An Overview of Diabetes
Sid McNulty
Consultant Physician & Endocrinologist

Constructivism and Experiential learning and the brain
Sensory
IntegrativeMaking sense
IntegrativePlanning
‘Motor’(plus verbal)
Concrete experience
Active reflection
Abstract conceptualisation
Active experimentation

Neuronal networksTap into and build on what the learner already
knows
ACEi actions
K+ sparing
Diuretic
Antihypertensive
Postural hypotension
Insulin action Hypoglycaemia
Addison’sLack of RAAS driveLack of insulin antagonism
Cushing’s opposite of Addison’sand therefore opposite of:Insulin and diuretics, and therefore….
Blockage of RAAS

Diagnosis of Diabetes
WHO (adopted in UK 6/00):
Symptoms of hyperglycaemia plus 1 bloodRandom/2 hr plasma gluc > 11.1 mmol/l, or
Fasting plasma glucose > 7.0 mmol/l
In the absence of symptoms, there must be 2 plasma glucose results in the diabetic range on separate days.

Diagnostic dilemmaSensitivity: positives identified as positive
Specificity: negatives identified as negative
100% specificOver 10m longOver 15,000 mphOver 6,000 Km highNo false alarmsLots of false -ve
100% sensitiveOver 1m longOver 10mphOff the groundDon’t miss a strikeLots of false +ve

Lethal Disease XAffects 1 in 10,000100% fatal – horrible and painful deathFantastic test for it 99% (99% sensitive ie picks
up disease as disease, and 99% specific ie picks up normal as normal)
You have the test1 week later the resultsYou are positiveWhat is your probability you have disease?What do you do?

Please stand up

Condition
Positive Negative
TestResult
Positive True +ve False +ve +ve predictive valueTP/TP+FP
Negative False -ve True –ve -ve predictive valueTN/TN+FN
Sensitivity 99%TP/TP+FN x100
Specificity 99%TN/TN+FP x
100
A ‘Good’ Test

A ‘Good’ Test?

The Devil is in the detail!

Condition
Positive Negative
TestResult
Positive True +ve False +ve +ve predictive valueTP/TP+FP
Negative False -ve True –ve -ve predictive valueTN/TN+FN
Sensitivity 99%TP/TP+FN x100
Specificity 99%TN/TN+FP x
100
A ‘Good’ Test

What tests meansSensitivity: about the disease…the people you identify
with the disease/total number with the disease (TP/TP+FN)…if you have disease, you test positive
Specificity: about the disease…the people you identify without the disease/total number without the disease (TN/TN+FP)… if you don’t have disease you test negative
Positive predictive value: about the test…the number of people you test positive with the disease/total number you test positive (TP/TP+FP)… if you test positive, likelihood you have disease
Negative predictive value: about the test…the number of people you test negative without the disease/total number you test negative (TN/TN+FN)… if you test negative, likelihood you don’t have the disease

