Facial Paralysis and Contemporary
Management
Michael Hall, MD Grand Rounds
PGY-3 May 13, 2015
Overview
• Anatomy
• General Concepts
• Causes
• Treatment Options
• Static
• Dynamic
• Management of the…
• Brow
• Eyelids
• Mid-Lower Face
• Rehab
• Complications and Management of Synkinesis
• Future Direction and Research
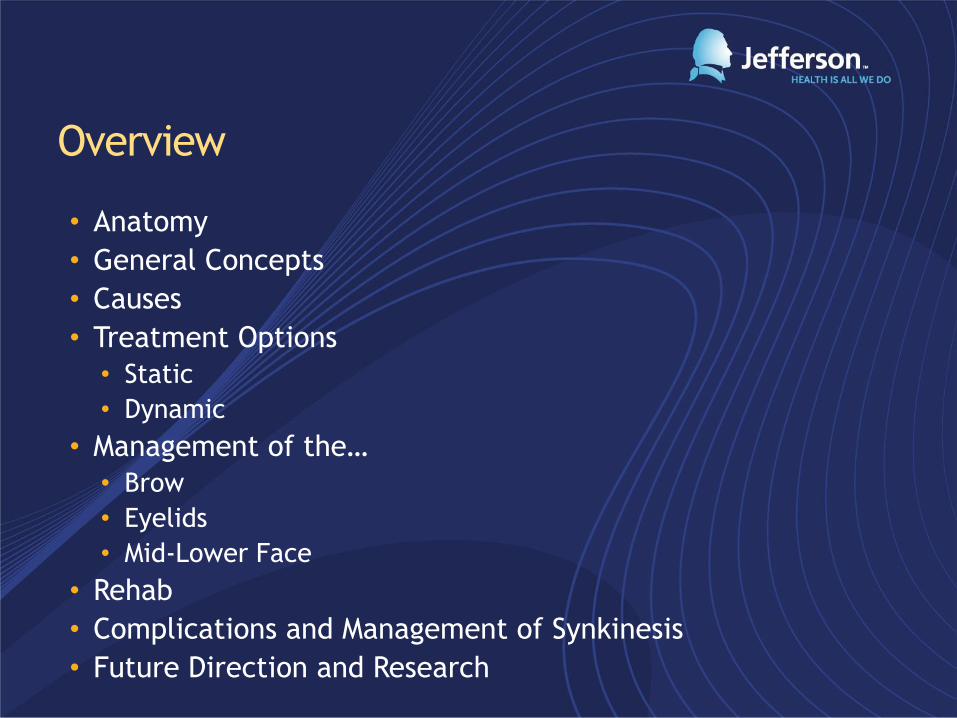
Anatomy
Major
Minor
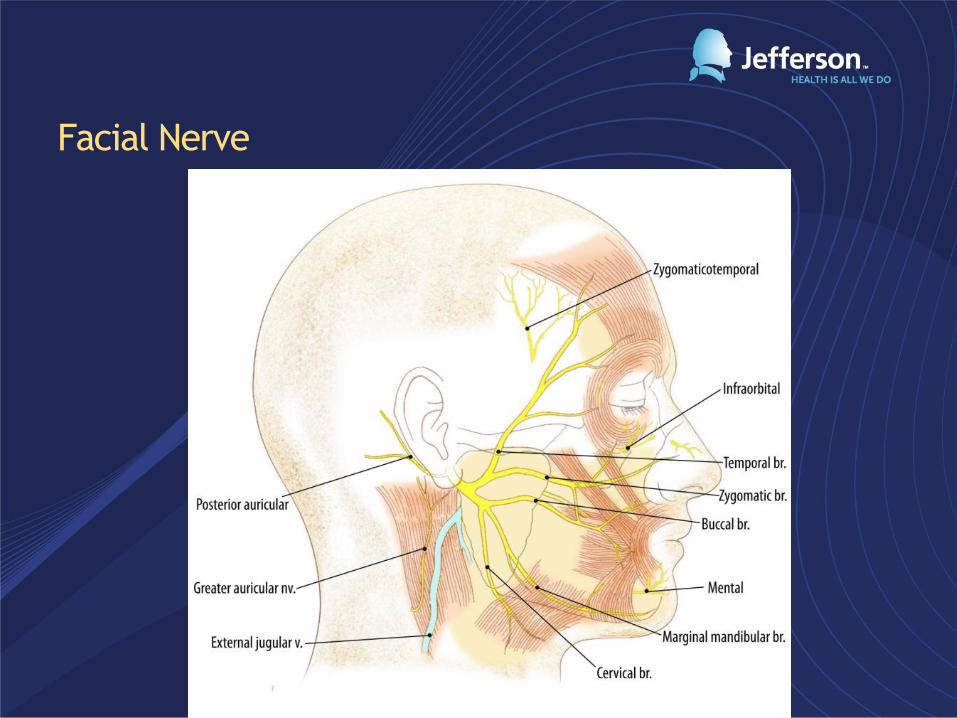
Facial Nerve
General Concepts
• Multiple etiologies
• Diverse presentation
• Not life threatening
• Severe QOL implications and psychological impact
• Prognosis and outcomes variable
Etiology
• Idiopathic
• Infection
• Trauma
• Iatrogenic
• Metabolic
• Toxic
• Vascular
• Neurologic
• Otologic
• Congenital
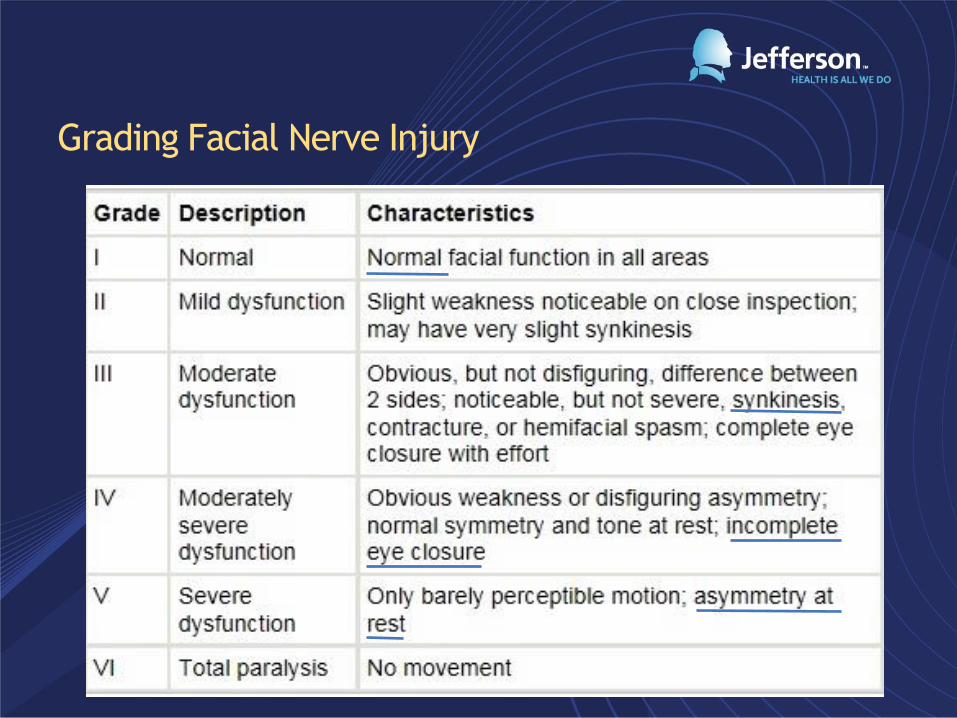
Grading Facial Nerve Injury
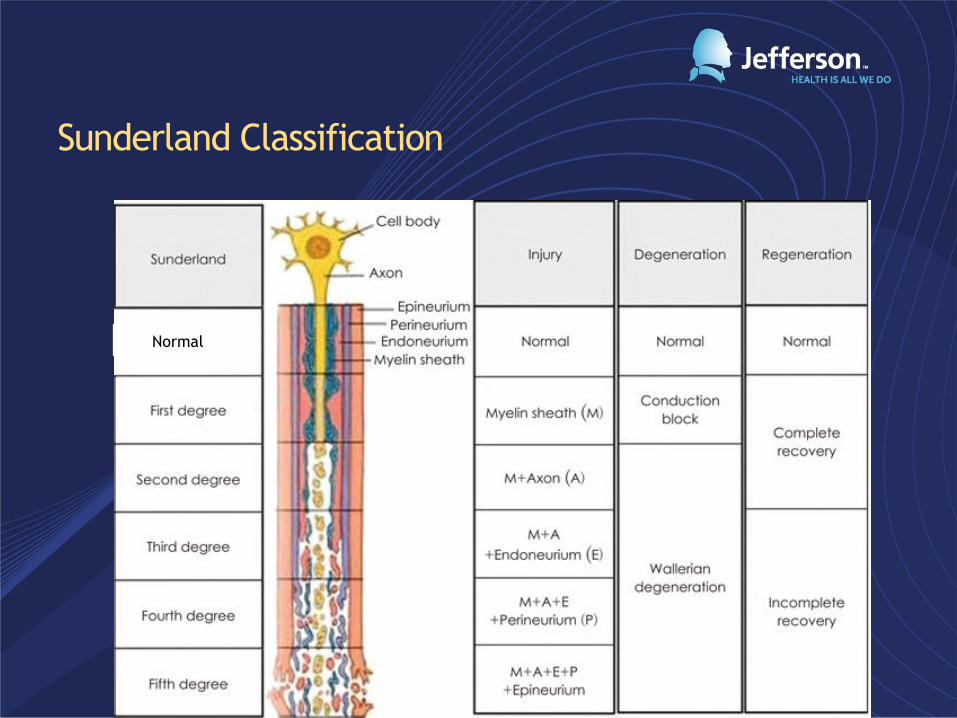
Sunderland Classification
Normal
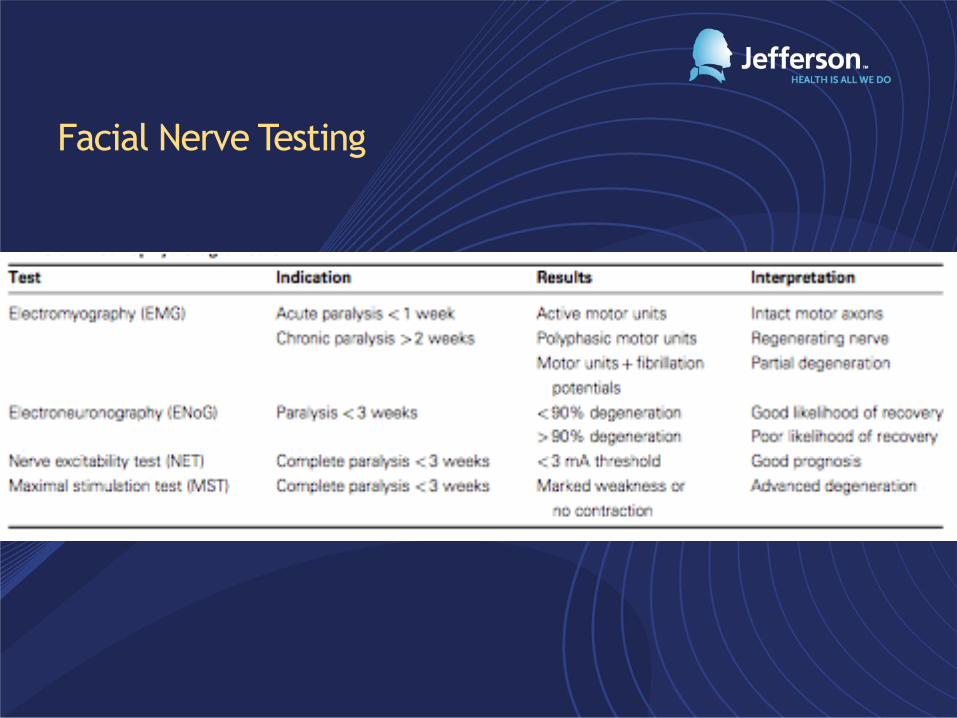
Facial Nerve Testing
Treatment Options
• Observation
• Conservative
