Feb 2010
Common Healthcare waste Appropriate Management Plant (CHAMP)
An economically appropriate approach for Bio Medical Waste Management in rural and smaller cities of India.
Feb 2010
PROJECT DETAILS Name of the Project : Healthcare Establishment
Waste Management and Education Programme
(HEWMEP)
Name of the Facility : Common Healthcare waste Appropriate Management Plant
(CHAMP) Project Location : Gulbarga city, Karnataka,
INDIA
Implementing Agency : Centre for Environment Education (CEE)
Feb 2010
The Implementing Agency
Centre for Environment Education (CEE) is a national Institute engaged in developing programmes and materials to increase awareness about the environment.
CEE was established in 1984 as a Centre of Excellence in Environmental Education, supported by the Ministry of Environment & Forests, Government of India. It is affiliated to the Nehru Foundation for Development.
CEE's primary objective is to improve public awareness and understanding of environmental issues with a view to promote the conservation and wise use of nature and natural resources.
Feb 2010
Objectives of HEWMEP Gulbarga
To set up a completely operational common facility for Bio-medical Waste Collection, Transportation, Treatment and Disposal for Healthcare Establishments (HCEs) in Gulbarga
To train hospital staff regarding methodology for proper Bio-Medical Waste Management in their HCEs
To create awareness among the general public regarding Bio-Medical Waste and its hazards
To prepare Educational materials regarding Bio-Medical Waste Management
Feb 2010
Aims of HEWMEP, Gulbarga project
Waste minimization- Segregation- Collection- Storage- Transportation- Treatment-
& Disposal-of biomedical waste in an eco-friendly and
technologically sound way.
Feb 2010
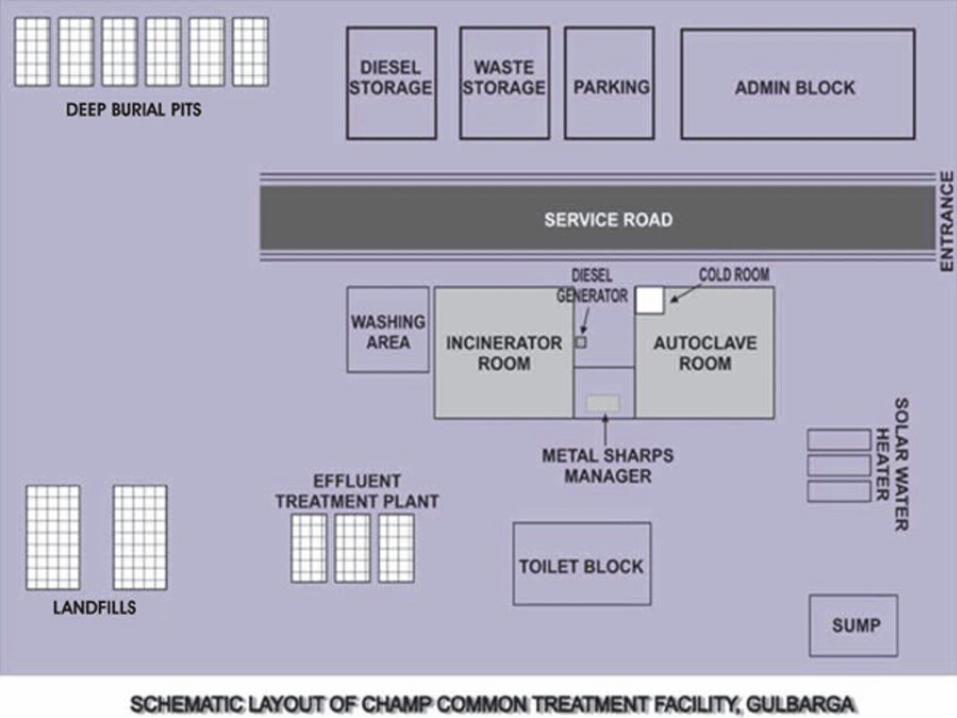
Salient features of CHAMP CTF
Comprehensive facility - involves collection, transportation, storage, treatment and disposal of the biomedical waste of Gulbarga city.
The facility has-
Specially fabricated transport vehicles for biomedical waste. The vehicles are retrofitted with the ionizer and filter system to check escape of micro organisms to the surroundings.
On site cold storage facility for the waste. Treatment facilities like Incinerator, Modified Autoclave, Metal
Sharps Manager and ETP for treatment of the waste. Landfill and deep burial for disposal of the waste. Eco friendly technique - solar water heater supplementing the
system.
Feb 2010
Implementation of HEWMEP, Gulbarga project - Historical1) Quantification Survey – to ascertain quantity of biomedical waste (bmw)
generated in Gulbarga which in turn, is required to ascertain the technologies to be employed.
2) Formation of Committees – District level and State level committees to facilitate implementation of project.
3) Land Acquisition and EIA – 5 acres of land been leased from District Administration for setting up the Common Facility under the project. EIA was carried out to assess the suitability of the site for the purpose.
4) Motivation and Orientation programmes – to encourage the participation of the stakeholders.
5) Signing of MoU with the individual HCEs to ensure their participation
6) Development of the training material for training and orientation of the stakeholders.
