EDS – my first 50 years!
Rodney GrahameHonorary Professor UCL Unit for
Rheumatology & Connective Tissue Disease, University College London and the
London International Hypermobility Clinic
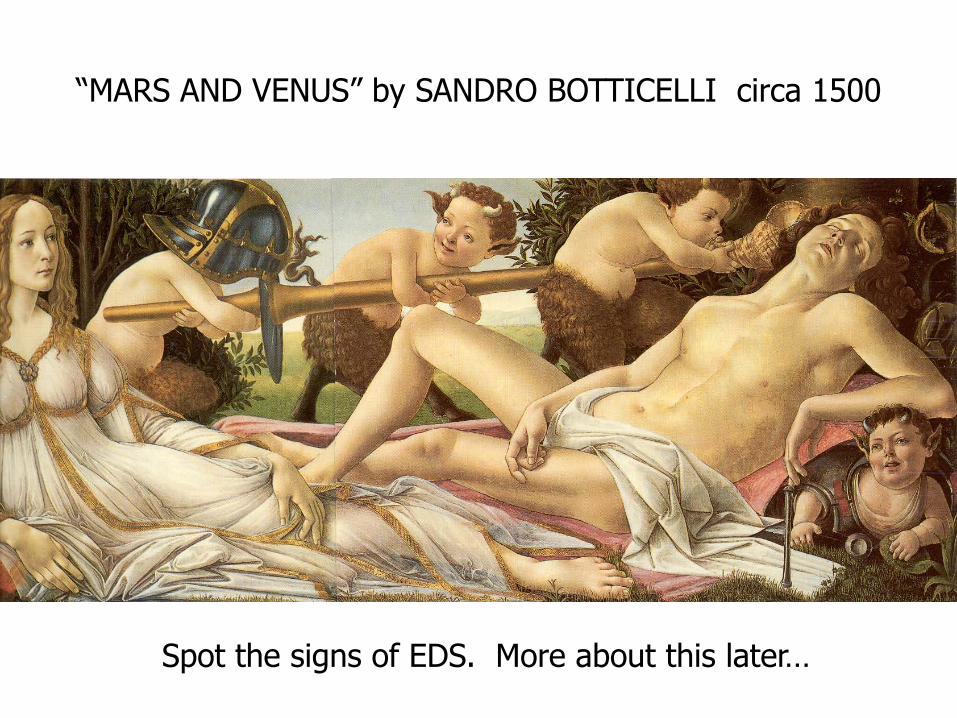
“MARS AND VENUS” by SANDRO BOTTICELLI circa 1500
Spot the signs of EDS. More about this later…






In the beginning…There were two diseases:
one for rheumatologists – JHSone for geneticists – EDS III
who rarely talked to one another!
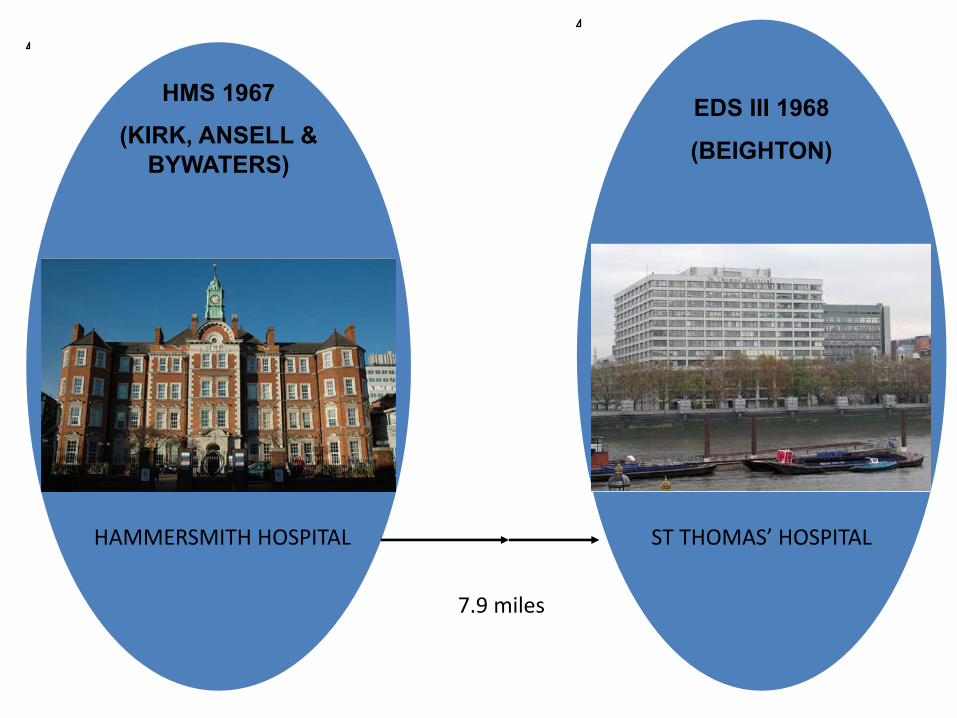
HMS 1967 (KIRK, ANSELL &
BYWATERS)
EDS III 1968 (BEIGHTON)
7.9 miles
HAMMERSMITH HOSPITAL ST THOMAS’ HOSPITAL

