Substance abuse
Eran Kozer MD
Pediatric Emergency Medicine
Assaf Harofeh Medical Center

Outline
� Case presentation
� Ethanol
� Marijuana
� Opioids
� Cocaine
� Amphetamines
�Designer drugs
� LSD & other hallucinogens
� PCP and ketamine

Outline
� Pharmacology (brief)
� Clinical aspects
� No discussion of treatments

Case Presentation
� At 4 am a 17 year old boy was found by his parents in his bed with generalized tonic clonic seizures.
� Taken to the ED (still seizing)
� P 114 bpm, temp 36.60C RR 20/min, BP 103/70 mm Hg, O2 sat 97%.
� History of complex partial seizures starting at 10 years of age
� Treated with carbamazepine
� Seizure free for 5 years
� Off medications for the last 2 years
� No recent febrile illness or trauma
� No petechiea or needle pricks
� Parents were not aware of substance abuse
� Lab – normal glucose and electrolytes
� Bicarbonate – 13 mmol/L, Anion gap –32 mmol/L, osmolal gap - 26mmol/kg

� DO you think the boy’s symptoms were caused by substance abuse?
� A – Yes
� B – No
� C – Can't tell

Which tests will you order?
� Urine tox screen
� Ethanol serum level
� Non of the above

Ethanol
� Rapid absorption from GI tract (<60 min)
� One standard drink (15g ethanol –bottle of beer, glass of
wine, 30 ml liquor)
raises ethanol serum level by 36mg/dl
� Enhancement of GABA activity in GABA receptors
� Blockade of NMDA (N-methyl-D-aspartate)
receptors

Ethanol level was 50 mg/dl

Clinical manifestations – low dose
� Selective CNS depressant at low doses
� Depress areas of highly integrated functions
� Loss of restrains & disinhibition
� Paradoxical stimulation
� Emotional liability
� Basic personality features are enhanced
Clinical manifestations – high dose
General CNS Depressant at high dose
� Irritability
� Abusive behavior and aggression
� Confusion, dysarthria, disorientation, lethargy
� Loss of protective reflexes
� Coma (blood ethanol >300 mg/dl)
� Death
So, is it a mixed overdose?Which of the following drugs may cause seizures?
� Marijuana ?
� Yes
� No
Marijuana
� Active ingredient – THC
� Immediate effect when smoked
� Peak effect 10-30 min
� Duration – 1-4h
� Binding to specific cannabinoid receptors in the cortex
Marijuana – Clinical effects
� Alteration of sensation, perception, cognition, psychomotor functions
� Euphoria, relaxation, sensory alterations
� Loss of motor skills and judgment
� Acute psychosis (not common)
� Seizures - rare
Marijuana –Physiological effects
� Increased heart rate
� Hypotension/ hypertension
� Tremor, muscle weakness
� Bronchodilation
� Conjunctival injection
� Increased appetite
� Urinary retention

Marijuana – Chronic heavy users
� Effects on the lungs
� Tolerance
� Dependence (psychological and physiologic)
� Withdrawal symptoms (sleep disturbances, irritability, nausea, decreased appetite)

Back to the case
� Treated with benzodiazepines and phenytoine. Seizures stopped after 1 hour
� CT Scan ordered

Copyright © 2007 by the American Roentgen Ray Society
Keogh, C. F. et al. Am. J. Roentgenol. 2003;180:847-850
27-year-old man found at home with decreased level of consciousness, aphasia, and spastic quadraparesis
Axial CT scan obtained through
brain at level of third ventricle
shows symmetric white matter
hypoattenuation in optic radiations
and posterior limbs of internal
capsule, simulating dragon's claws.

which substance did he use?
� Cocaine
� Marijuana
� LSD
� Heroin
Chasing the Dragon
� Inhalation of heated heroin
� Pharmacokinetic similar to IV
� Spongiform leukoencephalopathy
� Initial symptoms may occur after 2 weeks
� Bradykinesia, ataxia, speech abnormalities
� Spasticity or hypotonia
� Death in 25% of the cases