Contd…

Feb 2010
7) Setting up of the CHAMP common treatment facility-
Construction work at the CHAMP site Finalization of the technologies and the capacities of the
equipments / vehicles to be procured. Tendering and contracting Installation of the equipments and commissioning, trial run
of the equipments / vehicles. Routing plan for the collection of the waste. Trial run of the complete plant. Inauguration and the commissioning and operation of the
plant
8) Operation and Monitoring of the plant (ongoing till 2011)

Feb 2010
CHAMP CTF at Gulbarga
Feb 2010
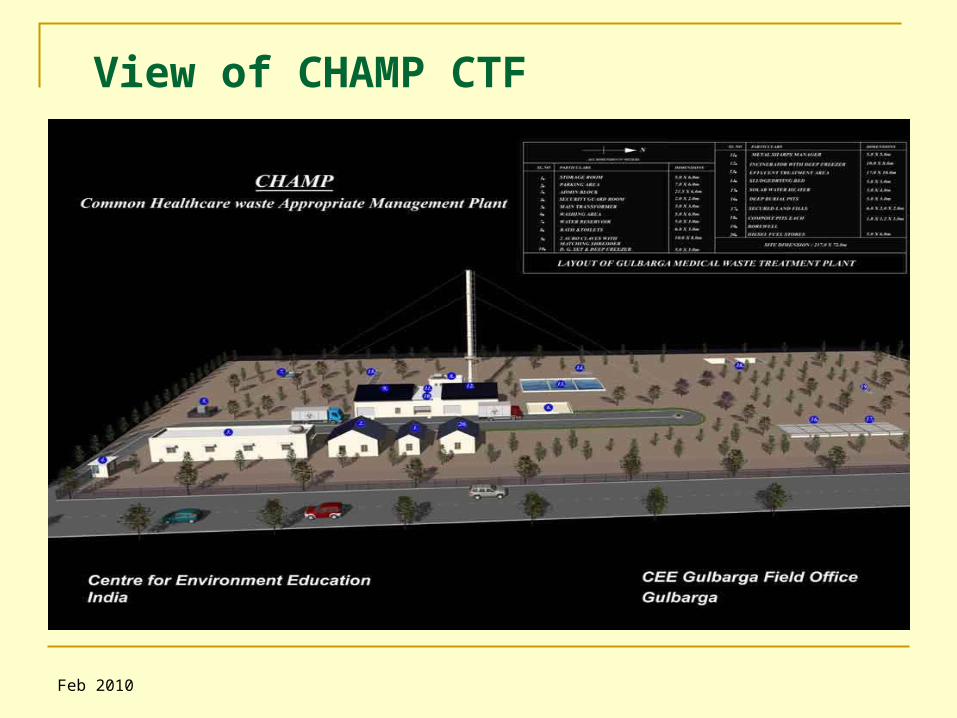
View of CHAMP CTF
Feb 2010
Feb 2010
Treatment Options at CHAMP CTF
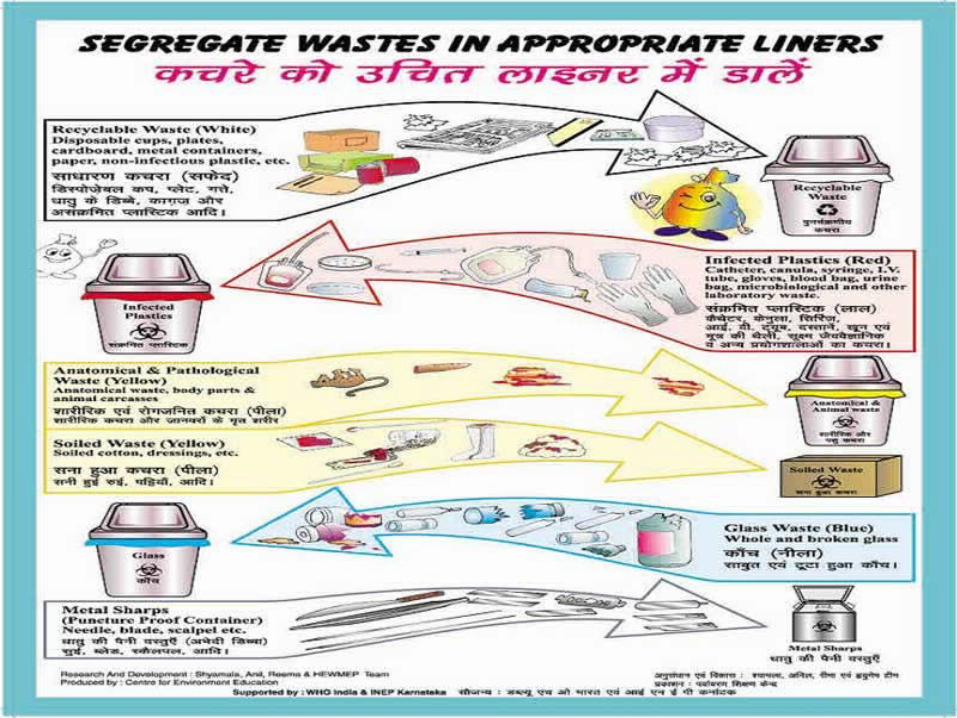
Treatment at the CTF site, Gulbarga is being done as per the Schedule 1 of Rule 5 of Biomedical Waste (Management and Handling) Rules, 1998.
To ensure the efficacy of the treatment, the project has been aiming at achieving 100 % segregation of waste at the source level.
The various treatment technologies engaged at the CHAMP CTF are…..