Gedankenversuch

Test: being called mags to diagnose being a woman
Male Female
True positive
Falsenegative
False positive
Truenegative
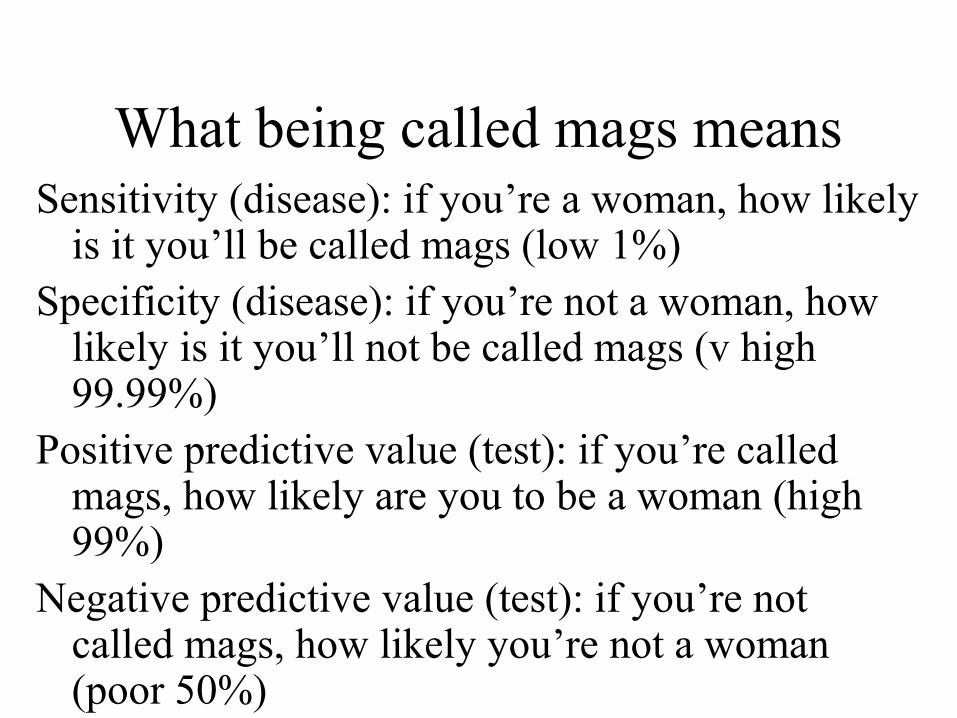
What being called mags meansSensitivity (disease): if you’re a woman, how likely
is it you’ll be called mags (low 1%)Specificity (disease): if you’re not a woman, how
likely is it you’ll not be called mags (v high 99.99%)
Positive predictive value (test): if you’re called mags, how likely are you to be a woman (high 99%)
Negative predictive value (test): if you’re not called mags, how likely you’re not a woman (poor 50%)

Lethal Disease XAffects 1 in 10,000100% fatal – horrible and painful deathFantastic test for it 99% (99% sensitive ie picks
up disease as disease, and 99% specific ie picks up normal as normal)
You have the test1 week later the resultsYou are positiveWhat is your probability you have disease?What do you do?

Please stand up, again

One million people1 in 10,000 with disease 1 in 100 with false +ve
1 in 10,000 with disease and +ve test ie 100 people
1 in 100 with +ve test and no diseaseie 10,000 people

One million peopleHow many have disease?1 in 10,000100 peopleHow many would test positive?1 in 10010,000If positive do you have disease? What is the positive predictive valueTP/TP+FP: 100/10,100ie 1 in 100 chance!Therefore – even the best test should be interpreted with clinical data, and should only be asked for in the right people (ETT ECGs, VQs etc etc)

What tests meansSensitivity: about the disease…the people you identify
with the disease/total number with the disease (TP/TP+FN)…if you have disease, you test positive
Specificity: about the disease…the people you identify without the disease/total number without the disease (TN/TN+FP)… if you don’t have disease you test negative
Positive predictive value: about the test…the number of people you test positive with the disease/total number you test positive (TP/TP+FP)… if you test positive, likelihood you have disease
Negative predictive value: about the test…the number of people you test negative without the disease/total number you test negative (TN/TN+FN)… if you test negative, likelihood you don’t have the disease

Incidence of Diabetes
The incidence is increasing steeply
World diabetic population is estimated to reach 221 million people by 2010 (double the number in 1994).
Over 1.4 million people in the United Kingdom (3% of the pop) have diagnosed diabetes mellitus, with perhaps another million as yet undiagnosed.
Amos AF et al.The rising global burden of diabetes...Diabetic Med 1997;14(suppl 5):S1-85.