Opioids
� Extract of poppy plant
� Available in various formulations – administration by all possible routes (parenteral, oral, transdermal, transmucosal, intranasal, rectal, inhalation)

Brief History
� Written evidence of opium use from 1500 BC
� 1804 – morphine isolated
� 1830’s Opium Wars between China and England
� 1874 – Heroin synthesized (marked by Bayer as antitussive agent)
1874 – Heroin synthesized (marked by
Bayer as antitussive agent)
Terminology
� Opiate – alkaloid derived directly from poppy opium (morphine codeine)
� Opioids – agents that are capable of producing opium like effect by binding to opioid receptors

Clinical effects
� CVS
� peripheral vasodilatation
� Orthostatic hypotension
� Flushing
� GI
� Reduced motility
� Reduced gastric acid secretion
� Increased sphincters tone

� CNS� Sedation……………coma
� Seizures (pethidine)
� Antitusive
� Respiratory� Respiratory depression
� Bronchospasm
� Pulmonary edema
� Other� Miosis
� Pruritus
Back to the case
� The CT scan was normal
� Slowly recovered
� Occasional myoclonic jerks
� Denies substance abuse

?

Cocaine
� Leaves of Erythroxylon Coca
� Documented use from the 6th century
�Local anesthetics solutions
"...This Intellectual beverage …contains the valuable NERVE STIMULANT and TONIC
properties of the coca plant...“

Pharmacology
�Mucosal absorption
� respiratory
� gastrointestinal
� Genitourinary (vagina, urethra)
� Onset of action 1-3 min peak 20-30 min
� Intravenous / Smoking
� Onset of action - seconds
� peak 5 min

CNS Effects
CNS stimulation
� cortex first
� Restlessness, excitement, increased motor activity
� Mediated at part by inhibition of dopamine reuptake
� Lower motor centers
� Seizures
CNS Effects
� TIA
� Increased risk of stroke
� Subarachnoid hemorrhage
� Dystonic reactions
� Migraine type headaches
� Leukoencephalopathy
� Cerebral vasculitis
� Psychiatric manifestations
Other clinical manifestations (partial list)
� Hyperthermia
� Myocardial ischemia
� Dysrhythmias
� Cardimyopathy (dilated)
� DVT
� Pulmonary effects (asthma exacerbation
pneumothorax, hemorrhage etc.)

Amphetamines
� Methamphetamine (crack, speed)
� 3,4 –Methylenedioxymethamphetamine
(MDMA) - Ecstasy
� Designer Amphetamines

Khat (gat)
� Cathinone
Amphetamines – Clinical manifestations
� Stimulation of adrenergic receptors in the CNS and peripheral nervous system
� Similar to cocaine but tend to be longer

Amphetamines – setting
� Rave parties
� Speed runs (days up to weeks)

Amphetamines – CNS effects
� Agitation
� Seizures (less common than cocaine)
� Intracerebral hemorrhage
� Headache
� Euphoria
� Anorexia
� Bruxism

Amphetamines – CNS effects
� Choreoatheotid movements
� Compulsive behavior
� Hyperreflexia
� Hyperthermia (central)

Amphetamines – CNS effects
Paranoid psychosis
� Dopaminergic activity
� Tend to reoccur
� May lead to suicide and homicides

Amphetamines –Other effects
� CVS –Hypertension, tachycardia, dysrhythmias, MI, aortic dissection, vasospasm
� Diaphoresis, tachypnea, mydriasis, tremor, nausea.

Amphetamines –Other effects
� Rhabdomyolysis, muscle rigidity
� Acute lung injury
� Ischemic colitis
Amphetamines – lab abnormalities
� Leukocytosis
� Hyperglycemia
� Hyponatremia
� Elevated CK
� Elevated liver enzymes
� Myoglobinuria

Designer drugs
�“Legal” highs
�Designed by pharmacists to bypass legislation
�Not included in the “Dangerous Drug Ordinance”
�Sold
�over the internet
�Street shops
�Other phenethylamines (2C drugs)
�Synthetic cannabinoids
�Synthetic cathinones (bath salts)
�Piperazines


Phenethylamines (2C drugs)
�A clinical picture of both stimulatory and hallucinogenic effects
�Tachycardia, hypertension, euphoria, agitation, psychosis, and hallucinations
� Other effects seen with serotonergic and sympathomimetic toxicity
�No data on long term effects



�Paramethoxymethamphetamine (PMMA), a hallucinogenic synthetic substituted amphetamine
�Was marketed in Israel because it was not included in the Israeli Controlled Substances Act (CSA).