Feb 2010
Incinerator (1 in no.) of capacity 50 kgs /hr for treatment of waste under categories* 1,2
Modified Autoclaves (2 in no) each of capacity 100kg/hr for treatment of waste under categories* 3,4,6,7
Metal Sharps Manager (1 in no) of capacity 10 kg/hr for treatment for metal sharps
Land filling for rejects, incinerator ash and hazardous chemicals categories 5 and 9 & solid part of category 10
Deep Burial as a stand-by option in case of breakdown or maintenance of incinerator at the site
ETP for the liquid waste generated at the site of category 10
* The various categories of the biomedical waste as classified in the BMWM Rules 1998 explained in the subsequent slides
Feb 2010
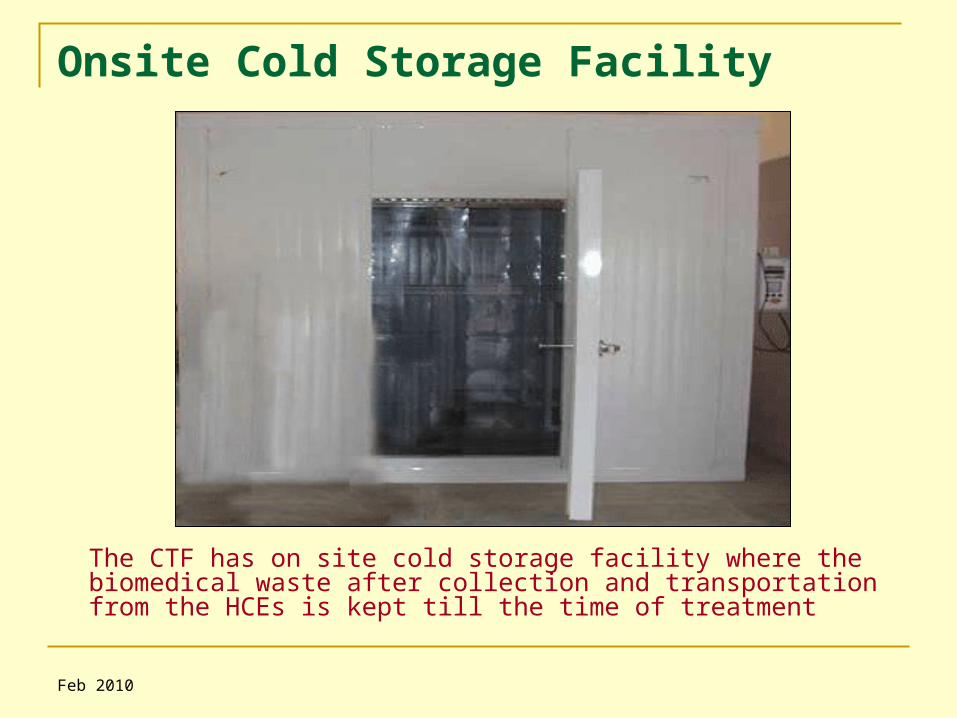
Onsite Cold Storage Facility
The CTF has on site cold storage facility where the biomedical waste after collection and transportation from the HCEs is kept till the time of treatment
Feb 2010
Incineration at the CHAMP CTF The burning of wastes at high temperatures, under controlled
conditions, is called incineration and this is carried out in a double-chambered device known as an incinerator
Waste is burnt in the primary chamber at 800-8500C and volatile gases emitted are again burnt in the secondary chamber at 1050 -11000C (residence time - at least 2 sec).
The incinerator at the CHAMP CTF is retrofitted with the High Pressure Venturi Scrubber, as air pollution control device. The equipment also has the facility of computer recording for CO, CO2 and O2 in gaseous emission of critical parameters.
The cycle time for the entire operation is about 1 hour. The volume is significantly reduced with assured sterilization and destruction.
The equipment follows all the latest specifications and guidelines specified by the CPCB in Sept 2003 for the Common Facility Incinerators
The equipment is used for the treatment of waste falling under Category 1,2 of BMWM Rules which consists of ……
Feb 2010
Incinerable Waste
Category 1– Human Anatomical Waste
(human tissues, organs, body parts)
Category 2– Animal Waste (animal tissues, organs, body parts, carcasses,
bleeding parts, fluid, blood and experimental animals used in research, waste generated by veterinary hospitals, colleges, discharge from hospitals, animal houses)
The category 1 and 2 waste are stored in yellow liners which have to be non chlorinated so as to minimize the chances of emission of dioxins and furans, major pollutants having carcinogenic properties

Feb 2010
50 Kg / hr capacity Incinerator at the CHAMP site
Feb 2010
Deep Burial at the CTF Site
Deep Burial is the stand-by option in case of the failure of incinerator operation for Category 1 and 2 Infectious waste
Infectious Waste belonging to Category 6 (soiled cotton, dressings etc.) is also disposed of in deep burial after sterilization in the modified autoclave
Feb 2010
Autoclaving at the CHAMP CTF site Steam is applied inside a double-walled jacket under pressure. Waste is fed into the chamber where it gets hydrated, agitated &
sterilised The waste is internally fragmented to attain a high level of sterilization. Steam sterilization followed by dehydration, results in dry waste, greatly
reduced in weight and volume The sterilized waste is then shredded in the shredding assembly fitted
below the autoclave system. Along with the shredding, hot water washing also takes place in the
shredder, making the sterilized and shredded waste suitable for recycling
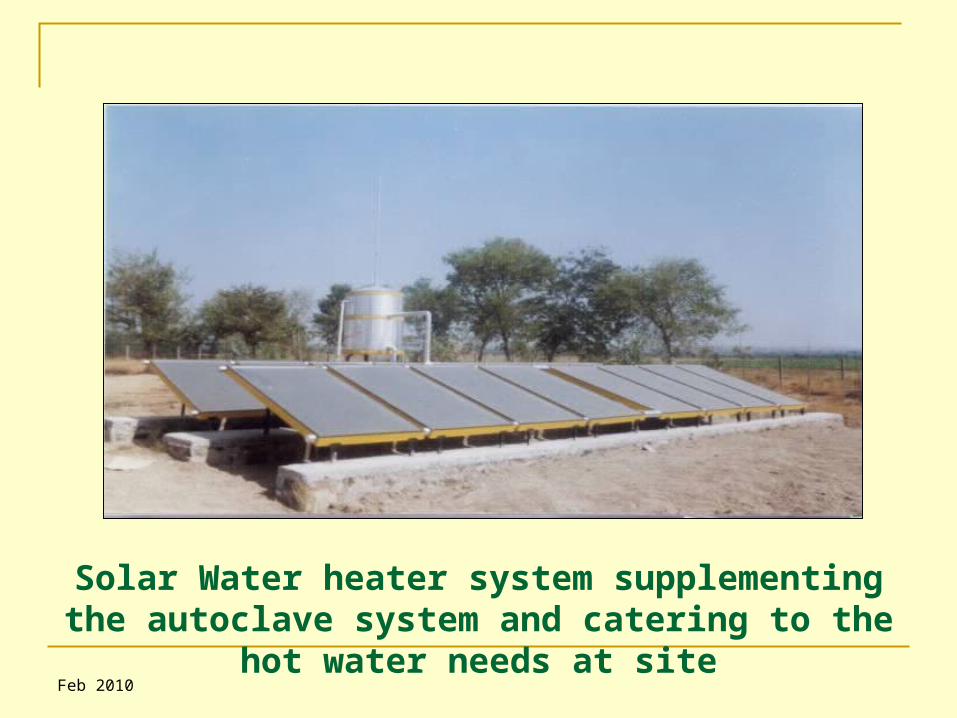
The salient feature of the modified autoclave system at CHAMP CTF site is that the solar water heater which supplies hot water for steam, which ensures energy efficiency and reduces the cost of operation by reducing diesel / electrical consumption for producing steam
Autoclaving is used to treat waste falling under the category 3, 6 and 7.