• Prednisone: 1mg/kg per day for 7-10 days with slow taper
• Acyclovir/Valcyclovir
• Chemodenervation, Fillers
• Direct Nerve Repair and Cable Grafting
• Static Procedures
• Facial Sling, Gold Weight
• Dynamic Procedures
• Nerve, muscle or free tissue transfer
Timing and Considerations with Facial Paralysis
• Patient Age
• Onset
• Immediate
• Delayed
• Duration
• Involved Branches
• Progression
• Complete
• Incomplete
• Patient Expectation
• Status of the Eye
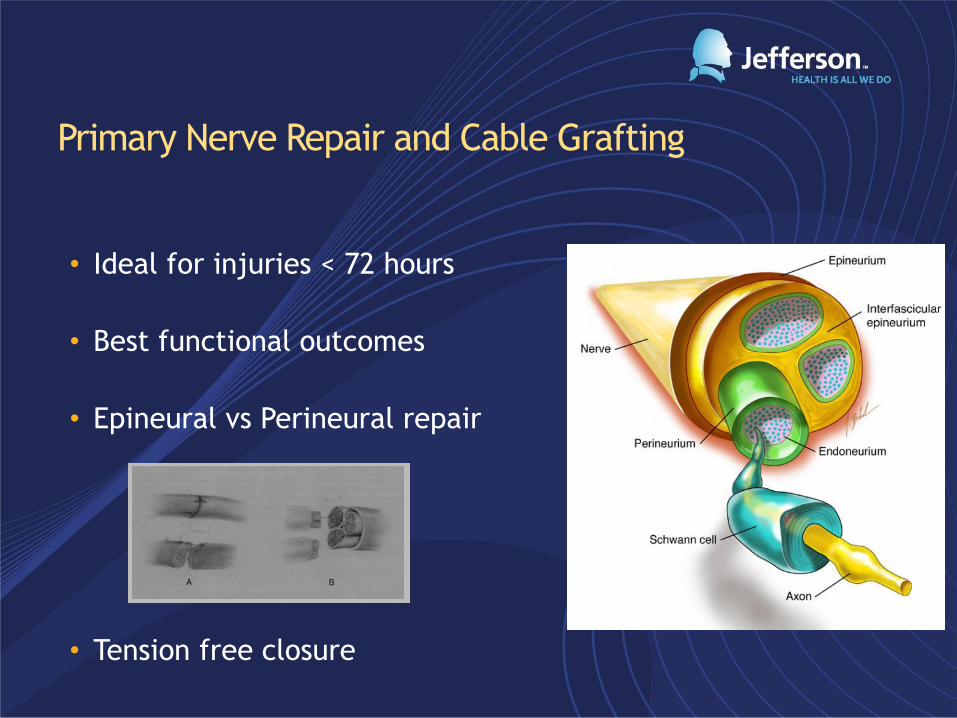
Primary Nerve Repair and Cable Grafting
• Ideal for injuries < 72 hours
• Best functional outcomes
• Epineural vs Perineural repair
• Tension free closure
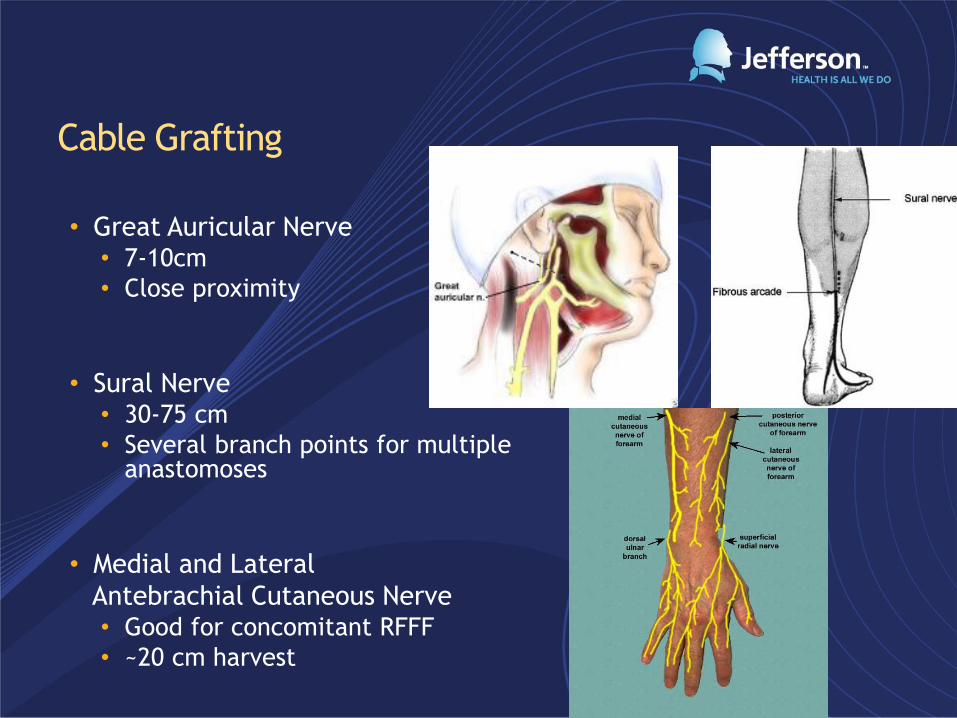
Cable Grafting
• Great Auricular Nerve • 7-10cm
• Close proximity
• Sural Nerve • 30-75 cm
• Several branch points for multiple anastomoses
• Medial and Lateral
Antebrachial Cutaneous Nerve • Good for concomitant RFFF
• ~20 cm harvest
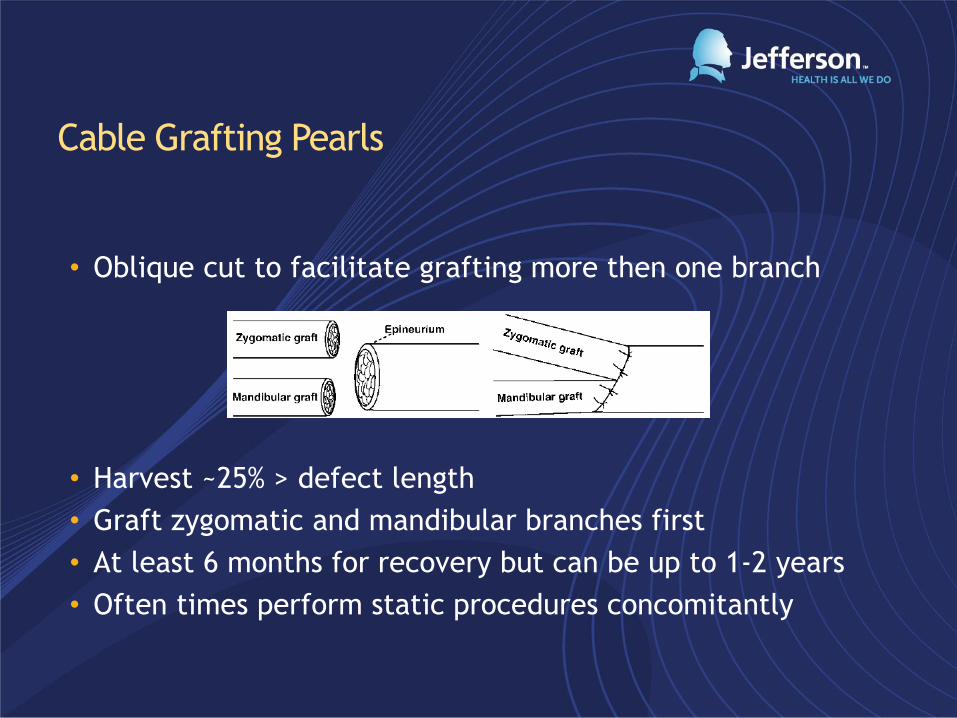
Cable Grafting Pearls