HMS 1967
(KIRK et al)
RHEUMATOLOGY
EDS III 1968
(BEIGHTON)
GENETICS
ERIC BYWATERSVICTOR McKUSICK

“THE HYPERMOBILITY SYNDROME”
“Musculoskeletal symptoms in the
presence of generalised joint laxity
in otherwise normal subjects”.

“THE HYPERMOBILITY SYNDROME”
“Another view is that isolated ligamentous laxity is a
mild mesenchymal developmental disorder which
lies at one end of a spectrum of heredofamilial
connective tissue disease with the fully-developed
picture of MFS or EDS at the other [Brown, Rowatt &
Rose 1966].

HMS 1967
(KIRK et al)
RHEUMATOLOGISTS
JOINTS
OVERLAP WITH HDCTs
BRIGHTON (1998)
ANXIETY & PHOBIAS (Bulbena 1988-)
AUTONOMIC DYSFUNCTION
(Gazit 2003)
GASTROINTESTINAL DYSMOTILITY (Zarate 2010)
EDS III 1968
(BEIGHTON)
GENETICISTS
GENETICS
HDCTs
BERLIN (1986)
VILLEFRANCHE (1997)
CHRONIC PAIN (Sacheti 1997)
AUTONOMIC DYSFUNCTION (Rowe 1999)
GASTROINTESTINAL DISORDERS
(Levy et al 1999)TINKLE et al 2009
‘INDISTINGUISHABLE FROM ONE ANOTHER’

Tinkle BT, Bird HA, Grahame R, Lavallee M, Levy HP, Sillence D. The lack of clinical distinction between the hypermobility type of Ehlers–Danlos syndrome and the joint hypermobility
syndrome (a.k.a. hypermobility syndrome).Am J Med Genet Part A 2009 149A:2368–2370.
• It is our collective opinion that BJHS/HMS and EDS hypermobility type represent the same phenotypic group of patients that can be differentiated from other HCTDs but not distinguished from each other.
• Clinically, we serve this population better by uniting the two diagnostic labels.With this approach, we can strive to better define the phenotype and improve measurable outcomes of this patient population.
• Furthermore, we recognize that it is important that, in those hypermobility patients who develop potentially debilitating symptoms of chronic fatigue or polyarthralgia, whatever the underlying cause, there should be prompt and appropriate intervention [Keer and Grahame, 2003].

There followed 40 years in the wilderness!

Changing Phenotype from 1967-2010
• We were seeing new co-morbidities appearing with bewildering frequency every 10 years.
• Difficulty in keeping pace with expanding phenotype.
• Handful of ‘EDS’ specialists.• Era of disbelief giving rise to denial and even
hostility emanating from colleagues in many specialties.
• Lack of treatment facilities.

MUSCULOSKELETAL PAIN/JOINT INSTABILITY
OVERLAP WITH HDCT/SKIN/HABITUS
UTERINE/RECTAL PROLAPSE
ANXIETY/PHOBIAS
DYSAUTONOMIAS
GI DYSMOTILITY
PROGRESSIVEDISABILITY
• 1967
• 1970
• 1980
• 1990
• 2000
• 2010
CHRONIC PAIN SYNDROME

MUSCULOSKELETAL PAIN/JOINT INSTABILITY
OVERLAP WITH HDCT/SKIN/HABITUS
UTERINE/RECTAL PROLAPSE
CHRONIC PAIN SYNDROME
DYSAUTONOMIAS
GI DYSMOTILITY
PROGRESSIVEDISABILITY
• 1967
• 1970
• 1980
• 1990
• 2000
• 2010
ANXIETY/PHOBIAS
CHIARI 1+
CRANIO-CERVICAL INSTABILITY
+TETHERED CORD
+LOW CSF PRESSURE
HEADACHE
2013MAST CELL ACTIVATION DISORDER
We wondered what was next…
Then something wonderful happened...
The Aims of Rehabilitation(After Anna Edwards-Fowler and Rosemary Keer)
developed from the 1980s• Reassurance, education and advice.• Improving spinal posture by developing core stability• Enhancing joint stability by encouraging joint-stabilising
exercises.• Improving joint proprioception by suitable exercises• avoiding resting in end-of-range (harmful) postures.• Manual therapy to restore normal (hyper) mobility. • Using pacing, coping and other behavioural strategies in severe
or widespread chronic pain.• Reversing deconditioning and enhancing fitness and stamina
by aerobic exercise.• Invoking self-management thereby restoring self-esteem and
self-efficacy.





