2
UAA Integrated Suicide Prevention Initiative
_______________________________________
The UAA-ISPI is a comprehensive, coordinated, culturally-sensitive
effort aimed at promoting campus-wide suicide prevention education
and awareness.
3
Introductions◦Who we are.◦Who are you?
This is a safe place to share. You know your limits – if you need a break, please do so.
Safe Place
4
Everyone’s situation is unique
No universal standards will prevent suicide
The purpose of this training is to prepare you to
provide help to someone at risk
There is no guarantee that a suicide can be
prevented
Please feel free to excuse yourself if the content
brings up overwhelming feelings or memories.
Disclaimer
5
A gatekeeper is a person who can
intervene with someone that is having
suicidal thoughts
A gatekeeper is not a professional mental
health provider
Student gatekeepers are vital
What is a Gatekeeper?
6
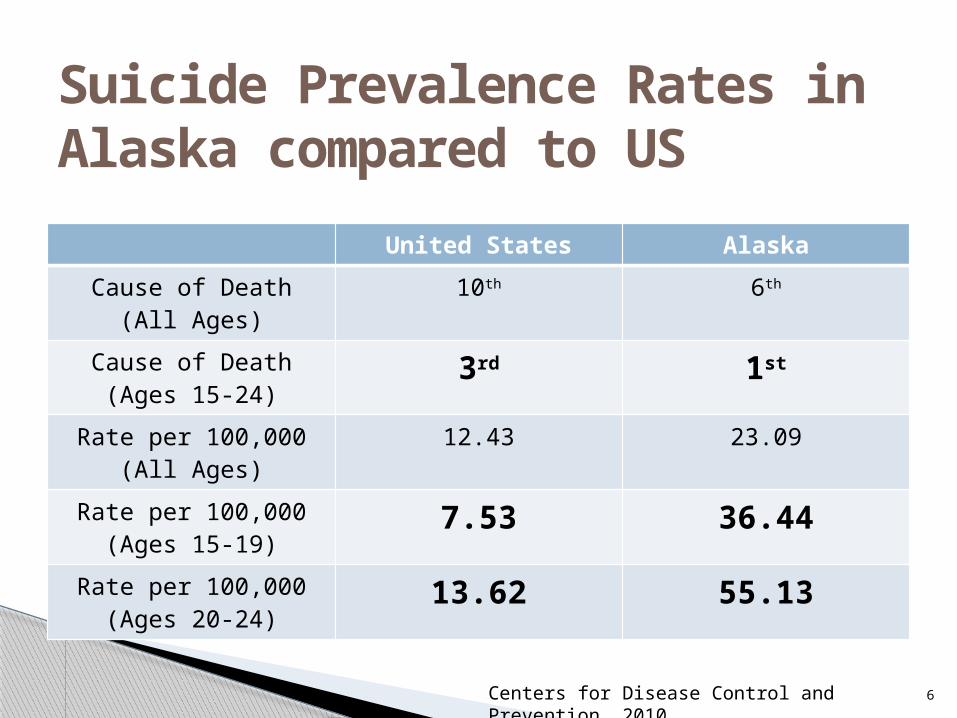
Suicide Prevalence Rates in Alaska compared to US
United States Alaska
Cause of Death(All Ages)
10th 6th
Cause of Death(Ages 15-24)
3rd 1st
Rate per 100,000(All Ages)
12.43 23.09
Rate per 100,000(Ages 15-19)
7.53 36.44
Rate per 100,000(Ages 20-24)
13.62 55.13
Centers for Disease Control and Prevention, 2010
7
Survey of students at UAA (2009 & 2011) 40.5% experienced hopelessness, and 38% felt so depressed that it was difficult to function◦ Impaired functioning is a symptom of clinical depression
Within the past 12 months:◦Half report feeling very lonely ◦ 45% report overwhelming anxiety◦ 36% overwhelmed with anger◦ 6% seriously considered suicide
Difficult problem areas: academics, career, finances, personal health, and relationships.
