Et h ical D i lemmas in M u I t icu It u ral Cou nsel i ng
Maria Sadeghi, Jerome M. Fischer, and Sean G. House
In a random survey of counselors working with socioracial minority clients ( N = 256), multicultural ethical dilemmas were rated according to frequency encountered and significance. Comparisons of counselors’ ratings of multicultural ethical dilemmas determined specific dilemmas relevant to counselors in various professional settings.
En una encuesta hecha al azar de consejeros/as que trabajan con clientes de minorias socioraciales (N= 256), se clasificaron dilemas eticos multiculturales de acuderdo con s u frecuencia y significancia. Las comparaciones de las clasificaciones de 10s dilemas eticos multiculturales subrayaron aquellos dilemas especificamente importantes para consejeros/as en varios escenarios profesionales.
ounseling today continues to move toward a cultural pluralism that embraces unity in diversity (Axelson, 1999). To provide the most C effective services to clients from diverse backgrounds, counselors need
to be trained in and to have experience with multicultural counseling. Arredondo et al. (1996) described multicultural counseling as the prepara- tion and practices that integrate multicultural and culture-specific awareness, knowledge, and skills into counseling interactions.
Although cross-cultural counseling has existed since the beginning of the profes- sion, studies show that counseling has not been as effective with ethnically differ- ent clients as with mainstream clients (S. Sue, 1977; S. Sue & Zane, 1987). A pos- sible explanation for the ineffectiveness of cross-cultural counseling could be the lack of culturally sensitive material taught in counseling programs (Arrendondo, 1985; Ponterotto & Casas, 1987; Smith, 1982; D. W. Sue et al., 1982). Although multicultural counseling has become the “hottest topic in counseling” in the past decade, the quality of training is still inadequate (Arredondo, 1994; Atkinson, 1994; Pedersen, 1994; Ridley, Mendoza, & Kanitz, 1994). The majority of coun- selor training programs fail to adequately recognize the ramifications of culture or to address issues that pertain to ethnic minorities (D. W. Sue & Sue, 1990). If counselors lack sufficient training in multicultural counseling it is likely that
they also lack the skills to deal with ethical issues presented by clients with multicultural backgrounds. Pedersen (1997) stated that most counselors have
Maria Sadeghi, Idaho Deparlment of Heallh and Welfare; Jerome M. Fischer and Sean G. House, College ofEducalion, University of Idaho. Zlis article was based on [he firs[ author’s doctoral disserlalion, whit% was chaired by the second author. Correspondence concerning this arlicle should be addressed loJerome M. Fischer, University of Idaho, College of Educalion, Counseling d School Psychology, MOSCOW, ID 83844 (e-mail: [email protected]).
JOURNAL OF MULTICULTURAL COUNSELING AND DEVELOPMENT July 2003 VOl. 31 179
not been sufficiently prepared to interpret the ethical guidelines with sensitiv- ity to racial and ethnic minority groups.
Until relatively recent times, counseling predominantly came from a Euro- American perspective (Pedersen, 1997). The textbooks, research findings, and psychological theories often contained culture-specific assumptions. Some of these assumptions include a universal definition of what constitutes “normal” behav- ior, individualism as preferable to collectivism, independence as more desirable than dependence, an emphasis on understanding linear thinking where each cause has an effect and each effect has a cause, and the paradigm wherein coun- selors change an individual to fit the system rather than changing the system to fit the individual.
Conjointly with counseling theories, approaches to counseling ethics have origi- nated from the Euro-American ethical theories of utilitarianism, Kantianism, and liberal individualism. These ethical theories were adapted to the biomedi- cal field by Beauchamp and Childress (1994) and to the field of counseling by Kitchener (1984). The foundation of these ethical approaches are “principle” ethics (Cottone & Claus, 2000).
A multicultural counseling perspective has emerged of late that seeks to build its theories with a focus on pluralism in order to ensure that no single political, economic, or special interest agenda is promoted. Furthermore, the study of traditional theories in counseling and psychotherapy has been changed to in- clude their adaptation to cultural diversity (Axelson, 1999).
Likewise, counseling ethics have moved toward embracing a multicultural perspective. Past ethical approaches have not been effective because tradi- tional ethical theories generally ignore race, ethnicity, and cultural diversity. Most theories are based on a utilitarian and Kantian moral agent operating in a vacuum without individuality as influenced by culture (Hinman, 2001). Rec- ognizing the cultural encapsulation of traditional counseling theories and ap- proaches to ethics, Pedersen (1997) challenged the counseling profession to refine its codes of ethics to make them more relevant to socioracial minority clients. Meara, Schmidt, and Day (1996) incorporated “virtue” ethics, with its sensitivity to a culturally diverse community’s wisdom and moral sense, as a complement to Euro-American “principle” ethics. Lastly, Cottone (2001) pro- posed a social constructivist model of ethical decision making in counseling that embraces a social context that encompasses a diverse worldview, both for the client as well as the counselor.
Although recent efforts have been made, there is a paucity of ethics education materials for counselors regarding multicultural issues (Casas, Ponterotto, & Gutierrez, 1986; Cayleff, 1986; Fitzgerald & Nutt, 1986; Goodyear, Crego, &
Johnston, 1992; Ibrahim & Arredondo, 1986; Jordan & Meara, 1990; Kitchener, 1992; Meara et al., 1996; Pope & Vetter, 1992; Welfel, 1992). This lack of multicultural ethical training suggests a need to develop multicultural ethics education materials for counselors. Furthermore, guidance for developing such
180 JOURNALOF MULTICULTURAL COUNSELING AND DEVELOPMENT July 2003 Vol. 31
materials could be obtained from an understanding of the types of ethical dilem- mas that multicultural counselors encounter.