Revised “1998 Brighton” diagnostic criteria for the Benign Joint Hypermobility Syndrome MAJOR CRITERIA MINOR CRITERIA
• Beighton score > 4/9 or (currently/historically)
• Arthralgia > 3 months in >4 joints
• Beighton score of 1,2, 3/9 (0, if aged 50+)
• Arthralgia in 1-3 joints/ back pain/spondylosis/ spondylolysis/’olisthesis.
• Dislocation in >1 joint, or in 1 joint on >1 x
• > 3 soft tissue lesions• Marfanoid habitus • Skin: striae, thin,
stretchy, abnormal scarring.
• Eye signs: drooping eyelids or myopia
• Varicose veins/hernia/ uterine/rectal prolapse
The BJHS is diagnosed with:2 major criteria or 1 major and 2 minor criteria or 4 minor criteria. 2 minor + 1° degree relative.
BJHS is excluded by presence of Marfan or Ehlers-Danlos syndromes (other than the EDS Hypermobility type formerly EDS III) as defined by the Ghent 1996 and Villefranche 1998 criteria respectively
Estimates of Misdiagnoses• Each consultant is actually seeing 224 JHS pts/yr.• Estimated 119,809 NEW JHS patients attending clinics annually.• Consultants estimate 5,600 NEW JHS patients attending their
clinics annually [10 EACH].• 119,809 JHS patients unrecognised p.a.• Equivalent to 94.52%.• Only 4.67% are being recognised.
“For every single patient in England with joint hypermobility syndrome fortunate enough to be
correctly diagnosed by a rheumatologist, there are 19 others who are not, passing unnoticed, undiagnosed
and presumably, untreated.”
Unique in the history of medicine• Medical students generally not taught about it.• Teachers of medical students don’t teach it.• Doctors in general tend not to know about it.• Rheumatologists still follow concepts of 1970s (comfort zone).• Most therapists not trained to treat it.• Epidemiologists have chosen to ignore it.• Research funding bodies rarely support it.• Patients better informed than their doctors.• Patients are left to their own devices.• No other disease is neglected in this way.

ADULT RHEUM
PAED RHEUM
PAEDS GENERAL
GASTRO
AUTONOMIC
CV-MED
URO- GYNAECOLOGY
NEURO-RADIOLOGY
NEUROSURGERY
PHYSIOTHERAPY
OCCUPATIONAL THERAPY
PODIATRY
PAIN PSYCHOLOGY
RHEUMATOLOGY NURSE
ORTHOPAEDICS OBSTETRICS PLASTIC SURG CARDIOLOGY NEUROLOGY SPORTS MED
PAIN MEDICINE ENDOCRINEetc.CLINICAL GENETICS
RESARCH TRAINING
Multi-Specialty Care

LEEDS
GLASGOW (RHEUMATOGY)
LEEDS (REHABILITATION)
BATH (RHEUMATOLOGY/REHABILITATION) – OPEN
LONDON (NEXT SLIDE)
GLASGOW
BATHLONDON
Closure of UK’s EDS Facilities

READAPTATION INTENSIVE/CHIRURGIE ORTOPEDIQUE
GENETIQUE SED- TYPES RARES
GASTROENTEROLOGIE –ADULTE & ENFANTS
KINESITHERAPIE -ENFANTS
DYSAUTONOMIEDOULEUR
Specialist Services for EDS
RHUMATOLOGIE;DOULEUR

MIS-DIAGNOSES
ADULTS CHILDREN
• FIBROMYALGIA• OSTEOARTHRITIS• SERONEGATIVE ARTHROPATHY• PSYCHOGENIC RHEUMATISM• DEPRESSION• CHRONIC FATIGUE SYNDROME
• CONGENITAL HYPOTONIA• LAZINESS• SCHOOL PHOBIA• DYSFUNCTIONAL FAMILY• FABRICATED OR INDUCED ILLNESS
[(FII) aka MUNCHAUSEN’S SYNDROME BY PROXY]

‘It isn’t that they can’t see the solution.It is that they can’t see the problem.’
GK Chesterton



“MARS AND VENUS” by SANDRO BOTTICELLI circa 1500

Watch this space
Next Instalment August 4 2068 : EDS My Second 50 Years!

Thank you!
Recommended

















