5/10/2018 Emergency Care Nursing - slidepdf.com
http://slidepdf.com/reader/full/emergency-care-nursing-55a0bf3cdadc5 1/14
BANDAGING
Bandaging is both a science and an art. The proper bandage, properly applied, can
aid materially in the recovery of the patient. A carelessly or improperly applied bandage can
cause discomfort to the patient and may imperil his life. Thus, it is important that enlisted
men of the Medical Department should become familiar with the various bandages and be
able to apply them properly. The following pages will aid the student and the teacher; but the
art of bandaging can be mastered only by constant practice.
USE OF BANDAGES
Bandages are employed to hold dressings, to secure splints, to create pressure, toimmobilize (make immovable) joints and in correcting deformity. Bandages should never be
used directly over a wound. They should only be used over a dressing.
- To support fractured bones
- To immobilize dislocated shoulder or jaw
- To apply pressure, stop bleeding and improve venous blood flow
- To secure dressing in place
- To retain splints in place
PRINCIPLES AND PRCEDURES
- Wash hands(wear gloves when necessary)
- Assist to assume comfortable position on bed or chair and support the body part to
be bandaged.
- Always stand in front of the part/victim to be bandaged except when applying a
bandage to the head, eye and ear.
- Be sure the bandage is rolled firmly.
- Make sure the body part to be bandaged is clean and dry.
- Assess skin before applying bandage for any breakdown.
- Observe circulation by noting pulse, surface temperature, skin color and sensation
of the body part to be wrapped.
- Always start bandaging from inner to outer aspect and far to near end.
When bandaging a joint, ensure flexibility of the joint. (Except immobilization of joint
is required)
- Always start and end with two circular turns.
- Cover the area 2 inches above and 2 inches below the affected area
- Overlap turns and slightly stretch the bandage.
- Cover 2/3 of the previous turn.
- Where possible, leave fingertips or toe tips exposed for observation(adequacy of
blood circulation)
- End the bandage on the outer side of the body. Do not end bandage on wound or at
the back of the body.
TYPES OF BANDAGES
1. Triangular bandage
-could be used on many parts of the body to support and immobilize.
2. Crape Bandage
-type of woven gauze which has the quality of stretching.
3. Gauze/cotton bandage
-lightly woven cotton material. Frequently used to retain dressings fingers,
hands, toes, feet, ears, eyes, head.
4. Adhesive bandage
-used to retain dressing and also used where application of pressure to an area is
needed.
METHODS OF APPLYING BANDAGES
- Circular
- Spiral
- Spi ra l Reverse
- Figure of E ight
- Recurrent
-
I. CIRCULAR TURN

5/10/2018 Emergency Care Nursing - slidepdf.com
http://slidepdf.com/reader/full/emergency-care-nursing-55a0bf3cdadc5 2/14
Purpose: Used chiefly to anchor bandages and to terminate bandages. Usually are not
applied directly over a wound because of the discomfort the bandage would cause.
1. Hold the bandage in your dominant hand, keeping the roll uppermost, and unroll the
bandage about 8cm. This length of unrolled bandage allows good control for
placement and tension.
2. Apply the end of the bandage to the part of the body to be bandaged. Hold the end
down with the thumb of the other hand.
3. Encircle the body part a few times or as often as needed, making sure that each
layer overlaps ½ -2/3 of the previous layer. This provides even support to the area.
4. The bandage should be firm, but not too tight. Ask the client if the bandage feels
comfortable. A tight bandage can interfere with blood circulation, whereas a loose
bandage does not provide an adequate protection.
5. Secure the end of the bandage with tape or a safety pin over an uninjured area. Pins
can cause discomfort when situated over an injured area.
II. SPIRAL TURNS
Purpose: Used to bandage parts of the body that are fairly uniform in circumference, for
example, the upper arm or the upper leg.
1. Make two circular turns. Two circular turns anchor the bandage.
2. Continue spiral turns at about a 30 degree angle, each turn overlapping the
proceeding one by 2/3 the width of the bandage.
3. Terminate the bandage with 2 circular turns and secure the end as described for
circular turns.
III. SPIRAL REVERSE TURNS
Purposes: Used to bandage cylindrical parts of the body that are not uniform in
circumference, for example, the lower leg or forearm.
1. Anchor the bandage with 2 circular turns, and bring the bandage upward at about a
30 degree angle.
2. Place the thumb of your free hand on the upper edge of the bandage. The thumb
will hold the bandage while it is folded on itself.
3. Unroll the bandage about 15cm (6 inches), and then turn your hand so that the
bandage falls over itself.
4. Continue the bandage around the limb, overlapping each previous turn by 2/3 the
width of the bandage. Make the bandage turn at the same position on the limb so
that the turns of the bandage will be aligned.
5. Terminate the bandage with 2 circular turns and secure the end as described for
circular turns.
IV. RECURRENT TURNS
Purposes: Used to cover distal parts of the body, for example, the ends of a finger, the skull
or the stump of an amputation.
1. Anchor the bandage with two circular turns,.
2. Fold the bandage back on itself, and bring it centrally over the distal end to be
bandaged.
3. Holding it with the other hand, bring the bandage back over the end to the right of
the center bandage but overlapping it 2/3 the width of the bandage.
4. Bring the bandage back to the left side, also overlapping the first turn by 2/3 the
width of the bandage.
5. Continue this pattern of alternating right and left until the area is covered. Overlap
the preceding turn by two-thirds the bandage width each time.
6. Terminate the bandage with two circular turns. Secure appropriately.
V. FIGURE 8 TURNS
Purposes: Used to bandage an elbow, knee or ankle, because they may permit some
movement after application.
1. Anchor the bandage with two circular turns.
2. Carry the bandage above the joint, around it and below it, making a figure eight.
3. Continue above and below the joint, overlapping the previous turn by two-thirds the
width of the bandage.
4. Terminate the bandage and above the joint with two circular turns and then secure
appropriately.