• Oblique cut to facilitate grafting more then one branch
• Harvest ~25% > defect length
• Graft zygomatic and mandibular branches first
• At least 6 months for recovery but can be up to 1-2 years
• Often times perform static procedures concomitantly

Matteo or Davis
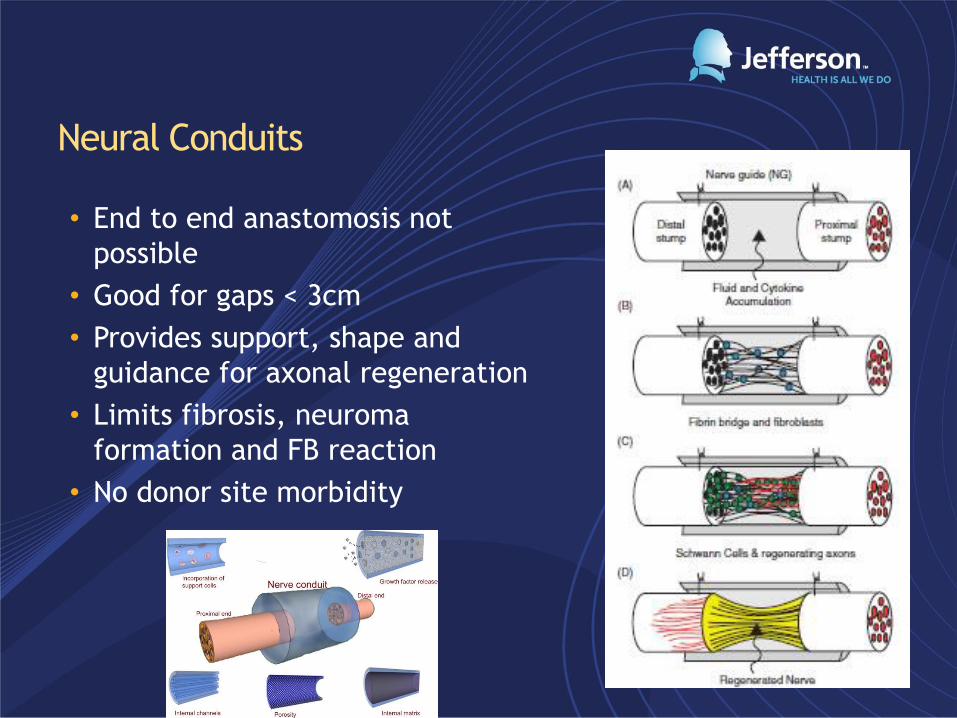
Neural Conduits
• End to end anastomosis not
possible
• Good for gaps < 3cm
• Provides support, shape and
guidance for axonal regeneration
• Limits fibrosis, neuroma
formation and FB reaction
• No donor site morbidity
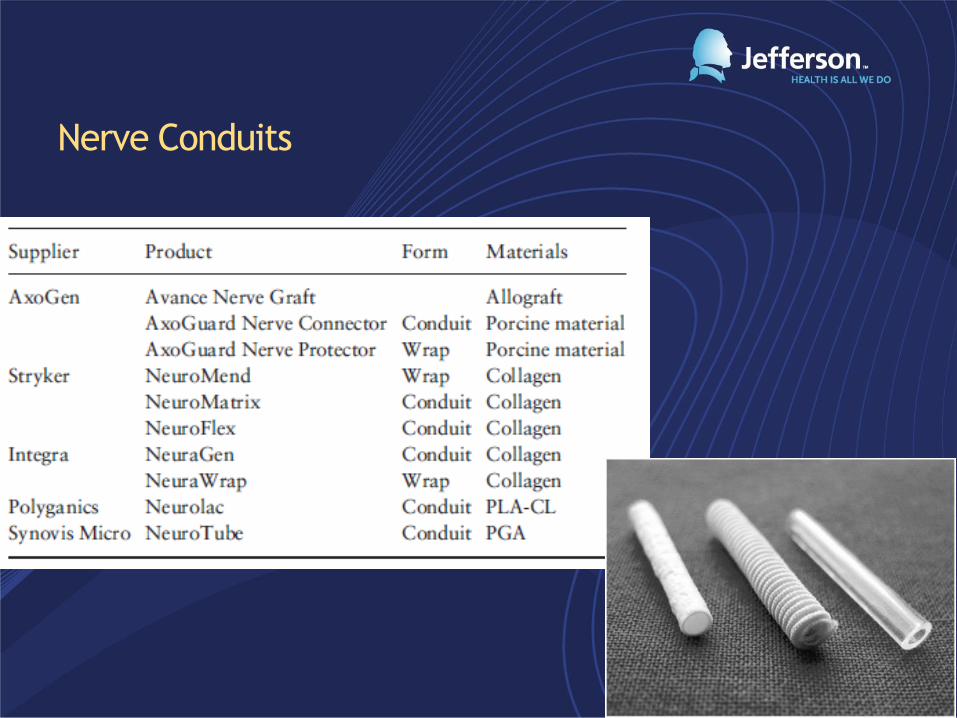
Nerve Conduits
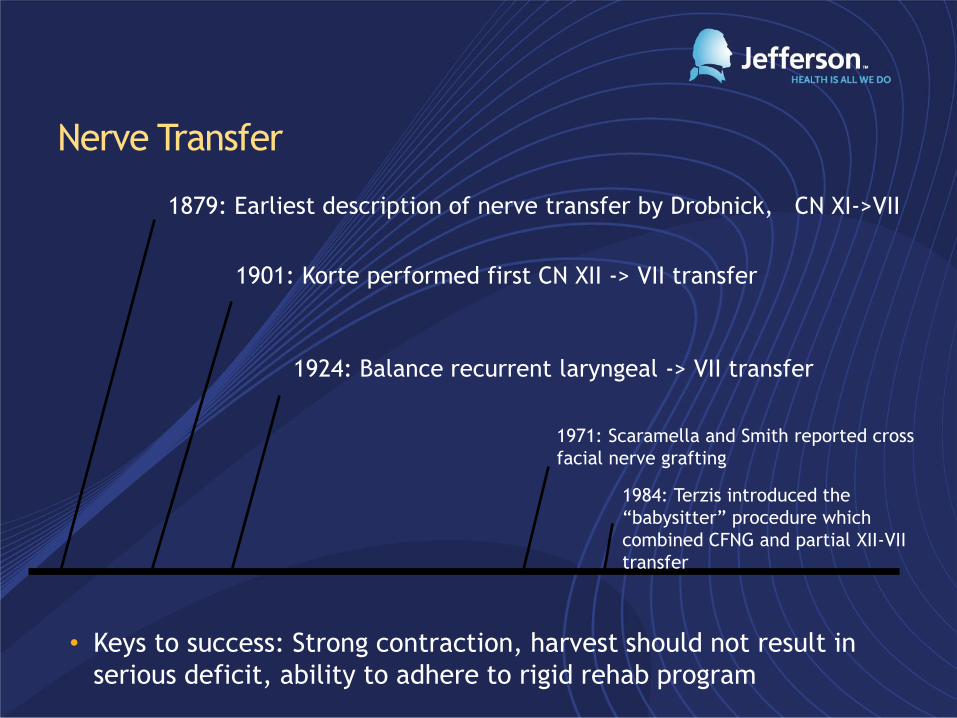
Nerve Transfer
• Keys to success: Strong contraction, harvest should not result in
serious deficit, ability to adhere to rigid rehab program
1879: Earliest description of nerve transfer by Drobnick, CN XI->VII
1901: Korte performed first CN XII -> VII transfer
1924: Balance recurrent laryngeal -> VII transfer
1971: Scaramella and Smith reported cross