The purpose of this study was to identify the specific types of ethical dilem- mas relevant to counselors who work with multicultural clients. Specifically, this study sought to answer the following research questions:
1. What are the multicultural dilemmas most frequently encountered by counselors?
2. How do counselors rate the significance of ethical dilemmas for inclu- sion in training materials designed to prepare counselors for dealing with multicultural ethical dilemmas?
3. What multicultural ethical dilemmas are frequently encountered and significant for inclusion in training materials relevant to counselors working at various professional settings.
od DEVELOPMENT OF THE INSTRUMENT
The Multicultural Counseling Ethical Dilemma Survey (MCEDS) was de- veloped for this research by the first and second authors. A modified Delphi method of research, which combines a qualitative and quantitative meth- odology, was used (Linstone & Turoff, 1975). The first stage of the process was to obtain relevant multicultural dilemmas. A qualitative process was used to interview 24 counselors. These counselors worked predominantly with socioracial minority clients, and the counselors had professional ex- perience ranging from preservice internship to 20 years. The interview process yielded 15 multicultural ethical dilemmas. In addition to the inter- view process, a review of relevant counseling and psychology literature identified 4 additional multicultural ethical dilemmas. Through this quali- tative review process, the researchers compiled a total of 19 multicultural ethical dilemmas. The second stage of the Delphi method was to validate the data collected,
using a quantitative process. This was accomplished through the content va- lidity ratio process (Cohen, Swerdlik, & Phillips, 1996). The 19 multicultural ethical dilemmas were rated for inclusion in the MCEDS by 10 nationally recognized counselor educators and professionals with expertise in the field of multicultural counseling. The professionals reviewed the 19 dilemmas and indicated whether each had validity as a multicultural ethical dilemma. The professionals rated each item for inclusion in the survey instrument using a Likert-type scale as follows: 1 = essential, 2 = use@ but not essential, and 3 = not essential. The following formula was used to compute the validity ratio:
JOURNAL OF MULTICULTURAL COUNSELING AND DEVELOPMENT July 2003 Vol. 31 181
ne- N / 2 CVR= N / 2 ’
where CVR= content validity ratio, ne= number of professionals indicating that the ethical dilemma was “essential,” and N= total number of professionals.
For significance at the .05 level and inclusion in the MCEDS, each multicultural ethical dilemma would have met the criteria of a CVR of .62 or higher (Cohen et al., 1996). Of the original 19 multicultural ethical dilemmas obtained from the qualitative process, 8 were retained for inclusion in the MCEDS.
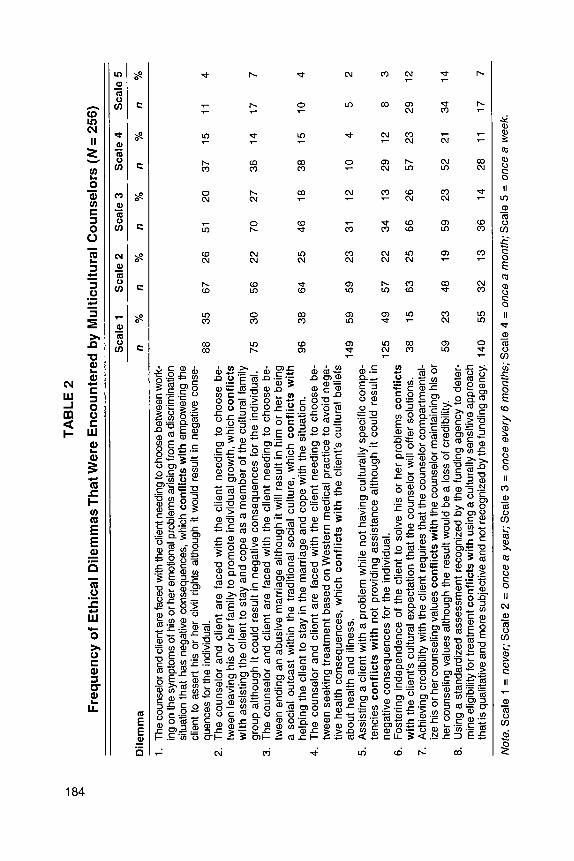
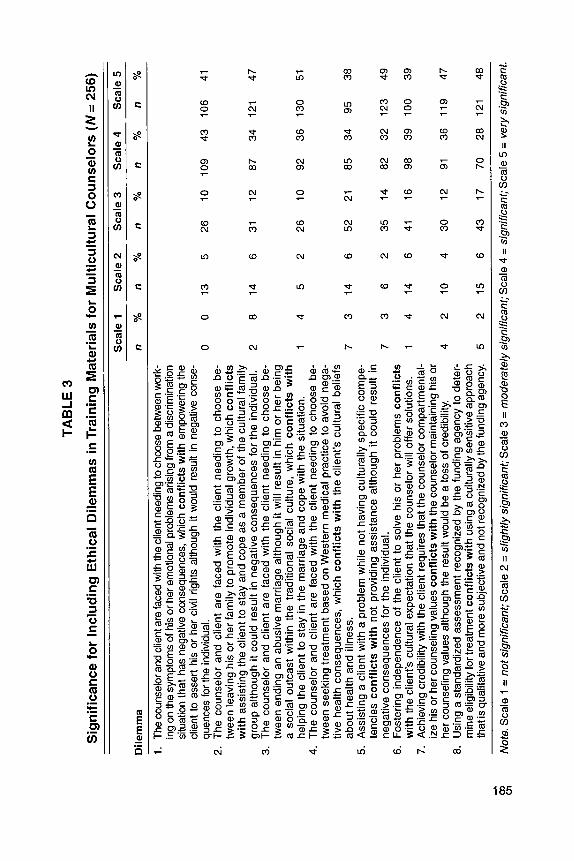
The third stage was to construct the survey instrument and conduct a pilot study. The MCEDS consisted of eight multicultural ethical dilemmas; survey respondents were asked to rate each dilemma on two Likert-type scales. The first scale asked respondents to rate the frequency with which they had en- countered the multicultural ethical dilemma in the following manner: 1 = never, 2 = once a year, 3 = once every 6 month, 4 = once a month, or 5 = once a week The second scale asked respondents to rate the significance of the dilemma to be used in preparation of counselors to deal with multicultural ethical dilemmas in the following manner: 1 = not significant, 2 = slightly signzficant, 3 = moderately significant, 4 = significant, or 5 = very signzjkant.
