EZOGABINE: A NEW ANGLE ON POTASSIUM
GATE
DR.JITENDRA AGRAWALFIRST YEAR RESIDENT

Epilepsy is among the most common neurological disorders, affecting approximately 50 million people worldwide. Partial onset seizure are the most common type of seizures in adults.
SEIZURE: is a paroxysmal event due to abnormal, excessive, hyper synchronous discharges from an aggregate of central nervous system, neurons.
EPILEPSY: describes a condition in which a person has recurrent seizures due to chronic underlying process.
INTRODUCTION

1. Partial seizures a. Simple partial seizures (with motor,
sensory, autonomic, or psychic signs) b. Complex partial seizures c. Partial seizures with secondary
generalization
Classification of seizure

2. Primarily generalized seizures a. Absence (petit mal)b. Tonic-clonic (grand mal)c. Tonic d. Atonice. Myoclonic 3. Unclassified seizures f. Neonatal seizures g. Infantile spasms
Classification of seizure

are those in which the seizure activity is restricted to discrete areas of the cerebral cortex.
SIMPLE PARTIAL SEIZURES: Clinical manifestation + consciousness is fully
preserved during seizures COMPLEX PARTIAL SEIZURES focal seizure activity + impairment of
conciousness PARTIAL SEIZURES WITH SECONDARY
GENERALIZATION seizures that begin as partial seizures and then
spread diffusely throughout the cortex
Partial Seizures

Pharmacological therapy is initial option for the treatment of patients with newly diagnosed epilepsy.
Focused area is to reduce seizure frequency with seizure freedom is ultimate goal.
without side effects. Monotherapy is preferable.
CURRENT STATUS OF TREATMENT

First-Line
a. Carbamazepine b. Phenytoin c. Lamotrigine d. Oxcarbazepine e. Valproic acid
CURRENT STATUS OF TREATMENT
Alternatives
a. Levetiracetamb. Topiramatec. Tiagabined. Zonisamidee. Gabapentinf. Phenobarbital g. Primidone h. Felbamate

Epilepsy a serious and potentially life threatening condition
In spite of many approved pharmacological agents, many patients are not adequately treated with currently available option.
Nearly a third patients with epilepsy have either intractable or uncontrolled seizures or have significant adverse side effects secondary to medication.
Why need of new drug?

Monotherapy is preferable to limit drug drug interactions and side effects… but
Epilepsy patient need more than one AED to achieve therapeutics success.
In spite of that adequate seizure control is not achieved.
So the new drug should have minimal drug interactions and minimal side effect
Why need of new drug?

Synonyms:Retigabine-(INN- international nonproprietary
name)
Ezogabine- (USAN- U.S. adopted name)
EZOGABINE: As an adjunctive therapy to partial onset seizures.

Recently approved as an adjunctive treatment for partial onset seizure for patients by
FDA in June 2011
EMEA in March 2011
EZOGABINE

Opening of neuronal voltage-gated potassium channels, which enhances inhibitory M-type potassium current.
The principal mechanism by which membrane repolarisation occurs after an action potential is an outward potassium current, termed the M-current .
Selectively enhance M-currents through KCNQ2/3 and KCNQ3/5
No effect on KCNQ1- present in cardiac cells KCNQ4-present in auditory system
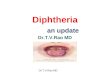
EZOGABINE- mechanism of action

Does not directly open the potassium channel
Act as prop or doorstop
Binding into hydrophobic pocket within ‘’gate’’ region of Kv7.2 and 3 channles
Wihich is the site for molecular ‘’hinge’’
Once lodges within this pocket
It bends the hinge slightly open
Decreasing the angle through which the gate must swing to full open.

Linear pharmacokinetic profile with dosage up to 1200mg/day
Rapidly absorbed after oral administration Bioavailibility of oral EZG is about 60% Protien binding is approximately 80% Volume of distribution at steady state is
about 2-3 L/kg
Pharmacokinetics

Metabolized by: N-acetylation to the mono-acetylated metabolite, glucuronidation to form N-glucronide structure Metabolites have minimal pharmacological activity
Majority of drug and metabolites excreted through kidney. Small amount excreted through feces.
Plasma half life is 8 hrs for drug and metabolites.
Pharmacokinetics

May increase the QTc interval.
PHARMACODYNAMICS

Low potential for drug interaction No potential to inhibit major cytochrome
P450 isoenzyme. It is neither substrate nor inhibitor of P-
glycoprotein transporter.
Drug interactions

No clinically significant effects of the following AEDs on Ezogabine pharmacokinetics:
Carbamazepine Levetiracetam Oxcarbazepine Phenobarbitol Phenytoin Topiramate Valproate
Drug interactions