�PMMA and paramethoxyamphetamine (PMA) belong to a group of methoxylated phenethylamine derivatives
�PMA enhances the release of serotonin, inhibits its reuptake and metabolism
�Little effect on the dopaminergic system
�PMA has monoamine oxidase (MAO)-A inhibitory properties.

Clinical effects
�Tachycardia
�Hypertension
�Hyperthermia
�Nystagmus
�Muscle spasm
�Bruxism
�Visual hallucinations
�Cardiac arrhythmias
�Respiratory failure
�Renal failure
�Seizures
�Death
�In fatal cases hyperthermia with a core temperature ranging between 39 and 42.8° C

Synthetic cannabinoids
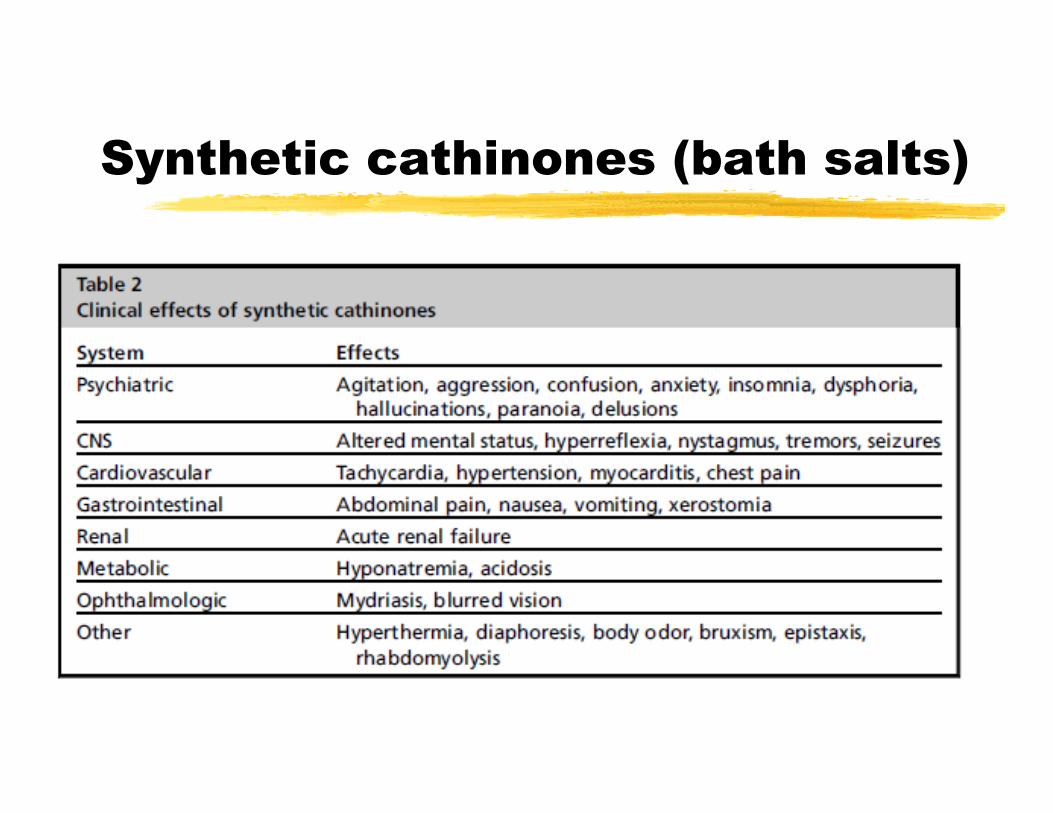
Synthetic cathinones (bath salts)