A pilot study was conducted that consisted of sending the MCEDS to 25 randomly selected American Multicultural Counseling and Development (AMCD) members. These individuals were removed from the data set from which the research sample for the larger study would be drawn. All 25 surveys were returned. The MCEDS was refined in terms of language of the ethical dilemmas and instructions to respondents based on these responses.
Finally, after completing the survey (N= 256), to determine internal consis- tency and to estimate the reliability and construct validity of the MCEDS, a Cronbach’s alpha of .82 was computed.
PARTICIPANTS
The survey was sent to a random sample of 813 individuals out of a population of 3,080 AMCD members.
Out of 813 surveys distributed, 256 usable questionnaires were returned, rep- resenting a 31% return rate.
The majority (59%) of participants were Caucasian (see Table 1). The second largest group who responded to the survey were African American (23%).
More than two thirds (68%) of the respondents (N= 256) had between 5 and 21 years of professional experience. Participants were asked what percentage of their client population included members of ethnoracial multicultural groups. Fifty-four percent responded that between 10% and 65% of their client popu- lation included members of ethnoracial multicultural groups. Another 25O/o indicated that more than two thirds (66%) of their client population included multicultural groups.
182 JOURNAL OF MULTICULTURAL COUNSELING AND DEVELOPMENT July 2003 Vol. 31
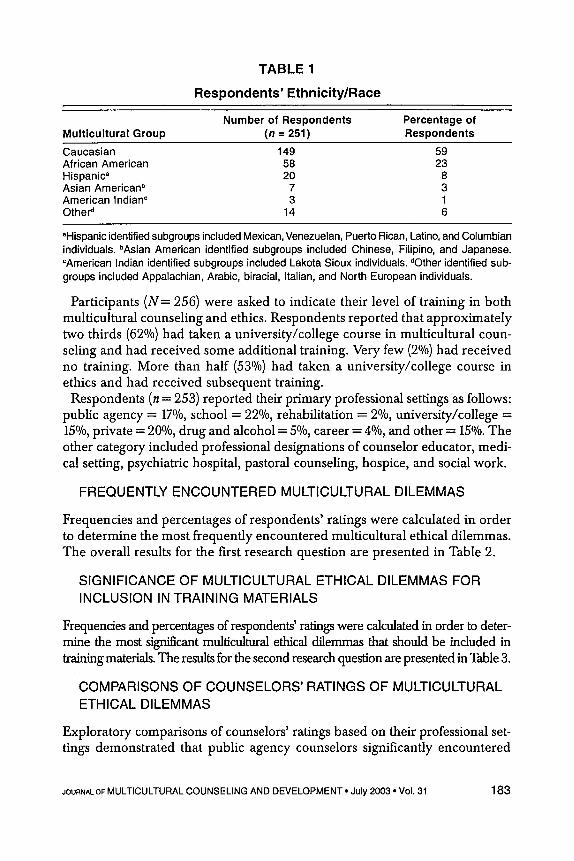
TABLE 1
Respondents’ Ethnicity/Race
Number of Respondents Percentage of Multicultural Group ( n = 251) Respondents
Caucasian 149 59 African American 58 23 Hispanic’ 20 8 Asian Americanb 7 3 American Indian” 3 1 Other‘ 14 6
“Hispanic identified subgroups included Mexican, Venezuelan, Puerto Rican, Latino, and Columbian individuals. bAsian American identified subgroups included Chinese, Filipino, and Japanese. “American Indian identified subgroups included Lakota Sioux individuals. dother identified sub- groups included Appalachian, Arabic, biracial, Italian, and North European individuals.
Participants ( N = 256) were asked to indicate their level of training in both multicultural counseling and ethics. Respondents reported that approximately two thirds (62%) had taken a university/college course in multicultural coun- seling and had received some additional training. Very few (2%) had received no training. More than half (53O/o) had taken a university/college course in ethics and had received subsequent training.
Respondents (n = 253) reported their primary professional settings as follows: public agency = 17%, school = 22%, rehabilitation = 2010, university/college = 15Ok0, private = 20%, drug and alcohol = 5%, career = 4%, and other = 15O/o. The other category included professional designations of counselor educator, medi- cal setting, psychiatric hospital, pastoral counseling, hospice, and social work.
FREQUENTLY ENCOUNTERED MULTICULTURAL DILEMMAS
Frequencies and percentages of respondents’ ratings were calculated in order to determine the most frequently encountered multicultural ethical dilemmas. The overall results for the first research question are presented in Table 2.