facial nerve grafting
1984: Terzis introduced the
“babysitter” procedure which
combined CFNG and partial XII-VII
transfer
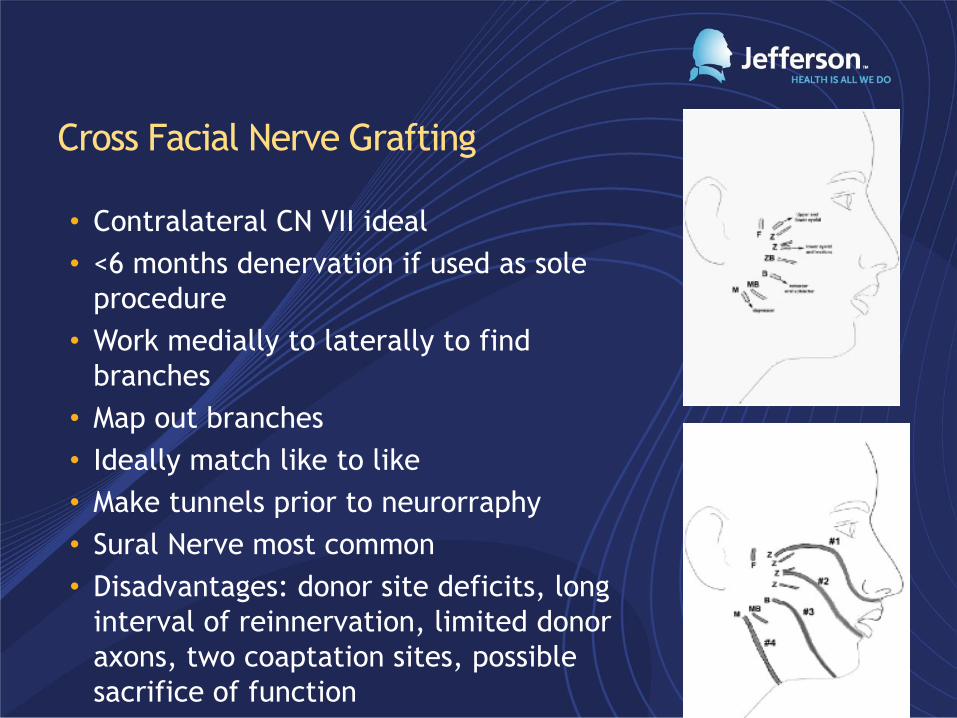
Cross Facial Nerve Grafting
• Contralateral CN VII ideal
• <6 months denervation if used as sole
procedure
• Work medially to laterally to find
branches
• Map out branches
• Ideally match like to like
• Make tunnels prior to neurorraphy
• Sural Nerve most common
• Disadvantages: donor site deficits, long
interval of reinnervation, limited donor
axons, two coaptation sites, possible
sacrifice of function

Scola


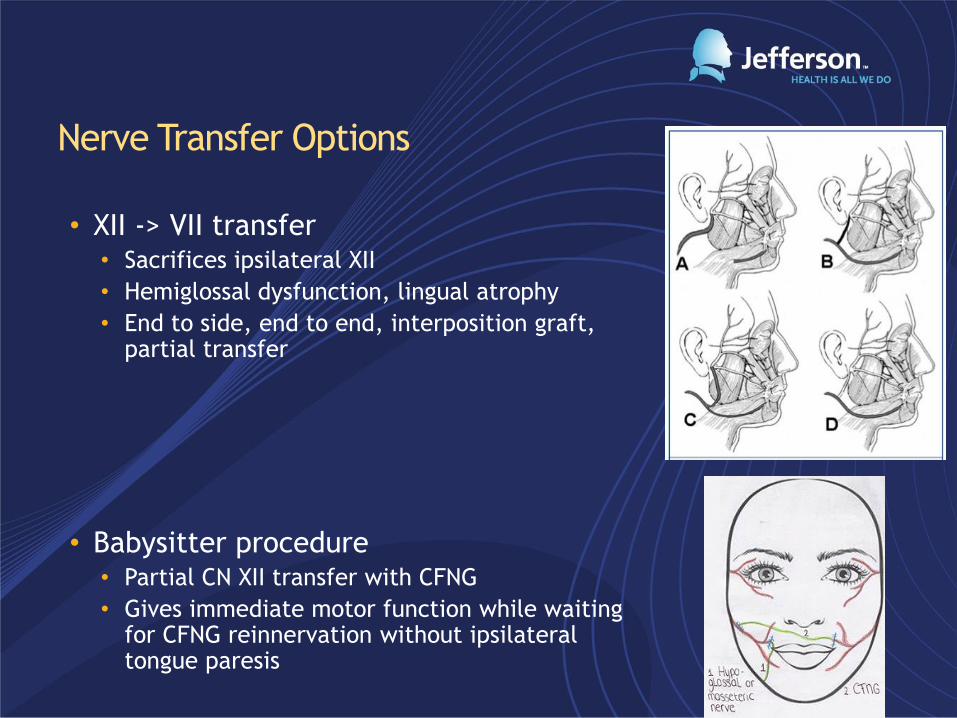
Nerve Transfer Options
• XII -> VII transfer • Sacrifices ipsilateral XII
• Hemiglossal dysfunction, lingual atrophy
• End to side, end to end, interposition graft, partial transfer
• Babysitter procedure • Partial CN XII transfer with CFNG
• Gives immediate motor function while waiting for CFNG reinnervation without ipsilateral tongue paresis

Nerve Transfer Options cont.