Types of diabetes
Type 1 (IDDM)
Absolute insulin deficiency
ß-cell failure
Young, thin
Prone to DKA
Type 2 (NIDDM)
Relative insulin deficiency
Insulin resistance
Old, ↑BMI (kg/m2)
Usually on tablets or diet (can be on insulin)
No DKA : instead HONK
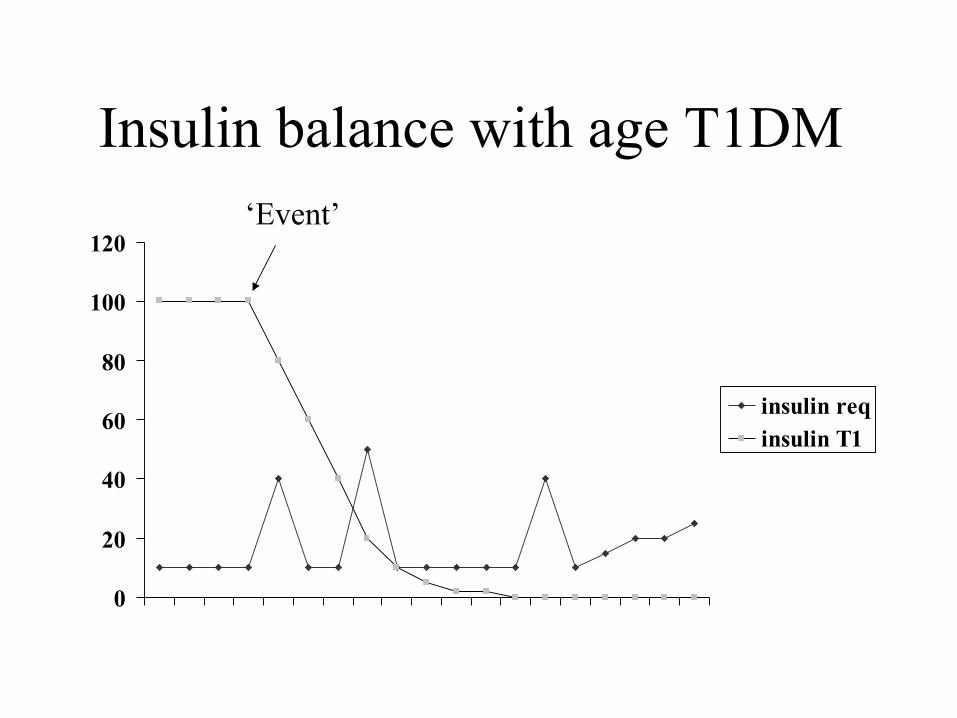
Insulin balance with age T1DM
0
20
40
60
80
100
120
insulin reqinsulin T1
‘Event’

Obesity and T2DM
Obesity
Inactivity
Insulin resistance
Hyperglycaemia
Micro- and macro-vascular complications
Hypertension
Dyslipidaemia
Endothelial dysfunction
Prothombotic state

The Progress to T2DM
Wt 70 kg
Requires 60 U
Panc Res 200 U
Level: 60 U
Normal
Wt 100 kg
Requires 150 U
PR 200 U
Level: 150 U
‘Normal’
Wt 70 kg
Requires 60 U
Panc Res 100 U
Level: 60 U
Normal
Wt 100 kg
Requires 150 U
Panc Res 100 U
Level: 100 U
DM & Hyperinsulin
NORMAL T2DM

12 v 121 v 1210 units?8 v 81 v 810 units/hr?
50 v 501 v 5010 units/50ml?
1010 units Actrapid at 100 mls/hr?

Insulin balance with age T2DM
0
20
40
60
80
100
120
insulin T1insulin T2

Insulin balance with age T2DM
0
20
40
60
80
100
120
insulin req0insulin T1insulin T2

Why worry with diabetic in-patients
Avoid emergencies:Main aim of your Mx
Plus tighten peri-operative glucose control

Diabetic emergencies
Hypoglycaemia
HyperglycaemiaDKA: Type 1
HHS/HONK: Type 2

HypoglycaemiaBMs 2-4
Autonomic symptoms: Sympathetic
Sweaty, agitated, nausea, shaky, pale, hungry
BMs 0-2
Neuroglycopenic:
Confusion, aggression, agitation, coma, hemiparesis etc