TRIANGULAR AND CRAVAT BANDAGES
The triangular bandage, also known as the handkerchief bandage, is used for the
temporary or permanent dressing of wounds, fractures, dislocations, etc., and for slings. It is
very valuable in first-aid work since it is quickly and easily applied, stays on well, and can be

5/10/2018 Emergency Care Nursing - slidepdf.com
http://slidepdf.com/reader/full/emergency-care-nursing-55a0bf3cdadc5 3/14
improvised from any kind of cloth, such as a piece of a shirt, an old sheet, a large
handkerchief, etc. Unbleached muslin is generally used in making triangular bandages,
although linen, wool, silk; etc., will answer the purpose. In making triangular bandages a
square of material about 3 by 3 feet, or slightly more, is folded diagonally to make one
bandage or may be cut along the fold to make two bandages. The long side of the triangle is
called the "base," the point opposite the base is called the "apex", and the points at each end
of the base are called the "ends" or "extremities." These bandages may be used either as a
triangle or as a cravat, the latter being made from the triangle by bringing the apex to the
base and folding it upon itself a sufficient number of times to obtain the width desired. The
names of the-various triangular and cravat bandages indicate the part of the body to which
the bandage is applied.
PROCEDURES
I. TRIANGLE OF FOREHEAD OR SCALP (fronto-occipital)
- Used to retain dressings on the forehead or scalp.
1. Place middle of base of triangle so that edge is just above eyebrows and bring apex
backward, allowing it to drop over back of head (occiput).
2. Bring ends of triangle around to back of head, above ears, and cross them over apex
at occiput.
3. Carry ends around to forehead and tie them in square knot.
4. Turn up apex of bandage toward top of head. Pin with safety pin or tuck in behind
crossed part of bandage.
II. TRIANGULAR ARM SLING (brachio-cervical triangle)
-Used for fractures or injuries of hand, wrist, and forearm.
1. Arm to be put in sling should first be bent at elbow so that little finger is about a
hand's breadth above level of elbow.
2. Drop one end of triangle over shoulder on injured side and let bandage hang down
over chest with base toward hand and apex toward elbow.
3. Slip bandage between body and arm. Carry lower end up over shoulder on injured
side.
4. Tie the two ends, by square knot, at back of neck. Knot should be on either side of
neck, not in middle, where it could cause discomfort when patient is lying on back.
5. Draw apex of bandage toward elbow until snug, bring it around elbow to front, and
fasten with safety pin or adhesive tape.
III. TRIANGULAR ARM SLING
- Another version of this sling is frequently used where it is desirable to support the
forearm, without pressure on the collarbone or shoulder of the injured side.
2. Start as in (1).
3. and pass lower end of bandage under injured shoulder. Ends of fingers shouldextend slightly beyond base of triangle.
4. Tie ends. Secure apex to sling at elbow by tucking in or with safety pin.
IV. SHOULDER-ARMPIT
- (bis-axillary) Used to hold dressings in the armpit (axilla) or on the shoulder.
1. Place middle of cravat in armpit over dressing.
2. Carry ends upward and over top of shoulder.
3. Cross ends lnd bring them across back and chest respectively to opposite armpit
where they are tied.
V. TRIANGLE OF CHEST OR BACK
- Used to retain dressings on burns or wounds.
1. Drop apex of triangle over shoulder on injured side. Bring bandage down over chest
(or back) to cover dressing and so that middle of base of bandage is directly below
injury. Turn up a cuff at base.
2. Carry ends around body and tie in square knot.
3. Bring apex down and tie to one of ends of first knot.
VI. TRIANGLE OF SHOULDER
- Used to retain dressings on shoulder. Requires two bandages, one a triangle, and the
other a cravat.
1. Place center of cravat at base of neck on injured side, and tie just forward of
opposite
armpit.
2. Place apex of open triangle under cravat at base of neck and over dressing on
injured
shoulder and upper arm.
3. Tuck apex under cravat at neck.
4. Cross ends of base and tie around arm; secure apex to cravat at neck by tucking in
6r
with safety pin.
VII. TRIANGLE OF FOOT
- Used to retain dressings of considerable size on the foot.
1. Center foot upon bandage at right angles to base. Heel should be well forward.
2. Carry apex of triangle over toes, and cover back of foot to ankle.
3. Tuck excess fullness of bandage into small pleats on both sides of foot.
4. Cross each half of bandage toward opposite sides of ankle. Bring ends of triangle
around ankle. Tie ends in square knots.
VIII. TRIANGLE OF HAND
- Used to retain dressings of considerable size on the hand.
1. Place middle of base of triangle well up on palmar surface of wrist.
2. Carry apex around ends of fingers and cover back (dorsum) of hand to wrist.
3. Tuck excess fullness of bandage into small pleats on both sides of fingers.
4. Cross each half of bandage toward opposite sides of wrist.
5. Bring ends of triangle around wrist.
6. Tie ends in square knot.
FOLDING TRIANGULAR BANDAGES
- for storage and shipment
1. Bandage unfolded.
2. Fold once left to right.
3. Fold ends right to left.

5/10/2018 Emergency Care Nursing - slidepdf.com
http://slidepdf.com/reader/full/emergency-care-nursing-55a0bf3cdadc5 4/14
4. Fold apex down to form square.
5. Fold in half, right to left.
6. Fold down through center
Cravat Bandaging
A triangular bandage can be folded into a strip for easy application during emergencies.
CRAVAT FOR HEAD OR EAR
INDICATION: The purpose of this bandage is to apply pressure to control hemorrhage from
wounds of scalp, or to hold dressings on wounds of ear or lower scalp. (Applied when thevictim has wound on the forehead)
1. Cover the wound with a dressing and place the middle of the bandage over the
wound as illustrated below.
2. Cross both ends of the bandage and gently pull and wrap them in opposite
directions around the head as illustrated.
