Dentin Hypersensitivity
DH102: Clinic IILisa Mayo, RDH, BSDH
Concorde Career College
Reference
Wilkins CH43
Outline
1. Define dentinal hypersensitivity2. Review Anatomy of Tooth Structures3. What can cause dentin exposure4. Hydrodynamic Theory5. Natural Desentization6. Desentization Products
Objective #1: Define Dentinal Hypersensitivity
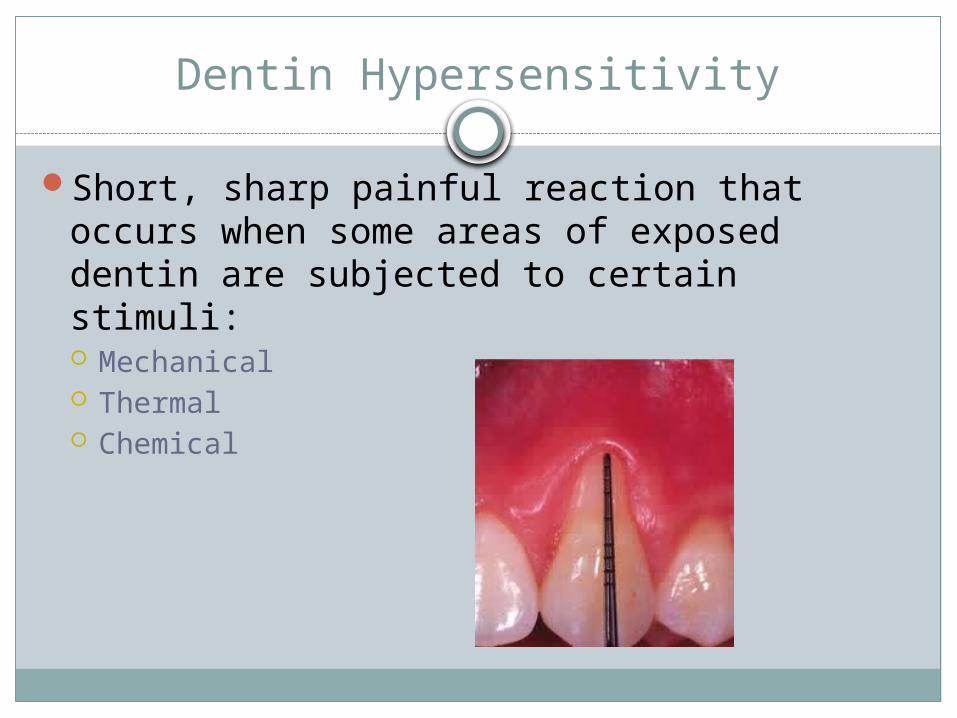
Dentin Hypersensitivity
Short, sharp painful reaction that occurs when some areas of exposed dentin are subjected to certain stimuli: Mechanical Thermal Chemical
Hypersensitivity
Patient Concerns Hot/cold sensitivity to foods/drinks Pain during dental appointments: metal instruments
can elicit pain Will ask RDH why they have pain
Dentinal Hypersensitivity Difficult to diagnose: their pain could be caused by
many factors. May not be dentinal sensitivity. Numerous tx approaches Pain elicited by a stimulus and alleviated upon its
removal
Stimuli That Elicit Pain Reaction
Tactile or mechanical Toothbrushing Eating utensils Dental instruments Friction from prosthetic devises such as denture
clasps Evaporative
Dehydration of oral fluids as from high-volume suction or applying air to dry teeth during intraoral procedures
Thermal Cold more common than hot
Stimuli That Elicit Pain Reaction
Chemical Acids in foods and beverages such as citrus fruits,
condiments, spices, wine, and carbonated beverages Acids produced by acidogenic bacteria following