• CN V transfer
• CN XI transfer
• Last resort, Mobius syndrome
• Less natural result and severe
donor site morbidity
• Cervical Roots


Static Procedures
• Good for temporary paralysis, poor candidates for dynamic
procedures, atrophied muscles, failed dynamic procedure
• Facial Slings, Gold weight, Lower lid tightening
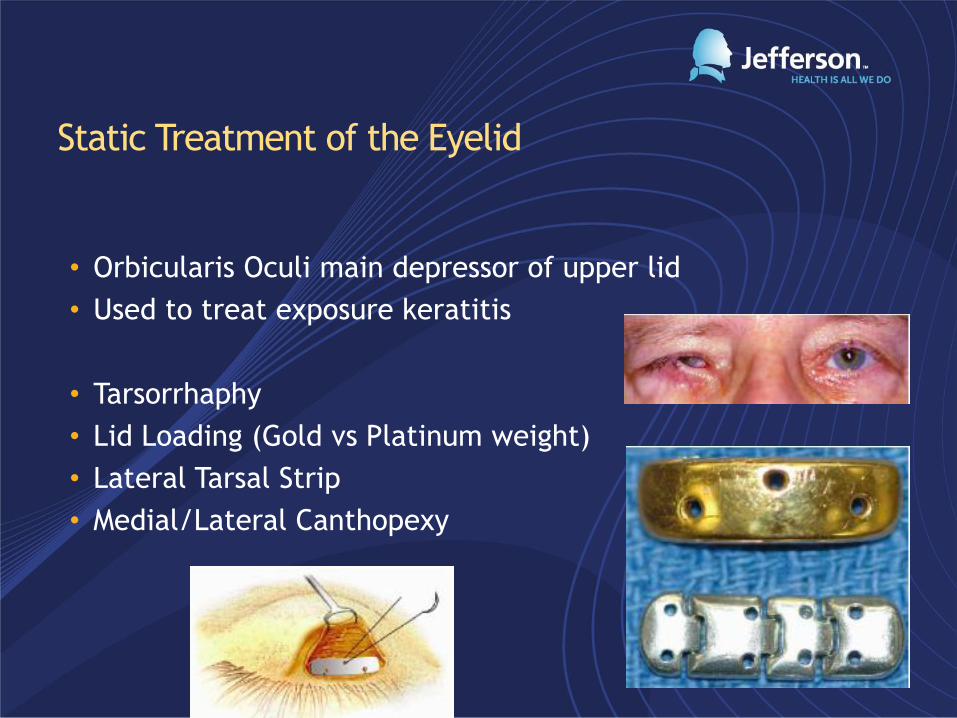
Static Treatment of the Eyelid
• Orbicularis Oculi main depressor of upper lid
• Used to treat exposure keratitis
• Tarsorrhaphy
• Lid Loading (Gold vs Platinum weight)
• Lateral Tarsal Strip
• Medial/Lateral Canthopexy
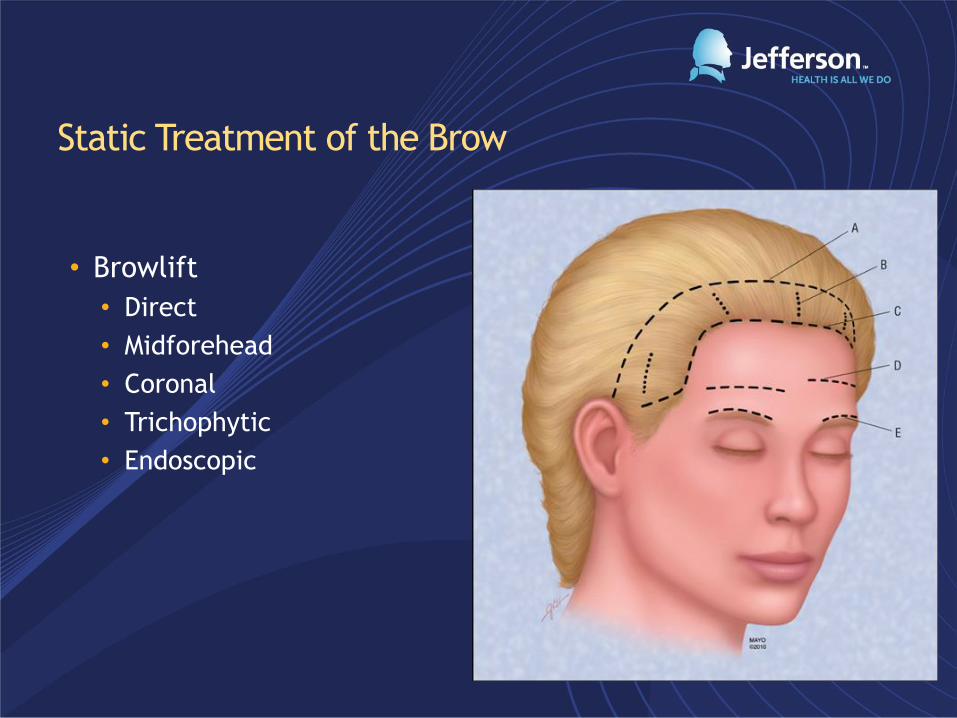
Static Treatment of the Brow
• Browlift
• Direct
• Midforehead
• Coronal
• Trichophytic
• Endoscopic
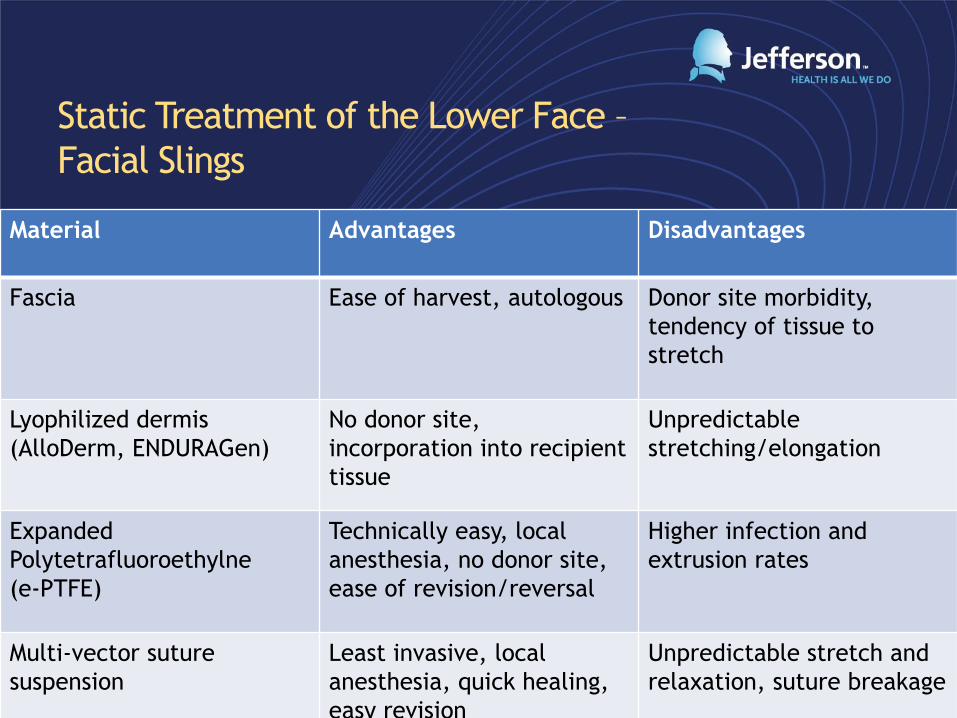
Static Treatment of the Lower Face –
Facial Slings
Material Advantages Disadvantages
Fascia Ease of harvest, autologous Donor site morbidity,
tendency of tissue to
stretch
Lyophilized dermis
(AlloDerm, ENDURAGen)
No donor site,
incorporation into recipient
tissue
Unpredictable
stretching/elongation
Expanded
Polytetrafluoroethylne
(e-PTFE)
Technically easy, local
anesthesia, no donor site,
ease of revision/reversal
Higher infection and
extrusion rates
Multi-vector suture
suspension
Least invasive, local
anesthesia, quick healing,
easy revision
Unpredictable stretch and
relaxation, suture breakage

Facial Slings
Dynamic Muscle Transfer
• Restore oral competence
• Most commonly used for long standing facial paralysis,
restoration of neural input not feasible
• Uses functional, innervated and vascular muscle
• 2 options
• Regional muscle transposition
• Free muscle transfer
• First description in 1911 by Eden, later
popularized in 1977 by Rubin
• Most commonly used muscles
temporalis, masseter and digastric
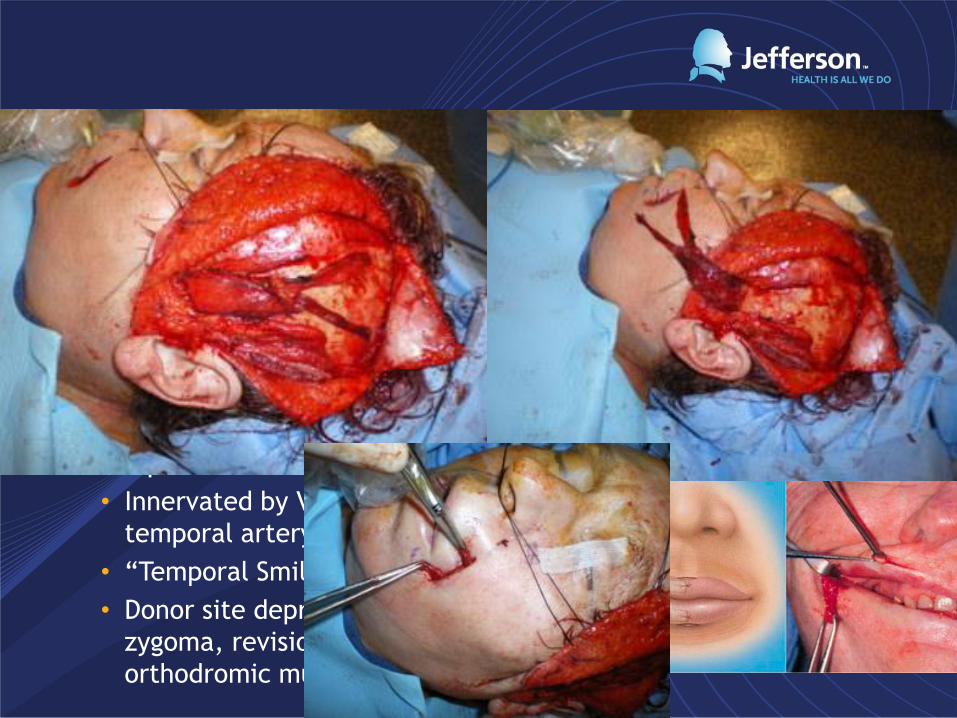
• Temporalis Muscle Transfer
• Innervated by V3, Blood supply deep
temporal artery
• “Temporal Smile”
• Donor site depression, bulge over
zygoma, revision surgery, lack of
orthodromic muscle contraction
Regional Muscle Transposition
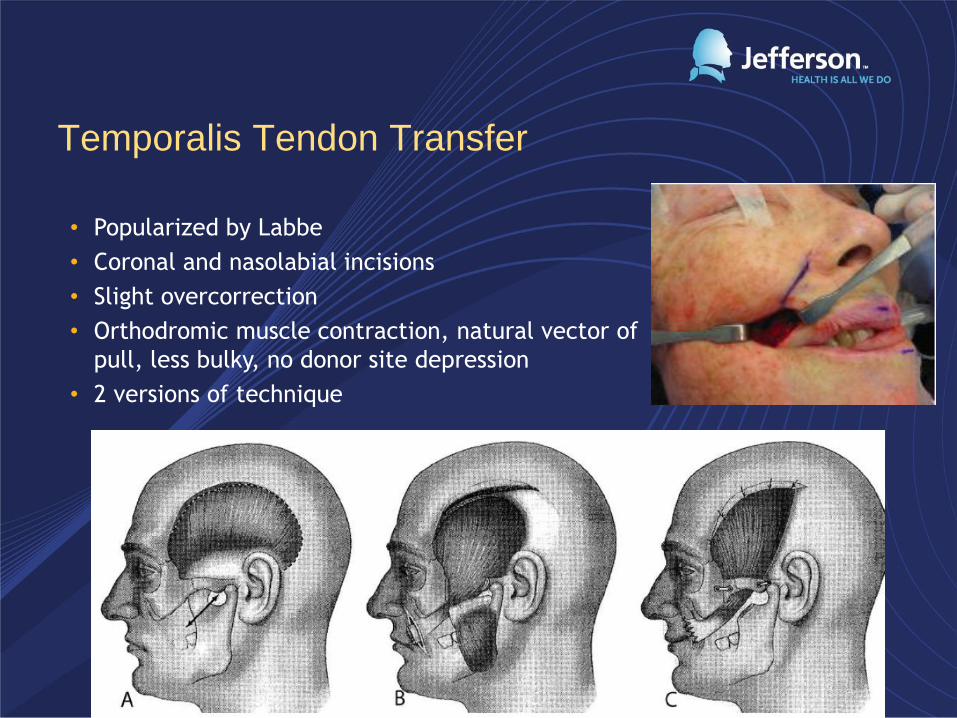
Temporalis Tendon Transfer
• Popularized by Labbe
• Coronal and nasolabial incisions
• Slight overcorrection
• Orthodromic muscle contraction, natural vector of
pull, less bulky, no donor site depression
• 2 versions of technique




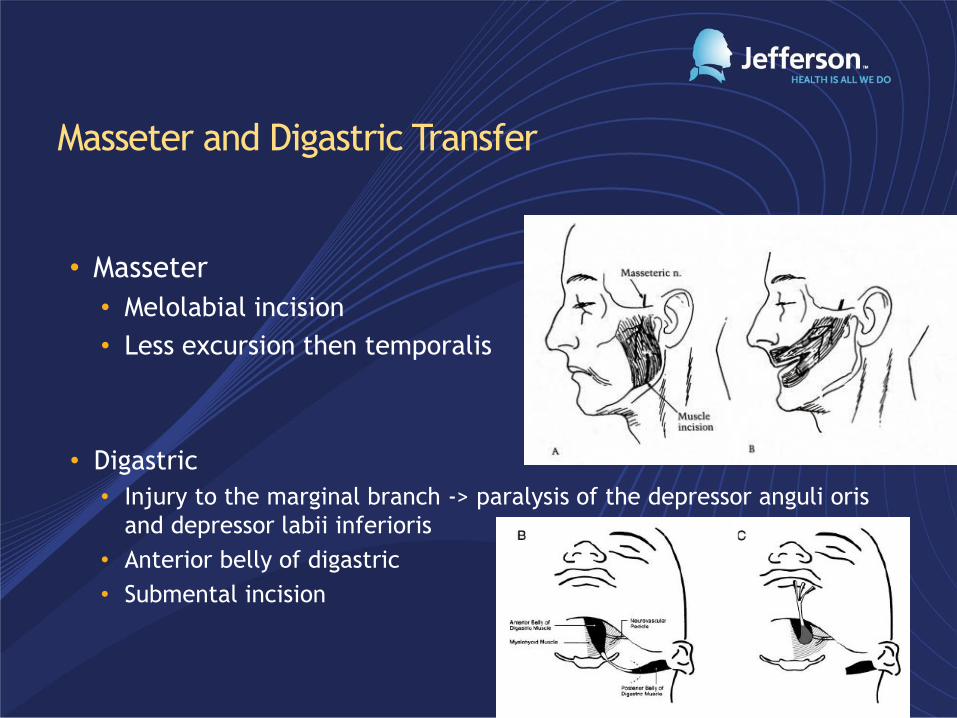
Masseter and Digastric Transfer
• Masseter
• Melolabial incision
