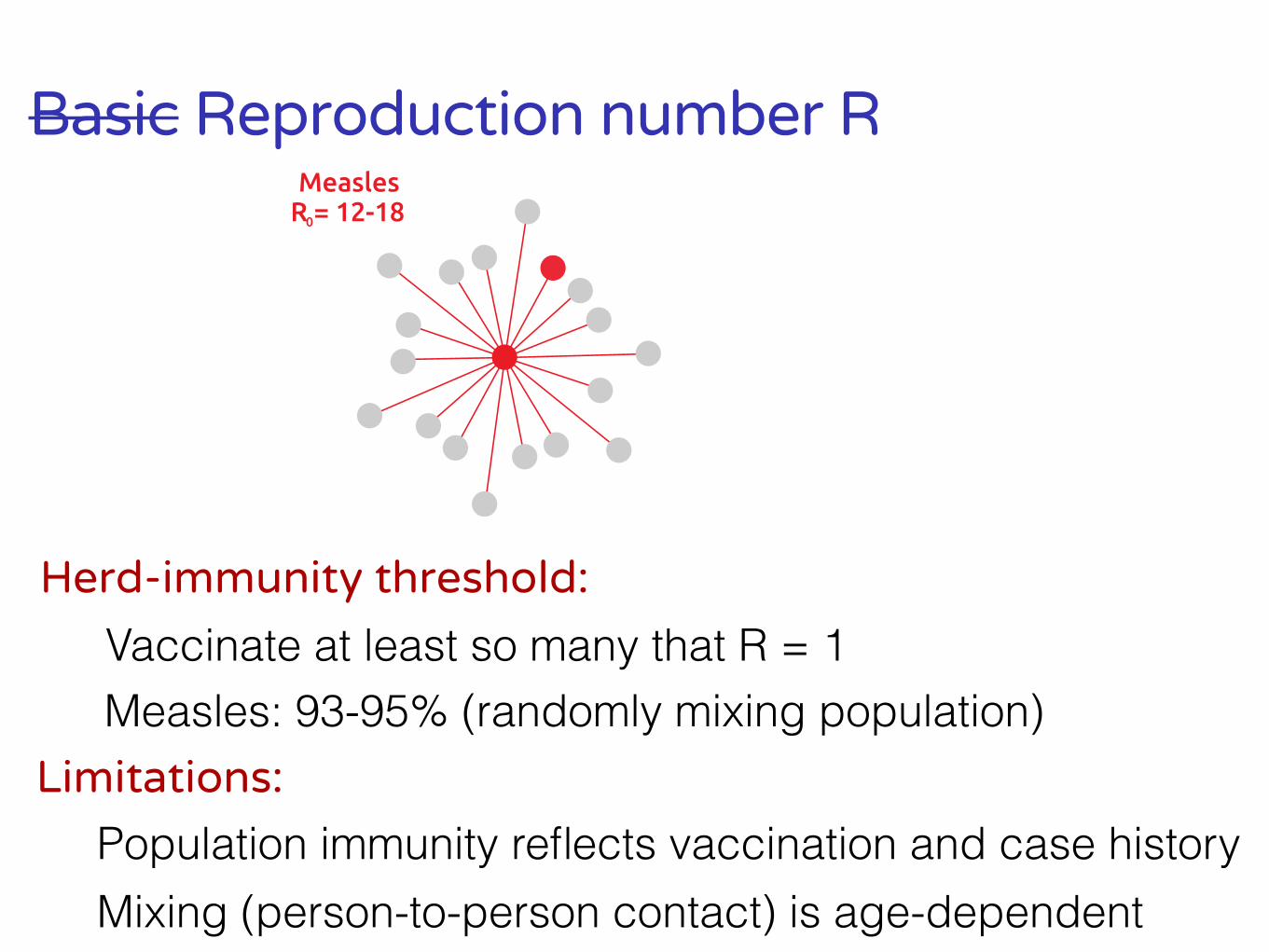
Basic Reproduction number R
Herd-immunity threshold:
Measles: 93-95% (randomly mixing population)Limitations:
Population immunity reflects vaccination and case history
Vaccinate at least so many that R = 1
MeaslesR = 12-180
Mixing (person-to-person contact) is age-dependent
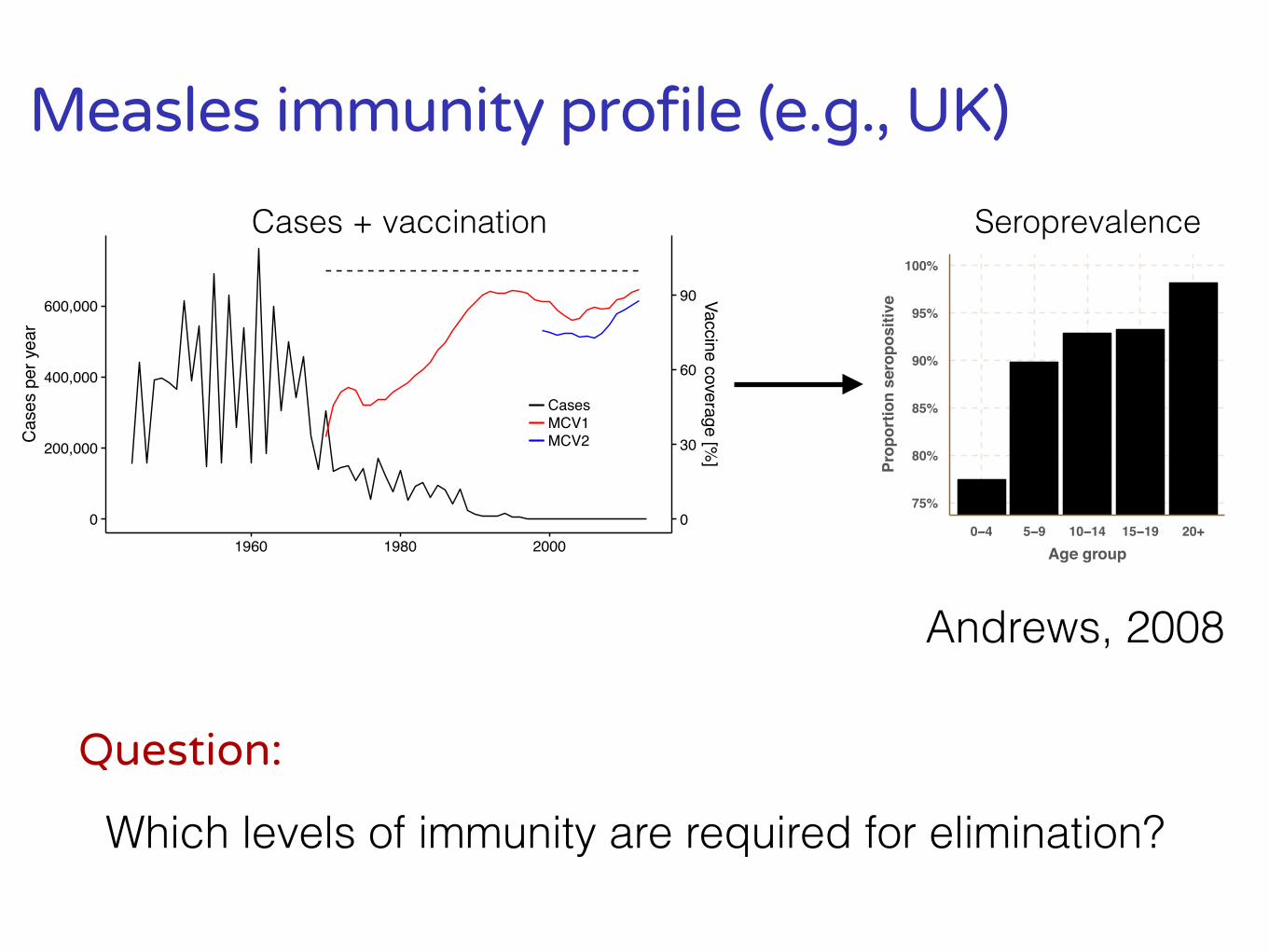