carbohydrate exposure Acids from gastric regurgitation Osmotic
Alteration of osmotic pressure in dentinal tubules due to isotonic solutions of sugar & salt
Characteristics of Pain from Hypersensitivity
Pain at onset Sharp, short, transient pain and rapid onset
Cessation From pain upon removal of stimulus
Chronic condition w/ acute episodesResponse to non-noxious stimulus (one that
would not normally cause pain or discomfort)Discomfort that cannot be ascribed by
another dental defect or pathology
Objective #2: Review Tooth Anatomy
Anatomy of Tooth Structures
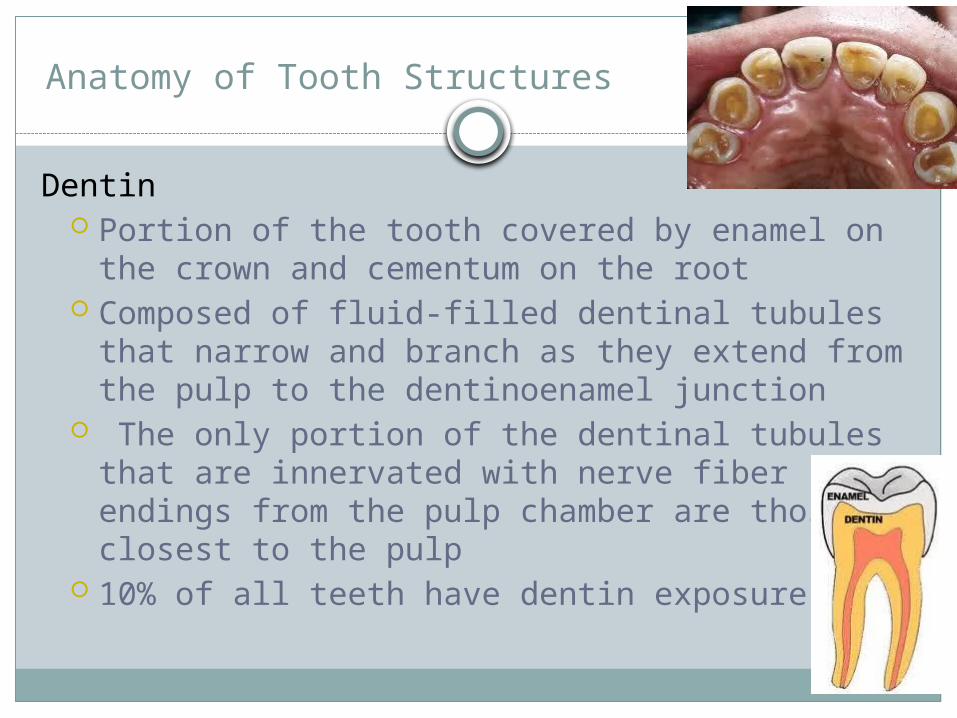
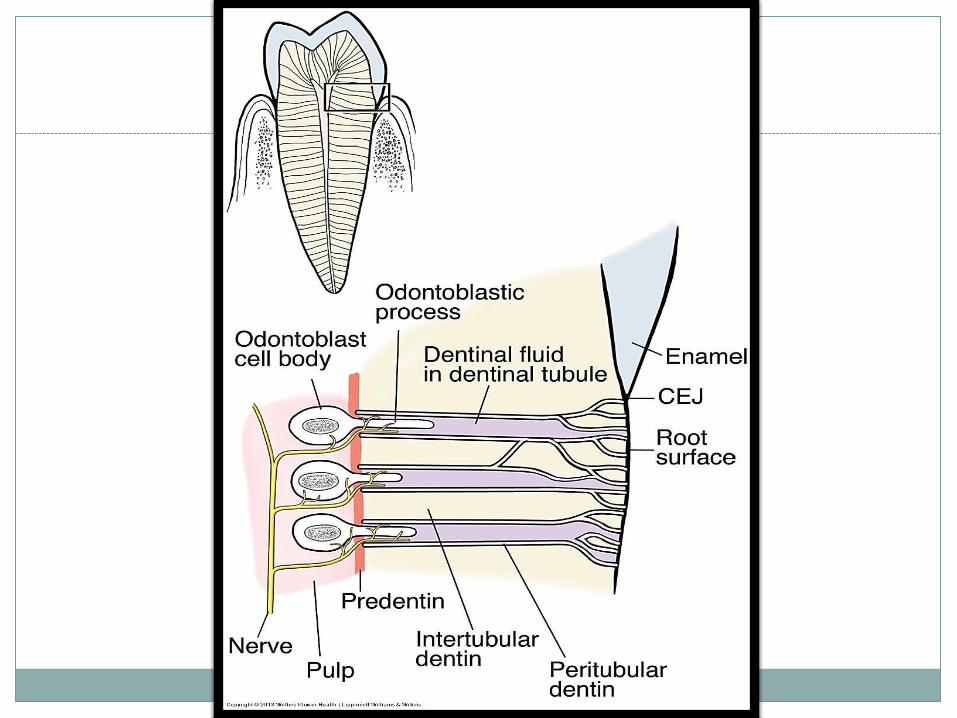
Dentin Portion of the tooth covered by enamel on the
crown and cementum on the root Composed of fluid-filled dentinal tubules that
narrow and branch as they extend from the pulp to the dentinoenamel junction
The only portion of the dentinal tubules that are innervated with nerve fiber endings from the pulp chamber are those closest to the pulp
10% of all teeth have dentin exposure
Anatomy of Tooth Structures
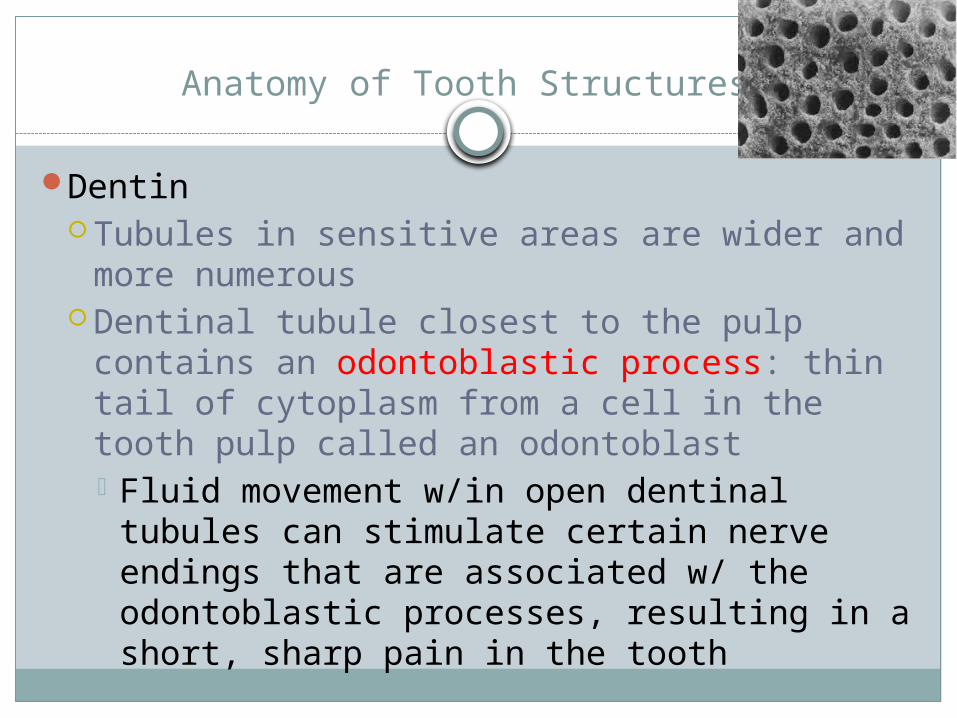
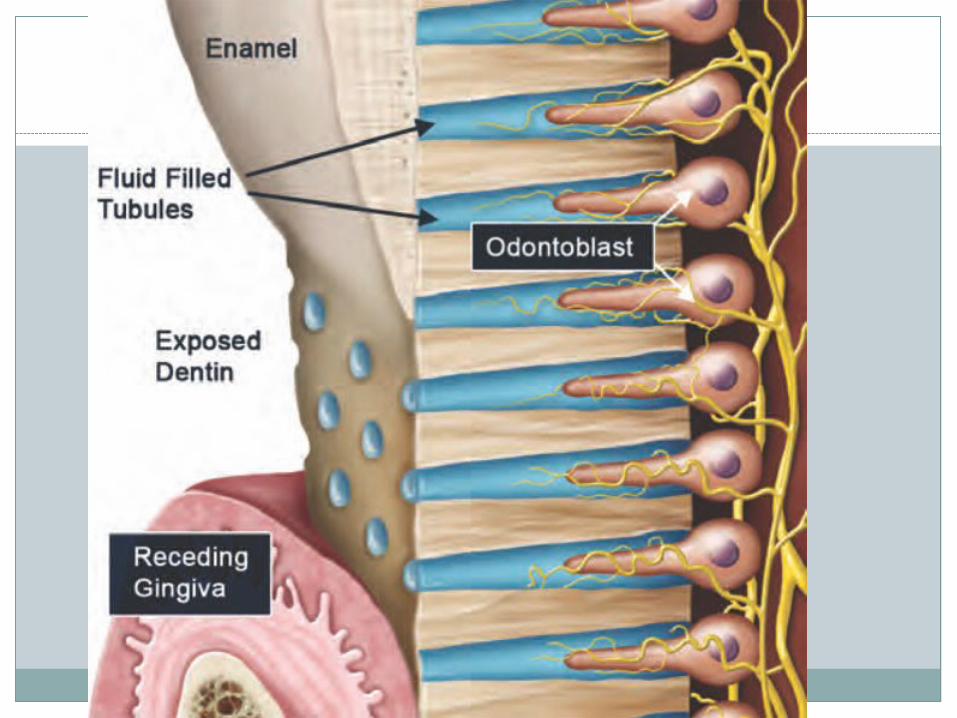
Dentin Tubules in sensitive areas are wider and
more numerous Dentinal tubule closest to the pulp contains
an odontoblastic process: thin tail of cytoplasm from a cell in the tooth pulp called an odontoblast Fluid movement w/in open dentinal tubules