Mechanism of Normoglycaemia
β cell
Proinsulin
Insulin C Peptide
↓ Glucose
Pancreas
Pancreas
Glucagon Glycogen Liver
↑ Glucose
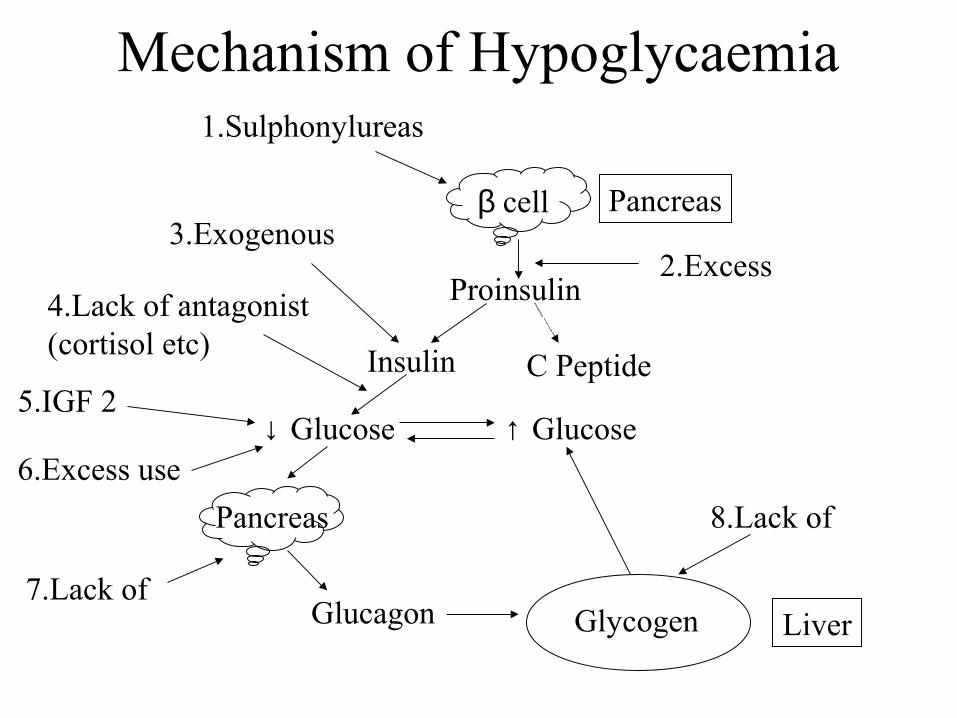
Mechanism of Hypoglycaemia
β cell
Proinsulin
Insulin C Peptide
↓ Glucose
Pancreas
Pancreas
Glucagon Glycogen Liver
↑ Glucose
1.Sulphonylureas
3.Exogenous
4.Lack of antagonist(cortisol etc)
5.IGF 2
6.Excess use
2.Excess
7.Lack of
8.Lack of

Treatment of HypoTreatment:
IV glucose 50ml 50%
IM glucagon 1 mg
?Treat causesteroids (Addison’s, NICTH)
surgery (Insulinoma, NICTH)
Diazoxide & high dose BFZ (Paliative Insulinoma)
DSN review/ Psych review

Presentation & definition of DKA
Young, thin, T1DM
Poly-uria, -dypsia, weight loss (passing sugar water)
SOB (kussmal - blowing off CO2 to ↓pH), dehydrated, ↓ BP, vasodilated, drowsy
Raised blood glucose (>15 mmol/L)
Metabolic acidosis:pH <7.3, Bicarb <15 mmol/L
Ketosis: ketostix > ++

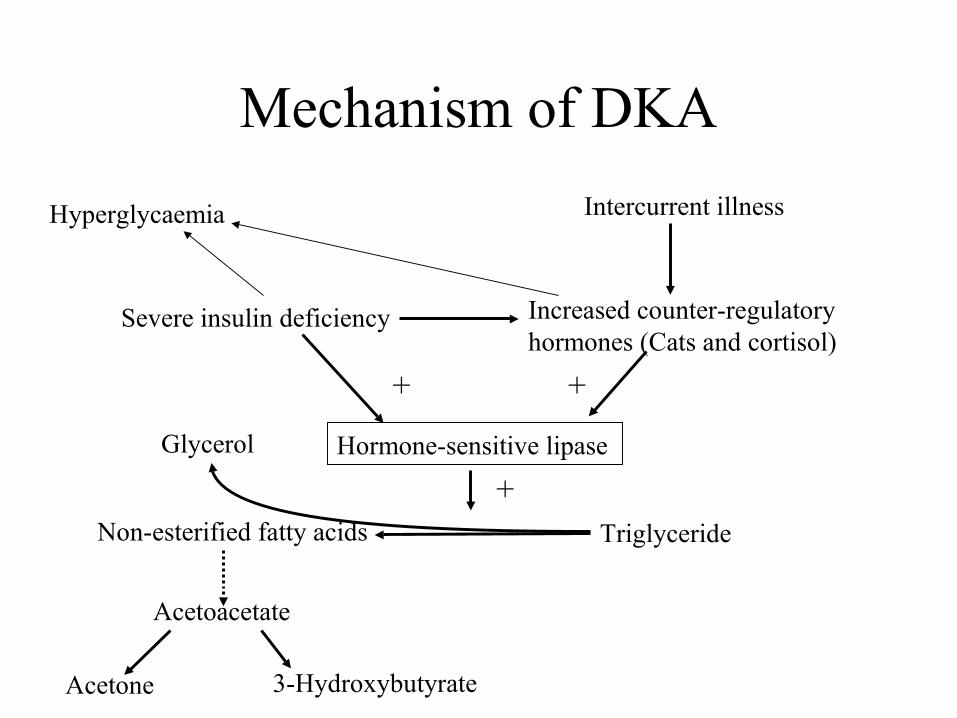
Mechanism of DKA
Intercurrent illness
Increased counter-regulatory hormones (Cats and cortisol)
Severe insulin deficiency
Hyperglycaemia