SIGNIFICANCE OF MULTICULTURAL ETHICAL DILEMMAS FOR INCLUSION IN TRAINING MATERIALS
Frequencies and percentages of respondents’ ratings were calculated in order to deter- mine the most si@cant multicultural ethical dilemmas that should be included in training materials. The results for the second research question are presented in Table 3.
COMPARISONS OF COUNSELORS’ RATINGS OF MULTICULTURAL ETHICAL DILEMMAS
Exploratory comparisons of counselors’ ratings based on their professional set- tings demonstrated that public agency counselors significantly encountered
JOURNALOF MULTICULTURAL COUNSELING AND DEVELOPMENT July 2003 Vol. 31 183
TA
BL
E 2
Fre
qu
ency
of
Eth
ical
Dile
mm
as T
hat
Wer
e E
nco
un
tere
d b
y M
ult
icu
ltu
ral C
ou
nse
lors
(N
= 25
6)
Sca
le 1
S
cale
2
Sca
le 3
Sca
le 4
S
cale
5
Dile
mm
a n
YO
n YO
n
%
n
%
n
%
1.
2.
3.
4.
5.
6.
7. a.
The
coun
selo
r and
clie
nt a
re fa
ced
with
the
clie
nt n
eedi
ng to
cho
ose
betw
een w
ork-
in
g on
the
sym
ptom
s of h
is o
r her
em
otio
nal p
robl
ems
aris
ing
from
a d
iscr
imin
atio
n si
tuat
ion
that
has
neg
ativ
e co
nseq
uenc
es, w
hich
con
flict
s w
ith e
mpo
wer
ing
the
clie
nt to
ass
ert
his
or h
er c
ivil
right
s al
thou
gh it
wou
ld r
esul
t in
nega
tive
cons
e-
The
coun
selo
r an
d cl
ient
are
fac
ed w
ith t
he c
lient
nee
ding
to
choo
se b
e-
twee
n le
avin
g hi
s or
her
fam
ily to
pro
mot
e in
divi
dual
gro
wth
, whi
ch c
onfl
icts
w
ith
assi
stin
g th
e cl
ient
to s
tay
and
cope
as
a m
embe
r of t
he c
ultu
ral f
amily
gr
oup
alth
ough
it c
ould
res
ult i
n ne
gativ
e co
nseq
uenc
es fo
r th
e in
divi
dual
. Th
e co
unse
lor
and
clie
nt a
re f
aced
with
the
clie
nt n
eedi
ng t
o ch
oose
be-
tw
een
endi
ng a
n ab
usiv
e m
arria
ge a
lthou
gh it
will
res
ult i
n hi
m o
r he
r bei
ng
a so
cial
out
cast
with
in t
he t
radi
tiona
l so
cial
cul
ture
, w
hich
con
flic
ts w
ith
The
coun
selo
r an
d cl
ient
are
fac
ed w
ith t
he c
lient
nee
ding
to
choo
se b
e-
twee
n se
ekin
g tre
atm
ent b
ased
on
Wes
tern
med
ical
pra
ctic
e to
avo
id n
ega-
tiv
e he
alth
con
sequ
ence
s, w
hich
con
flic
ts w
ith
the
clie
nt's
cul
tura
l be
liefs
ab
out h
ealth
and
illn
ess.
149
59
Ass
istin
g a
clie
nt w
ith a
pro
blem
whi
le n
ot h
avin
g cu
ltura
lly s
peci
fic c
ompe
- te
ncie
s co
nflic
ts w
ith
not
pro
vidi
ng a
ssis
tanc
e al
thou
gh i
t co
uld
resu
lt in
ne
gativ
e co
nseq
uenc
es fo
r th
e in
divi
dual
. 125
49
Fost
erin
g in
depe
nden
ce o
f th
e cl
ient
to s
olve
his
or
her
prob
lem
s co
nflic
ts
with
the
clie
nt's
cul
tura
l exp
ecta
tion
that
the
coun
selo
r will
offe
r sol
utio
ns.
38
15
Ach
ievi
ng c
redi
bilit
y w
ith th
e cl
ient
requ
ires
that
the
coun
selo
r com
partm
enta
l- iz
e hi
s or
her
cou
nsel
ing
valu
es c
onfli
cts
with
the
coun
selo
r mai
ntai
ning
his
or
her c
ouns
elin
g va
lues
alth
ough
the
resu
lt w
ould
be
a lo
ss o
f cre
dibi
lity.
U
sing
a s
tand
ardi
zed
asse
ssm
ent r
ecog
nize
d by
the
fund
ing
agen
cy to
det
er-
min
e el
igib
ility
for t
reat
men
t con
flict
s w
ith u
sing
a c
ultu
rally
sen
sitiv
e ap
proa
ch
that
is q
ualit
ativ
e an
d m
ore
subj
ectiv
e an
d no
t rec
ogni
zed b
y th
e fu
ndin
g ag
ency
. 140
quen
ces
for t
he in
divi
dual
. aa
35
75
30
help
ing
the
clie
nt t
o st
ay in
the
mar
riage
and
cop
e w
ith t
he s
ituat
ion.
96
38
59
23
55
67
56
64
59
57
63
48
32
26
51
20
37
15
11
4
22
70
27
36
14
17
7
23
31
12
10
4 5
2
22
34
13 29
12
a 3
25
66
26
57
23
29
12
19
59
23
52
21
34
14
13
36
14
28
11
17
7
Not
e. S
cale
1 =
nev
er; S
cale
2 =
onc
e a
year
; Sca
le 3 =
onc
e ev
ery
6 m
onth
s; S
cale
4 =
onc
e a
mon
th; S
cale
5 =
onc
e a
wee
k.