• Less excursion then temporalis
• Digastric
• Injury to the marginal branch -> paralysis of the depressor anguli oris
and depressor labii inferioris
• Anterior belly of digastric
• Submental incision
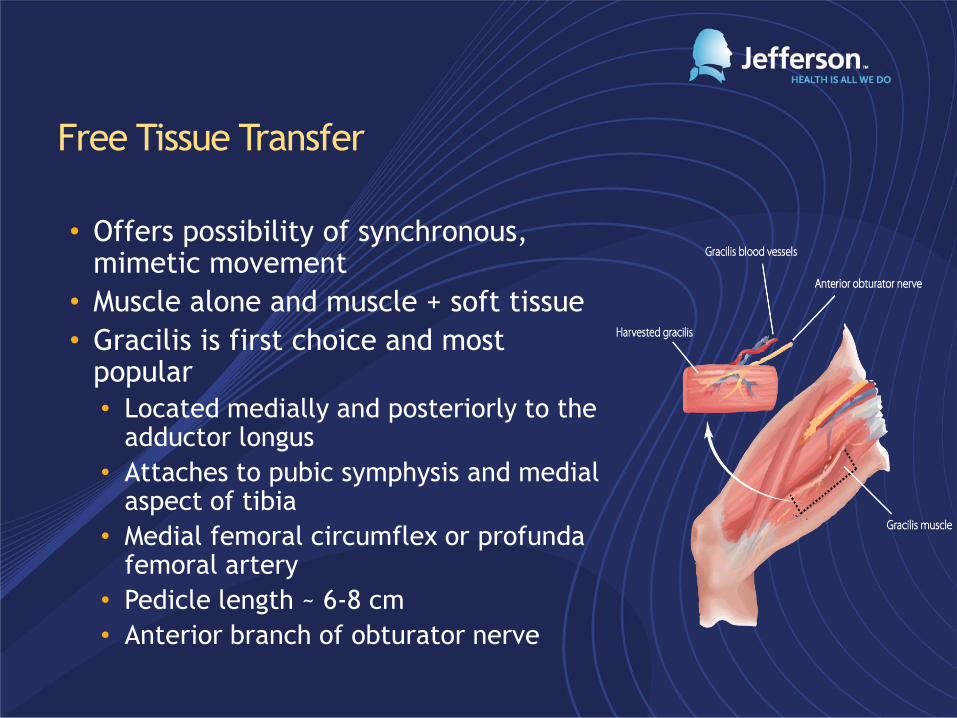
Free Tissue Transfer
• Offers possibility of synchronous, mimetic movement
• Muscle alone and muscle + soft tissue
• Gracilis is first choice and most popular
• Located medially and posteriorly to the adductor longus
• Attaches to pubic symphysis and medial aspect of tibia
• Medial femoral circumflex or profunda femoral artery
• Pedicle length ~ 6-8 cm
• Anterior branch of obturator nerve

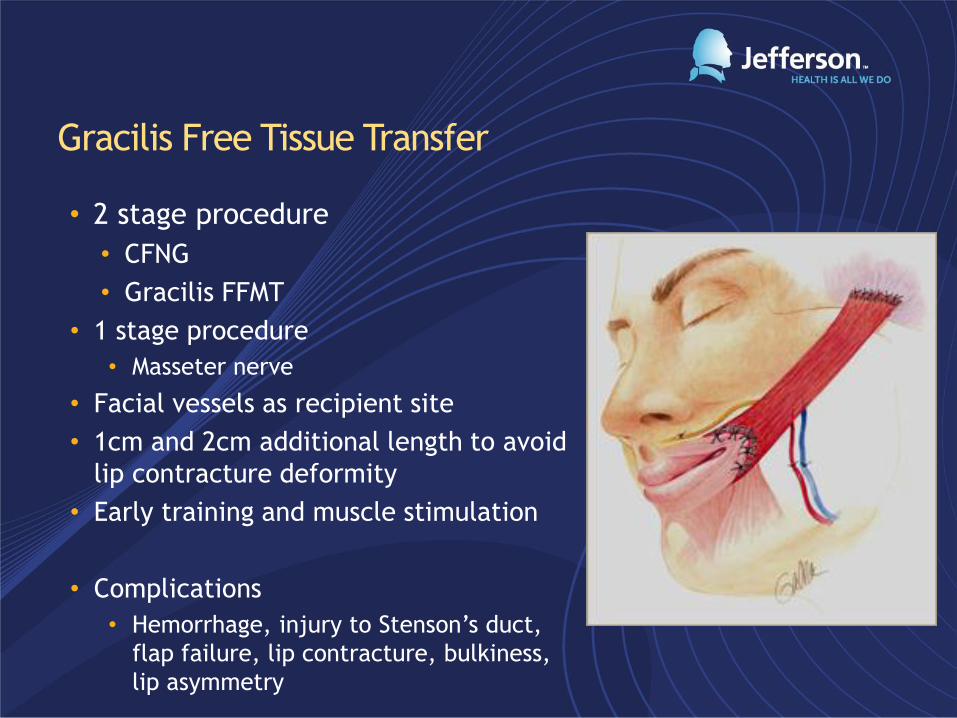
Gracilis Free Tissue Transfer
• 2 stage procedure
• CFNG
• Gracilis FFMT
• 1 stage procedure
• Masseter nerve
• Facial vessels as recipient site
• 1cm and 2cm additional length to avoid
lip contracture deformity
• Early training and muscle stimulation
• Complications
• Hemorrhage, injury to Stenson’s duct,
flap failure, lip contracture, bulkiness,
lip asymmetry
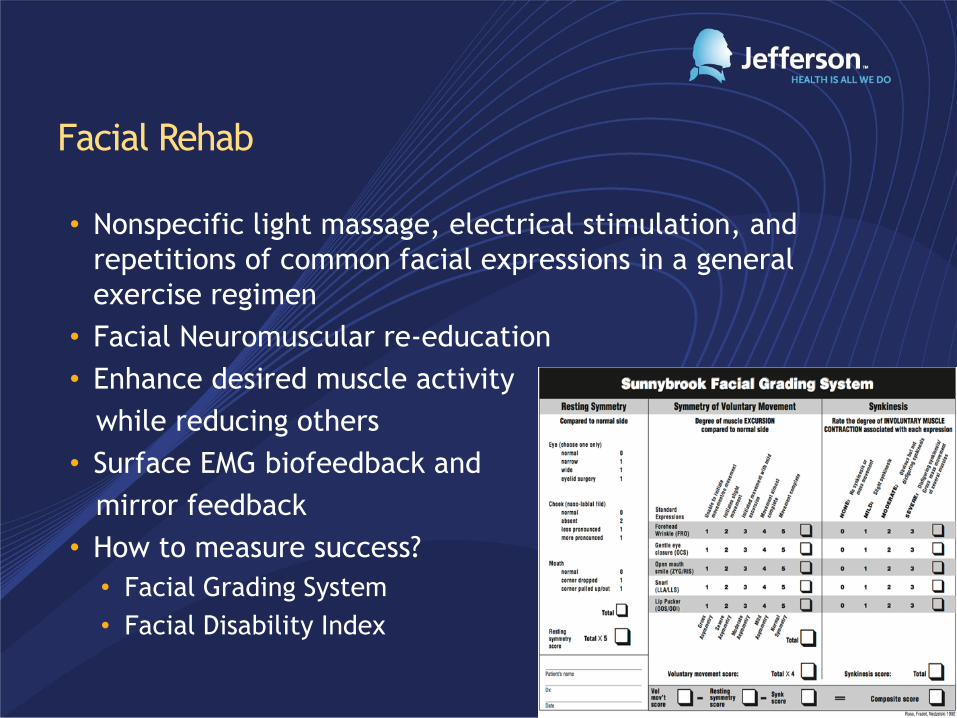
Facial Rehab
• Nonspecific light massage, electrical stimulation, and
repetitions of common facial expressions in a general
exercise regimen
• Facial Neuromuscular re-education
• Enhance desired muscle activity
while reducing others
• Surface EMG biofeedback and
mirror feedback
• How to measure success?
• Facial Grading System
• Facial Disability Index

Management of Synkinesis
• Abnormal involuntary movement
that occurs simultaneously during
voluntary muscle contraction
• Aberrant nerve regeneration
• Sunderland Class III and above
• ~20% patients
• Treatments include facial
neuromuscular retraining, Botox
injection, selective neurolysis or
myomectomy

Future Direction and Research
• Platelet rich plasma
• Neural tube additives
• Facial Analysis
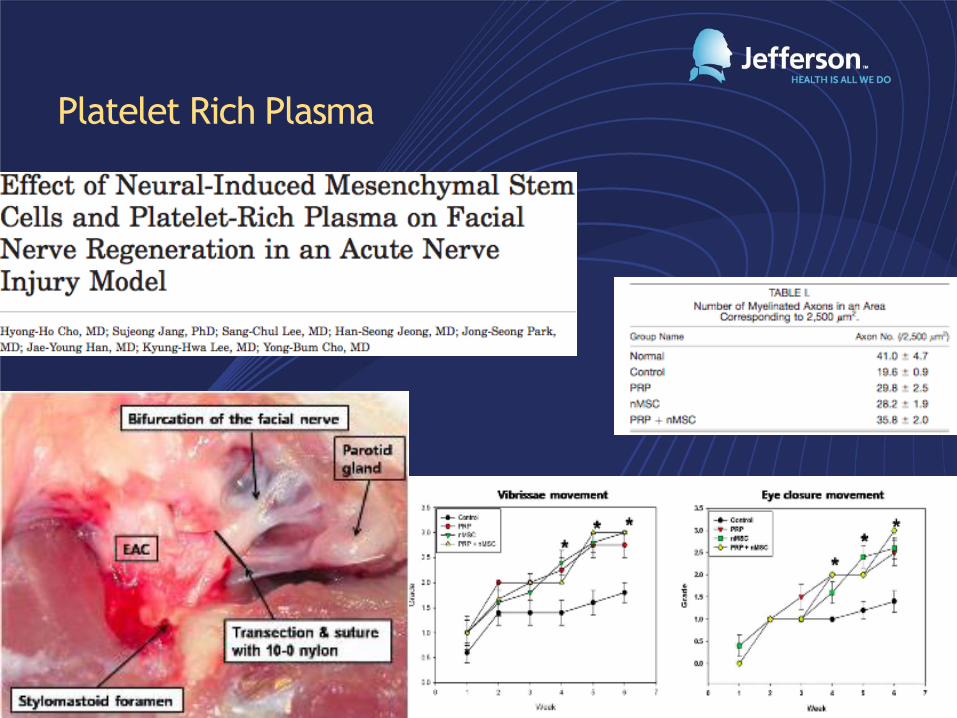
Platelet Rich Plasma
Neural Tube Additives
Facial Analysis
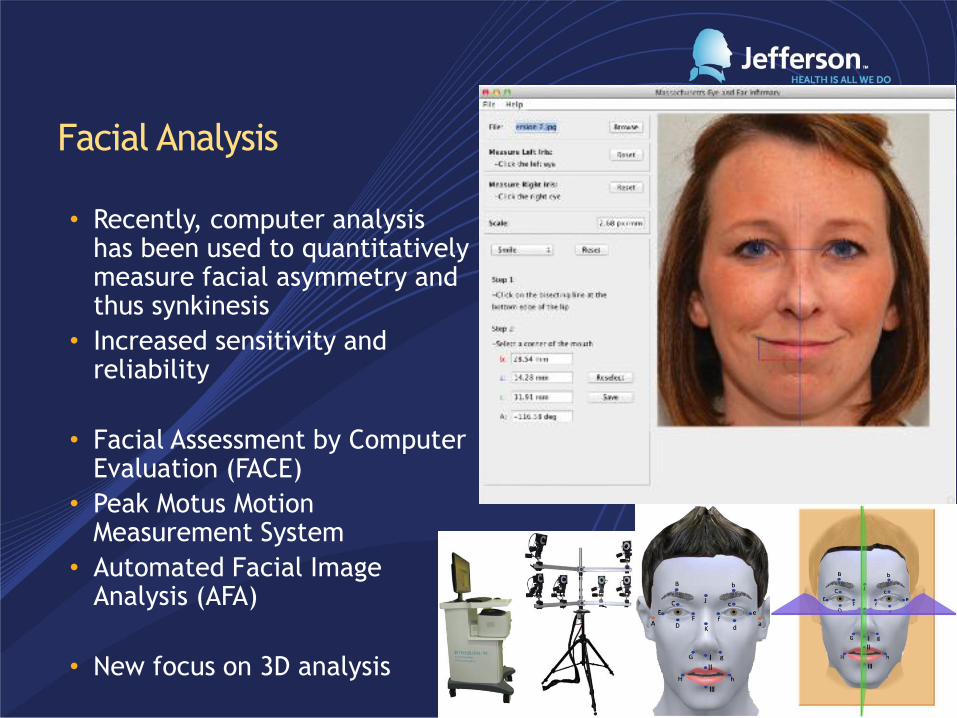
• Recently, computer analysis has been used to quantitatively measure facial asymmetry and thus synkinesis
• Increased sensitivity and reliability
• Facial Assessment by Computer Evaluation (FACE)
• Peak Motus Motion Measurement System
• Automated Facial Image Analysis (AFA)
• New focus on 3D analysis
Conclusion
• Many options to treat facial paralysis from neurorraphy to
free muscle transfer
• Onset, timing and duration of paralysis is important