3. As illustrated below, tie both ends in square knot, making sure that it is fully tight.
CRAVAT FOR JAW OR CHEEK
INDICATION: The cravat of jaw (mento-vertico-occipital cravat) is used to hold dressings on
the chin, cheeks, and scalp, and as a temporary support to immobilize a fractured or
dislocated jaw. (Applied when there is a fractured jaw or wound on the ear of the victim)
1. After making a triangular bandage into a cravat of proper width, place it under the
chin and carry ends upward with one end longer than the other.
2. Bring longer end over the top of head. Cross both ends on side of head. (Ends shouldnow be of equal length)
3. Pass ends around head in opposite directions and tie with square knot on other side
of head on primary turn of cravat.
CRAVAT FOR THE EYES
INDICATION: The cravat bandage of the eye is used to hold a dressing over the eye. Two
cravats are required. (Applied when there is wound or injury in either of the victim’s eye,
laceration of the eyelids, or lacerated eyeball.)
1. Lay center of first cravat over top of head with the front end falling over uninjured
eye. Bring second cravat around head, over eyes, and over loose ends of first
cravat.
2. Tie in front. Bring ends of first cravat over top of head, tying there and pulling
second cravat up and away from uninjured eye.
SHOULDER-ARMPIT CRAVAT
INDICATION: The shoulder – armpit cravat (bis-axillary) is used to hold dressings in the armpit
(axilla) or on the shoulder. (Applied when there is wound or injury over the shoulders, burns,
or shoulder dislocation.)
1. Place cravat over dressing in armpit so the front end is longer than the back.
2. Carry the ends upward. Bring ends across each other over top of shoulder.
3. Cross ends over back and chest respectively to opposite armpit.
4. Tie ends just in front of uninjured armpit.
CRAVAT OF THE ELBOW
INDICATION: The cravat of elbow is used to hold dressings around the elbow. (Applied when
there is sprain on either right or left elbow of the victim)
1. Bend the arm to approximately 90 degrees and at the elbow and place the mid-portion of the cravat bandage at the elbow bringing and holding the ends of the
bandage upwards.
2. Cross both bandage ends and gently rolled extending both ends downward.
3. Roll both ends gently around the arm and pull both ends opposite the elbow and tie
it in square knot.
CRAVAT OF OPEN PALM
INDICATION: (Applied when there is vertical wound on either right or left palm of the victim.)
1. Apply a dressing to the wounded area and lay the mid of the cravat bandage over
the palm with the ends hanging on both sides.
2. Bring the end of the cravat from the little finger across back of the hand rolling it
upward over the base of the thumb; gently and slightly pull it downward across the
palm.
3. Hold the thumb end of the cravat and roll it across the back of the hand and pull it
over the palm towards the hollow portion of the palm in between the thumb and thepalm.
4. Take both ends to the back of the wrist of the hand and roll them crossing each
other, and then roll them up over the wrist and cross the both ends again.
5. Roll both ends at the back of the hand and tie with a square knot at the top of the
wrist.
CRAVAT OF CLOSE PALM (Applied when there is burned on the hand)
1. Lay the mid of the bandage over the wrist Hold the thumb end of the cravat and roll
it across the back of the hand rolling it upward over the base of the thumb, covering
only the four fingers; gently and slightly pull it downward.
2. Hold the other end of the bandage, roll it across the back of the hand rolling it in
between the thumb and index finger take both ends to the back of the wrist, cross
the ends, then roll them up over the wrist and cross it again.
3. Roll both ends at the back of the hand and tie with a knot at the top of the wrist
CRAVAT OF THE KNEE
INDICATION: The cravat of knee is used to hold dressings around the knee. (Applied when
there is wound in either right or left knee of the victim.)

5/10/2018 Emergency Care Nursing - slidepdf.com
http://slidepdf.com/reader/full/emergency-care-nursing-55a0bf3cdadc5 5/14
1. Bend the leg to approximately 90 degrees at the knee and place the middle of the
cravat bandage at the upper portion of the knee bringing and holding both ends of
the bandage downward.
2. Cross both bandage ends and gently rolled extending both ends downwards.
3. After rolling the bandage, at the same time pull both ends, tie both ends tightly
opposite the knee in square knot, and tuck in the remaining ends.
CRAVAT OF THE LEG
INDICATIONS: The cravat of leg is used to hold dressings around the leg.
1. Place center of cravat over dressing.
2. Begin ascending turns with upper end, and descending turns with lower end, with
each turn covering two-thirds of preceding turn until dressing is covered.
3. Terminate by tying both ends in square knot.
CRAVAT ANKLE WRAP
INDICATION: The cravat ankle wrap is used to hold dressings around the ankle.
1. Place the middle of the cravat under the heel of the foot.
2. Then bring the bandage up in back of the heel and around to the front of the ankle.
3. Now criss-cross it in a sort of figure-eight form around the ankle.
4. Tie it firmly in front of the ankle.
SPLINTING
Splint - Any device used to immobilize a fracture or dislocation. It can be soft or rigid,
commercially manufactured or improvised from virtually any object that can provide stability.
Splints are used to support and immobilize suspected fractures, dislocations, or sever
sprains; to help control bleeding; to help control pain; and to prevent further damage to
tissues from the movement of bone ends.
RULES FOR SPLINTING
Do not splint if it will cause more pain for the victim.
Both before and after you apply the splint, assess the pulse and sensation below the
injury. You should evaluate these signs every 15 minutes after applying the splint to
make sure the splint is not impairing the circulation.
Immobilize the joints both above and below the injury.
Splint an injury in the position you found it. If there is no distal pulse or movement,
you may attempt to return the bone to its normal alignment by placing one hand above
the injury and another below. Then pull with gentle traction while moving the injury
back toward the correct anatomical position.
Remove or cut away all clothing around the injury site with a pair of bandage scissor
so you won’t accidentally move the fractured bone ends and complicate the injury.
Remove all jewelry around the fracture site.
Cover all wounds, including open fractures, with sterile dressing before applying a
splint, then gently bandage. Avoid excessive pressure on the wound.
If there is a severe deformity or the distal extremity is cyanotic or lacks pulses, align
the injured limb with gentle traction before splinting, following the guidelines above.
