
Causes of Hypomelanosis
CONT.

Other causes of Hypomelanosis1.Albinism2.Chédiak–Higashi syndrome3.Piebaldism4.Waardenburg syndrome5.Nevus depigmentosus6.Idiopathic Guttate Hypomelanosis7.Vogt–Koyanagi–Harada syndrome8.Phenylketonuria (PKU)

Albinism

Albinism• From Latin albus, meaning "white“.• DEFINITION: group of genetic disorders characterized by
diffuse pigmentary dilution due to a partial or total absence of melanin pigment within melanocytes of the skin, hair follicles and eyes.• Mostly autosomal recessive.• Absence of pigmentation from birth but normal number of
melanocytes are present within the epidermis.• The international average for albinism is about 1 in 20,000.• Sunburns, skin cancers are common.




An individual can be carriers of genes for albinism without exhibiting any
traits, albinistic offspring can be produced by two non-albinistic parents.



There are two main types of albinism:A. OCULOCUTANEOUS (OCA): Affecting the eyes, skin and hairpeople with this type of albinism have white or pink hair, skin, and iris color, as well as vision problems.Most severe type.B. OCULAR (OA): Hypopigmentation involving primarily the retinal pigment epithelium. person's skin and eye colors are usually in the normal range.
Types of Albinism

Eye affection in Albinism1.Translucent or light-colored eyes
due to reduced pigmentation in iris 2.Light sensitivity (photophobia)3.Reduced visual acuity or
functional blindness4.Reduced retinal pigmentation 5.Rapid eye movements (nystagmus)
Involuntary eye movements 6.Crossed eyes (strabismus)7.Hypoplastic foveae8.Lack of stereopsis /binocular vision


OCA1A
• White hair, milky white skin, and blue–gray eyes at birth. • Melanocytic nevi amelanotic.• The hair may develop a slight yellow
tint due to denaturing of hair keratins. • Extreme sensitivity to UV light and a
strong predisposition to skin cancer. • Reduced visual acuity is most severe,
and some patients are legally blind.

OCA1B1. “Yellow albinism” dt. the eventual color
of the patient’s hair (the formation of yellow pheomelanin requires less tyrosinase activity).
2. “Minimal pigment OCA”, 3. “Platinum OCA” 4. “Temperature-sensitive OCA”. The abnormal
tyrosinase enzyme is temperature-sensitive, losing its activity above 35°C. As a result, melanin synthesis does not occur in warmer areas of the body
• All of these patients have little or no pigment at birth, but they develop some pigmentation of the hair and skin during the first and second decades of life.
• The majority burn without tanning after sun exposure.• Some degree of iris translucency is often present. • Amelanotic or pigmented melanocytic nevi can
develop.

OCA2• Clinical spectrum is broad, ranging from
minimal to moderate pigmentary dilution of the hair, skin and iris.• Little to no ability to tan. • Pigmented melanocytic nevi and
lentigines may develop in sun-exposed areas.

OCA3• “Rufous” vast majority of OCA3
patients in individuals with type III–V skin color red–bronze skin color, ginger-red hair, and blue or brown irides. • “Brown” light brown skin, light brown
hair and blue–grey irides.

OCA4• Most common among individuals with
albinism who are from Japan (~25% of patients)• Hair color ranges from white to yellow–
brown.• Patients may or may not develop
increased pigmentation of the skin and hair over time.

OA1• Substantial reduction in visual acuity.• Hypopigmentation of the retina.• Presence of macromelanosomes in the eyes.• Affected boys have nystagmus, photophobia and foveal
hypoplasia. • Iris hypopigmentation with translucency.• Their skin is usually clinically normal without notable
pigmentary dilution.

Treatment of Albinism• There is no cure for albinism.• Treatments only ease the symptoms.• PHOTOPROTECTION: to avoid cutaneous
photocarcinogenesis, in particular the development of SCC;1. Large brimmed hat.2. Wear dark glasses.3. Always wear sunscreen SPF > 20.4. Special UV proof clothing/swimsuits.5. Sun avoidance during peak hours of UV
exposure.• VISUAL REHABILITATION: with longitudinal care as required. Glasses are
often prescribed to correct vision problems and eye position. Eye muscle surgery is sometimes recommended to correct nystagmus or strabismus.