can stimulate certain nerve endings that are associated w/ the odontoblastic processes, resulting in a short, sharp pain in the tooth
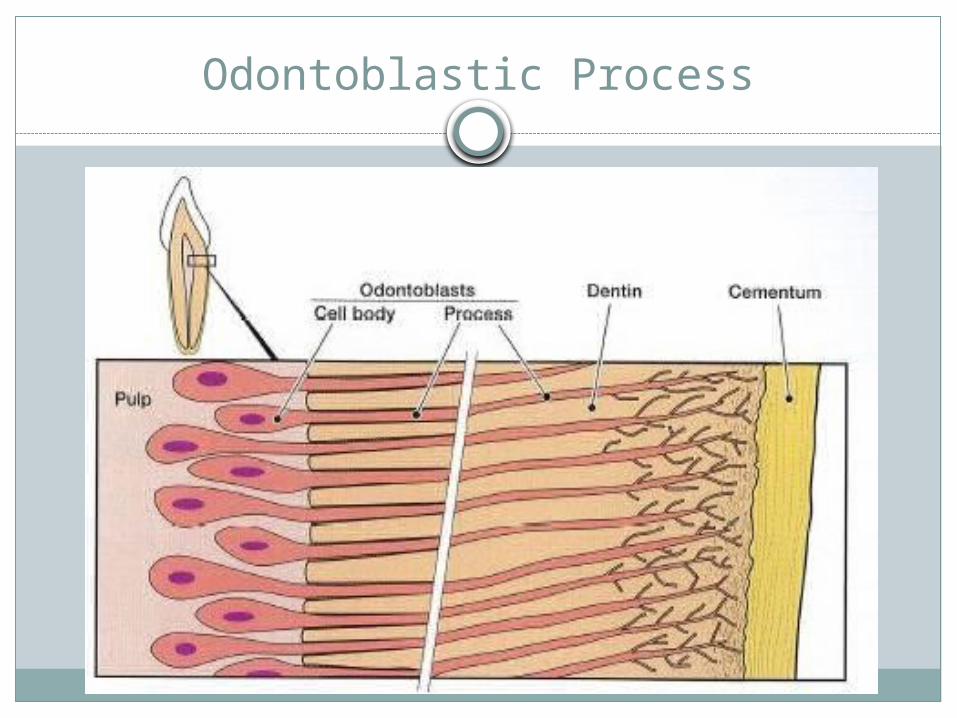
Odontoblastic Process
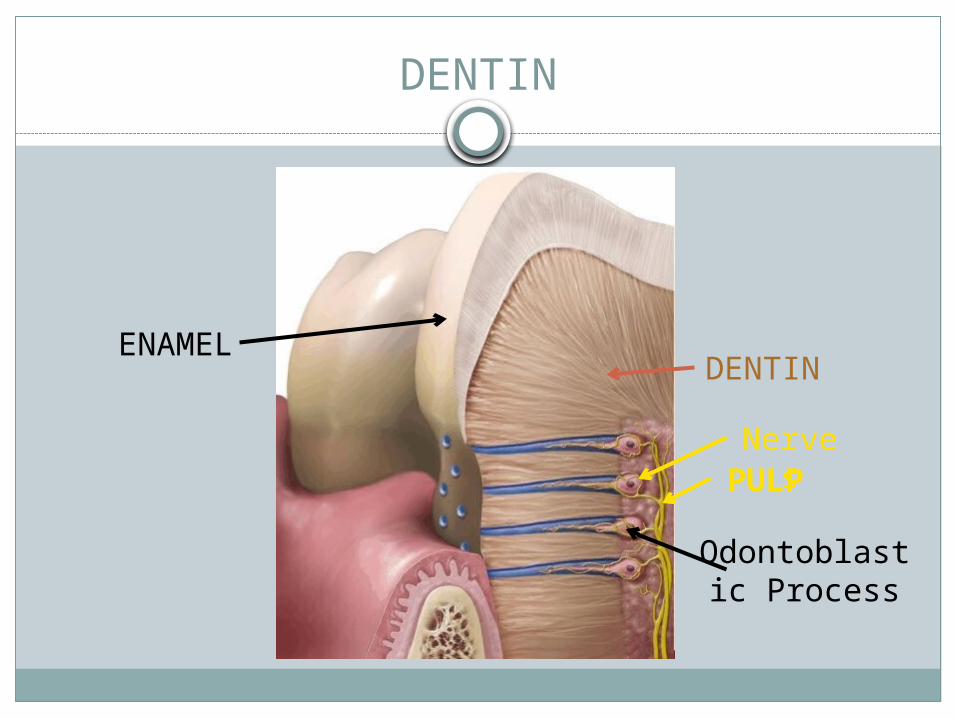
DENTIN
PULP
DENTINENAMEL
Odontoblastic Process
Nerves
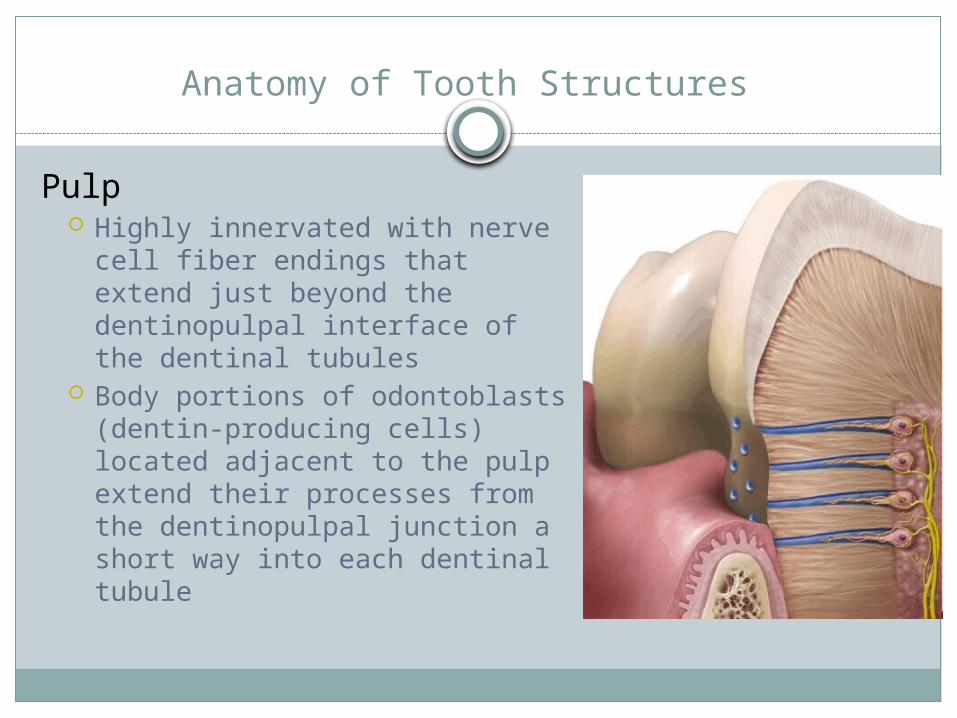
Anatomy of Tooth Structures
Pulp Highly innervated with nerve
cell fiber endings that extend just beyond the dentinopulpal interface of the dentinal tubules
Body portions of odontoblasts (dentin-producing cells) located adjacent to the pulp extend their processes from the dentinopulpal junction a short way into each dentinal tubule
Anatomy of Tooth Structures
Nerves Nerve fiber endings extend just beyond the
dentinopulpal junction and wind around the odontoblastic processes as shown in the next slide
Nerves react via the same neural depolarization mechanism (sodium potassium pump), which characterizes the response of any nerve to a stimulus
Objective #3: What Can Cause Dentin Exposure
Mechanisms of Dentin Exposure
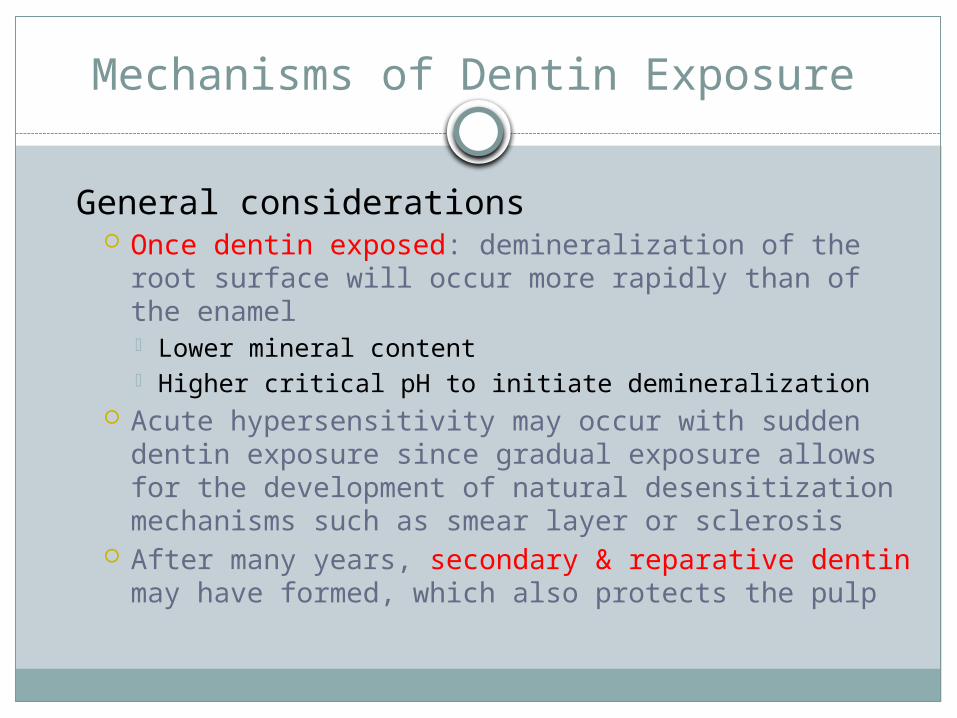
General considerations Once dentin exposed: demineralization of the root
surface will occur more rapidly than of the enamel Lower mineral content Higher critical pH to initiate demineralization
Acute hypersensitivity may occur with sudden dentin exposure since gradual exposure allows for the development of natural desensitization mechanisms such as smear layer or sclerosis