Never intentionally replace protruding bone ends.
Pad the splint to prevent pressure and discomfort to the victim.
Apply the splint before trying to move the victim
When in doubt, splint the injury.
If the victim shows sign of shock, align the victim in the normal anatomical position
and arrangw for immediate transport without taking the time to apply a splint.
TYPES OF SPLINTS
1. Rigid Splint
Are commercially manufactured splints made of wood, aluminum, wire,
plastic, cardboard or compressed wood fibers
2. Traction Splints
Gently pulling the direction opposite the injury, alleviating pain, reducing
blood loss and minimizing further injury.Traction splints are not intended to reduce
the fracture, but simply to immobilize the bone ends and prevent further injury. A
traction splint should be used only for a broken thigh, and should be performed onlyby EMTs or those who have had special training in applying traction splints.
3. Pneumatic (Air) Splints
Are soft and pliable before being inflated but rigid once they are applied
and filled with air. Air splints should only be used on fractures where there is no
deformity, but immobilization is needed. A similar type of splint is the vacuum
splint,
4. Improvised splints
It can be improvised from a cardboard box, cane, ironing board, rolled up
magazine, umbrella, broom handle, catcher’s shin guard, or any other similar
object.
You can also use a self splint( also called an anatomical splint) by tying or
taping an injured part to an adjacent uninjured part. Ex. Splint a finger to a finger a
toe to a toe, a leg to the other leg, or an arm to the chest. An effective improvised
splint must be
Light in weight, but firm and rigid
Long enough to extend past the joints and prevent movements on either
side of the fracture
as wide as the thickest part of the fractured limb

5/10/2018 Emergency Care Nursing - slidepdf.com
http://slidepdf.com/reader/full/emergency-care-nursing-55a0bf3cdadc5 6/14
Padded well so the inner surface is not in contact with the skin
HAZARDS OF IMPROPER SPLINTING
IMPROPER SPLINTING CAN:
Compress the nerves, tissues and blood vessels under the splint, aggravating the
existing injury and causing new injury
Delay the transport of a victim who has a life threatening injury.
Reduce distal circulation, threatening the extremity.
Aggravate the bone or joint injury by allowing movement of the bone fragments or
bone ends or by forcing bone ends beneath the skin surface
Cause or aggravate damage to the tissues, nerves, blood vessels, or muscles as a
result of excessive bone or joint movement.
LOWER ARM AND WRIST
The lower arm, including the wrist and hand is common area for fractures.
There are two bones in the lower arm, the radius and the ulna.
If a fracture is suspected in either one or both of these bones, the victim should be seated
and the part protected by fixation.
1. Two wooden padded splints are needed. These splints should be long enough to
extend from the elbow down the ar, beyond the palm and figertips for an armfracture.
The splints should extend from the middle of the lower arm and beyond the
fingertips for a wrist injury, fracture or sprain.
2. One splint should be on the palm side and the other splint opposite, so that the arm
is centered between the splints.
3. The splints should be secured with roller gauze, elastic bandage, several neckties, or
two or three triangular bandages folded as cravats.
The fingertips should remain exposed at all times.
4. The injured arm should be placed in an arm sling with the fingertips exposed and
the arm should be elevated.
5. Another triangular bandage should be folded as a cravat, and the injured area
secured to the body.This bandage should surround the body from a midpoint in the
upper arm.
6. The victim should remai quiet, sitting or reclining, until suitable transportation is
provided.
UPPER ARM - HUMERUS
This bone is not as commonly fractured as the lower arm bones or the wrist. Such a
fracture would be indicated by pain from motion, swelling, and tenderness in the area.
1. The victim should be seated and quiet until transportation is provided.
2. Padded wooden splints should be placed on both sides of the arm, one from the
armpit down the inside and past the elbow joint, the second from the shoulder
down the outside of the arm and past the elbow joint.
3. The splints should be secured reasonably tight with triangular bandages folded as
cravats, or with neckties or roller-type bandages.
4. The arm should be placed in an arm sling with fingertips exposed and the arm
reasonably elevated.
5. Two cravats should be used to secure the arm to the body, surrounding the body
from a midpoint of the upper arm, and then tying the cravat ends on the opposite
side of the body.
ELBOW JOINT
This is important joint and protection should be given to prevent damage to the tissues that
surround it. Henderson states that such fractures may result in varying degrees of permanent
disability. If the elbow is fractured, there may be dislocation the first-aider should.
1. Place the victim in lying position to guard against shock.
2. The arm including the elbow should remain in position it was found.
3. If the arm is straight, splint with wooden splint from the armpit and beyond the
fingertips, placing the splint on the other s ide.
4. If the arm is bent, secure the arm to the body by means of an arm sling and by
cravats to maintain the bent position.
5. Provide suitable transportation to medical help.
6. If fracture is compound, cover the wound with dressing; then apply the splints. The
wound should be left for the physician to treat.
FINGEREach of the four fingers has three bones, and the thumb two bones. The fracturing of a finger
is rather common. When it occurs it is evident because there are pain, deformity, swelling
and inability to use the part. Finger injuries are common in physical activities, especially
football, basketball, and baseball.
If the finger is injured, it could be a sprain, a dislocation, or fracture. Only and x-ray can tell
for certain the nature of injury. In all three situations, splinting will protect.
1. Have the victim sit down and put his injured finger in an extended position.
2. Place a tongue blade, finger stall, or some firm material as a splint from the palm of
the hand to beyond the fingertip on the underside.
3. Secure the splint with a roller gauze or muslim strips.
4. Transport the victim to medical help for x-ray and treatment.
5. If it is a evident that the finger is dislocated, place the hand in a downward position
and exert a steady pull to position the finger.
LOWER LEG – TIBIA AND FIBULA The larger bone of the lower leg is the tibia, and if it is fractured it will be evident, as the
victim will immediately cease to use the part. However, persons have been known to
continue activity after a fracture of the small bone, the fibula. If the two bones are fractured,
the victim will be disabled immediately.