Measles immunity profile (e.g., UK)
75%
80%
85%
90%
95%
100%
0−4 5−9 10−14 15−19 20+Age group
Prop
ortio
n se
ropo
sitiv
e
Seroprevalence
Andrews, 2008
Question:
Which levels of immunity are required for elimination?
0
200,000
400,000
600,000
0
30
60
90
1960 1980 2000
Cas
es p
er y
ear
Vaccine coverage [%]
CasesMCV1MCV2
Cases + vaccination
Vaccination vs immunity targets
Vaccination target
Vaccinate (e.g. 95%) in each birth cohort.
Immunity target
Aim for age-specific levels of immunity, including past birth cohorts.
80%
85%
90%
95%
100%
0−4 5−9 10−14 15+Age
Immunity
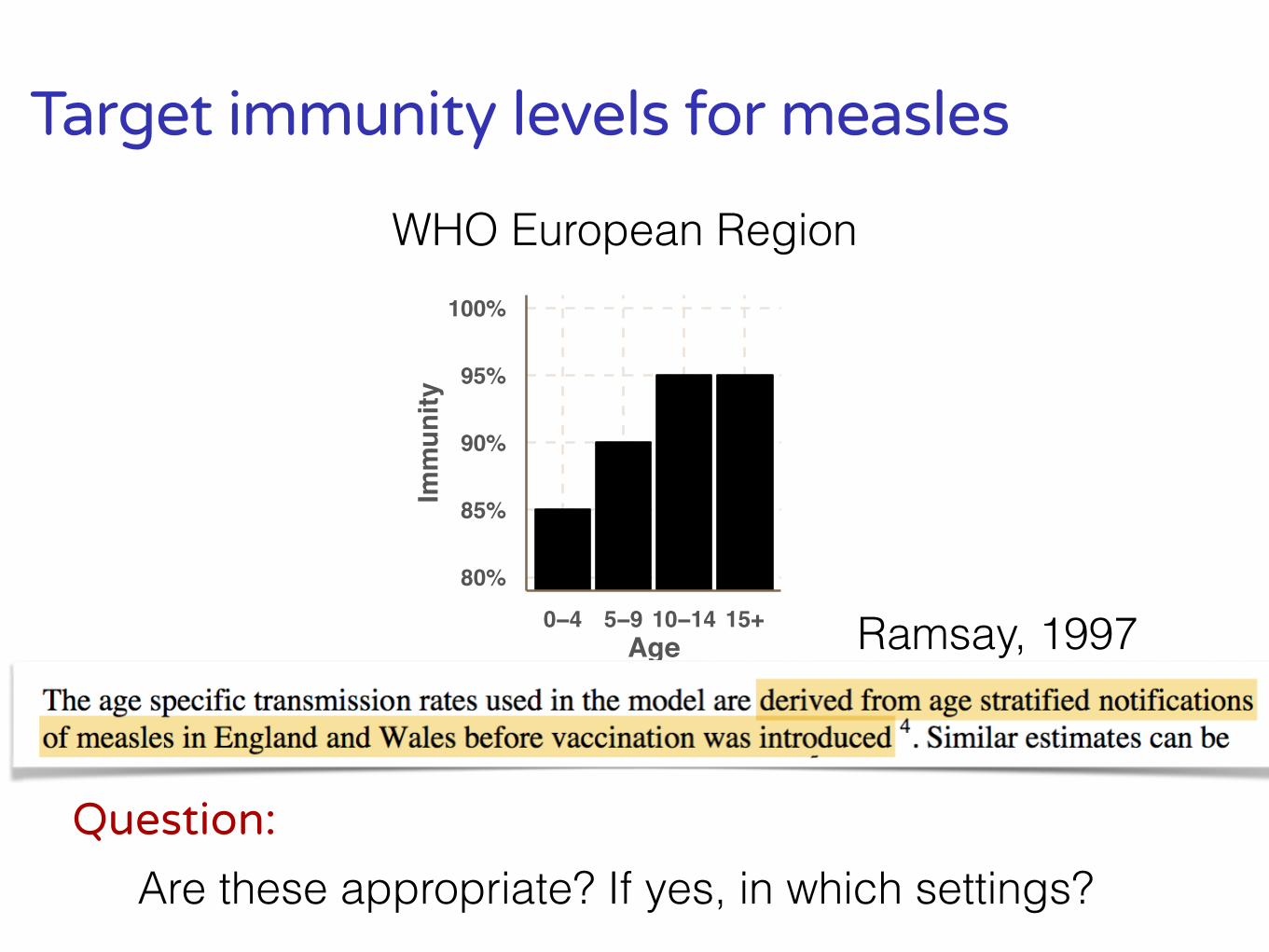
Target immunity levels for measles
Ramsay, 1997
Question:
Are these appropriate? If yes, in which settings?