• Must match goals of the patient with goals of surgeon
• New and dynamic field of facial plastic surgery with
continual advancements which will allow for objective data
and better results

Thank You
• Dr. Heffelfinger
• Dr. Krein

References • Prendergast, PM. “Anatomy of the Face and Neck.” Cosmetic Surgery. Editors MA Shiffman, A Di Giuseppe. Berlin: Springer-Verlag, 2012. 29-45.
• Kim J. The Effective Treatment for Incomplete Recovery after Facial Nerve Paralysis. Korean J Otorhinolaryngol-Head Neck Surg. 2013 Jul;56(7):397-405
• Arslantunali D, Dursun T, Yucel D, Hasirci N, Hasirci V. Peripheral nerve conduits: technology update. Med Devices (Auckl). 2014 Dec 1;7:405-24
• Tian L, Prabhakaran MP, Ramakrishna S. Strategies for regeneration of components of nervous system: scaffolds, cells and biomolecules. Regenerative Biomaterials. 2015; 2(1): 31-45.
• Gerth DJ, Tashiro J, Thaller SR. Clincal outcomes for conduits and scaffolds in peripheral nerve repair. World J Clin Cases. 2015 Feb 16; 3(2): 141–147.
• Isaacs J, Browne T. Overcoming short gaps in peripheral nerve repair: conduits and human acellular nerve allograft. Hand. 2015; 9: 131-137.
• Cho HH, Jang S, Lee SC, Jeong HS, Park JS, Han JY, Lee KH, Cho YB. Effect of Neural-Induced Mesenchymal Stem Cells and Platelet-Rich Plasma on Facial Nerve Regeneration in an Acute
Nerve Injury Model. Laryngoscope May 2010; 120: 907-913.
• Hadlock TA, Urban LS. Toward a universal automated facial measurement tool in facial reanimation. Arch Facial Plast Surg. 2012 Jul-Aug;14(4):277-82
• Zhao L, Qu W, Wu Y, Ma H, Jiang H. Dorsal root ganglion-derived Schwann cells combined with poly(lactic-co-glycolic acid)/chitosan conduits for the repair of sciatic nerve defects in
rats. Neural Regen Res. 2014 Nov 15; 9(22): 1961–1967.
• Georgiou M, Golding JP, Loughlin AJ, Kingham PJ, Phillips JB. Engineered neural tissue with aligned, differentiated adipose-derived stem cells promotes peripheral nerve regeneration
across a critical sized defect in rat sciatic nerve. Biomaterials. 2015 Jan;37:242-51
• Ma F, Xiao Z, Meng D, Hou X, Zhu J, Dai J, Xu R. Use of natural neural scaffolds consisting of engineered vascular endothelial growth factor immobilized on ordered collagen fibers filled
in a collagen tube for peripheral nerve regeneration in rats. Int J Mol Sci. 2014 Oct 15;15(10):18593-609
• Hernández-Cortés P, Toledo-Romero MA, Delgado M, Sánchez-González CE, Martin F, Galindo-Moreno P, O'Valle F. Peripheral nerve reconstruction with epsilon-