1. Place the victim in a reclining position.
2. Use ice packs or cold to limit swelling and bleeding.

5/10/2018 Emergency Care Nursing - slidepdf.com
http://slidepdf.com/reader/full/emergency-care-nursing-55a0bf3cdadc5 7/14
3. Place the injured leg between two padded splints, one extending from the groin
(between the legs), and the second splint corresponding with the first in position
but on the outside of the leg.
4. Secure the splints with four or five triangular bandages, folded as cravats but not
tight enough to limit circulation.Place the victim on a litter and transport him to
the hospital in a reclining position, preferably keeping the injured leg in an
elevated position.
KNEE CAP OR PATELLA
The most common fracture of the knee occurs at the kneecap, as a result of a crushing
below. The great majority of such accidents are sustained in automobile accidents when the
person riding next to the driver is thrown forward against the dashboard.
Knee fractures also result from athletic injuries and other crushing blows. The seat belt has
proven to be the best device for preventing this type of accident in the automobile crash.
Fractured kneecaps are indicated by swelling and pain in the joint. The victim will not attempt
to straighten the knee and it is frequently possible to feel the parts of the broken bone, the
patella.
1. Place the victim in a lying-down position (supine) and protect against shock.
2. Apply cold compresses or ice packs to the injured area to limit swelling and bleeding
3. Place a padded wooden splint, six inches wide and thick enough to support, from the
buttocks to beyond the heel and the underneath side of leg
4. Secure the extended leg which has been placed upon the splint with four or five
triangular bandages, folded as cravats
5. Place the splinted leg in an elevated position and wait for transportation ‘
6. Transport to a hospital and medical help in a lying position
UPPER LEG - FEMURThe upper leg has only one bone, the femur. This bone supports the entire body
weight when a person stands. If the shaft or main portion of the femur is fractured or broken,
the individual will be immobilized at once. The upper end of the femur terminates into a
round ball-like part which fits into the pelvis to form a ball-and-socket joint, the hip joint. It is
not uncommon for the head of the femur to be broken off, especially In older persons, Such
injuries would be the most difficult to ascertain without the x-ray. Fracture of the femur or
upper leg can be protected by either fixation or traction splinting.
1. Keep the victim down and protect for shock.
2. Straighten the leg as gently as possible.
3. Place a padded wooden splint from the armpit on the injured side to six to twelve
inches beyond the feet.
4. Place a second padded wooden splint between the legs, from the groin to some six
to twelve inches beyond the feet. Pad the area over the crest of the ileum to
lessen pressure on the greater trochanter of the femur.
5. Secure the two splints with six to eight triangular bandages folded as cravats. Placethree or four of these cravats around the two splints and the injured leg,
between the ankle and the groin; then with two or three additional cravats tie
around the torso and the long splint.
6. Secure the two legs together, from hip to feet with two or three more triangular
bandages as cravats.
7. Keep the victim down and comfortable until transportation is available to medical
help.
PELVIS OR HIP
Fractures of the pelvis are most common in older people and usually result from
falls. Fractures of the pelvis to persons of all ages are common in crushing-type injuries, such
as result from automobile accidents. If there is any likelihood of a fracture to this area, the
victim should not be permitted to get on his feet. It is dangerous because bone fragments
could penetrate the bladder, reproductive organs, intestines, blood vessels, and nerves.
Indications of a fractured pelvis are pain, inability to lift or move the leg, false position of the
leg and/or foot, and a deep bruise. Frequently the leg and foot assume a turned-out position.
The first-aid protection for a fracture of the pelvis is the use of fixation splinting.
1. Place the victim in a lying-down position (supine) and gently straighten the leg. The
victim should be protected against shock.
2. Place a padded splint, a board six to twelve inches wide and at least an inch thick,
beneath the victim on the injured side. The splint should extend several inches
beyond the head and the feet.
3. Place a folded blanket or pad between the victim’s legs.
4. With three triangular bandages folded as cravats, secure the leg to the splint, with
three more cravats, secure the upper body or torso to the splint.
5. With two or three additional cravats, secure the two legs, going around the legs,
splint, and folded blanket.
6. Transport the victim to the hospital in an ambulance or other suitable conveyance.
Select messages to forward.Select messages to delete.Delete All
SPINAL INJURY
VICTIM ASSESSMENT To assess a responsive victim:
1. Note the mechanism of injury- especially the type of movement and amount of force
that was involved in the injury. Even if a victim can move or walk around, spinal
injury may exist- so always suspect spinal injury if the mechanism of injury
suggests it.
2. Ask:
Does your neck or back hurt? Pain from a spinal injury often radiates from
the neck to the arms, from the upper back to the ribs, and from the lower back
to the legs- so pain maybe confined to the neck or back.
What happened?
Where does it hurt?
Can you move your hands and feet?
Can you feel me touching your fingers?
Can you feel me touching your toes?
Can you feel which toe I am pinching?

5/10/2018 Emergency Care Nursing - slidepdf.com
http://slidepdf.com/reader/full/emergency-care-nursing-55a0bf3cdadc5 8/14
Can you feel which finger I am pinching?
3. Inspect the back for contusions, deformities, lacerations, punctures, penetrations,
and swelling. If necessary, cut clothing away so you can see the area clearly.
4. Palpate gently for areas of tenderness or deformity.
5. Assess equality of strength in the victim’s extremities.
Have the victim grip and squeeze both your hands; note differences in
strengths.
Have the victim gently push his/her feet against your hands; note strengthand equality.
To assess an unresponsive victim:
1. Note the mechanism of injury. If the mechanism of injury suggests spinal injury and
the victim is unconscious, assume spinal injury has occurred.
2. Inspect for contusions, deformities, lacerations, punctures, penetrations, or swelling;
palpate for areas of deformity.
3. Ask others at the scene about the mechanism of injury and the victim’s mental
status before you arrived in the scene.
FIRST AID CARE FOR SPINAL INJURY
The general rule for management of spinal injury is to support and immobilize the spine, the
head, the torso, and the pelvis. Your goal is to end up with a victim who is properly
immobilized on a backboard. It is better to overtreat than to risk further injury.