TAB
LE 3
Sig
nific
ance
for
Incl
udin
g E
thic
al D
ilem
mas
in T
rain
ing
Mat
eria
ls fo
r M
ultic
ultu
ral C
ouns
elor
s (N
= 25
6)
Sca
le 1
S
cale
2
Sca
le 3
S
cale
4
Sca
le 5
Dile
mm
a n
%
n %
n
%
n %
n
%
1.
2.
3.
4.
5.
6.
7.
8. Th
e co
unse
lor a
nd c
lient
are
face
d w
ith th
e cl
ient
nee
ding
to c
hoos
e be
twee
n wor
k-
ing
on th
e sy
mpt
oms
of h
is o
r her
em
otio
nal p
robl
ems
aris
ing
from
a d
iscr
imin
atio
n si
tuat
ion
that
has
neg
ativ
e co
nseq
uenc
es, w
hich
con
flict
s w
ith e
mpo
wer
ing
the
clie
nt to
ass
ert
his
or h
er c
ivil
right
s al
thou
gh it
wou
ld r
esul
t in
nega
tive
cons
e-
quen
ces
for t
he in
divi
dual
. Th
e co
unse
lor
and
clie
nt a
re f
aced
with
the
clie
nt n
eedi
ng t
o ch
oose
be-
tw
een
leav
ing
his
or h
er fa
mily
to p
rom
ote
indi
vidu
al g
row
th, w
hich
con
flic
ts
wit
h as
sist
ing
the
clie
nt to
sta
y an
d co
pe a
s a
mem
ber o
f the
cul
tura
l fam
ily
grou
p al
thou
gh it
cou
ld r
esul
t in
nega
tive
cons
eque
nces
for
the
indi
vidu
al.
The
coun
selo
r an
d cl
ient
are
fac
ed w
ith t
he c
lient
nee
ding
to
choo
se b
e-
twee
n en
ding
an
abus
ive
mar
riage
alth
ough
it w
ill r
esul
t in
him
or
her b
eing
a
soci
al o
utca
st w
ithin
the
tra
ditio
nal
soci
al c
ultu
re,
whi
ch c
onfl
icts
wit
h he
lpin
g th
e cl
ient
to s
tay
in th
e m
arria
ge a
nd c
ope
with
the
situ
atio
n.
The
coun
selo
r an
d cl
ient
are
fac
ed w
ith t
he c
lient
nee
ding
to c
hoos
e be
- tw
een
seek
ing
treat
men
t bas
ed o
n W
este
rn m
edic
al p
ract
ice
to a
void
neg
a-
tive
heal
th c
onse
quen
ces,
whi
ch c
onfl
icts
wit
h th
e cl
ient
's c
ultu
ral b
elie
fs
abou
t hea
lth a
nd il
lnes
s.
Ass
istin
g a
clie
nt w
ith a
pro
blem
whi
le n
ot h
avin
g cu
ltura
lly s
peci
fic c
ompe
- te
ncie
s co
nflic
ts w
ith
not
pro
vidi
ng a
ssis
tanc
e al
thou
gh i
t co
uld
resu
lt in
ne
gativ
e co
nseq
uenc
es fo
r th
e in
divi
dual
. Fo
ster
ing
inde
pend
ence
of
the
clie
nt to
sol
ve h
is o
r he
r pr
oble
ms
conf
licts
w
ith th
e cl
ient
's c
ultu
ral e
xpec
tatio
n th
at th
e co
unse
lor w
ill o
ffer s
olut
ions
. A
chie
ving
cre
dibi
lity
with
the
clie
nt r
equi
res
that
the
coun
selo
r com
partm
enta
l- iz
e hi
s or
her
cou
nsel
ing
valu
es c
onfli
cts
with
the
coun
selo
r mai
ntai
ning
his
or
her c
ouns
elin
g va
lues
alth
ough
the
resu
lt w
ould
be
a lo
ss o
f cre
dibi
lity.
U
sing
a s
tand
ardi
zed
asse
ssm
ent r
ecog
nize
d by
the
fund
ing
agen
cy to
det
er-
min
e el
igib
ility
for t
reat
men
t con
flict
s w
ith u
sing
a c
ultu
rally
sen
sitiv
e ap
proa
ch
that
is q
ualit
ativ
e and
mor
e su
bjec
tive
and
not r
ecog
nize
d by
the
fund
ing
agen
cy.
0 0
13
5
2 8
14
6
14
52
7 3
14
6
73
62
14
14
6
4 2
10
4
5 2
15
6
26
31
26
52
35
41
30
43
10
12
10
21
14
16
12
17
109
87
92
85
82
98
91
70
43
106
34
121
36
130
34
95
32
123
39
100
36
119
28
121
41
47
51
38
49
39
47
48
-1.
Not
e. S
cale
1 =
not
sig
nific
ant;
Sca
le 2
= s
light
ly s
igni
fican
t; S
cale
3 =
mod
erat
e/y
sign
ifica
nt; S
cale
4 =
sig
nific
ant;
Sca
le 5
= v
ery
sign
ifica
nt.
Dilemma 3 more than school, rehabilitation, university/college, private, drug and alcohol, career and those designating a different professional category, ~ ‘ (7 , N = 252) = 26.69, p < .05. Drug and alcohol counselors significantly encountered Dilemma 7 more than counselors in other professional settings, ~ ~ ( 7 , N = 250) = 14.4, p < .05. When compared with counselors in other professional settings, coun- selors in the private professional setting rated Dilemma 4 as significantly more important for including in training materials, f ( 7 , N = 251) = 14.5, p < .05.