Feb 2010
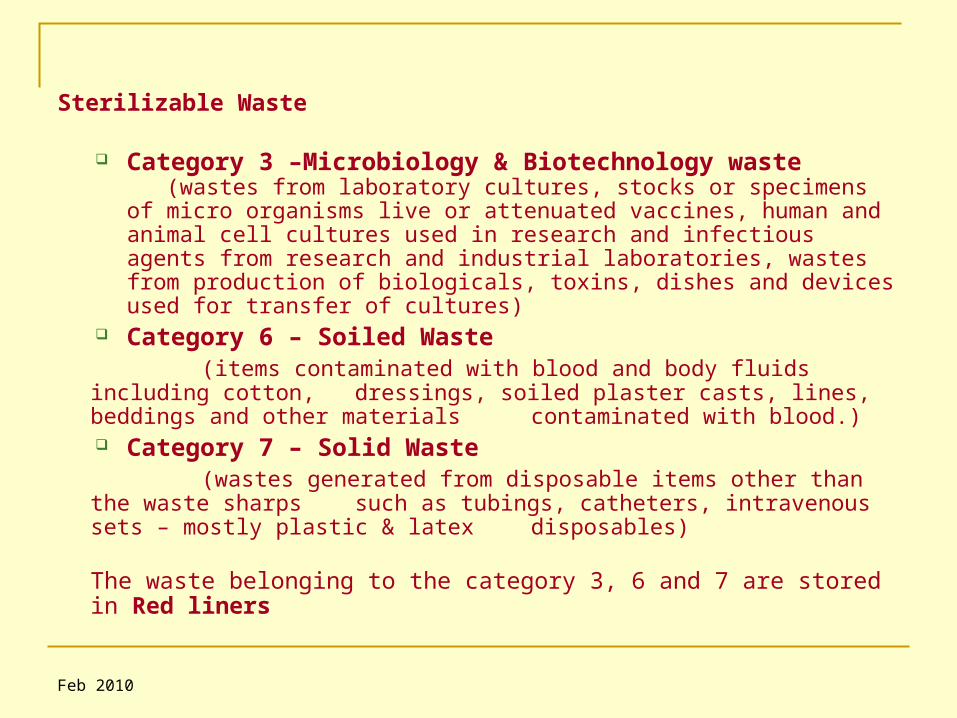
Sterilizable Waste
Category 3 –Microbiology & Biotechnology waste (wastes from laboratory cultures, stocks or specimens of micro organisms live or attenuated vaccines, human and animal cell cultures used in research and infectious agents from research and industrial laboratories, wastes from production of biologicals, toxins, dishes and devices used for transfer of cultures)
Category 6 – Soiled Waste (items contaminated with blood and body fluids including cotton, dressings, soiled plaster casts, lines, beddings and other materials
contaminated with blood.) Category 7 – Solid Waste
(wastes generated from disposable items other than the waste sharps such as tubings, catheters, intravenous sets – mostly plastic & latex disposables)
The waste belonging to the category 3, 6 and 7 are stored in Red liners

Feb 2010
100 kg / hr each – Modified Autoclaves
Feb 2010
Solar Water heater system supplementing the autoclave system and catering to the hot water needs at site
Feb 2010
Treatment of waste sharps The waste metals sharps are treated in the Metal Sharps Manager
at the site. All the HCEs are provided with puncture proof metal
boxes which have keyhole arrangements that separate the needles from syringes. A protected opening for dropping the blades, canula needles and scalpels is also present in the box
The metal boxes are brought from the HCEs to the site; the metal sharps from the metal boxes are then transferred to the metal sharps manager, present at the site
The metal sharps manager has a powerful shredding mechanism which mutilates the needles into small pieces. The system is also retrofitted with hot air oven that sterilizes the mutilated needles at 164oC
Waste belonging to category 4 (needles, syringes, disposable scalpels, blades, sutures etc.) are treated in the equipment

Feb 2010
Hopper for sharp feeding
Oven assembly for hot air sterilization
Shredding Mechanism
Shredded and sterilized sharps
Metal Sharps Manager at CHAMP
Metal Sharps Collection Box at HCES
Key hole arrangement
Opening for bigger sharps
Feb 2010
Discarded Medicines, Cytotoxic Drugs and Incineration Ash
Category 5 comprises of wastes comprising of outdated, contaminated and discarded medicines
Category 9 consists of incineration ash
Category 10 consists of solid Chemical wastes
The above mentioned waste is stored in Black Plastic Bags and kept for secured landfilling as per the BMWM Rules, 1998
Feb 2010
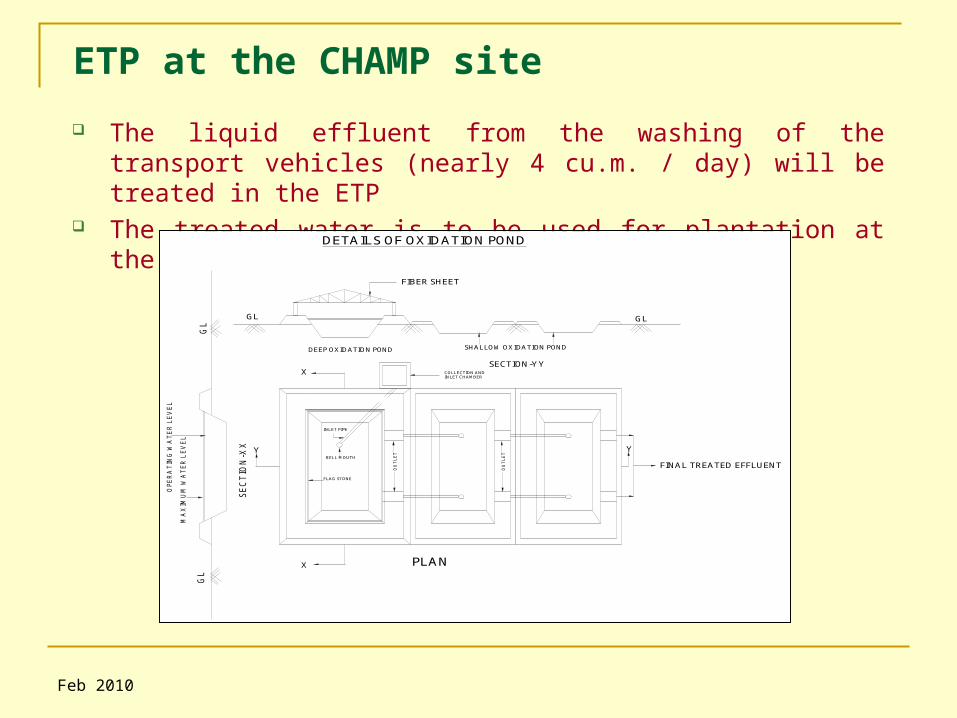
ETP at the CHAMP site
The liquid effluent from the washing of the transport vehicles (nearly 4 cu.m. / day) will be treated in the ETP
The treated water is to be used for plantation at the site.