Suicide Risk & Alaskan Students
8
SydneyTurn to Vignette #1
9
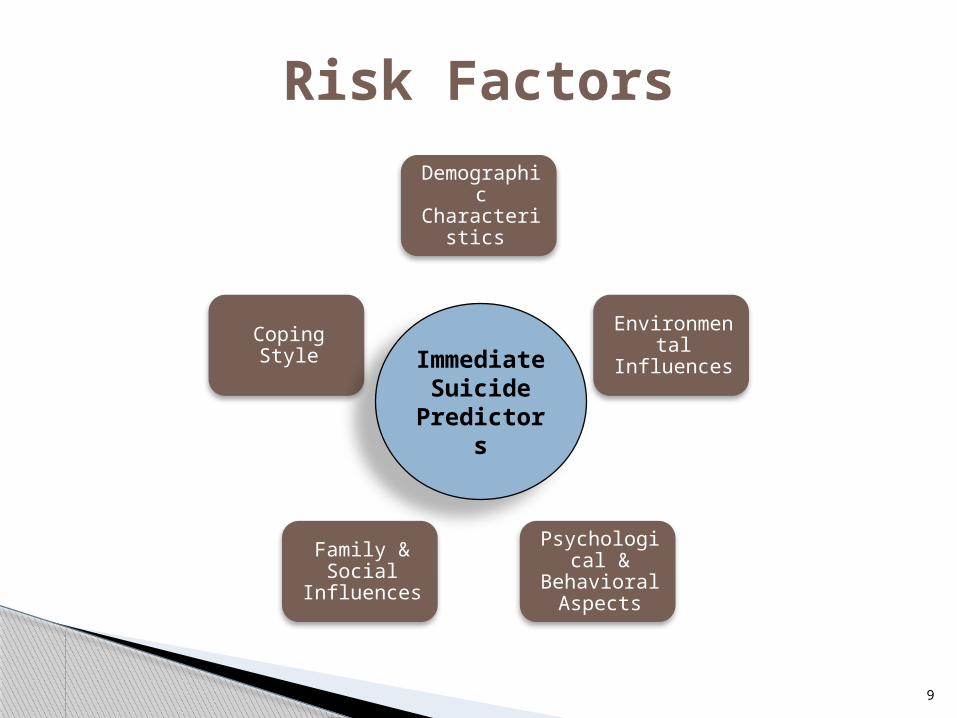
Risk FactorsDemographi
c Characteristi
cs
Environmental Influences
Psychological &
Behavioral Aspects
Family & Social
Influences
Coping StyleImmediate Suicide Predictor
s
10
Demographic characteristics
◦ Males, older students (25 years +), graduate students
◦ Non-traditional students
◦ Other groups
ethnic, military families, LGBTQ, first-year, international
Environmental influences
◦ Negative school experience
◦ Trouble adjusting to higher education
◦ Pending legal trouble
Risk Factors
11
Psychological & behavioral aspects◦Overly withdrawn, feeling depressed or worthless◦Problems with alcohol or substance use◦History of suicide attempt
Family & social influences◦Career decision◦Oppression or stigmatization ◦ Interpersonal relationships
Coping styles◦Certain personality types◦Being easily overwhelmed, stressed, upset◦ Inability or unwillingness to reach out for help
Risk Factors
12
Verbal◦ direct verbal communication◦ indirect, such as via written material (e.g.,
assignments, email messages, papers) Behavioral◦ giving away possessions, writing a suicide note,
acquiring means to complete suicide, organizing personal matters, suddenly resigning from organizations or clubs
Situational◦ stressful or traumatic experience
Immediate Predictors
13
Protective Factors
Sense of Connection
Family & Social
Fulfillment
Community Belonging
Individual Characteristics
14
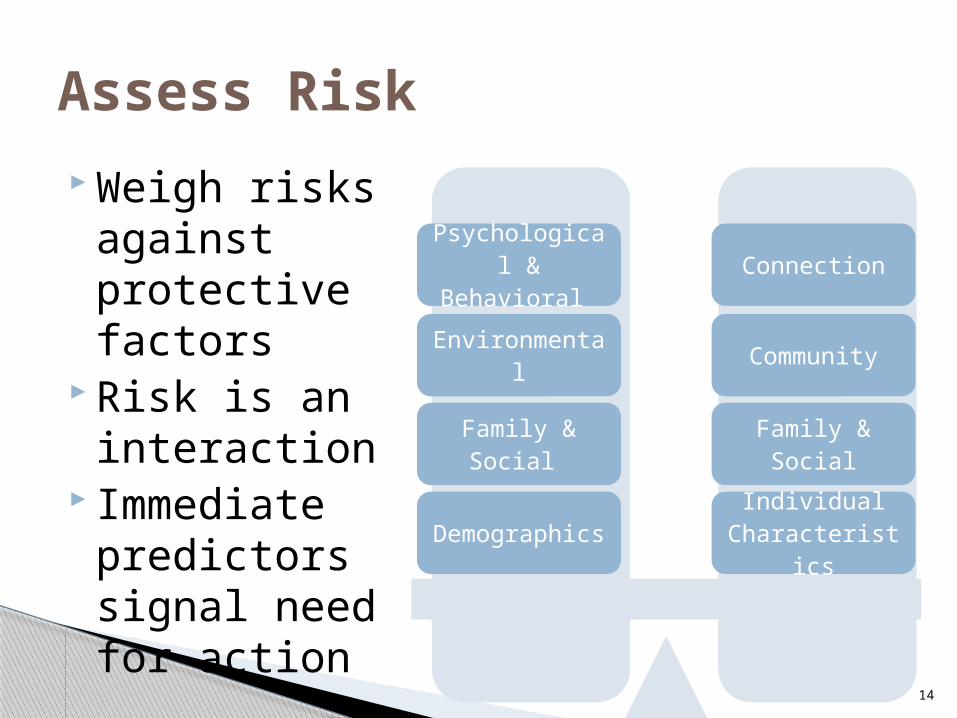
Assess Risk
Weigh risks against protective factors
Risk is an interaction
Immediate predictors signal need for action
Risk FactorsProtective
Factors
Individual Characteristic
s
Family & Social
Community
Connection
Demographics
Family & Social
Environmental
Psychological & Behavioral
15
SydneyTurn back to Vignette #1
Risk factors, protective factors, & immediate suicide predictors.
16
Many people are uncomfortable and/or unsure
◦ Reacting to someone who may be suicidal
◦ Interacting with someone considering suicide
◦ Talking about suicide
Asking a person about suicide won’t make matters