Chédiak–Higashi syndrome(CHS)

CHS• Rare AR disorder characterized by;
1.OCA with a silvery-gray cast to the hair, photophobia, nystagmus and ocular hypopigmentation.
2.An admixture of hyper- and hypopigmentation may be evident in chronically sunexposed skin, especially in patients with relatively dark constitutive pigmentation.
3.Bleeding diathesis due to diminished function of platelet dense granules.
4.Progressive neurologic dysfunction.5.Severe immunodeficiency due to abnormal
lytic granules in lymphocytes, NK cells and neutrophils ( phagocytosis).
6.Accelerated phase, lymphoma-like-syndrome usually life-threatening in childhood.


CHS• A hallmark of the disorder is the
presence of giant lysosome-related organelles, including melanosomes, platelet dense granules and neutrophil granules. Examination of a peripheral blood smear for the latter represents a simple method of screening for this condition. • CHS is caused by mutations in the
lysosomal trafficking regulator gene (LYST), which encodes a cytoplasmic protein that regulates fission/fusion of lysosome-related organelles.


Treatment of CHS• There is no specific treatment.• Bone marrow transplants appear to have been
successful in several patients. • Infections are treated with antibiotics and abscesses
are surgically drained when appropriate. • Antiviral drugs such as acyclovir have been tried
during the terminal phase of the disease. • Cyclophosphamide and prednisone have been tried. • Vitamin C therapy has improved immune function and
clotting in some patients

Piebaldism

Piebaldism• Rare, AD with variable phenotype,
presenting at birth characterized by; poliosis and congenital, stable, circumscribed areas of leukoderma due to an absence of melanocytes within involved sites.• Mutations in the KIT proto-oncogene
(encodes a member of the tyrosine kinase family of transmembrane receptors). A functioning KIT receptor is required for the normal development of melanocytes, both immediately before melanoblast migration from the neural crest and postnatally.


C/P of Piebaldism• White forelock (~90%) triangular or
diamond-shaped, and often symmetrical. The apex can reach the vertex posteriorly, and the affected area may extend to the root of nose and include medial third of eyebrows.
• Poliosis of the eyebrows and eyelashes is a common finding.


C/P of Piebaldism• Leukoderma favors midline & static
and occur on the central anterior trunk, mid upper arm to wrist, mid-thigh to mid-calf, and shins classically spare the posterior midline (hands and feet are not usually affected) .
• Leukodermic patches are irregular, well-circumscribed and milk-white.
• Characteristic feature is the presence of normally pigmented or hyperpigmented islands within the areas of lack of pigmentation and on normal skin.




Tx of Piebaldism• Photoprotection.• Cosmetic camouflage.• Autografts of normal skin into amelanotic areas, same
techniques used in vitiligo.

Waardenburg syndrome (WS)

WS• Is a rare autosomal dominant or autosomal recessive disorder that is
characterized by various combinations of the following features:
1. Achromia of the hair, skin or both in the same pattern as Piebaldism.
2. Congenital deafness.3. Partial or total heterochromia
irides (including isohypochromia).4. Medial eyebrow hyperplasia
(synophrys).5. A broad nasal root.6. Dystopia canthorum (an increase
in the distance between the inner canthi, with a normal inter-pupillary distance).

Clinical Classification of WS
Type 1 Dystopia canthorumType 2 No dystopia canthorum
Type 3 Type 1 + upper limb abnormalities (e.g. hypoplasia, syndactyly)+ unilateral upper lid ptosis
Type 4 Type 2 + Hirschsprung disease







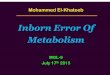
Nevus depigmentosus

Nevus depigmentosus• Pigmentary Mosaicism disorder.• Usually single hypopigmented patch at any site of body.• Stable areas of leukoderma are actually
hypomelanotic rather than amelanotic due to block in transfer of melanosomes from melanocytes to keratinocytes melanocyte count is overall stable with only a in melanin. • Most lesions measure a few centimeters in diameter
and have serrated irregular but well-defined borders, often breaking apart into smaller macules at periphery.• Configuration may be geographic, quasidermatomal
distribution or systematized (multiple streaks following the lines of Blaschko).• Can be distinguished from a nevus anemicus by diascopy.• Sporadic occurrence, no medical significance and no
treatment required assurance is sufficient.



Nevus depigmentosus: (a) Well demarcated hypopigmented macular patch on the flank. (b) Non-
inflammatory, no dermal pigment (H and E, ×100). (c) Epidermal hypomelanosis (Masson Fontana stain, ×100)

Idiopathic Guttate Hypomelanosis (IGH)

IGH• Very common acquired disorder of unknown
cause, but sun exposure probably plays a role.• Usually occurs after age 40 seen in up to 80% of
patients over the age of 70 years.• Occurs in all races and skin types, apparent
female predominance is due to perception of a cosmetic problem.
• Lesions occur on the shins and extensor forearms; are multiple usually small (0.5-8mm), and never occur on the face or trunk.
• Lesions are irregularly shaped and very sharply defined smooth porcelain white macules, and are only of cosmetic significance.
• Once present, they do not change in size or coalesce.
• Rx: Photoprotection / Cryotherapy or dermabrasion.