In the current study, the MCEDS was developed to identify specific types of ethical dilemmas encountered by counselors working with socioracial minor- ity clients. The return rate of questionnaires (31%) indicates that caution must be used when generalizing the results of this research to counselors who did not participate in the study. However, considering the demographics of the counselors responding to the survey, they reported that they were very expe- rienced, well trained in multicultural counseling, and worked with a substan- tial number of multicultural clients. An important finding was that respon- dents indicated all eight ethical dilemmas would be significant or very signifi- cant for including in multicultural counseling training materials.
Caution should also be used when interpreting the results of this research be- cause of limitations to the internal validity of the research. The first limitation is instrumentation. The researchers are aware that the language used to describe the multicultural ethical dilemmas may be problematic because each respondent may not discern the content as clearly as the next, and the content of dilemmas may be subjectively interpreted by the respondents in different ways. This limitation may explain an internal consistency coefficient of .82. The second limitation is mortal- ity. Only 31% of the sample returned the surveys, hence inference to the larger populations is not possible. Finally, selection is a limitation to internal validity. The respondents who voluntarily completed the surveys and returned them may have had special characteristics that make them a subset of the population.
We acknowledge that the data obtained in this study represent a beginning. Value differences between counselors and clients are crucial ethical challenges that must be met to have an effective delivery of counseling services. To meet these chal- lenges, this study encourages further research to refine the instrument developed, improve the methodology, and strengthen the external and internal validity.
An important finding of this study was the identification of Dilemma 6 (“Fos- tering independence of the client to solve his or her problems conflicts with the client’s cultural expectation that the counselor will offer solutions”) as a central multicultural ethical issue because of the frequency with which it was encountered and the significance counselors rated it for inclusion in training. This dilemma was encountered by 86% of the respondents at least once a year.
186 JOURNAL OF MULTICULTURAL COUNSELING AND DEVELOPMENT July 2003 Vol. 31

The importance of this dilemma identifies a fundamental cultural tension be- tween traditional counseling culture and the cultures of some multicultural clients regarding the values of independence versus interdependence. The Western counseling philosophies exemplified in most cognitive-behavioral, humanistic-existential, and psychodynamic modalities are deeply embedded in the beliefs of individualism and empowerment (Ivey, Ivey, & Simek-Mor- gan, 1996). Counselors have traditionally taught clients to take responsibility and ownership for their lives, although this value is not always shared by cli- ents coming from collectivist cultures. Given that independence is a strong American value, counselors should be aware of how their own values, beliefs, attitudes, and personality styles may influence how they behave with clients from more collectivistic cultures.
Dilemma 7 (“Achieving credibility with the client requires that the counselor compartmentalize his or her counseling values conflicts with the counselor main- taining his or her counseling values, although the result would be a loss of credibil- ity”) was also identified as paramount because of the high frequency with which it was encountered and the high rating of significance for inclusion in training materials. This suggests that counselors encountering this dilemma are likely to experience internal conflict and tension when struggling with their own values in relation to the values of their clients. This may mean that counselors are conflicted when trying to remain genuine and provide unconditional positive regard to cli- ents who hold different cultural values. Counselors may experience discomfort when compartmentalizing their counseling values while faced with clients who require the counselor to operate from a set of values that are more congruent with the client’s culture. When a counselor chooses to allow his or her values to be reflected in the counseling setting, the client who is from a different culture may feel misunderstood or may decide not to continue receiving counseling services. This may create dissonance for the counselor. Although this dissonance may not be alleviated, an understanding of its source may be beneficial.
One explanation for these two dilemmas having been identified as central may be that these dilemmas are also manifested in counseling situations in which the counselor and the client are of the same culture. However, with multicultural clients, the resolution of these two dilemmas may have much more significant consequences. If counselors choose to uphold their counsel- ing values in spite of being incongruent with the client’s values, the multicultural client may view counseling as not only ineffective but also as discriminatory.
Dilemma 1 (“The counselor and client are faced with the client needing to choose between working on the symptoms of his or her emotional problems arising from a discrimination situation that has negative consequences, which conflicts with empowering the client to assert his or her civil rights although it could result in negative consequences for the individual”) was identified as the second most significant dilemma to be included in training materials. As Pedersen (1997) and others have emphasized, it is important to deal with the
JOURNALOF MULTICULTURAL COUNSELING AND DEVELOPMENT July 2003 Vol. 31 187
oppression multicultural clients regularly experience. It is also important for counselors to recognize how clients’ experience of oppression can become a core part of their psychological makeup. To ignore this would be unethical. One suggestion for resolving this dilemma is for counselors to assume an ad- vocacy role on behalf of their multicultural clients. The resolution of this di- lemma would be more systemic than personal. That is, by working as agents of social change to make a difference socially and politically concerning cul- turally related issues, counselors can both reduce the tension of this dilemma and empower their multicultural clients.
This research identified a number of dilemmas that were important for in- cluding in training materials for counselors in specific professional settings. Comparisons of counselors’ ratings determined that public agency counselors encountered Dilemma 3 (“The counselor and client are faced with the client needing to choose between ending an abusive marriage although it will result in him or her being a social outcast within the traditional social culture, which conflicts with helping the client to stay in a marriage and cope with the situ- ation”) significantly more than school, rehabilitation, university/college, pri- vate, drug and alcohol, career, and those designating a different professional category. This finding is congruent with the difficult family circumstances that are prevalent among clients who seek services from public counseling agen- cies. The greater prevalence of this dilemma among public agency counselors suggests that these counselors become more involved with cases of domestic violence, often with clients who may come from diverse backgrounds. Increasing public agency counselors’ awareness of this ethical tension may help them to seek support among community leaders of cultural groups who may offer al- ternative ways of ending abusive situations rather than ending a marriage or allowing an abusive relationship to continue.