Mechanism of DKA
Hormone-sensitive lipase
TriglycerideNon-esterified fatty acids
Acetoacetate
3-HydroxybutyrateAcetone
Glycerol
+
Insulin
-
Mechanism of DKA
Intercurrent illness
Increased counter-regulatory hormones (Cats and cortisol)
Severe insulin deficiency
Hormone-sensitive lipase
TriglycerideNon-esterified fatty acids
Acetoacetate
3-HydroxybutyrateAcetone
Glycerol
+ +
+
Hyperglycaemia

Mechanism of DKA
Hyperglycaemia Ketone bodies
Osmotic diuresis Vomiting Acidosis
Electrolyte
depletionDehydration Vasodilatation
Hypotension Hypothermia

Management of DKA General
NG tubeReduced consciousnessGastroparesis
IV access? Central line only if indicated
Catheter?UTI may have precipitated DKADehydrated and immunosuppressedSerious risk of introducing ascending infectionTherefore only if not PU’d in 3 hours
Remove / treat precipitator (low threshold for Abs)?Heparin (coma or Osmolality >350 mOsm/L)

Management DKA SpecificT1DM
Acute decompensation
pH <7.3, Bicarb <15, Ketosis, Gluc >15
IV insulin 0.1 unit/kg/hr = 6-8 units/hr
IV fluids 5 Ltr/24hr
? Abs (WCC/Temp mean little)
No Bicarb
Inform your senior

13th May 2010
Died July 1997
Retired last year and still facing 12 charges!

HyperOsmotic NonKetotic Coma (AKA) Hyperglycaemic HyperOsmolar Syndrome
Presentation & DefinitionIn Type 2 DM
Longer Hx -poly-uria/dypsia
Dehydration, ↓BP, unwell
High RBG (usually >>30 mmol/L)
Osmolality >350
(Na+ + K+) x2 + Urea + Glucose = Osmol
Management of HHS SummaryT2DM, older, co-morbidity, more sick
Osmol > 350 mmol/Ltr
Gluc usually >>30 mmol/Ltr
Same general management as DKA
IV insulin 0.1 units/kg/hr = 6-8 units/hour
IV fluids 3-5 Ltr/24hr
Go more gentle!
?Full heparin dose
Abs, MI screen etc
Inform your senior

GKI/Alberti (to give insulin to T1DM)
15 units Actrapid
500 ml 10% Dextrose
10 mmol KCl
80-100ml/hour
If BMs high add another 5 units (and on)
If BMs low add 5 units less (and on)
Check K 1 hour before bag change
Restart sc insulin 1/2 hour before eating

Complications & DiabetesMicrovascular v Macrovascular
‘KNIVES’
K - kidneys
N - nerves
I - impotence, infection
V – vascular (IHD, CVA, PVD)
E - eyes
S - skin infections

Macrovascular risk factors
Male
Age
Family History
Other Vascular Disease:CVA, TIA
LVH
Diabetes
Hypertension
Lipids:↑Chol, ↑LDL, ↓HDL, ↑ TGs
Smoking
Obesity
Exercise

Diabetic complications
Prevention of complications
Risk reduction – relative versus absolute
Risk elimination
Residual risk

Intervention studies - Drug X
Reduces total chol 70%Reduces LDL 50%Increases HDL 10%Would you take it?
Surrogate markersLosing weight reduces cholLosing weight by losing legs
Reduces relative risk of MI 50%Would you take it?