BELL MOUTH
FLAG STONE
COLLECTION ANDINLET CHAMBER
INLET PIPE
OU
TL
ET
GL
GL
SE
CT
ION
-XX
MA
XIM
UM
WA
TE
R L
EV
EL
OP
ER
AT
ING
WA
TE
R L
EV
EL
GL GL
SECTION-YY
FIBER SHEET
PLAN
DEEP OXIDATION POND SHALLOW OXIDATION POND
DETAILS OF OXIDATION POND
FINAL TREATED EFFLUENT
Y Y
X
X
OU
TL
ET

Feb 2010
Vehicles for biomedical waste collection and transport
Specially fabricated transport vehicles for biomedical waste. The vehicles are retrofitted with the ionizer – filter system to check escape of micro organisms to the surroundings
Feb 2010
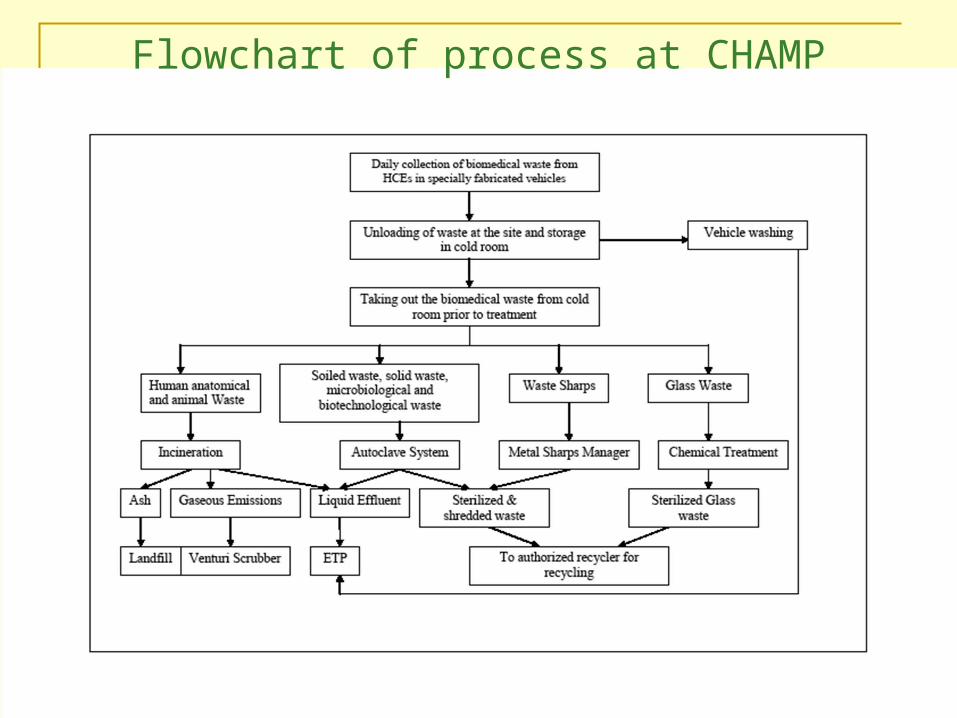
Flowchart of process at CHAMP
Feb 2010
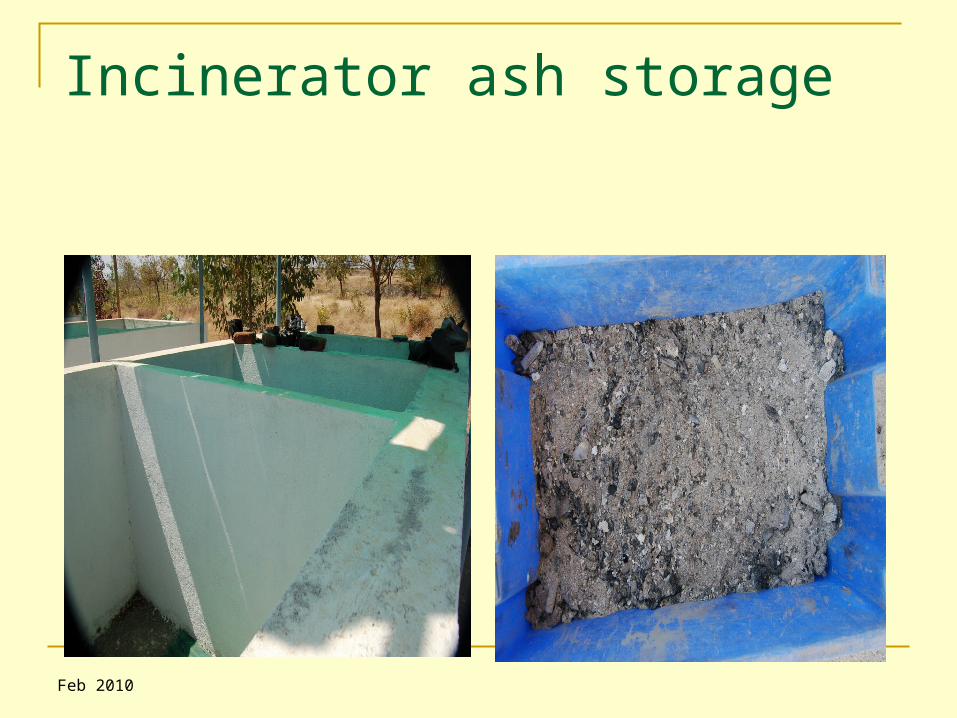
Incinerator ash storage

Feb 2010
Treated plastic waste before sale

Feb 2010
Treated Glass & Metal Sharps

Feb 2010
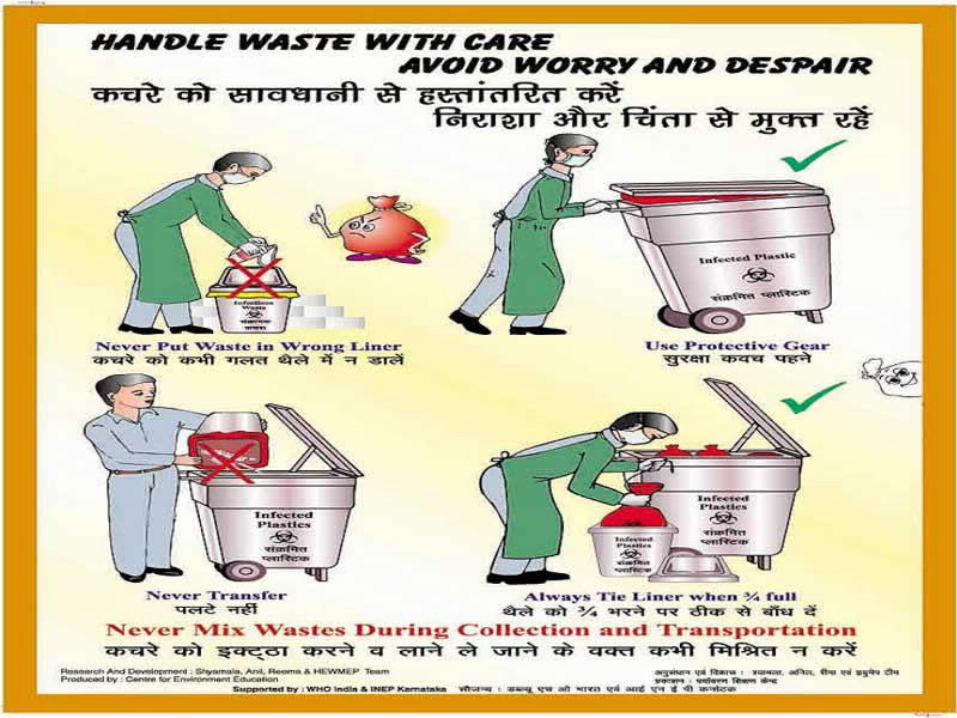
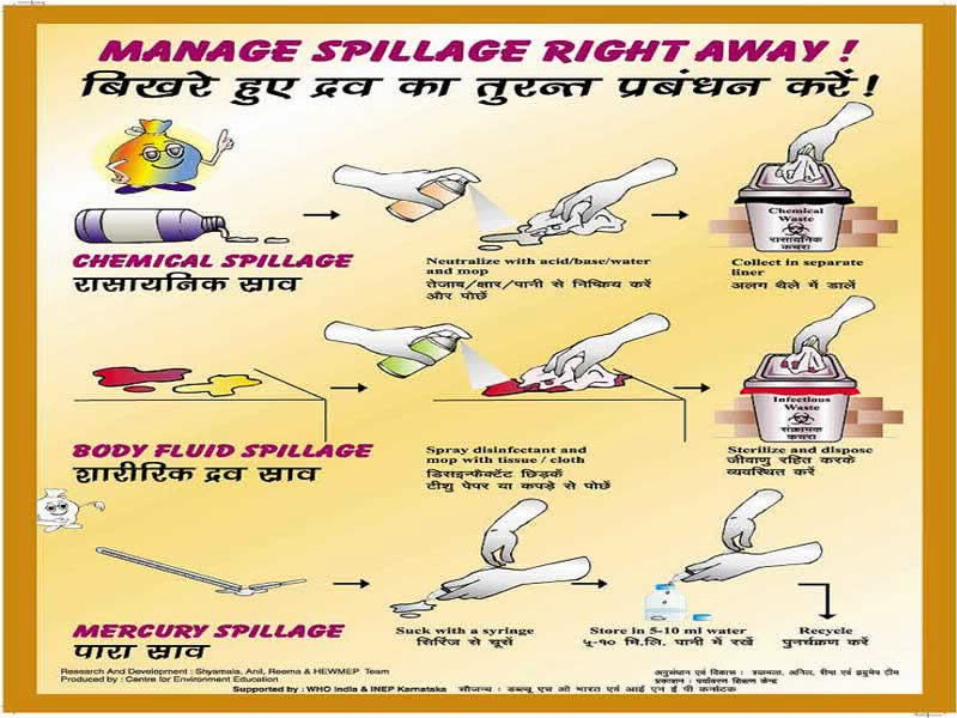
Education and Training is an integral component of O&M of CHAMP which we call Healthcare Establishments Waste Management and Education Programme (HEWMEP)