Activate the EMS system; then:
1. The first priority is to establish and maintain an open airway and adequate
ventilation. Use the modified jaw-thrust technique to open the airway and provide
rescue breathing if breathing is inadequate.
2. Establish and maintain in-line stabilization.
Place the head in a neutral line-position unless the victim complains of pain
or the head is not easily moved in position.
If you encounter resistance, stabilize the neck in the position in which you
found it.
Place the head in alignment with the spine.
Maintain a constant manual in-line stabilization until the victim is properly
secured to a backboard with the head immobilized.
Prevent movement of the victim’s head by one of the following methods:
Having a person hold the head and neck in a neutral in-line position.
Kneel with the victim’s head held firmly between your knees.
Perform the initial assessment; check pulse and circulation; perform CPR if
necessary, but do not move the victim. Control hemorrhage, but never try to stop the
flow of blood or fluid from the ears, nose, or mouth. Never apply pressure to a bleeding
head wound if you suspect skull fracture.
Complications of Spinal Injury
Inadequate Breathing Effort
Respiratory paralysis may occur with spine injury, and death may occur rapidly if
respiratory assistance is delayed. The diaphragm may continue to function even if the chest
wall muscles are paralyzed; a victim who is breathing with the diaphragm alone will have
shallow breathing with little movement of the chest or abdomen.
Paralysis
There is usually weakness, loss of sensation, or paralysis below the level of injury. In the
conscious victim, paralysis of the arms or legs is considered the most reliable sign of spinal
injury.
NECK AND BACK
The procedures for caring for a victim of a broken back are the same as those listed for one
with a broken neck, with this important exception: The victim must be transported in the
face-down position.
Injuries to the back and neck should receive the utmost protection. Careless handling can
injure the spinal cord and cause paralysis or death. First-aiders should not attempt to move
the victim until sufficient help is available and a rigid platform is at hand for use as a litter.
Planking is available and a rigid platform is at hand for use as a litter. Planking is preferable
because of the ease in securing the triangular bandages which are used as cravats. Such a
platform can be made with a minimum of effort, or in an emergency a door can be used as
the rigid-type litter. The first-aider can make several checks to determine where the back is
injured. Back and neck injuries can be protected by the first-aider by applying fixation
splinting:
1. Prepare a rigid platform from two boards longer than the victim’s body and
strong enough to support his weight without bending. Three or four cross
boards, three or four inches wide, should be placed at the location where
the feet, knees, hips, and shoulders of the victim will be. These boards
should be nailed together, leaving a reasonable space between the twolong boards for the cravats o secure the injured victims to the rigid litter.
2. If possible, pad the boards with a blanket.
3. Place the victim on the stretcher, face down for a back injury, face up for a
neck injury. There should be sufficient people to easily lift the victim and to
keep his head and body straight without and bending, twisting, or jarring.

5/10/2018 Emergency Care Nursing - slidepdf.com
http://slidepdf.com/reader/full/emergency-care-nursing-55a0bf3cdadc5 9/14
The lifter should carefully rehearse, one person sould give command, and
then all should work as a unit. Special consideration should be given to the
head and neck to prevent possible turning, twisting, or falling. It is
advisable for one person to maintain the position of the head by applying a
steady pull.
4. Secure the victim firmly by tying the legs, hips, torso, head and neck. The
arms can be folded across the body and secured at the wrists.
5. Pad on each side with pillows, paper, clothing, wrapped bricks, sand bags,
etc,.to keep the head in position. Nothing should be placed between the
litter and the head. Place padding beneath the body curves.
6. Carefully place the victim in an ambulance on his rigid platform litter;
transport slowly and carefully to the hospital and medical staff. If possible,
the hospital should be advised that a back and neck injury victim is in
transit.
TRANSPORT A CASUALTY USING A ONE-MAN CARRY
One-man manual carries are used to move a casualty when the time or materials
needed to make a litter are not available and/or other personnel are not available to assist
you in moving the casualty. If the casualty is conscious, tell him what you are going to do and
get him to help you as much as possible.
CHOOSE AN APPROPRIATE ONE-MAN CARRY
When choosing a one-man carry, consider the casualty's injuries, the military
situation, the distance to be covered, the weight of the casualty, your s trength andendurance, and obstacles to be encountered.
BASICS
TURN A CASUALTY
• Some carries require the casualty to be in a prone position; others require him to be
in a supine position.
• Kneel at the casualty's uninjured side.
o If you are in a chemical environment, squat--do not kneel.
• Place the casualty's arms above his head and cross his far ankle over the near one.
RAISE A CASUALTY TO A STANDING POSITION
Some one-man carries requires the casualty be raised to a standing position. If the
casualty is conscious, you may be able to assist him to stand up. If the casualty is
unconscious, however, you need to raise him to a standing position without his help.
RAISE A CASUALTY TO A STANDING POSITION
Regular Method
• Position the casualty in a prone position.
• Straddle the casualty, slip your hands under his chest, and lock your hands together.
• Lift the casualty and begin walking backward until he is on his knees.
• Continue walking backward until his legs are straight and his knees are locked.
RAISE A CASUALTY TO A STANDING POSITION
• Walk forward and bring the casualty to a standing position. Keep the
casualty tilted slightly backward so his knees will remain locked. If his knees
do not remain locked, walk backward until they lock and then move forward
until the casualty is in the standing position.
• Grasp one of the casualty's wrists and raise his arm. Use your other arm to
hold the casualty erect.
RAISE A CASUALTY TO A STANDING POSITION
• Move under the casualty's arm to his front, lower his arm, and put both of
your arms around the casualty's waist to support the casualty. Interlock the
fingers of your hands.
• Place your foot between the casualty's feet and spread them so his feet are
about six to eight inches apart.
RAISE A CASUALTY TO A STANDING POSITION
Alternate Method
• This method is used if it will be safer for the casualty due to his injuries.
• Position the casualty in a prone position.