HP of IGH• Flattening of the dermal–
epidermal junction (most consistent histologic features). • Moderate to marked reduction or
focal absence of melanin granules in the basal and suprabasal layers.• Basket-weave hyperkeratosis. • There is a moderate to relatively
marked reduction in the number of DOPA-positive epidermal melanocytes (10–50% compared with normal skin), but these cells are never totally absent.

Vogt–Koyanagi–Haradasyndrome (VKHS)

VKHS
• Rare multisystemic disease involving various melanocyte-containing organs, such as eyes, meninges, central nervous system, skin, membranes, mucosa and inner ear.

Etiology of VKHS
• Unknown. An abnormal response to a virus, and immunological mechanisms, have been postulated.

Major features of VKHS






• Mainly affects dark-skinned people or white people with dark pigmentation. It is rare but widely distributed. • Most cases occur in the third and fourth decades but children may be
affected. It affects the skin, eyes, inner ears and meninges. • CRITERIA FOR DIAGNOSIS ARE AS FOLLOWS:
1.No history of ocular trauma or surgery preceding the initial onset of uveitis.
2.No clinical or laboratory evidence suggestive of ocular disease entities.3.Bilateral ocular involvement: an early sign is diffuse choroiditis; a late
sign is ocular depigmentation.4.Neurological findings: meningismus, CSF pleocytosis5.Auditory findings: tinnitus, labyrinthine deafness.6.Skin and hair changes: alopecia areata, vitiligo, poliosis.
• Typically, this condition is first diagnosed by ophthalmologists as the uveitis starts the march of symptoms and signs.
C/P of VKHS

Histologic examination VKHS
• Amelanotic skin (which often appears after the systemic symptoms) demonstrates absence of melanocytes + mononuclear infiltrate consisting primarily of CD4+ lymphocytes, suggesting a prominent role for cell-mediated immunity i.e. autoimmune disease, with the melanocyte, tyrosinase or tyrosinase-related protein as targets. Colloid–amyloid bodies are also found at the dermal–epidermal junction.

Phenylketonuria (PKU)

PKU• PKU is an inherited disorder that increases the levels of
phenylalanine in the blood.• Due to defective hepatic enzyme PHENYLALANINE
HYDROXYLASE (PAH) necessary to metabolize the amino acid phenylalanine ('Phe') to the amino acid tyrosine.



• Early diagnosis is essential because symptoms are not obvious in a newborn infant. • Mental retardation may develop gradually.• An early clue to the disease is lighter color of the
skin and hair than unaffected family members, eczema and a musty odor.
• Delayed mental and social skills.• Head size significantly below normal (microcephaly).• Hyperactivity.• Jerking movements of the arms or legs.• Seizures.• Skin rashes.• Unusual positioning of hands.
C/P of PKU


• PKU is normally detected using the HPLC test• Guthrie test: Devised by Dr. Robert Guthrie (1916 - 1995)
after the birth of his own child with PKU. The test has been widely used throughout North America and Europe as one of the core newborn screening tests since the late 1960s. • In recent years it is gradually being replaced in many areas
by newer techniques such as tandem mass spectrometry that can detect a wider variety of congenital diseases.
Dx of PKU

Guthrie test
A small drop of blood is taken from the heel of a newborn and applied to a card A small portion of the dried disc is incubated on a petri dish plated with Bacillus subtilis bacteria in the presence of a growth inhibitor, B-2-thienyl-alanine. The presence of high levels of Phe in the blood sample overcomes the inhibition, and allows the bacteria to grow.

Treatment



References
• Dr. Angelo Smith M.D WHPL• Mohammad Jafferany Ajyad general hospital Makkah.• Bolognia 3rd ed.• http://www.edoj.org• http://www.e-ijd.org• http://www.medscape.com• Google Images

THANK YOU
Recommended





![Studying Psychological Disorders - … Psychological Disorders: ... Schizophrenia (group of psychotic disorders) ... disorders.ppt [Compatibility Mode]](https://img.pdfslide.net/doc/110x75/5afbf38c7f8b9a444f8b7406/studying-psychological-disorders-psychological-disorders-schizophrenia.jpg)