worse – in fact not asking may increase suicide risk
It is important to reflect on personal reactions to
suicide, including personal experiences and readiness
to respond
Common Personal Reactions
17
Helping a Person who is Suicidal
“People are not driven to suicide by a caring person who inquires as to whether
or not they are suicidal. People may, however, be driven to suicide by an
avoidance of the topic on the part of the listener from whom they need a
concerned response.”
(Fujimura, Weis, & Cochran, 1985, p. 613)
18
1. Appear calm◦Rather than appearing inconvenienced, frustrated
or frantic (even though this may be how you feel)◦Avoid saying:
“Don’t be ridiculous!” or “Why would you want to do that?”
2. Talk to the person privately◦Make the interaction as normal and natural as
possible
3. Build rapport and trust◦A person who is having suicidal thoughts may be
less than willing to confide in you
Effective Interaction
19
4. Use reflective listening◦Begin with,
“It sounds like…(reflect what you’ve heard).”
or◦ “So what you’re saying is…(reflect what was heard).”
This kind of communication helps the suicidal person feel understood
Keeps communication open Encourages more disclosure Elicits more information
◦Pay attention to potential nonverbal communication
Effective Interaction
20
5. Assess general risk
◦ Ask about immediate predictors
◦ Ask about risk factors and potential stressors
(e.g., substance use, relationships, academics)
6. Speak directly about suicide
◦Avoid euphemisms or any indirect wording
◦Use the actual words “death” and/or “suicide”
◦Asking directly eliminates any guesswork
Effective Interaction
21
Collaborate with the person if possible
Generate ideas what match the person’s
risk level
Take concrete action
Attend to safety
Develop an Action Plan
Plans not involving
formal treatment
Outpatient treatment
interventions
Voluntary psychiatric
hospitalization
Involuntary psychiatric
hospitalization
22
Emphasize that help is available and is effective
Provide resources
◦ Normalize accessing support
“There are places on campus that can help students who are
stressed out.”
