Microsoft PowerPoint - (2007-11 TUGA) Debate in vagianl pevlic
surgery to meh.ppt Ming-Ping Wu 1,2,
Director, Div. Urogynecology & Pelvic Floor Reconstruction,
Dept. Obstetrics and Gynecology1,
Chi Mei Foundation Hospital, Tainan, Taiwan; College of Medicine,
Taipei Medical University2,
Taipei, Taiwan
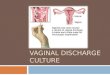
Anterior repair/ paravaginal repair + prosthestic reinforcement
Continence surgery ± sling, Burch colposuspension, bulking
agents
• Middle compartment Abdominal hysterectomy+ sacrocolpopexy Vaginal
hysterectomy+ iliococcygeus/ sacrospinous fixation Abdominal or
vaginal sacrospinous/ sacrohysteropexy
• Posterior compartment Posterior repair Rectopexy Anal sphincter
repair
Birch C 2002 Curr Opin Obstet Gynecol
+ prosthestic reinforcement
+ prosthestic reinforcement
Why do we need prostheses in pelvic reconstructive surgery ?
• The high recurrence rate after surgery for pelvic organ prolapse
(POP) makes the more refined reconstructive surgery
imperative
High failure rate 30% (Olsen AL 1997 Obstet Gynecol)
• The long-term anatomic outcomes of traditional cystocele
repair
High failure rate 37% (Quiroz LH 2006 Contemp Ob/Gyn)
• Therefore, biological and synthetic prostheses merged as adjuvant
materials.
Reasons for surgical failure • Poor patient selection • Suboptimal
surgical technique • Inappropriate choice of suture materials •
Persistence of predisposing risk factors
Poor tissue quality Impaired healing Chronic increased
intra-abdominal pressure
• due to COPD, asthma, or constipation
High-grade cystocele Age 60 or above
Whitesides JL 2005 Obstet Gynecol Surv
pubovervical f.
Rectovaginal f.
1) Does it improve the function of the repair?
2) Does it improve the durability of the repair?
3) Does the graft increase the rate of complication?
History of prosthesis
• Inguinal hernia repair in general surgery 43% recurrence in the
suture repair group 24% in the mesh augmented repair group
• Luijendij R 2000 NEJM
• History of synthetic non-absorbable prostheses 1903 metallic
silver mesh 1938 Nylon 1956 Dacron (Mersilene) 1958 polypropylene
(Marlex)
Advantages of prostheses
• the surgeon can repair all vaginal defects faster and with less
effort.
• Well anatomic support anterior compartment, anchored to
ATFP
• Level II attachment
Posterior compartment, to the level of the ischial spine, • level I
support. (DeLancey 1992 JOL Am J Obstet Gynecol)
• Concomitant surgery POP + SUI using different shaped
materials.
The purposes of prosthesis in pelvic reconstructive surgery
• The purposes of prostheses in pelvic reconstructive surgery
are
to substitute the lacking supportive tissue, to reinforce the
inadequate tissue, to generate new supportive tissue, to
consolidate the insufficient surgical technique.
The Evolution of Pelvic Reconstructive Surgeries
VTH+ A-P colporrhaphy
Sacro-spinous lig. suspension
Biologic materials**
Huang KH & Wu MP Incont Pelvic Floor Dysfunc
*Prolift (J&J); Perigee+Apogee (AMS); post. IVS (Tyco); Nazca
(Promedon)
**SIS (Cook); Pelvicol (Bard)
response than autologous tissue
• Be chemically inert • Be able to be modeled in
the required shape • Be able to sterilized • Be resistant to
infection
Must not • Physically modified by
tissue fluids • Induced an inflammatory
reaction or antibodies • Be carcinogenic • Induce allergy or
hypersensitvity • Promote adhesion at the
surface of contact or viscera
Cossen M 2003 Int Urogyn J
The different prostheses in pelvic reconstructive surgery
Baessler & Maher 2006 Curr Opin Obs Gyn
The comparison of the microscopic appearance of synthetic
prostheses.
Birch C 2005 Best Proc Res Clin Obstet Gynecol
Classification of Synthetic Prostheses
component Brand names
I Monofilament macroporous
II monofilament microporous
IV submicronic < 1µ polypropylene sheet
Silastic (Dow Corning) Cellgard (Hoescht)
Birch C 2002 Curr Opin Obstet Gynecol
Different Synthetic Prostheses
Type Fiber type Pore size
component Brand names
SIS (Cook) Pelvicol (Bard)
Autologous Rectus shealth Fasica lata Vaginal mucosa
The Evolution of Pelvic Reconstructive Surgeries
VTH+ A-P colporrhaphy
Sacro-spinous lig. suspension
Biologic materials**
Abdominal sacro-colpopexy with synthetic mesh: surgical
outcomes
Birch C Fynes MM 202 Curr Opin Obstet Gynecol
Abdominal sacro-colpopexy with synthetic mesh: surgical
outcomes
• A systematic review of 98 articles success rates for apical
support of 78–100% support of all segments of 58–100%
• [Nygaard IE 2004 Obstet Gynecol ].