Relative risk reduction
RR↓ 50%
RR↓ 50%
RR↓ 50%

Risk of AE Relative versus absolute risk
RR↓ 50%
Absolute risk reduction
Absolute risk reduction
Absolute risk reduction

Lies, damn lies and statistics6/49 x 5/48 x 4/47 x 3/46 x 2/45 x 1/44 =
720/10,068,347,520 =
1 in 13,983,816
Increase your relative risk by 100%
To 1 in 6,991,908
Absolute risk increase 1 in 13 million
Reduce your relative risk by 50%
1 in 27,967,632
Absolute risk reduction 1 in 13 million

Numbers Needed to Treat….
100 patients
10 events
100 patients
5 events
Relative risk reduction 50%
Treat 100 people, 5 events prevented, therefore treat 20 to prevent 1

This maybe all that we can offer you
1000 patients
10 events
1000 patients
5 events
Relative risk reduction 50%
Treat 1000 people, 5 events prevented, therefore treat 200 to prevent 1

Intervention studies - Drug X
Reduces total chol 70%Reduces LDL 50%Increases HDL 10%Would you take it?
Surrogate markersLosing weight reduces cholLosing weight by losing legs
Reduces relative risk of MI 50%Would you take it?Serious adverse event 1% per yearWould you take it?

What does risk reduction mean?
What was not going to happenWhen does this not happen
What did happenin spite of intervention..When did you cause this?
What didn’t happen with intervention…When does this not happenWhen did you prevent this?

RR reduction 50% with 20% side effects
What was not going to happenPlus SEPrimum non nocere First do no harm!
What did happenin spite of intervention..When did you cause this?Plus SE
What didn’t happen with intervention…When did you prevent this?Plus SE

Maximilien François Marie Isidore de Robespierre (May 6, 1758–July 28, 1794),
On ne peut pas faire d'omelette sans casser des oeufs
You can't make an omelette without breaking eggs
Primum non nocere

Risk of crossing the roadPark cars
Eyes closed
Heavy traffic
Run out
Pedestrian crossing
Wait for green man
Look both ways
Walk briskly don’t run
No guarantee to be or not be run over
NB you do get to the other side.The prevention of accident happens in definite time frame
Prevention of macrovascular complications
Primary prevention
All T2DM & most T1DM (10y risk <15%)
Tight glycaemic control (~UKPDS & DCCT)
Tight BP control (UKPDS)
Tight lipid management
Aspirin, ACE I/AT2A, smoking, BMI
Secondary prevention
Hx of CVA, MI, IHD, PVD, Amputation

Glycaemia in T2DM
HbA1c 2/12 marker (area under the curve)
Mean 5.4%, SD 0.4%
i.e. normal <6.2
HbA1c <7.5 <6.5

Normality
Mean1 SD
2 SDs3 SDs
68%
95%
99%

HbA1c: mean 5.4%, SD 0.4%
5.4% 6.2%
68%
95%
99.5%
7.0%4.6%
2.5% ‘normal population’
0.25%

Oral HypoglycaemicsMetformin (if BMI >24)
500 - 1000mg b.d - t.d.s
Side effects - GI….lactic acidosis
Contraindications - CRF, CCF, hepatic problems
No weight gain, no hypos
Gliclazide (if BMI <22)
40 - 320mg per day (od - bd)
Side effects weight gain & hypos
Glitazones (pioglitazone > rosiglitazone), acarbose etc