Training of HCE personnel is being done at different levels. This includes training for doctors, nurses, administrators, paramedical personnel, housekeeping staff, engineering, kitchen and laundry personnel, ayahs, wardboys, security staff, gardeners, rag pickers, sorters, reprocessors and people from different areas in the hospitals who are involved in Bio-Medical Waste Management (BMWM)
Different types of educational material have been prepared, published and used for the training, with approval from MoEF, Govt of India, WHO-India & Govt. of Karnataka. The materials used are in Kannada, Hindi and English
Education &Training on Biomedical Waste Management
Feb 2010

Feb 2010
Feb 2010

Feb 2010
Feb 2010
Feb 2010
Feb 2010
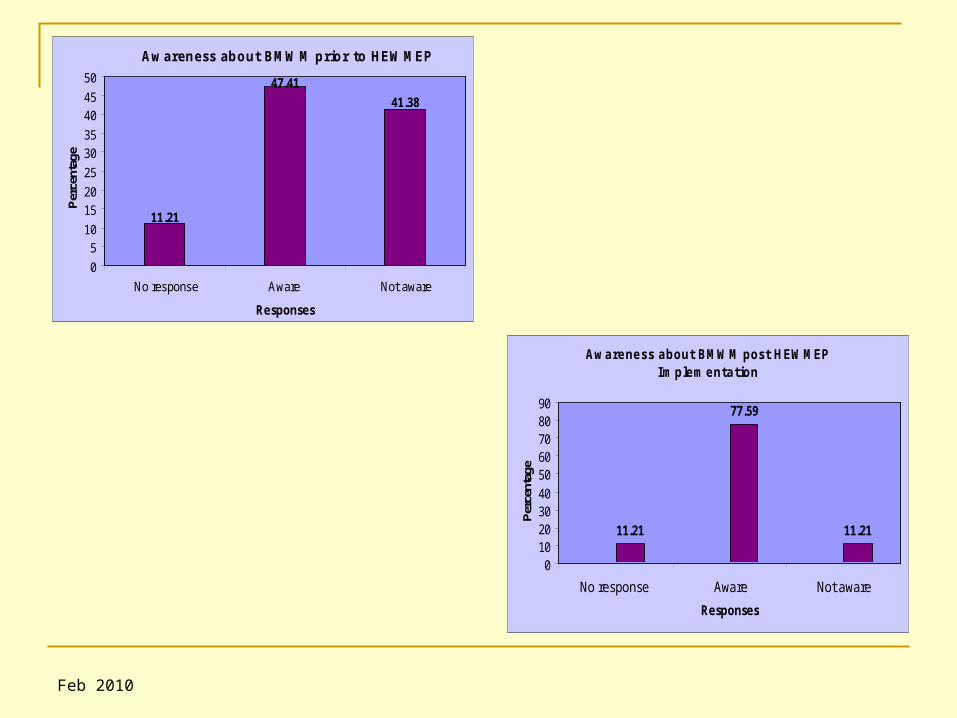
Scenario before and after HEWMEP, Gulbarga & Implementation of CHAMP A ‘Knowledge, Attitude and Practice (KAP)’ survey in all