WHO European Region
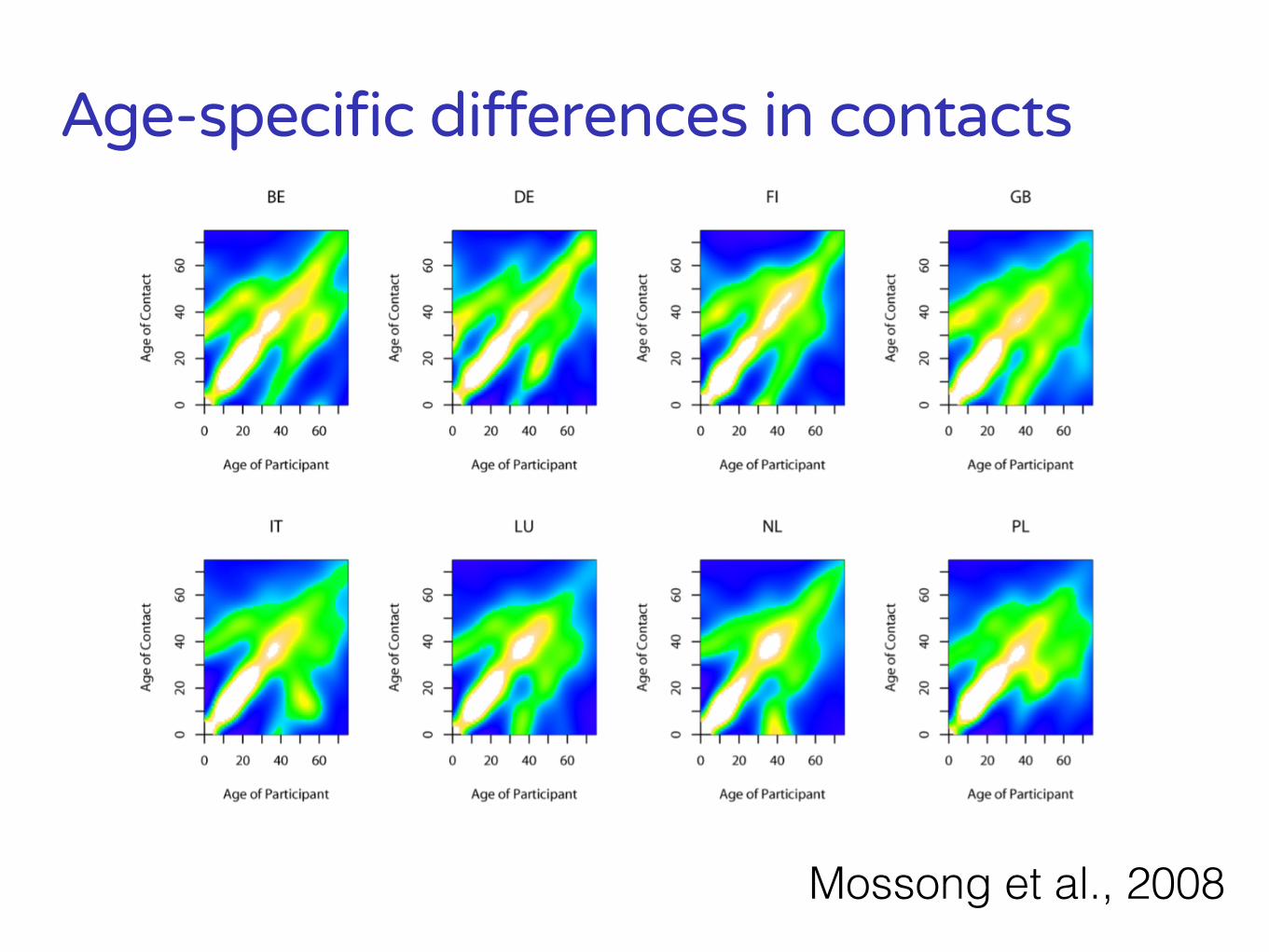
Age-specific differences in contacts
Mossong et al., 2008
80%
85%
90%
95%
100%
0−4 5−9 10−14 15+Age
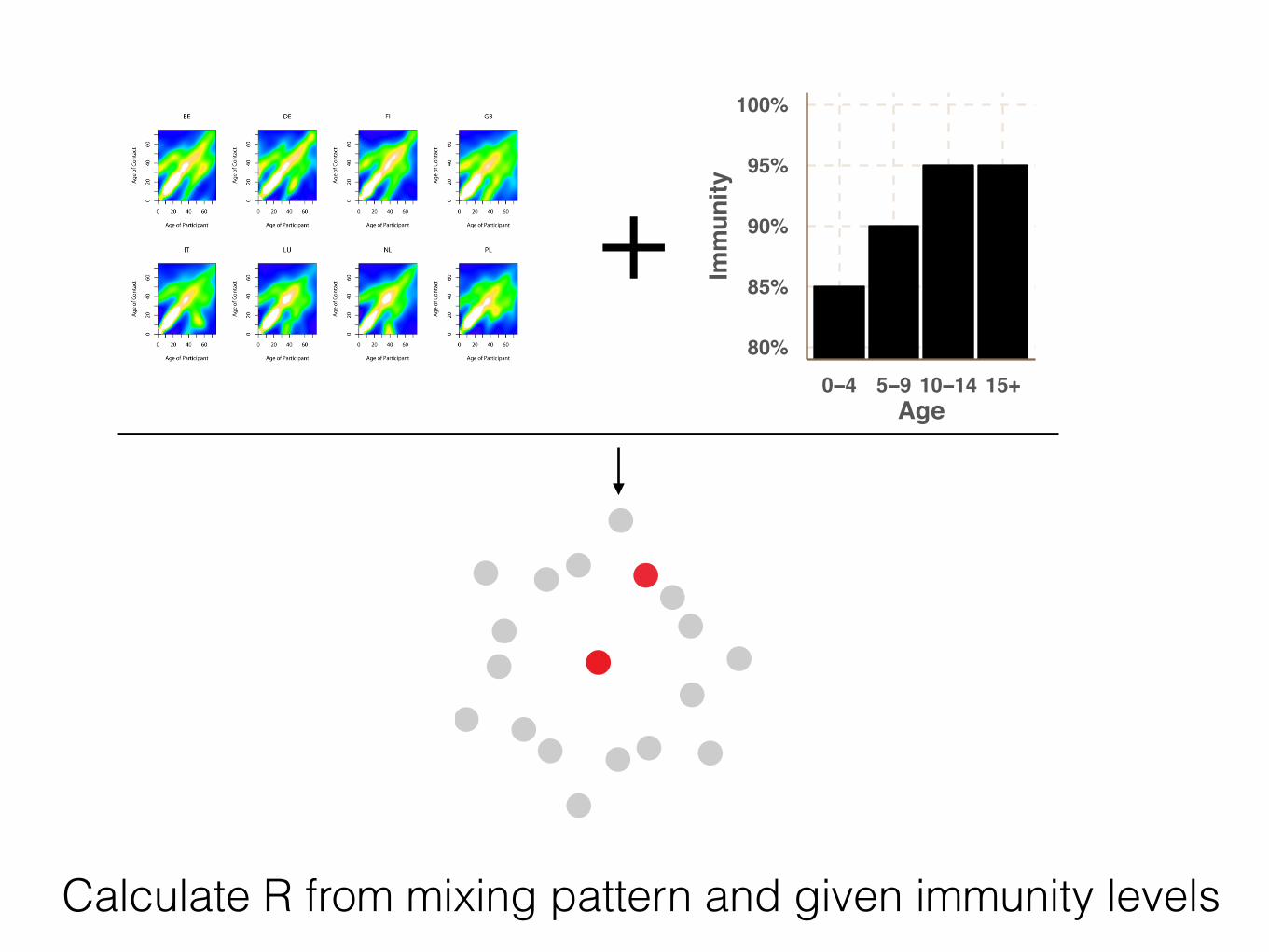
Immunity+
Calculate R from mixing pattern and given immunity levels

Contact data used in this study
2. Results
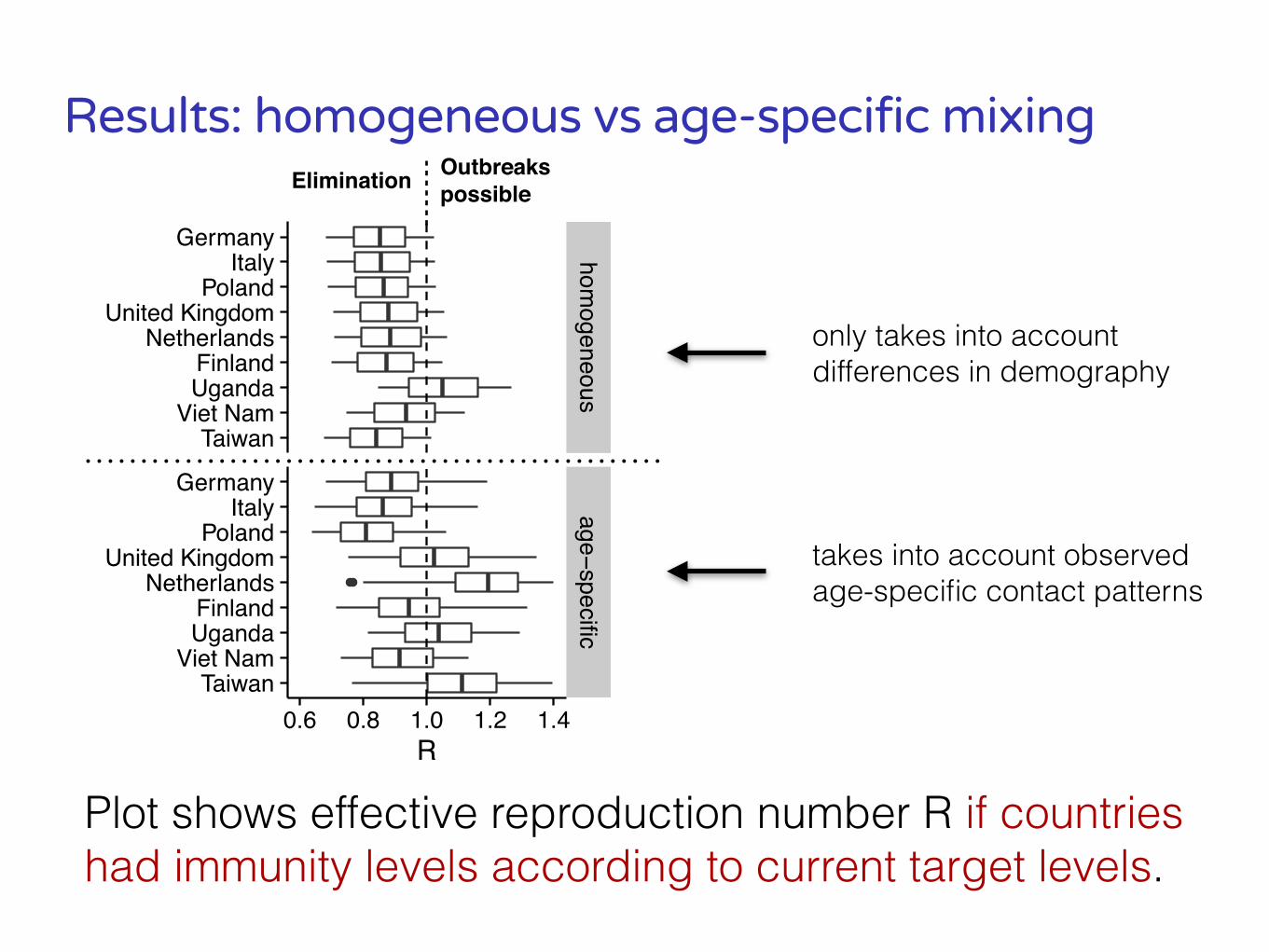