• Kneel on one knee at the casualty's head, facing the casualty's feet.
o If you are in a chemical environment, squat--do not kneel.
• Put your hands under his armpits, down his sides, and across his back.

5/10/2018 Emergency Care Nursing - slidepdf.com
http://slidepdf.com/reader/full/emergency-care-nursing-55a0bf3cdadc5 10/14
RAISE A CASUALTY TO A STANDING POSITION
• Rise, lifting the casualty to his knees. Keep the casualty's head from snapping back.
• Lower your arms, secure a hold on the casualty, and raise him to a standing position
with his knees locked.
• Put your arms around the casualty's waist, interlock your fingers, and tilt his body
slightly backward to keep his knees from buckling.
• Place your foot between his feet and spread them so his feet are six to eight inches
apart.
TYPES OF ONE MAN CARRY
Fireman's Carry
• Used to quickly move an unconscious or conscious casualty.
• Can be used to move the casualty a moderate or long distance.
• Leaves one of the bearer's arms free to carry a rifle, move around obstacles,
etc.
PERFORM THE FIREMAN'S CARRY
1. Raise the casualty to a standing position.
2. Grasp the casualty's wrist and lift his arm over his head while continuing to support
the casualty with your other arm.
a. If the casualty has an injured arm, grasp the wrist of the uninjured arm.
3. Bend at the waist and kneel, pulling the casualty over your shoulder. At the same
time, slip your arm from his waist, pass the arm between the casualty's legs, and
grasp behind the casualty's knee.
4. Move the hand grasping the casualty's wrist to the hand at the casualty's knee.
5. Grasp the casualty's wrist with the hand behind the casualty's knee, thus freeing the
hand that previously held the wrist.
6. Place your free hand on your knee and push on your knee to slowly rise to a
standing position. This will help to prevent back strain.
7. Adjust the casualty's body so his weight is distributed comfortably.
8. Move forward, carrying the casualty.
Support Carry
• Used only with a conscious casualty who can walk or at least hop on one leg.
• Can be used to move a casualty a long distance or until the casualty tires.
PERFORM THE SUPPORT CARRY
1. Position the casualty in a sitting position.
2. Bend down at the casualty's side so you are facing in the same direction as the
casualty.
a. If the casualty has an injured leg, position yourself with the injured leg next
to you.
3. Bring the casualty's near arm over your shoulder and grasp his wrist with your hand
that is away from the casualty.
4. Put your inside arm around the casualty's waist.
5. Stand up, helping the casualty to rise to a standing position also.
6. Assist the casualty to walk or hop on one leg.
7. Adjust your walking motion as needed to help the casualty maintain his balance.
Arms Carry
• Used to move a conscious or unconscious casualty.
• Used to move a casualty a short distance
PERFORM THE ARMS CARRY
1. Raise the casualty to a standing position.
2. Slide one of your arms under the casualty's arm, behind his back, and under his
other arm.
3. Move to the casualty's side, bend down, and place your other arm behind thecasualty's knees.
4. Lift the casualty from the ground and stand erect.
5. Carry the casualty high on your chest to lessen fatigue.

5/10/2018 Emergency Care Nursing - slidepdf.com
http://slidepdf.com/reader/full/emergency-care-nursing-55a0bf3cdadc5 11/14
Saddleback / Piggy Back Carry
• Used only for a conscious casualty who can put his arm around your neck.
• Can be used to move a casualty a moderate or long distance.
PERFORM THE SADDLEBACK CARRY
1. Raise casualty to a standing position or have the casualty stand up.
2. Grasp the casualty's wrist and lift his arm over his head while continuing to
support the casualty with your other arm.
3. Turn so your back is to the casualty and bring his arm over your shoulder.
Support the casualty's waist with your other arm, if needed.
4. Grasp the casualty's other wrist and lift his arm over your shoulder or have the
casualty put his other arm around your neck
5. Have him grasp one of his wrists with his other hand.
6. Stoop and move your arms around the outside of the casualty's thighs.
7. Bring your hands inside the casualty's thighs to your sides, lifting his thighs.
8. Stand up and clasp your hands together in front of you.
9. Adjust the casualty to make the weight distribution more comfortable.
10. Walk forward.
Pack-Strap Carry
• Used for a conscious or unconscious casualty.
• Can be used to move a casualty a moderate distance.
• Not used if the casualty has a broken arm.
PERFORM THE PACK-STRAP CARRY
1. Raise the casualty to a standing position.
2. Grasp one of the casualty's wrists and lift his arm above his head while
continuing to support the casualty's waist with your other arm.
3. Turn so your back is to the casualty. Bring the casualty's raised arm over your
shoulder as you turn.
4. Bend your knees somewhat so your shoulder fits under his arm.
5. Release his waist, grasp his other wrist, and bring that arm over your other
shoulder.
6. Hold both wrists so his hands are in a palms down (palms toward your body)
position. Twisting his hands could result in injury to the casualty's joints when
he is lifted and carried.
7. Bend forward and lift the casualty as high on your back as possible.
8. Walk forward, keeping bent so the casualty's weight is balanced on your backand his feet are not dragging.
Drags
Neck Drag
• Used to move a conscious or unconscious casualty.
• Used to move a casualty for a short distance.
• Keeps rescuer close to the ground
• Used when moving behind a low wall, under a vehicle, or through a culvert.
•
Not used if the casualty has a broken arm.
PERFORM THE NECK DRAG
1. Position the casualty on his back.
2. Tie the casualty's hands together with material which will not cut his wrists, such as
a field dressing or a cravat. Do not tie the materials tight enough to interfere with
the blood circulation.
a. If the casualty is conscious, tell him to interlock his fingers.
3. Face the casualty's head and straddle his hips on your knees.
4. Loop the casualty's arms around your neck.
5. Crawl forward on your hands and knees, dragging the casualty beneath.
a. Keep the casualty's head from dragging on the ground.