Hypoglycaemics
Incretins – Exanatide, gliptins
Insulins:
long v short
free v pre-mixed
human v pork v analogue
?CSII etc
Combination with OHA
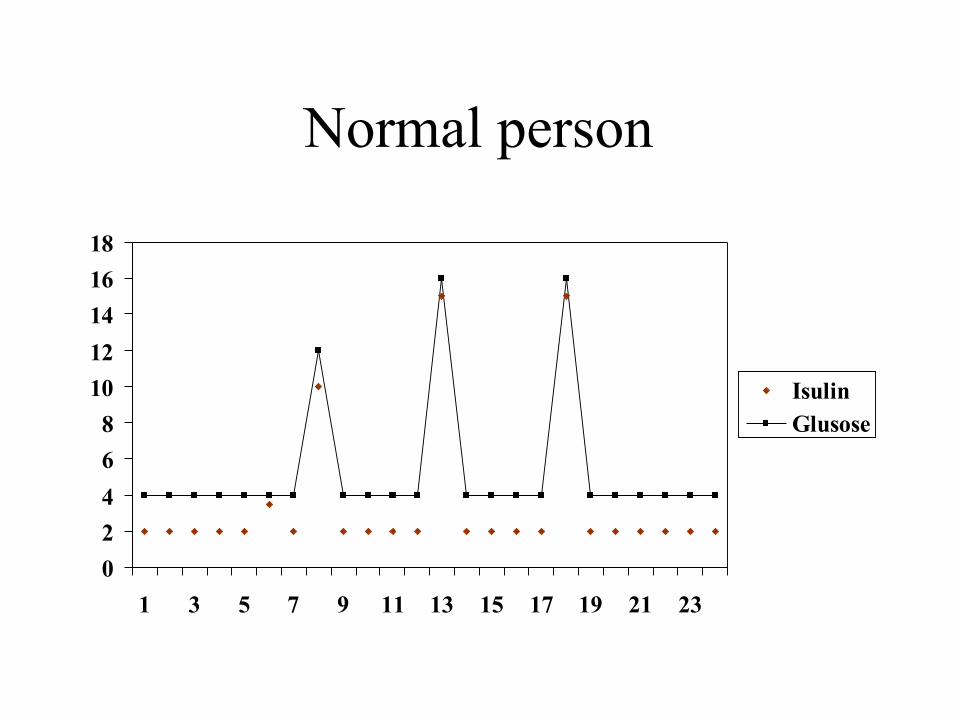
Normal person
0
2
4
6
8
10
12
14
16
18
1 3 5 7 9 11 13 15 17 19 21 23
IsulinGlusose

BD Mix
0
5
10
15
20
25
30
35
40
shortlong
7am 6pm
Breakfast
Lunch
Dinner
Snack

Basal Bolus
0
5
10
15
20
25
30
35
1 3 5 7 9 11 13 15 17 19 21 23
BasalBolus
am short
Lunch short
Dinner short
Evening background

Titrating Insulin-BD mix
BM reading Insulin
7 am Nocte long
Noon Mane short
6 pm Mane long
10 pm Nocte short

Titrating Insulin-Basal Bolus
BM reading Insulin
7 am Nocte basal
Noon Mane short
6 pm Noon short
10 pm Supper short

Lipid loweringDiet/lifestyle/co-morbid/smoking
CVS equivalent (or CVS risk >15%@10 yr)
LDL/Total Chol (>2.0/4.0) - Statins
HDL/Trigs (<1, >2.2) - ? Fibrates
Statins - Simva 40, Atova 40-80mg noctegood for total and LDL chol
Fibrates - Fenofibrate micro 267mg mane
good for trigs and HDL
Nicotinic acid - good for trigs and HDL
Ezetimibe - add on therapy, Omacor - post MI

ABCD tool

Anti-hypertensivesACE I/AT2A
Ramipril 2.5 - 10mg, Irebesartan 150 - 300mg
Partic if: CCF, IHD, MI, nephropathy, CVA
CI: pregnant, renovascular disease (watch Creat)
Thiazide diuretics (low dose!) - BFZ 2.5 mg o.d
β blockers - atenolol 50mg
Partic if MI, IHD, CCF
CCB - Amolidipine 5-10mg o.d
α blockers - Doxazosin XL 4-16mg (BPH)
Central acting etc

Microvascular Complications
Retinopathy
Nephropathy
Neuropathy
Erectile dysfunction

Prevention of microvascular complications
Primary prevention
Tighten control:
Glycaemia, BP, Lipids
Aspirin, ACE I, Anti Obesity
Secondary prevention
Catch & Treat early (as above, laser Rx etc)
Therefore screen for them
Funduscopy, feet inspection, urine & blood tests
Annual Screen
HbA1c/Lipids/Creat/BP/Wt
Alb:Creat Ratio
Feet - pulses, sensation (10g MF), ulcers
Eyes - dilated funduscopy, VAs
Kidneys - BP/ACR/Creat
Smoking status
Mx T2DM ConclusionsLifestyle: Smoking, Diet, Exercise & Weight
Annual screen for complications
Glycaemic control (UKPDS Metformin > Glic)
CVS Risk Calculation (>15%) v Equiv
Lipid controlLFD, Statin, ?Fibrates
BP controlACE I, ATII, Diuretics, β Blocker, CCB, other
Other drug Rx: Aspirin,?anti obesity,?anti smoking, ?HRT

Questions?
Recommended