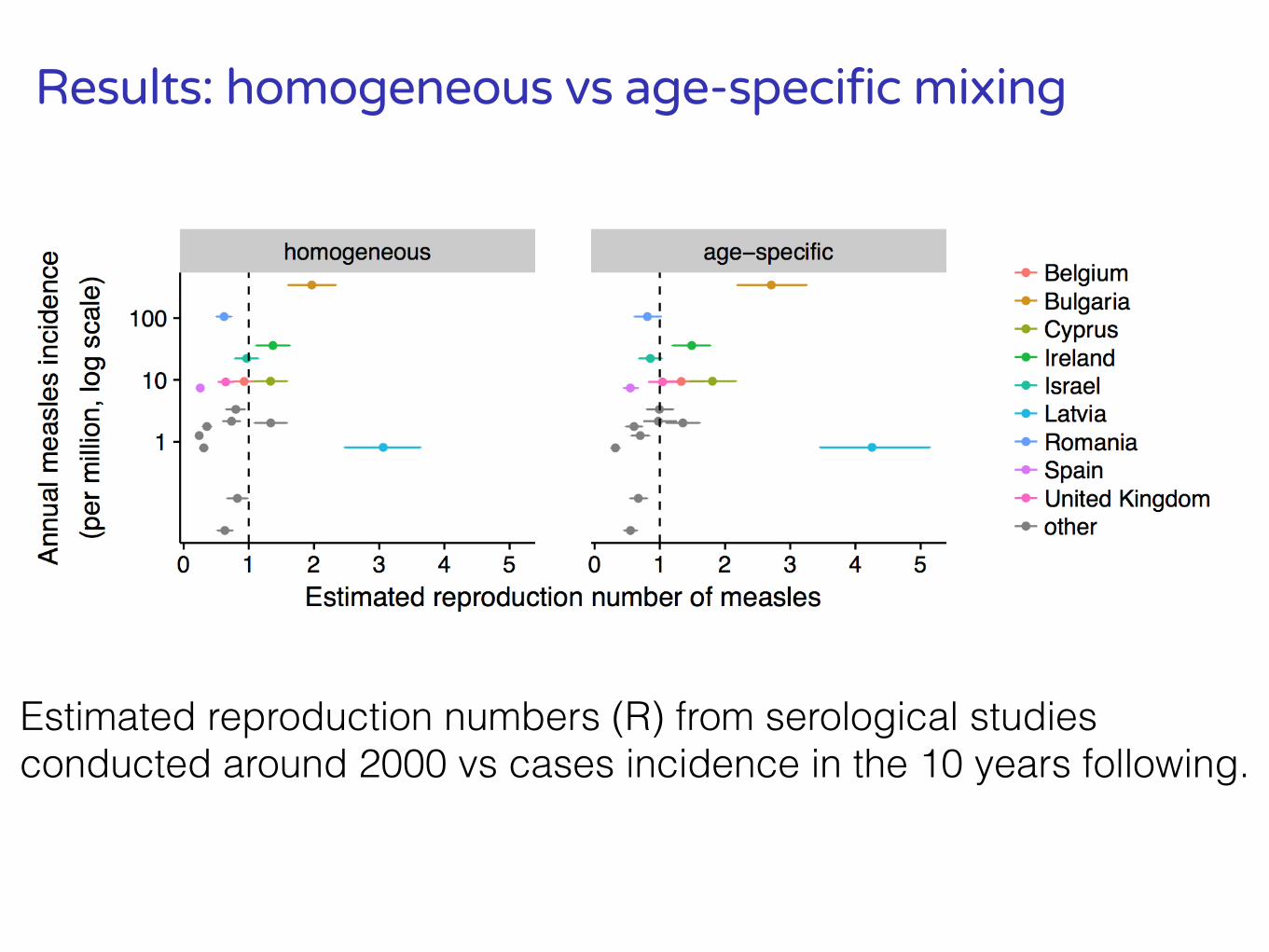
Results: homogeneous vs age-specific mixing
homogeneous
age−specific0.6 0.8 1.0 1.2 1.4
TaiwanViet Nam
UgandaFinland
NetherlandsUnited Kingdom
PolandItaly
Germany
TaiwanViet Nam
UgandaFinland
NetherlandsUnited Kingdom
PolandItaly
Germany
R
Plot shows effective reproduction number R if countries