caprolactone conduits seeded with vasoactive intestinal peptide gene-transfected mesenchymal stem cells in a rat model. J Neural Eng. 2014 Aug;11(4):046024
• Ni HC, Tseng TC, Chen JR, Hsu SH, Chiu IM. Fabrication of bioactive conduits containing the fibroblast growth factor 1 and neural stem cells for peripheral nerve regeneration across a
15 mm critical gap. Biofabrication. 2013 Sep;5(3):035010
• Berrocal YA, Almeida VW, Gupta R, Levi AD. Transplantation of Schwann cells in a collagen tube for the repair of large, segmental peripheral nerve defects in rats. J Neurosurg. 2013
Sep;119(3):720-32
• Sherris DA. Refinement in reanimation of the lower face. Arch Facial Plast Surg. 2004 Jan-Feb;6(1):49-53
• Tan ST. Anterior belly of digastric muscle transfer: a useful technique in head and neck surgery. Head Neck. 2002 Oct;24(10):947-54.
• Alex JC, Nguyen DB. Multivectored Suture SuspensionA Minimally Invasive Technique for Reanimation of the Paralyzed Face. Arch Facial Plast Surg May-Jun 2004; 6: 197-201.
• Husseman J, Mehta RP. Management of Synkinesis. Facial Plast Surg. 2008 May;24(2):242-9
• Chuang DC. Free Tissue Transfer for the Treatment of Facial Paralysis. . Facial Plast Surg. 2008 May;24(2):194-203.
• VanSwearingen J. Facial Rehabilitation: A Neuromuscular Reeducation, Patient-Centered Approach. . Facial Plast Surg. 2008 May;24(2):250-259.
• Humphrey CD, Kriet JD. Nerve Repair and Cable Grafting for Facial Paralysis. Facial Plast Surg. 2008 May;24(2):170-176.
• Terzis JK, Konofaos P. Nerve Transfers in Facial Palsy. Facial Plast Surg. 2008 May;24(2):177-193.
• Hadlock T. Facial Paralysis: Research and Future Directions. Facial Plast Surg. 2008 May;24(2):260-267.
• Melvin TN, Limb CJ. Overview of Facial Paralysis: Current Concepts. Facial Plast Surg. 2008 May;24(2):155-163.
• Liu YM, Sherris DA. Static Procedures for the Management of the Midface and Lower Face. Facial Plast Surg. 2008 May;24(2):211-215.
• Chu EA, Byrne PJ. Treatment Considerations in Facial Paralysis. . Facial Plast Surg. 2008 May;24(2):164-169.
• Boahene KDO. Dynamic Muscle Transfer in Facial Reanimation. . Facial Plast Surg. 2008 May;24(2):204-210.
• Bhama PK, Hadlock TA. Contemporary Facial Reanimation. Facial Plast Surg 2014;30:145–151
• Bergeron CM, Moe KS. The Evaluation and Treatment of Upper Eyelid Paralysis. . Facial Plast Surg 2014;30:220-230.
Recommended