For drug and alcohol counselors, Dilemma 7 (“Achieving credibility with the client requires that the counselor compartmentalize his or her counseling values conflicts with the counselor maintaining his or her counseling values, although the result would be a loss of credibility”) was encountered significantly more frequently than it was for school, rehabilitation, university/college, private, pub- lic agency, career counselors, and those designating a different professional cat- egory. This dilemma may be encountered by drug and alcohol counselors on a more frequent basis because the clients they assist may present with more char- acteristics that are devalued by mainstream culture. For many U.S. citizens, drug and alcohol problems are seen as a moral failing (Benshoff & Janikowski, 2000). This moral defect perspective, coupled with the stereotypes individuals have of people from minority backgrounds such as a lack of Protestant work ethic (e.g., punctuality, diligence, achievement, repression of immediate needs for long- term success), may pose too many conflicts of values for a counselor to compart- mentalize. Having this dilemma as a part of their training curriculum would give counselors a chance to sort out what these value conflicts are before they begin
188 JOURNALOFMULTICULTURAL COUNSELING AND DEVELOPMENT July 2003 Vol. 31
counseling individuals who come from multicultural backgrounds and who have drug and alcohol problems. Perhaps drug and alcohol counselors need to sepa- rate cultural values that may have an important place in a client’s life from behaviors that sustain a dependence on chemicals.
Comparisons of counselors’ ratings determined that counselors in the private professional setting rated Dilemma 4 (“The counselor and client are faced with the client needing to choose between seeking treatment based on a Western medical practice to avoid negative health consequences, which conflicts with the client’s cultural beliefs about health and illness”) as significant for inclu- sion in training materials more than school, rehabilitation, university/college, public agency, career counselors, and those designating a different professional category. The higher rating of this dilemma suggests that private practice coun- selors are called on more often to interact with the medical community. Per- haps private practice counselors are asked to assist when medical treatment teams are faced with particularly difficult cases that require ethical decision making regarding multicultural clients. An exploration of this dilemma by pri- vate practice counselors may give them greater insight into the dynamics of such issues. The higher ratings by private counselors suggests that they en- counter a medical model (i.e., diagnoses, treatment, cure) more often than do agency and school counselors. The medical model may be in conflict with multicultural values more often than other approaches. Training private coun- selors to take a systems approach to counseling may provide greater insight into this ethical issue.
1
The results of this study have important implications for the practice of coun- seling, the continued improvement of counselor training programs, and re- search applications. The eight multicultural ethical dilemmas identified in this study are encountered by practicing counselors on a fairly frequent basis. Pro- viding in-service training, workshops, and continuing education opportunities for practicing counselors with these multicultural ethical dilemmas as the basis for open discussions, analysis, and clarification would enhance the delivery of counseling services to the expanding diverse population of the United States. Practicing counselors cannot face the multicultural ethical challenges as posed by these dilemmas on an individual basis. Participating in an intensive analyti- cal process with the multitude of perspectives that a group of counselors can bring to the resolution of these dilemmas would be a fertile process.
Furthermore, the ethical dilemmas identified by seasoned counselors in this study, as ones they have faced and view as important in their work, can help counselors-in-training prepare for real-world situations. The respondents indi- cated that all of the dilemmas should be included in training materials. As counseling programs increasingly focus on competency-based skills, the abil-
JOURNAL OF MULTICULTURAL COUNSELING AND DEVELOPMENT July 2003 Vol. 31 189

ity to successfully negotiate multicultural ethical dilemmas should be consid- ered a task requiring proficiency. Counseling programs that are committed to including diversity issues in their curriculum must recognize the importance of preparing students for the ethical situations that arise in multicultural coun- seling. The dilemmas identified in this study can help bolster the training materials used in teaching multicultural counseling.
The results of this study can also help the development of the profession by leading to refinement of the existing codes of ethics. This type of refinement has been suggested by Pedersen (1997). Although the codes of ethics address the importance of culturally sensitive counseling, they are often vague when it comes to assisting counselors in dealing with real dilemmas that arise in multicultural counseling situations. By using the information from this study, the ethical codes may be further enhanced to reflect the essence of multicultural ethical dilemmas and provide assistance in resolving those dilemmas. This would be of great benefit to the profession and the clientele served.
Lastly, this research is only a beginning. Understanding the multicultural value conflicts that emanate when individuals and groups from culturally di- verse backgrounds come together in relationships, neighborhoods, communi- ties, and across borders is crucial. The counselors who responded to this study only make up a small slice of the total worldview. Research should be con- ducted with individuals in other professional groups to identify the ethical dilemmas they face as they deliver services. However, identifying multicultural ethical dilemmas will not solve problems. Cottone (2001) and Meara et al. (1996) have proposed models for ethical decision making that may assist coun- selors in the resolution of these multicultural dilemmas. Further research should be aimed at determining the effectiveness of the models in their application to these and other multicultural dilemmas.
Arredondo, P. (1985). Cross-cultural counselor education and training. In P. B. Pedersen (Ed.), Handbook ofcross-culturalcounseling and therapy (pp. 281 -289). Westport, CT: Greenwood Press.