◦ Provide a hard copy of resources
◦ Even if the individual appears to resist the idea, suggest
the idea of getting help and provide information on
resources
Develop an Action Plan
23
Examples of action plans
Low risk:
◦Careline information, talk with the person
Medium risk
◦Stay with the person, seek immediate assistance
High risk (immediate predictors)
◦ Call 911 to transport person to Providence, stay with
him/her.
Develop an Action Plan
24
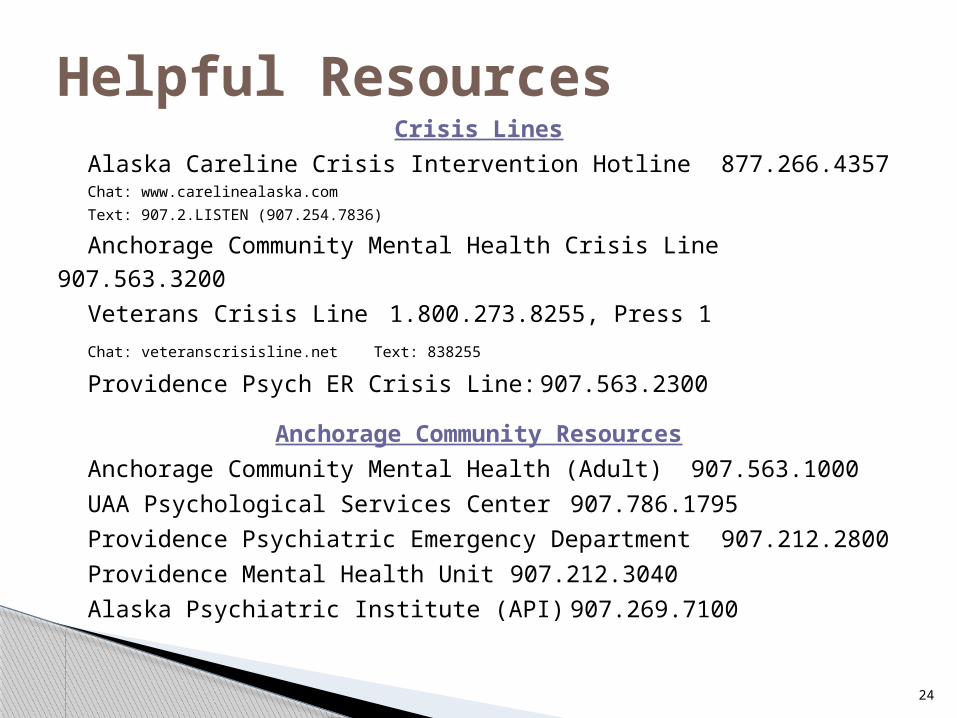
Crisis Lines
Alaska Careline Crisis Intervention Hotline 877.266.4357Chat: www.carelinealaska.com
Text: 907.2.LISTEN (907.254.7836)
Anchorage Community Mental Health Crisis Line 907.563.3200
Veterans Crisis Line 1.800.273.8255, Press 1
Chat: veteranscrisisline.net Text: 838255
Providence Psych ER Crisis Line: 907.563.2300
Anchorage Community Resources
Anchorage Community Mental Health (Adult)907.563.1000
UAA Psychological Services Center 907.786.1795
Providence Psychiatric Emergency Department 907.212.2800
Providence Mental Health Unit 907.212.3040
Alaska Psychiatric Institute (API) 907.269.7100
Helpful Resources
25
A student is a direct threat to themselves Police can be helpful to ensure safety and
provide direct transport to services Be as collaborative as possible with the
student “I’m really concerned for your immediate safety and feel like someone needs to be here right now to help you through this.”
Emergency Care
26
Nick, Randi, & ColinPractice your skills!

27
Questions or Comments?
Recommended