After many years, secondary & reparative dentin may have formed, which also protects the pulp
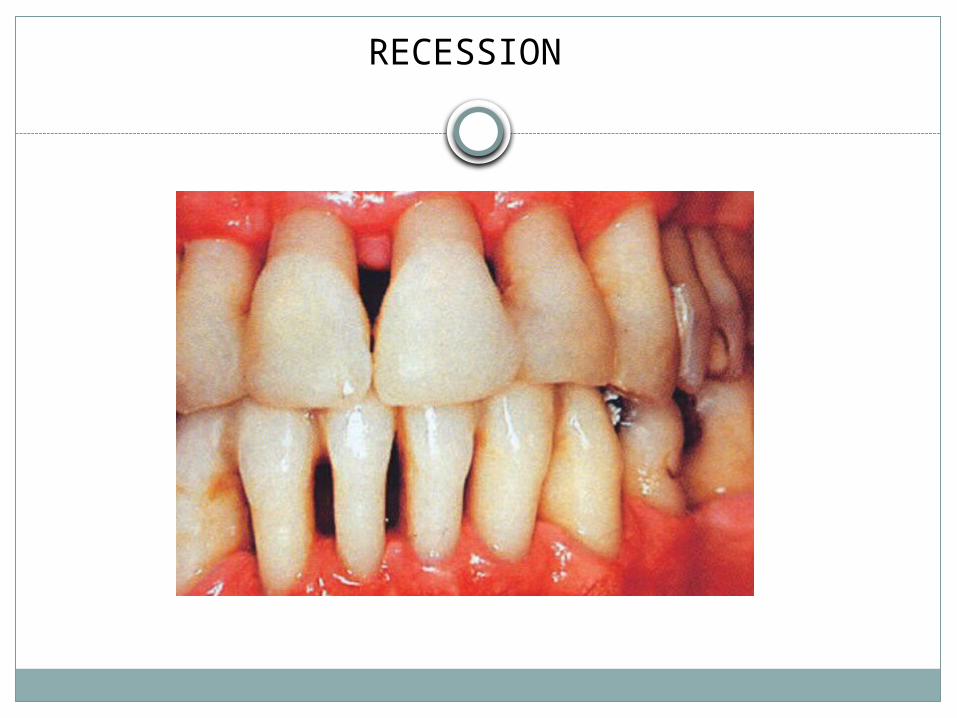
RECESSION
Factors Contributing to Gingival Recession & Root Exposure
Improper oral hygiene self-care Medium or hard toothbrushes Aggressive brushing Improper brushing motion
Anatomy and physiology of area Anatomically narrow zone of attached gingiva is more
susceptible to abrasion that can lead to recession and subsequent cemental exposure
Malocclusion Tight, short labial frena that pulls on gingival tissues
Subgingival instrumentation Large amts of sub-g calculus can pull gums away from
tooth and create recession May heal after removal
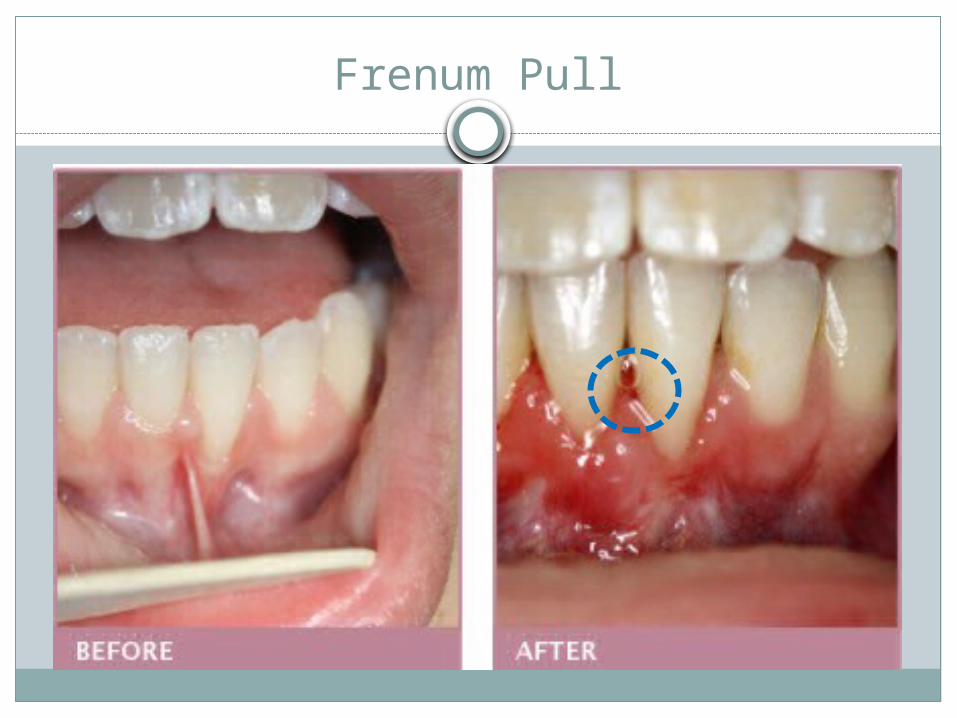
Frenum Pull
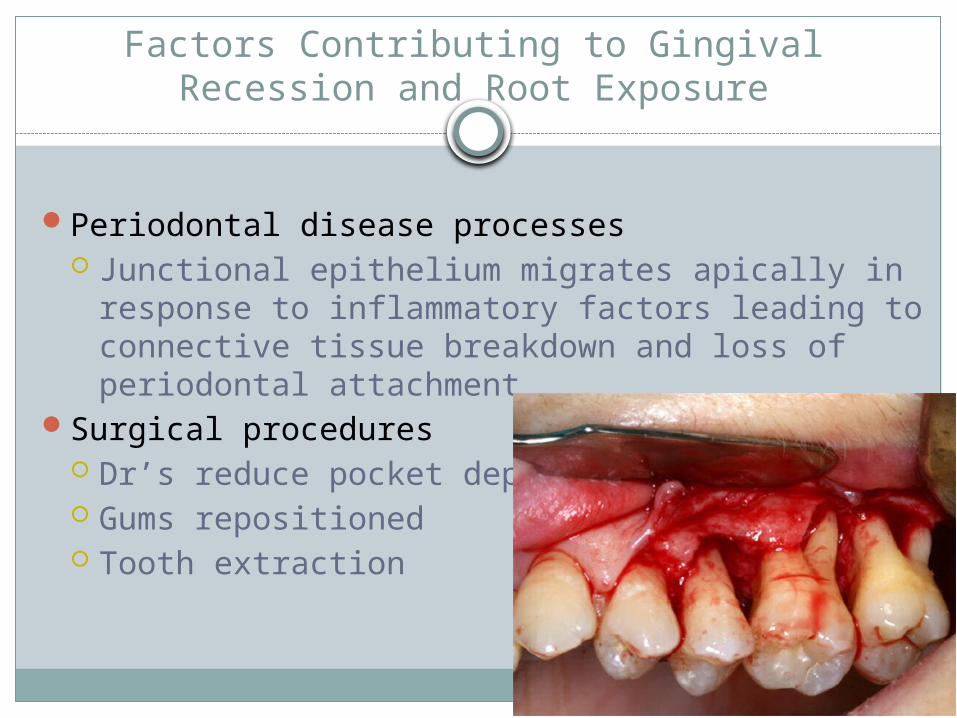
Factors Contributing to Gingival Recession and Root Exposure
Periodontal disease processes Junctional epithelium migrates apically in
response to inflammatory factors leading to connective tissue breakdown and loss of periodontal attachment
Surgical procedures Dr’s reduce pocket depths Gums repositioned Tooth extraction
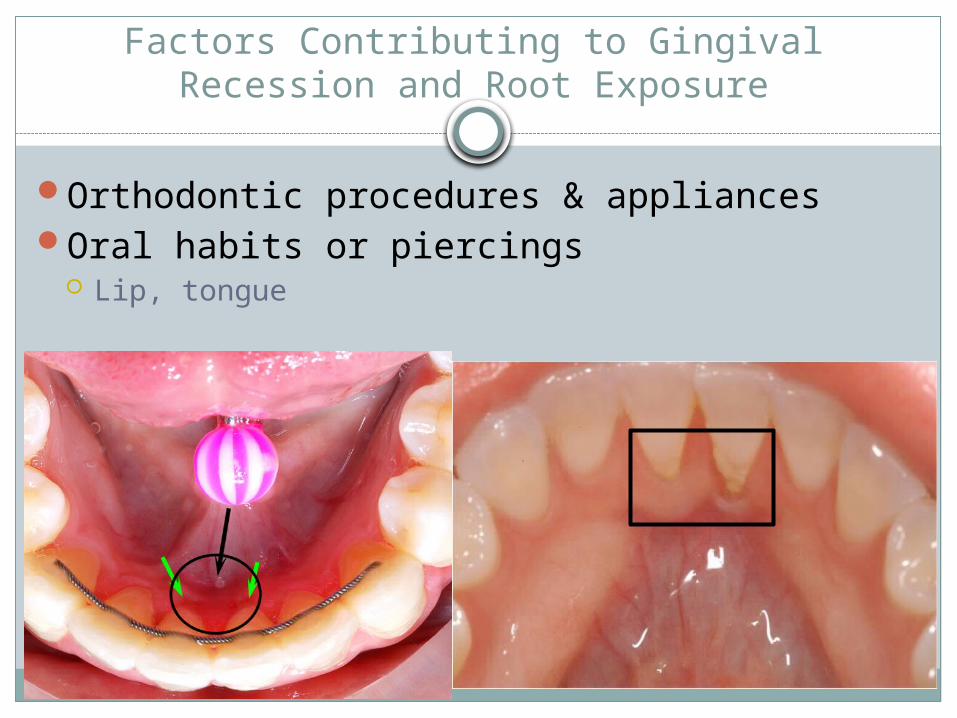
Factors Contributing to Gingival Recession and Root Exposure
Orthodontic procedures & appliancesOral habits or piercings
Lip, tongue
Factors Contributing to Loss of Enamel & Cementum
Anatomy of cervical area Thin and easily abraded when exposed Enamel and cementum do not meet at CEJ in about 10% of teeth