Arredondo, P. (1994). Multicultural training: A response. The Counseling Psychologist, 2,308-314. Arredondo, P., Toporek, R., Brown, S., Jones, J., Lock, D. C., Sanchez, J., & Stadler, H. (1996).
Operationalization of the multicultural counseling competencies.Journa1 OfMulticultural Coun- seling and Development, 24, 42-78.
Atkinson, D. R. (1994). Multicultural training: A call for standards. The Counseling Psychologist,
Axelson, J. A. (1999). Counseling and develojmenl in a multicultural society (3rd ed.). Pacific Grove, CA: Brooks/Cole.
Beauchamp, T. L., & Childress, J. F. (1994). Principles of biomedical ethiw (4th ed.). Oxford, En- gland: University Press.
Benshoff, J. J., & Janikowski, T. P. (2000). Z7ze rehabilitation model of substance abuse counseling. Belmont, CA: Brooks/Cole
Casas, M., Ponterotto, J. G., & Gutierrez, J. M. (1986). An ethical indictment of counseling research and training: The cross-cultural perspective. Journal of Counseling and Development, 64, 347-349.
21,257-277.
190 JOURNAL OF MULTICULTURAL COUNSELING AND DEVELOPMENT July 2003 Vol. 31
Cayleff, S. E. (1986). Ethical issues in counseling gender, race, and culturally distinct groups. Journal of Counseling and Development, 64, 345-347.
Cohen, R. J., Swerdlik, M. E., & Phillips, S. M. (1996). Psychological testing and assessment (3rd ed.). Mountain View, CA: Mayfield.
Cottone, R. R. (2001). A social constructivism model of ethical decision making in counseling. Journal of Counseling d Development, 79, 39-45.
Cottone, R. R., & Claus, R. E. (2000). Ethical decision-making models: A review of literature. Journal of Counseling d Development, 78, 275-283.
Fitzgerald, L. F., & Nutt, R. (1986). The Division 17 principles concerning the counseling/psycho- therapy of women: Rationale and implementation. The Counseling Psychologist, 14, 180-216.
Goodyear, R. K., Crego, C. A,, &Johnston, M. W. (1992). Ethical issues in the supervision of student research: A study of critical incidents. Professional Psychology: Research and Practice, 23, 203-210.
Hinman, L. M. (2001). The place of race, ethnicity, and culture in moral theory. Retrieved June 13, 2003, from http://ethics.acusd.edu/presentations/Theory/race/race.ppt
Ibrahim, F. A., & Arredondo, P. M. (1986). Ethical standards for cross-cultural counseling: Counselor preparation, practice, and research. Journal of Counseling and Development, 64, 349-352.
hey, A. E., hey, M. B., & Simek-Morgan, L. (1996). Counseling and psychotherapy: Integrating skills, theory, andpractice (4th ed.). Englewood Cliffs, NJ: Prentice-Hall.
Jordan, A. E., & Meara, N. M. (1990). Ethics and the professional practice of psychologists: The role of virtues and principles. Professional Psychology: Research and Practice, 21, 107-1 14.
Kitchener, K. S. (1984). Intuition, critical evaluation and ethical principles: The foundation for ethical decisions in counseling psychology. The Counseling Psychologist, 12, 43-55.
Kitchener, K. S. (1992). Psychologist as a teacher and mentor: Affirming ethical values through- out the curriculum. Professional Psychology: Research and Practice, 23, 190-195.
Linstone, H., & Turoff, M. (1975). The Delphi method: Techniques and applications. Reading, MA: Addison-Wesley.
Meara, N. M., Schmidt, L. D., & Day, J. D. (1996). Principles and virtues: A foundation for ethical decisions, policies, and character. 7%e Counseling Psychologist, 24, 4-77.
Pedersen, P. (1994). A handbookfor developing multicultural awareness (2nd ed.). Alexandria, VA: American Counseling Association.
Pedersen, P. (1997). The cultural context of the American Counseling Association code of eth- ics. Journal of Counseling &Development, 76, 23-28.
Ponterotto, J. G., & Casas, J. M. (1987). In search of multicultural competence within counselor education programs. Journal of Counseling and Development, 65, 430-434.
Pope, K. S., & Vetter, V. A. (1992). Ethical dilemmas encountered by members of the American Psychological Association. American Psychologist, 47, 397-41 1.
Ridley, C. R., Mendoza, D. W., & Kanitz, B. E. (1994). Multicultural training: Reexamination, operationalization, and integration. The Counseling Psychologist, 2, 227-289.
Smith, E. (1982). Counseling psychology in the marketplace: The status of ethnic minorities. The Counseling Psychologist, 10, 61 -67.
Sue, D. W., Bemier, T. E., Drurran, A., Feinber, L., Pedersen, P., Smith, E. T., et al. (1982). Position paper: Cross-cultural counseling competencies. Z2e Counseling Psychologist, 70, 45-52.
Sue, D. W., & Sue, D. (1990). Counseling the culturally different: Theory andpractice. New York: Wiley.
Sue, S. (1977). Community mental health services to minority groups: Some optimism, some pessimism. American Psychologist, 32, 616-624.
Sue, S., & Zane, N. (1987). The role of culture and cultural techniques in psychotherapy: A reformulation. American Psychologist, 42, 37-45.
Welfel, E. R. (1992). Psychologist as ethics educator: Successes, failures, and unanswered ques- tions. Profssional Psychology: Research and Practice, 23, 182-189.
JOURNAL OF MULTICULTURAL COUNSELING AND DEVELOPMENT July 2003 Vol. 31 191
Recommended