had immunity levels according to current target levels.
only takes into account differences in demography
takes into account observed age-specific contact patterns
Outbreaks possibleElimination
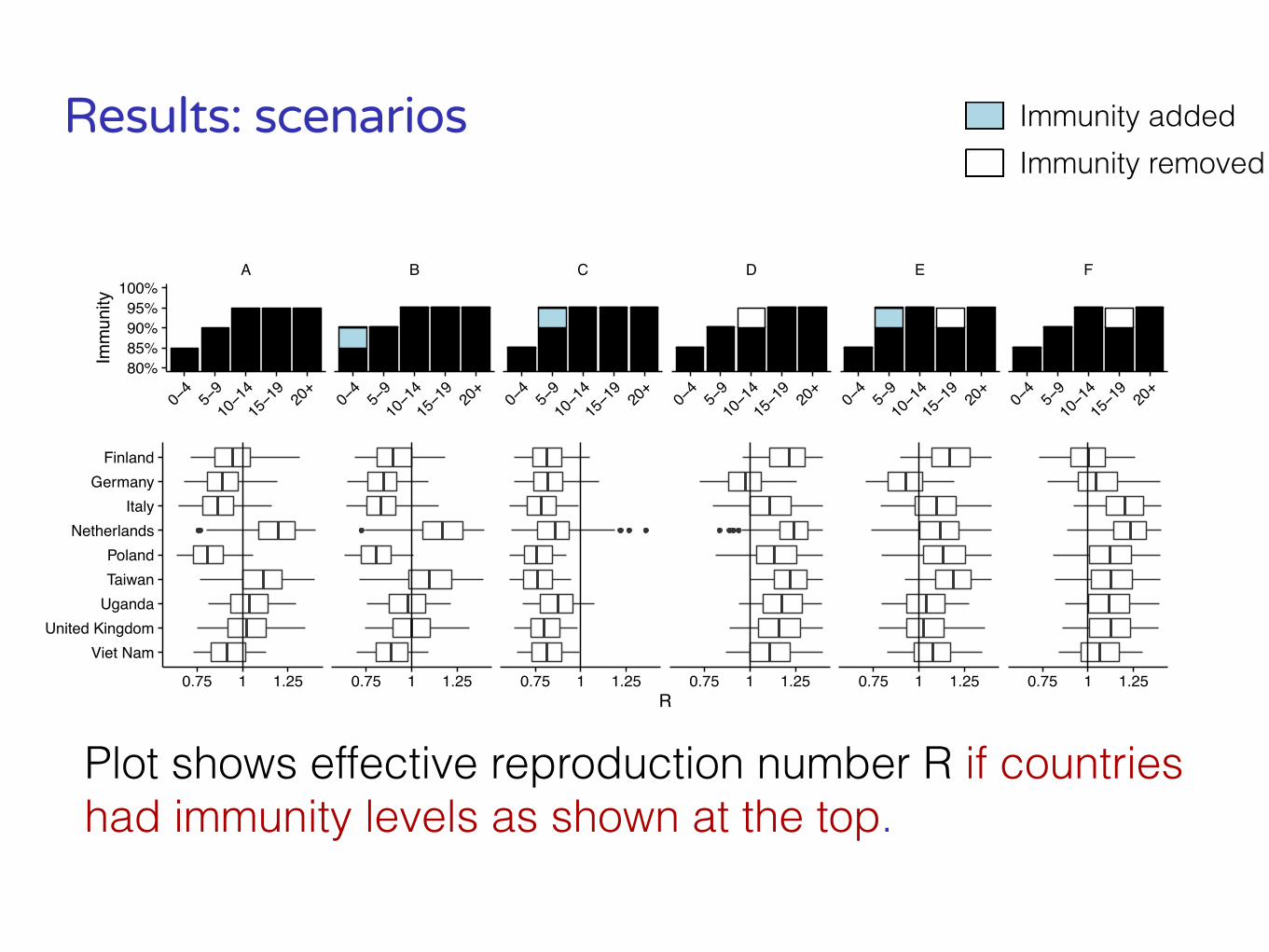
Results: scenarios
Plot shows effective reproduction number R if countries had immunity levels as shown at the top.
