Evaluating Adenopathy:When to Worry and What to Do
Kate Kolibaba, M.D.Northwest Cancer Specialists
Vancouver, [email protected]

Adenopathy: Objectives
Lymphatic system basicsCauses of lymphadenopathyEvaluation

The Lymphatic System

What is the Lymphatic System?
Network of organs, such as the tonsils, spleen, liver, bone marrow and lymphatic vessels that connect “glands”, the lymph nodes
Lymph nodes located throughout the bodyLymph nodes filter foreign particles out of the
lymphatic fluid Contain B and T lymphocytes

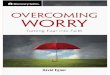
Lymph Node - Normal Histology
afferent lymphatic vessel capsule
follicle (mainly B-cells)- germinal centre- mantle zone
C
cortex
medullaparacortex
efferent lymphatic vessel
artery
vein

Lymphatic Tissue
Lymphocytes originate in bone marrow
Lymphocytes undergo proliferation and differentiation in lymphoid tissue
• B-lymphocytes- tend to reside in lymph nodes & spleen
• T-lymphocytes- tend to circulate throughout the lymphatic system

Lymphocytes
20% of white blood cells are lymphocytesMost lymphocytes are in lymph nodes, spleen,
bone marrow and lymphatic vesselsT cells, B cells, natural killer cells
• B cells produce antibodies• T cells help B cells produce antibodies and fight
viruses

Lymphadenopathy
Enlargement or change in texture of a lymph nodes
Adenopathy• Benign vs. malignant• Require treatment
Evaluation

Goals of Evaluation
Identify the infrequent but serious causes of lymphadenopathy• History, including exposures• Age of patient• Location

Differential Diagnosis
MIAMI• Malignancy• Infection• Autoimmune• Miscellaneous-sarcoidosis, hyperthyroidism• Iatrogenic-serum sickness, medications

Infectious Causes of Adenopathy
Tuberculosis
Bacterial• Brucellosis, cat-scratch, STDs
Viral• HIV, hepatitis, CMV, EBV, rubella

Autoimmune Causes of Adenopathy
Lupus erythematosis
Rheumatoid arthritis
Dermatomyositis
Sjogren’s syndrome

Drugs Associated with Adenopathy
allopurinol
atenolol
captopril
carbamazepine
gold
hydralazine
penicillins
phenytoin
primidone
pyrimethamine
quinidine
Trimethoprim/sulfa-methoxizole
sulindac

Likelihood of Malignancy
Series of patients having biopsy:• 21% in patients under 30• 41% in patients 31-50• 61% in patients over 50
Lee et al; J Surg Oncol 1980; 14: 53 – 60

Likelihood of Malignancy
Lymphadenopathy that lasts
< 2 weeks or > one year
with no size increase
is unlikely to be neoplastic

Associated Symptoms
Fever, night sweats, weight loss• “B” symptoms, lymphoma
Fatigue, malaise, fever• Atypical lymphocytosis,
mononucleosis
Arthralgias, weakness, rash• autoimmune

Physical Examination
Supraclavicular most likely to be malignant• 54-85% neoplastic in biopsy series

Axillary and Inguinal Adenopathy
Drain extremities
Often nonspecific, reactive
Up to 2 cm can be normal

Nodal Character
There is no specific size threshold that raises suspicion
Hard, painless• Malignant (metastatic) or granulomatous
Rubbery• Lymphoma

Evaluation of Adenopathy
Results of initial assessment• Benign or self-limited disease• Autoimmune or serious infectious• Malignancy• Unexplained
Bazemore and Smucker, Am Fam Physician 2002; 66: 2103-2110.

Evaluation of Adenopathy
Empiric treatment• Often antibiotics and/or corticosteroids
are prescribed, but no data exists to support this approach

Benign or Self-Limited Disease
Treatable
Yes No
Treat Reassurance,appropriately explain course of disease
Offer follow-up for persistent or changing adenopathy

Suspected Autoimmune or Serious Infectious Disease
Specific Testing
Positive Negative
Treat Seeappropriately “Unexplained”

Suspected Malignancy
Biopsy
Positive Negative
Treat Seeappropriately “Unexplained”

Unexplained Adenopathy
Review risk factors for malignancy
If high risk, proceed with excisional biopsy

Unexplained Adenopathy
Low Risk for Malignancy
Generalized Regional
Referral or Follow-up

Unexplained Generalized Adenopathy
Consider miscellaneous causes• Sarcoidosis• Silicosis, berylliosis• Storage diseases: Gaucher, Fabry’s• Hyperthyroidism, hypertriglyceridemia• Kawasaki syndrome

Unexplained Generalized Adenopathy
Positive Negative
Biopsy most abnormal node Treat
CBC, RPR, PPD, HIV, HBsAg, ANA
Positive Negative
Follow-up

More About Biopsies
FNACore needle biopsyExcisional biopsy

Fine Needle Aspiration
FNA - Fine Needle Aspiration• Simple - 21-23 gauge needle,5-10 cc
syringe• Relatively atraumatic• Sensitivity of 73-99%• Ideal for simple cyst aspiration• Can’t distinguish in-situ vs invasive cancer• Can confirm relapse of known cancer

Core Needle Biopsy
CNB - Core Needle Biopsy• 14 - 20 gauge cutting needle• greater trauma• high sensitivity – 80-100%• distinguishes between invasive and
in-situ• Diagnostic of many malignancies• Non-diagnostic for lymphoma• Avoid bone

Open Biopsy
Open Biopsy (incisional or excisional)• any suspicious finding• clinical or radiologic finding with negative FNA
or CNB• atypia on FNA or CNB
- 20-50% malignancy on open biopsy
• recurring cyst, enlarging node

Adequate Biopsy is Critical
Open biopsy required to discern reactive (benign) from malignant lymphoid disorder
Open biopsy required for lymphoma• Diagnosis must be biopsy-proven before
treatment is initiated• Need enough tissue to assess architecture• FNA is never adequate

Diagnosing Lymphoma
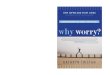
Nodular (follicular) Diffuse
small cell large cell
Indolent Aggressive

Lymph node biopsy – Follicular NHL

A practical way to think of lymphoma
Category Survival of untreated patients
Curability To treat or not to treat
Non-Hodgkin lymphoma
Indolent Years Generally not curable
Generally defer Rx if asymptomatic
Aggressive Months Curable in some
Treat
Very aggressive
Weeks Curable in some
Treat
Hodgkin lymphoma
All types Variable – months to years
Curable in most
Treat

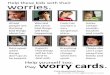
Relative Frequencies of Lymphoma
HodgkinLymphoma 15%
NHL
Diffuse large B-cell
Follicular
Other NHL
Non-Hodgkin Lymphomas 85%
~85% of NHL are B-lineage
Recommended