Cradle Drop Drag

5/10/2018 Emergency Care Nursing - slidepdf.com
http://slidepdf.com/reader/full/emergency-care-nursing-55a0bf3cdadc5 12/14
• Used to move a conscious or unconscious casualty.
• Used to move a casualty up or down steps or low drops or to quickly move a
casualty from a life-threatening situation.
PERFORM THE CRADLE DROP DRAG
1. Position the casualty on his back.
2. Kneel at the casualty's head.
3. Slide your hands (palms up) under his shoulders and grasp the clothing under hisarmpits.
4. Partially rise, pulling the casualty to a semi-sitting position.
5. Support his head on one of your arms.
a. If possible, bring your elbows together and use both forearms to support
the head.
6. Rise to a stooped position.
7. Walk backward, dragging the soldier backward.
8. If you go down steps, let his hips and legs drop from step to step.
Shoulder drag
• The shoulder drag is accomplished by placing the victim in a supine position
(laying on his back), grasping shoulders, and dragging him in the desired
direction
Clothing Drag
1. Tie the patient's wrists together if you have something quickly available. If nothing is
available, tuck the hands into the waist band to prevent them from being pulled
upwards.
2. Clutch the patient's clothing on both sides of the neck to provide a support for the
head.
3. Pull the patient towards you as you back up, watching the patient at all times. Thepulling force should be concentrated under the armpits and NOT the neck.
Blanket Drag
1. Lay a blanket lengthwise beside the patient.
2. Kneel on the opposite side of the patient and roll the patient toward you.
3. As the patient lies on their side while resting against you, reach across and
grab the blanket.
4. Tightly tuck half of the blanket lengthwise under the patient and leave the
other half lying flat.
5. Gently roll the patient onto their back.
6. Pull the tucked portion of the blanket out from under the patient and wrap
it around the body.
7. Grasp the blanket under the patient's head to form a support and means
for pulling.
8. Pull while backing up and while observing the patient at all times.
TWO MAN CARRY
SEAT CARRY
- Is a method of lifting and moving a victim in which two rescuers form a “seat” with their
arms
Version one: The hammock variation
1. Raise the victim to a sitting position. Each
first aider steadies the victim by positioning
an arm around the victim’s back.
2. Each first aider slips another arm to the
victim’s thighs, then clasp the risk of the
other first aider. One pair of arms should
make a seat and the other should make a
back rest.
3. Slowly raise the victim from the ground
moving in unison.
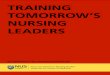
Version two: The interlocking wrist variation
1. Both the rescuers face each other, with their handsout.
2. Each rescuer takes their left hand and grabs their
right wrist.

5/10/2018 Emergency Care Nursing - slidepdf.com
http://slidepdf.com/reader/full/emergency-care-nursing-55a0bf3cdadc5 13/14
3. Keeping the hands in this position, each rescuer grabs the other's left wrist with the
right hand. This should
4. provide a sturdy base upon which the victim may sit. The victim should place his/her
arms around the shoulders of each rescuer.
EXTREMITY LIFT
- Is a method of lifting and carrying a victim in which 2 rescuers carry the victim by the
extremities . Do not use this method if the victim has back or any serious injuries.
1. One first aider kneels at the victims head, the other kneels at the
victims knees.
2. The person at the head places one hand under each of the victims
shoulders; and grasps the victims wrists.
3. The person on the victim’s knees pulls the victim to a sitting position
by pulling on the victims wrist, the person at the head assist by
pushing the victims shoulders and supporting the back.
4. The person at the knees slips his hands beneath the victims knees
5. Both first aiders crouch on their feet and simultaneously stands in one
fluid motion.
CHAIR LITTER CARRY
If the victim has no contraindicating injuries and if a chair is available, you can use this
method.
-The chair carry, can be used to move a victim away from a
position of danger. The victim is seated on a chair and the chair is
carried by two people. This is a good method to use when you
must carry a victim up or down steps or through narrow, winding
passageways.
• Do not attempt if the casualty has an injured neck,
back, or pelvis!
• Sit the victim on a chair.
• One first aider carries the back of the chair while the
other carries the legs; the chair itself is used a litter.
• Be sure that the chair is sturdy enough to support the weight of the victim.
Modified Two-Man Arms Carry
1. Two litter bearers kneel on one knee by the
victim’s side (opposite side from litter).
2. One bearer slips his arms under the victims
back and waist.
3. The other bearer slips his
hands under the victim’s
hips and knees.
4. Both bearers lift in unison
upon command from the
leader.
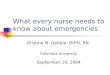
THREE MEN CARRY
FLAT LIFT AND CARRY (THREE
RESCUERS)
The three-rescuer flat lift and carry, when three rescuers lift and carry the victim to
a stretcher, is an effective way to move a severely injured victim who cannot sit in a chair or
when a cot cannot be moved close to the victim. It has the advantage
of permitting you to move the victim through narrow passages and
downstairs. Use this method only if the victim does not have spinal
injury.
1. Three first-aiders line-up on the least injured side of the
victim; if one first aider is noticeably taller, that person
stands at the victims shoulder; another stands at the victims
hips, and the third at the victims knees.

5/10/2018 Emergency Care Nursing - slidepdf.com
http://slidepdf.com/reader/full/emergency-care-nursing-55a0bf3cdadc5 14/14
2. Each first aider kneels on the knee closest to the victims feet.
3. The f irst-aider at the victims
shoulder works his or her hand
underneath the victim’s neck and
shoulders; the next first aider’s
hands go underneath the victim’s
hips and pelvis; and final first-
aider’s hands go underneath the
victims knees.
4. Moving in unison, the firs-aiders
raise the victim to knee level and
slowly turn the victim toward
themselves until the victim rests on
the bends of their elbows.
5. Moving in unison, all three rise to a
standing position and walk with the
victim to a place of safety or to the
stretcher. To place the victim on
the stretcher, simply reverse the
procedure.
This move can also be done with
four first aiders: position them at the victims
head, chest, hips, and knees. Support is
then given to the head, chest, hips, pelvis,
knees and ankles.
Recommended