Occlusion Constant trauma to teeth When recession present & pt grinds – can cause abfractions
Attrition and abrasion Mechanical wear Clenching / Grinding
Erosion Chemical wear of teeth From diet such as high acids, citric acids, wine, sodas Bulimics

EROSION

ATTRITION
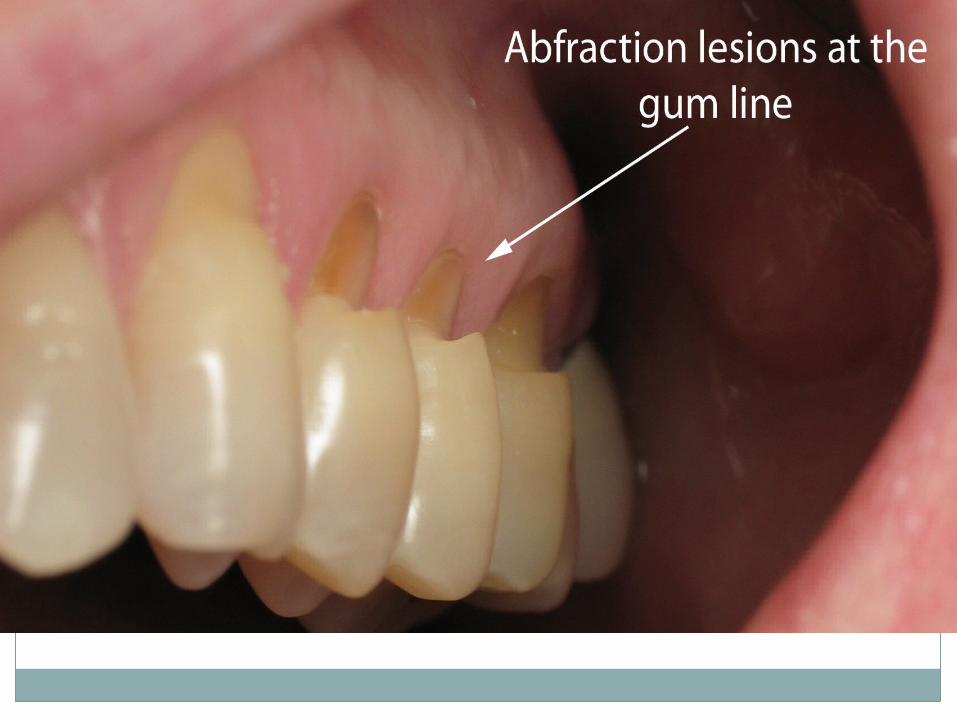
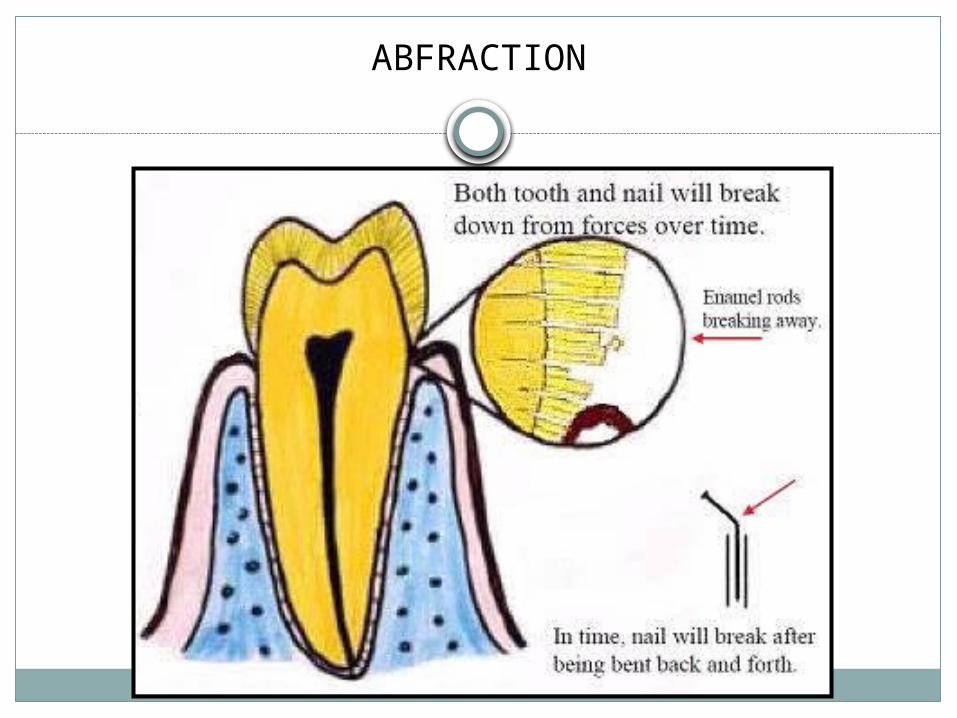
ABFRACTION
http://www.youtube.com/watch?v=yeMrp1OHiBg&list=TLiKey6xaSc-mx7C8gTGYWtcmG7kG3C0o8
Objective #4: Hydrodynamic Theory
Hydrodynamic Theory
Currently accepted explanation for transmission of stimuli from the outer surface of the dentin to the pulp
Developed by Brannstrom (1960s): theorized that a stimulus at the outer aspect of dentin will cause fluid movement within the dentinal tubules Fluid movement creates a pressure on the
nerve endings within the tubule Transmits pain impulses by stimulating the
nerves in the pulp
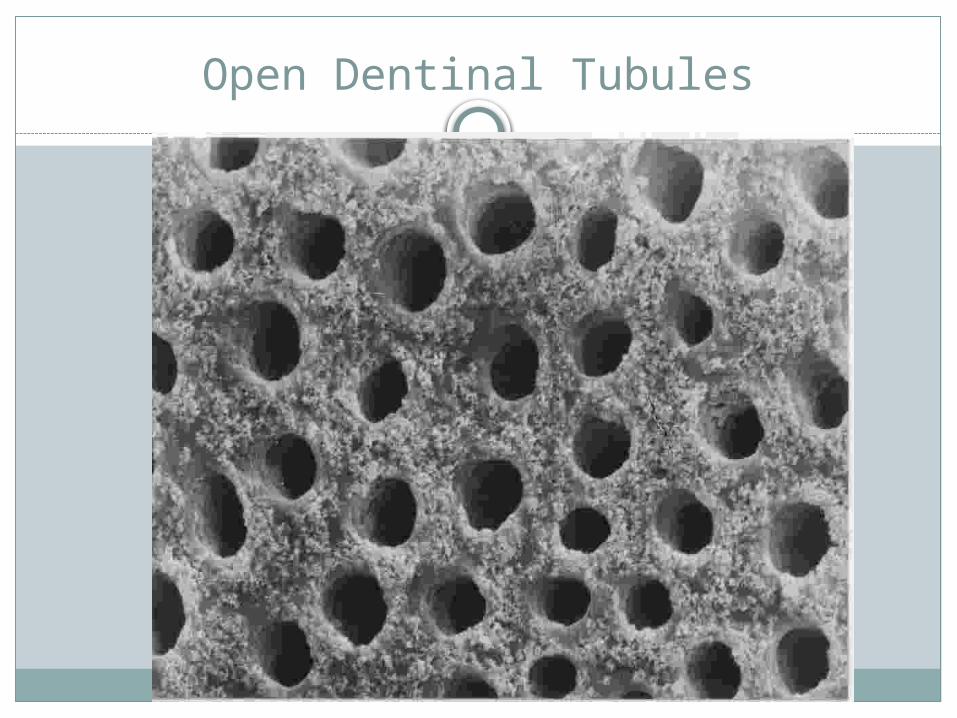
Open Dentinal Tubules
Hydrodynamic Theory
Explains the following Dentinal tubules exposed Pain-producing stimuli are present Pain-producing stimuli initiate the flow of
lymphatic fluid within dental tubules Odontoblasts and their processes act as
receptors and transmitters of sensory stimuli Movement of tubular fluids causes nerve
endings in the pupal wall to be stimulated & produce pain
Objective #5: Natural Desentization