However lamotrigine increase 15% concentration of ezogabin
Ezogabine plasma levels may be reduced by concomitant administration of phenytoin or carbamazepine.
N-acetyl metabolite of ezogabine may inhibit renal clearance of digoxin
Drug interactions

Indicated for adjunctive treatment for Partial onset seizures With or without generalization For patients 18 years of age and older.
INDICATION

Patients can be considered drug resistant when
Failed to have seizure control with 2 or more AEDs
Used appropriately Tolerated by the patient.
INDICATION

The initial dosage should be 100 mg 3 times daily (300 mg per day) for 1 week.
Titrate to maintenance dosage by increasing the dosage at weekly intervals by no more than 150 mg per day.
Optimize effective dosage between 200 mg 3 times daily (600 mg per day) to 400 mg 3 times daily (1,200 mg per day).
DOSAGE AND ADMINISTRATION

When discontinuing EZOGABINE, reduce the dosage gradually over a period of at least 3 weeks.
Dosing adjustments are required for geriatric patients and patients with moderate to severe renal or hepatic impairment.
DOSAGE AND ADMINISTRATION

Most frequent Somnolence Dizziness Confusion Asthenialess frequent Speech disorder Vertigo Tremor Amnesia
ADVERSE DRUG REACTION

Urinary retention Urinary hesitancy This is because of Inhibition of bladder contractility secondary
to ezogabine’s effect on KCNQ channels in detrusor muscle of the bladder.
ADVERSE DRUG REACTION

urologic symptoms should be carefully monitored.
Closer monitoring is recommended for, benign prostatic hyperplasia [BPH] cognitively impaired patients anticholinergics
PRECAUTION

Monitor for dizziness and somnolence QT prolongation: QT interval should be
monitored in patients taking concomitant medications known to increase the QT interval or with certain heart conditions.
when EZOGABINE is discontinued, it should be withdrawn gradually when possible to minimize the potential of increased seizure frequency
PRECAUTION

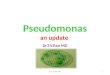
STUDY 205:A multicenter, randomized, double-blind, placebo-controlled trial was performed of retigabine for partial-onset seizures.
CONCLUSION: Adjunctive therapy with retigabine is well tolerated and reduces the frequency of partial-onset seizures in a dose-dependent manner.
CLINICAL TRIALS

Study 301: multicenter, randomized, double-blind, parallel-group trial of ezogabine (retigabine) in partial epilepsy.
CONCLUSION: EZG(RTG) is effective as add-on therapy for reducing seizure frequency in patients with drug-resistant partial-onset seizures.
CLINICAL TRIALS

STUDY 302: This was a multicenter, randomized, double-blind, placebo-controlled trial in adults with ≥4 partial-onset seizures per month receiving 1 to 3 antiepileptic drugs.
CONCLUSIONS: In this dose-ranging, placebo-controlled trial, adjunctive EZG (RTG) was effective and generally well tolerated in adults with refractory partial-onset seizures
CLINICAL TRIALS

Percent Change from Baseline in Total Partial Seizure Frequency(Double-Blind Phase) – ITT Population for Study 205 and ITT Double-Blind Population for Studies 301 and 302

first antiepileptic drug with a very specific effect on central nervous system potassium channels.
Having minimal drug interactions Mostly renal excretion few safety concerns most side effects are those typically seen
with antiepileptic agents.
Conclusion

There are no adequate and well-controlled studies in pregnant women.
conclusion

Harrision’s principles of internal medicine, 17th edition
Ezogabine: A New Angle On Potassium Gates.Epilepsy Currents, Vol. 11, No. 3 (May/June) 2011 pp. 75–78© American Epilepsy Society.
Porter RJ, Partiot A, Sachdeo R, Nohria V, Alves WM. Randomized, multicenter, dose-ranging trail of retigabine for partial-onset seizures. Neurology. 2007;68:1197-204.
REFERENCES

French J, Abou-Khalil B, Leroy R, Yacubian E, Shin P, et al. Randomized, double-blind, placebo-controlled trial of ezogabine (retigabine) in partial epilepsy. Neurology. 2011 May 3;76(18):1555-63.
Brodie M, Lerche H, Gil-Nagel A, Elger C, Hall S, et al. Efficacy and safety of adjunctive ezogabine (retigabine) in refractory partial epilepsy. 2010 Nov.Neurology. 16:75:1817-24.
Wikipedia and various internet sites Steve chung, kirsten M Kelly, Courtney Schussee;
Neurology research international journal, 20 june 2011.
REFERENCES

THANK YOU




Recommended