• Synthetic rather than biological prostheses randomized trial
polypropylene mesh (91% cure) better than cadaveric fascia lata
(68% cure) (p= 0.007) at 1 year follow-up in favor of the
polypropylene mesh group at POP-Q points Aa and C, as well as
overall prolapse stages, sig.
• [Culligan PJ 2005 Obstet Gynecol].
The Evolution of Pelvic Reconstructive Surgeries
VTH+ A-P colporrhaphy
Sacro-spinous lig. suspension
Biologic materials**
Anterior compartment repairs with prosthetic reinforcement
Birch C 2005 Best Practice & Research
Sig.
Sig.
Anterior vaginal wall prolapse repair with nonabsorbable mesh
• high anatomical cure rates polypropylene meshes 87%, 91.6%, 100%
(Salvatore S 2002 Neurourol Urodyn, de Tayrac R 2005 J Reprod Med,
Milani R et al. 2005 BJOG)
• with relatively high mesh erosion rates 8.3%, 13% (de Tayrac R et
al. 2005 J Reprod, Salvatore S al. 2002 Neurourol Urodyn, Med,
Milani R et al. 2005 BJOG)
• Worsening dyspareunia anterior mesh repair, 20% posterior mesh
repair 63% (Milani R et al. 2005 BJOG)
• Comparable incidence of de novo dyspareunia In patients with (9%)
without (11%) vaginal erosion (p=0.85) (Deffieux X et al. 2007 Int
Urogyn J)
How do you read this?
The Evolution of Pelvic Reconstructive Surgeries
VTH+ A-P colporrhaphy
Sacro-spinous lig. suspension
Biologic materials**
Huang KH & Wu MP Incont Pelvic Floor Dysfunc
*Prolift (J&J); Perigee+Apogee (AMS); post. IVS (Tyco); Nazca
(Promedon)
Advantages of procedural kits-I
• Simple and efficient surgical technique Reduced surgery time
Short learning curve Simple and precise transfer of the anchoring
arms. Simplified tension-free system
Advantages of procedural kits-II
• Anatomically-designed needle system Minimally invasive needles
enable easy and accurate placement. The handle’s ergonomic design
provides optimal control over the needle’s insertion.
Gynecare Prolift Prolift Pelvic Floor Repair System
Gynecare Prolift Prolift Pelvic Floor Repair System
Anterior incision
Nazca POP repair system
TVT-O
A B
Options TVM +/- TVT-O
perioperative and immediate post-operative results,
• Success rate: 95.3% (failure rate 4.7%) recurrent prolapse even
asymptomatic or low grade symptomatic prolapse
• Mesh exposure 4.7% (5/110) 2/ 5 required a surgical
management
• Prolift seems to be a safe technique to correct POP. However,
anatomical and functional results of a long-term follow-up has not
yet to confirm the effectiveness and safety of the procedure
[Fatton B 2006 Int Urogyn J].
Mesh erosion or migration
• Current available mesh polypropylene 0.5%, polyethylene
terephthalate (Mersilene) 3.1% (J&J) Gore-Tex 3.4% (Gore)
polyethylene 5.0% (Marlex) (Bard) Teflon 5.6% (DuPont) Nygaard IE
2004 Obstet Gynecol.
Huang KH & Wu MP Incont Pelvic Floor Dysfu
Mesh erosion due to different materials
• Type II, III : 20–30% woven, multi-filamentous in nature limited
host-tissue ingrowth leading to erosions, draining sinuses, and
fistulae.
(Debodinance P et al. 1999 Eur J Obstet Gynecol Reprod Biol
],[Julian TM 1996 Am J Obstet Gynecol)
17% intravaginal slingplasty (Tyco.) (Siegel AL et al. 2005 J
Urol)
• Type I: 0.5- 5% (Fatton B et al. 2007 Int Urogyn J)
Mesh erosion due to different approaches
• Approach abd. sacro-colpopexy 3.2% sacral colpoperineopexy 4.5%
Suture vaginally, introduce mesh abd. 16% Introduce mesh vaginally
40%
(Visco AG 2001 Am J Obstet Gyneol)
• Techniques Erosion 17.5% 2.7% in the avoidance of T-shaped
colpotomies, concomitant hysterectomy and perineal incision
(Debodinance P 2004 J Gynecol Obstet Biol Reprod)
Take-home message-1
• The high recurrence rate after surgery for pelvic organ prolapse
(POP) makes the more refined reconstructive surgery
mandatory.
• The prostheses are viewed as a scaffold for tissue in-growth and
not as a permanent bridge.
• The use of synthetic prostheses is well established in
sacro-colpopexy,
controversial for repair of anterior and posterior wall
defects.
Take-home message-2 • Synthetic prostheses may have slightly
higher
success rates but higher erosion rate biologic materials: better
tolerated & lower erosion rate.
• Which prostheses (synthetic or biological) is superior in vaginal
surgery currently: inconclusive
• Ideal prostheses with various characters are not available
currently,
synthetic non-absorbable, synthetic absorbable, mixed synthetic, or
biological?
The surgeons themselves should be the decision-makers, not the
manufacturers!
Thank you!