1. Sclerosis of dentin (your oral embry book p.101 refers to this as tertiary dentin, reactionary/response, reparative dentin)
2. Secondary Dentin3. Smear layer4. Calculus
Natural Desensitization
1. Sclerosis of dentin (tertiary dentin) Occurs by mineral deposition within tubules
as a result of traumatic stimuli, such as attrition or dental caries
Creates a thicker, highly mineralized layer of peritubular dentin (deposited within the periphery of the tubules)
Results in a smaller-diameter tubule that is less able to transmit stimuli through the dentinal fluid to the nerve fibers at the dentinopulpal interface
Natural Desensitization
2. Secondary Dentin Deposited gradually on the floor and roof of the pulp
chamber after teeth are fully developed Secreted more slowly than primary dentin that formed
prior to tooth eruption: both types created by odontoblast
Creates a “walling off” effect between the dentinal tubules and the pulp to insulate the pulp from dentin fluid disturbances caused by a stimulus such as dental caries
As aging occurs, secondary dentin accumulates, resulting in a smaller pulp chamber with fewer nerve endings and less sensitivity
Natural Desensitization
3. Smear layer Consists of organic and inorganic debris that
covers the dentinal surface and the tubule Accumulates following scaling and root
instrumentation, use of toothpaste (abrasive particles), cutting with a bur, attrition, or abrasion
Occludes the dentinal tubule orifices forming a “smear plug” or “bandage” that blocks stimuli