Immunity addedImmunity removed
A B C D E F
0−4
5−910−1
415−1
920
+0−
45−
910−1
415−1
920
+0−
45−
910−1
415−1
920
+0−
45−
910−1
415−1
920
+0−
45−
910−1
415−1
920
+0−
45−
910−1
415−1
920
+80%85%90%95%
100%
Imm
unity
0.75 1 1.25 0.75 1 1.25 0.75 1 1.25 0.75 1 1.25 0.75 1 1.25 0.75 1 1.25
Viet NamUnited Kingdom
UgandaTaiwanPoland
NetherlandsItaly
GermanyFinland
R

●●
●
●
●
●●
●
●
●
●●
●
●
●
● ●
●
●
●
●● ●
●
●
●
●● ●
●
●
●
●
●● ●
●● ●
●● ●
●
● ●
●
●●
●
● ●
●
●●
●
● ●
●
●●
●
●● ●
●
●
●● ●
●
●
●● ●
●
●
● ● ●
●
● ● ●
●
● ● ●
●
●●
●
●●
●
●●
●
● ●
●
● ●
●
● ●
● ● ● ●● ● ● ●● ● ● ●
●
● ●●
●
●
● ●●
●
●
● ●●
●
●
●●
●
●
●
●●
●
●
●
●●
●
●
●
●
●
●
●
●
●
●●
●
●●
●
●●
●●
● ●●
●● ●
●●
● ●
●
●●
●
●
●●
●
●
●●
●
●
● ●● ●
●
● ●● ●
●
● ●● ●
Belgium Cyprus Czech Republic Hungary
Ireland Israel Latvia Lithuania
Luxembourg Malta Romania Slovakia
Slovenia Spain Sweden United Kingdom
60%70%80%90%
100%
60%70%80%90%
100%
60%70%80%90%
100%
60%70%80%90%
100%
[0,5)[5,
10)
[10,15
)
[15,20
)
[20,25
)
[25,30
)[0,
5)[5,
10)
[10,15
)
[15,20
)
[20,25
)
[25,30
)[0,
5)[5,
10)
[10,15
)
[15,20
)
[20,25
)
[25,30
)[0,
5)[5,
10)
[10,15
)
[15,20
)
[20,25
)
[25,30
)
Age group
Prop
ortio
n im
une
● Serology
Finding gaps in immunity: serology
Andrews et al. (2008)
Results: homogeneous vs age-specific mixing
Estimated reproduction numbers (R) from serological studies conducted around 2000 vs cases incidence in the 10 years following.