Healthcare Establishments (HCEs) in Gulbarga was carried out in 2002 (prior to implementation of CHAMP) and subsequently in 2007 - 2008 (after CHAMP became operational) for ascertaining the level of awareness and compliance to the biomedical waste management (BMWM) Rules and prescribed procedures
The survey showed that although the HCEs still lag behind in the implementation of various recommended BMWM procedures (specifically those which have cost implications), there has been tremendous improvement in awareness amongst the healthcare workers especially after implementation of CHAMP
Feb 2010
Awareness about BMWM prior to HEWMEP
11.21
47.41
41.38
0
510
1520
25
3035
4045
50
No response Aware Not aware
Responses
Per
cent
age
Awareness about BMWM post HEWMEP Implementation
11.21
77.59
11.21
0102030405060708090
No response Aware Not aware
Responses
Per
cent
age
Feb 2010
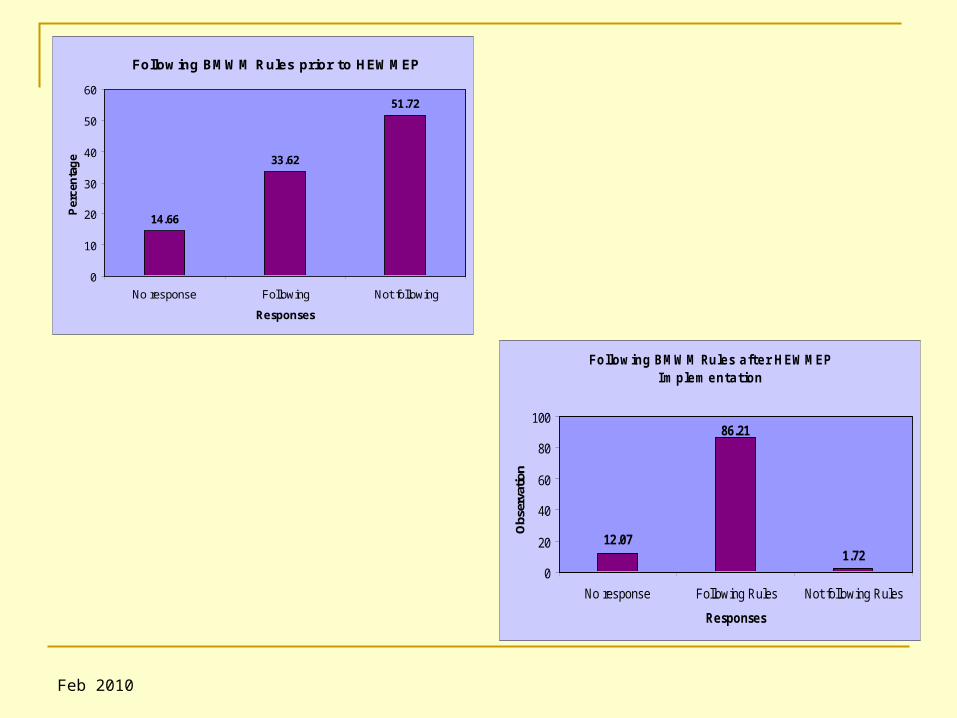
Following BMWM Rules prior to HEWMEP
14.66
33.62
51.72
0
10
20
30
40
50
60
No response Following Not following
Responses
Per
cen
tag
e
Following BMWM Rules after HEWMEP Implementation
12.071.72
86.21