May have a positive or negative effect It protects from hypersensitivity, but may
interfere with reattachment of periodontal tissues
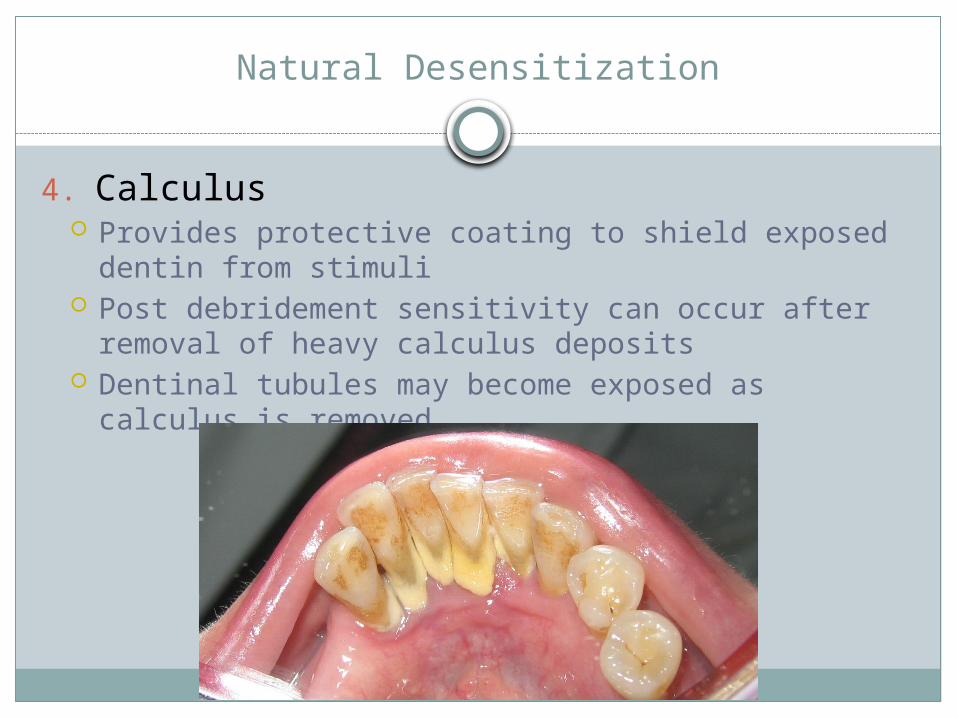
Natural Desensitization
4. Calculus Provides protective coating to shield exposed dentin
from stimuli Post debridement sensitivity can occur after removal
of heavy calculus deposits Dentinal tubules may become exposed as calculus is
removed
Patients and Their Pain
Dentinal Hypersensitivity Statistics Prevalence of hypersensitivity 8-30% of
adults Greatest age to be affected = 20-40yrs
Incidence decreases with increasing age = secondary dentin, sclerosis of dentin
Higher incidence in perio patients
Differential Diagnosis
Diagnostic techniques and tests Visual assessment of the tissues and teeth Palpitation both extra and intraoral Ask about sinus issues Occlusal exam: articulating paper Radiographic assessment: pulpal pathology? Vertical
root fracture? Percussion: use handle to tap on tooth to see if pain
elicited Mobility? Pain from biting: Bite Stick, cracked tooth Transillumination: cracked tooth Thermal/Electric tests on the pulp: Cold-Test
Question
After many years of root exposure, what structure can form that protects the root and pulp?
a. Primary dentinb. Secondary dentinc. Reparative dentin
Question
After many years of root exposure, what structure can form that protects the root and pulp?