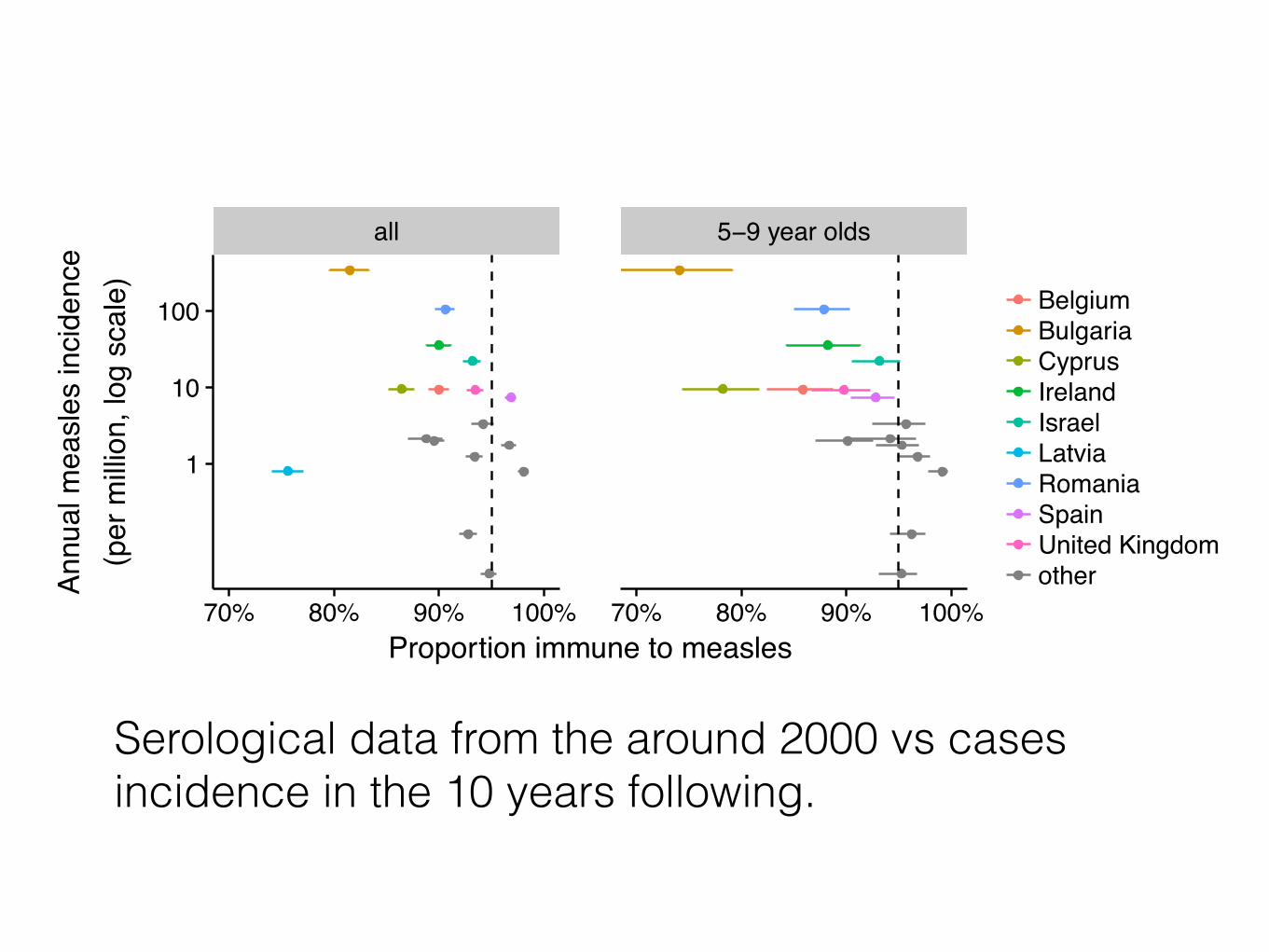
Serological data from the around 2000 vs cases incidence in the 10 years following.
all 5−9 year olds
70% 80% 90% 100% 70% 80% 90% 100%
1
10
100
Proportion immune to measles
Annu
al m
easl
es in
cide
nce
(per
milli
on, l
og s
cale
)
BelgiumBulgariaCyprusIrelandIsraelLatviaRomaniaSpainUnited Kingdomother
3. Conclusions and recommendations
Lessons from the United States
- Pre-elimination outbreaks in vaccinated school-aged populations (>90% uptake)=> high vaccination levels needed to prevent outbreaks in schools.
- Lower coverage at 2nd birthday may be sufficient to prevent outbreaks IF population immunity is high among school-age children (except if there are high contact rates among preschool children, e.g, childcare)
Measles eliminated in 2000
Conclusions
- Old immunity targets are not sufficient for measles elimination.
- For elimination in all scenarios, need higher immunity levels in 5-9 year olds compared to previous targets.
- Besides, it is important to maintain high levels of immunity in older age groups.
- Serological studies can help identify gaps in in immunity in key age groups.
Limitations
- National targets don’t take into account heterogeneity and clustering of susceptibles.
- Targets don’t take into account waning immunity.
- Results depend on reported contact rates.
- Range of 11-18 for R0 may not apply to all settings
Programmatic implications
- Achievements towards elimination usually expressed via coverage levels, but they only tell part of the story
- School-entry checks could be a method to identify and correct missing immunity in 5 year olds
- Serological studies could be needed to identify immunity gaps in older age groups
Measles and Rubella SAGE WG proposed recommendations (1)
1. Achieving at least 95% immunity across all age groups, geographical regions and population subgroups through coverage of at least 95% of each birth cohort with 2 doses of MCV remains the primary goal for measles elimination.
2. To achieve this, countries ideally should assess age-group specific immunity levels to identify age-groups with levels of immunity below predefined thresholds to be targeted for vaccination.
Measles and Rubella SAGE WG proposed recommendations (2) 3. Neglecting immunity gaps in children older than five years of age, adolescents
and adults could make it more difficult and costly to achieve measles elimination.
4. Immunity gaps in school-aged children are important and could increase the disease burden and mortality among infants younger than 1 year of age as school-aged children are likely sources of measles virus infection within families (as siblings in school or in the future as parents). Therefore, the MR SAGE WG recommends that:
• Countries conducting follow-up MCV vaccination campaigns should target school-age children 5-9 years of age whenever MCV coverage among this epidemiologically important age group is assessed to be significantly lower than 95%.
• Countries should put into place school entry checks for vaccination as they are an important tool to help identify and address immunity gaps in school-age children.
Recommended