Piperazines
�Initially developed as antihelminthic drugs but later studied as antidepressants
�Piperazines are some of the most common active substances found in drugs purchased on the Internet.
�Typical users are young males

Piperazines
�Most symptoms with piperazine use resemble a sympathomimetic toxidrome
�Insomnia, anxiety, headaches, nausea, tremors, shakiness, diaphoresis, dizziness, palpitations, shortness of breath, confusion, hallucinations, and paranoia.
Since all of the above may cause
seizures – what is the next step ?
� Toxicology screen: blood ?
� Toxicology screen: Urine ?
Toxicology screen: blood
�Volatile alcohols
�Acetaminophen
�Salycilates
�Others

Urine toxic screen
• Immunoassays: most
common but non specific

�Cannabis metabolites,
�Cocaine metabolites,
�Opiate metabolites, Metahdone
�Amphetamines, Metamphatamines
�PCP
�GHB
�Benzodiazepines, barbiturates
�TCA
Urine toxic screen
• HPLC (High Pressure
Liquid Chromatography) -
more than 700 toxins can
be identified
• GCM
Drugs that may be missed by
toxicology screen
� LSD
� Fentanyl
� Lorazepam
� Ketamine
� GHB…...

LSD & other Hallucinogens
� Acts on serotonin receptors in the CNS
� Lysergic acid & derivates
� Phenylethylamines

Other hallucinogenic agents
� Anticholinergics
� belladonna alkaloids
� MDMA
� Mushrooms

LSD & other Hallucinogens
� Physiologic effects
� Mydriasis, tachicardia, hypertension, tachypnea hyperthermia, diaphoresis, (mild)
� Nausea and vomiting
� Precede hallucinogenic effects
LSD & other Hallucinogens
CNS effects
� Dizziness
� Hyperactivity
� Muscle weakness
� Ataxia
� Altered mental status
� Coma
� Hippus (spasmodic rhythmical pupillary dilation and constriction)
Psychological effects
� Usually fully awake
� Emotional liability
� Loss of body image
� Alteration in visual perception
� Excessive attention to details

Psychological effects
� Usual thoughts may look novel and profound
� Intensification of sensory perceptions (colures are brighter, sound magnification)
� Synthesis (hearing colures )
Acute psychiatric effects
� Acute panic reaction (most common)
� Psychosis
� Major depression

LSD - Long term effects
� Prolonged psychosis
� Severe depression
� Exacerbation of preexisting psychiatric disease
Hallucinogen Persisting
Perception Disorder (HPPD)
� Flashbacks (usually of former hallucinogenic experience)
� May be triggered by stress or illness
� Few month to 5 years
� No established treatment

Dissociative agents
� Initially developed as anesthetic agents
� PCP (phencyclidine)
� Ketamine
Dissociative agents - pathophysiology
� NMDA receptors in the cortex and limbic structures
� Antagonize (not competitive) glutamate action
� Monoaminic reuptake inhibition
� σ (sigma) receptors
� Ach receptors

Available forms
� PCP - powder, liquid, tablets, leaf mixture (for smoking), rock crystals
� Ketamine –powder, tablets, liquid; rarely used IV

Clinical Manifestations
� Sympathomimetic effects
� Hypertension
� Cerebral hemorrhage (rare)
� Vomiting (marijuana)
� Both cholinergic and anticholinergic effects (miosis or mydriasis, bronchospasm, hypersalivation)

Clinical Manifestations - CNS
� Nystagmus
� Ataxia & altered gait
� Diplopia
� Dystonic reactions
� Myoclonic movements
� Tremor
� Seizures (rare)

Clinical Manifestations – CNS
� Diminution of sensory modalities
� Depersonalization, hostility
� Alteration of body image
� Dissociation – calm; agitated; stupor; delirium; apathy; coma

Few words on treatment
� Don’t forget the ABC’s
� Check bedside glucose if the patient is obtunded
� Thiamine ? for ethanol intoxication not routinely used in teenagers
� Naloxon
� Other antidotes – rarely used

What you see may be just the tip of the iceberg
Recommended