a. Primary dentinb. Secondary dentinc. Reparative dentin
Objective: Desentization Products
Desensitizing Agents and Theorized Mode of Action: Mosby’s
Potassium salts Formulations containing potassium
chloride/nitrate/citrate/oxalate Reduce depolarization of the nerve cell membrane
and transmission of the nerve impulse by occluding dentinal tubules
OTCFluorides
Decrease the lumen diameter, block/occlude open dental tubules
Calcium phosphate technology Caries control to reduce demin and to remineralize by
releasing Ca, Phosphate ions for deposition of new tooth mineral (hydroxyapatite)
May occlude dentinal tubule openings
Desensitizing Agents and Theorized Mode of Action: Mosby’s
Oxalates Block open dental tubules Oxalate salts (potassium & ferric oxalate) decrease
the lumen diameterGlutaraldehyde
Can be combined with HEMA, a hydrophylic resin which seals tubules
Creates Ca-crystals w/in dentinal tubule to decrease the lumen diameter
Arginine and calcium carbonate Occlusal tubules using arginine (amino acid),
bicarbonate, Ca-carbonate Marketed as a px paste to be applied before
instrumentation
Types of Desentizing Tx
No single agent or form of tx is effective for all persons
Numerous agents have varying degrees of success Solutions, gels, pastes of fluoride in varying
compounds and % Adhesive, varnish, bonding materials Polymerizing agents
1. Glass ionomer cements (GIC)2. Adhesive resin primers3. Iontophorectic devises4. Laser therapy5. Restorations
Glass Ionomer Cements
Used in cervical abrasion and abfractionsSensitive area etched with 50% citric acidRinse with waterDryGlass ionomer placed
Adhesive Resin Primers
Reduce dentin permeability by occluding open tubules
Material rubbed on sensitive area for approximately 30 sec and air-dried
Iontophoretic Devises
Application of an electric current to impregnate tissues with ions from dissolved salts
Fluoride iontophoresis is thought to result in the increased uptake & penetration of fluoride ions into dentin
Devises are technique sensitive
Laser Therapy
One-time tx that reduces or eliminates dentin sensitivity
Seals tubulesSensitive dentin treated with laser is found to
be harder compared with untreated dentin
Restorations
Placed on surface where dentin is exposed to help reduce sensitivity
Unfilled or partially filled resins Covers patent dentinal tubules
Dentin-bonding agents Obturation of the tubule opening
Composite/glass ionomer
Soft Tissue Grafting
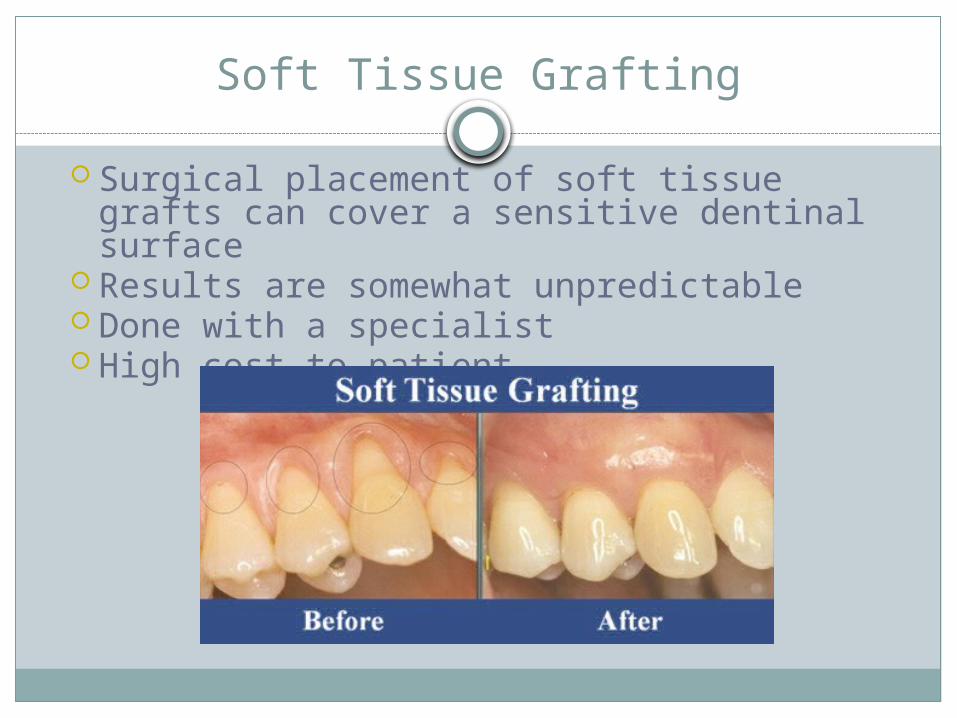
Surgical placement of soft tissue grafts can cover a sensitive dentinal surface
Results are somewhat unpredictable Done with a specialist High cost to patient
Behavioral Changes
Dietary modifications Limit acidic foods and beverages Evaluate use of dental products: no acid
formulations – can contribute to erosion Avoid hot/cold extremes in the mouth: no ice, coffee
not too hot…Excellent dental biofilm controlEval toothbrush type and techniqueEliminate parafunctional habits: mouthguard, ortho,
occlusal adjustmentsMedical referral for acid-reflux / GERD issues, Bulimia
suspectedAt home fluoride tx
FLUORIDE TRAY
Dental Professional Measures
Fluoride varnishes Does not require a dry tooth surface:
advantageous since this drying the tooth can be a painful procedure for a patient with dentin hypersensitivity
Novamin
Ca and Phosphate ions in ACP will seek out areas of demin and enhance enamel remin., occlude dentinal tubules, increase F uptake, prevent caries progression
High risk caries groups should usePeople w/ sensitivity should useShould be used in combo with FToothpaste, polish paste, sealant
Recaldent / Casein Phosphopeptides
Enhance the effects of Fluoride & provides a supersaturated environment of Ca and P for remin.
Not a Fluoride substituteHigh caries risk, sensitivity issuesCaries preventionGum, pastes, professional application
Additional Considerations
Tooth-whitening-induced sensitivity Commonly associated with carbamide peroxide A reversible pulpitis is caused from the dentin fluid
flow and pulpal contact of the material, which changes the osmolarity, without apparent harm to the pulp
Hypersensitivity = few days to several months Exposed dentin and pre-existing dentin
hypersensitivity increase risk for hypersensitivity secondary to whitening
Reduce tooth-whitening-induced sensitivity: Potassium nitrate, fluoride, or other desensitization product prior to & concurrently while whitening
Question
Novamin is made of which two ions:a. Calcium, phosphateb. Calcium, fluoridec. Phosphate, fluorided. Phosphate, Potassium
Question
Novamin is made of which two ions:a. Calcium, phosphateb. Calcium, fluoridec. Phosphate, fluorided. Phosphate, Potassium
Recommended