0
20
40
60
80
100
No response Following Rules Not following Rules
Responses
Obs
erva
tion
Feb 2010
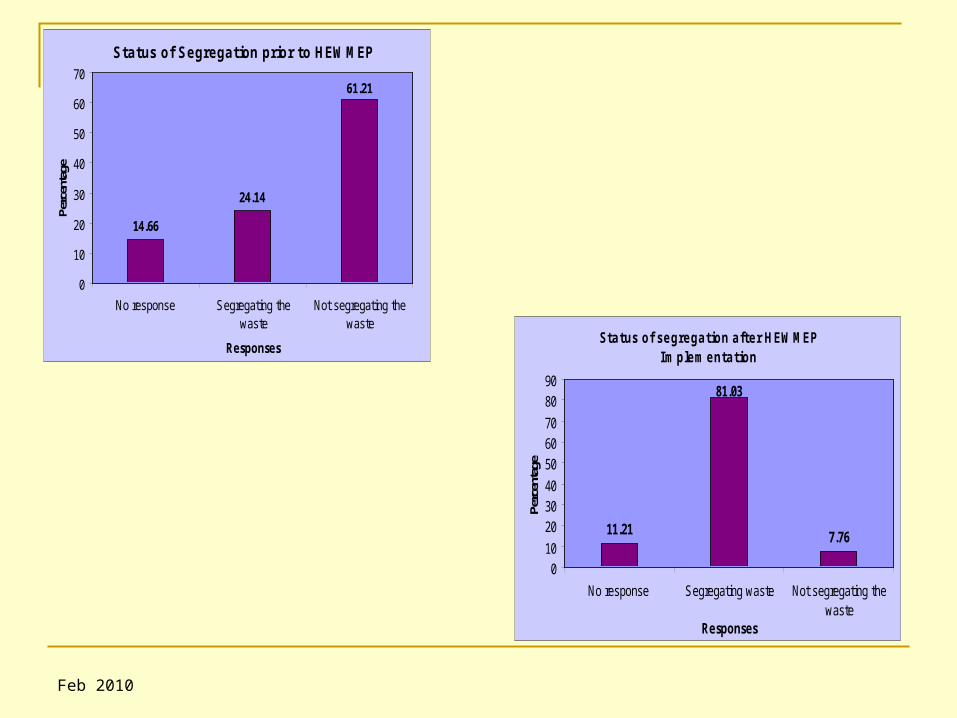
Status of Segregation prior to HEWMEP
14.66
24.14
61.21
0
10
20
30
40
50
60
70
No response Segregating thewaste
Not segregating thewaste
Responses
Perc
enta
ge
Status of segregation after HEWMEP Implementation
11.21 7.76
81.03
010
203040
506070
8090
No response Segregating waste Not segregating thewaste
Responses
Perc
enta
ge
Feb 2010
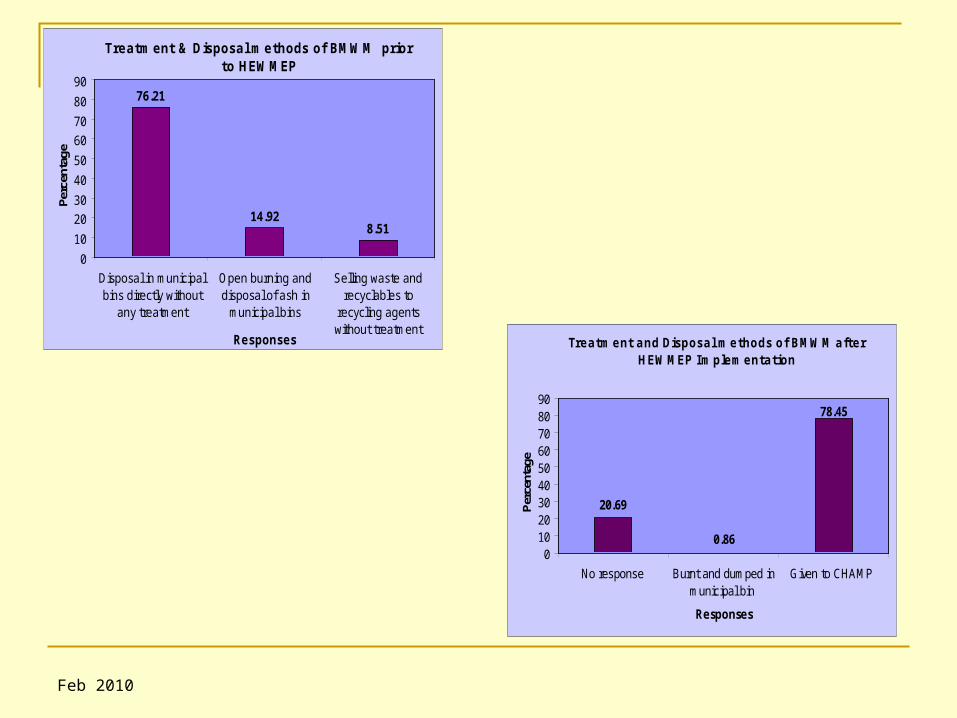
Treatment & Disposal methods of BMWM prior to HEWMEP
76.21
14.928.51
0
10
20
30
40
50
60
70
80
90
Disposal in municipalbins directly without
any treatment
Open burning anddisposal of ash in
municipal bins
Selling waste andrecyclables to
recycling agentswithout treatment
Responses
Perc
enta
ge
Treatment and Disposal methods of BMWM after HEWMEP Implementation
20.69
0.86
78.45
0102030405060708090
No response Burnt and dumped inmunicipal bin
Given to CHAMP
Responses
Per
cent
age
Feb 2010
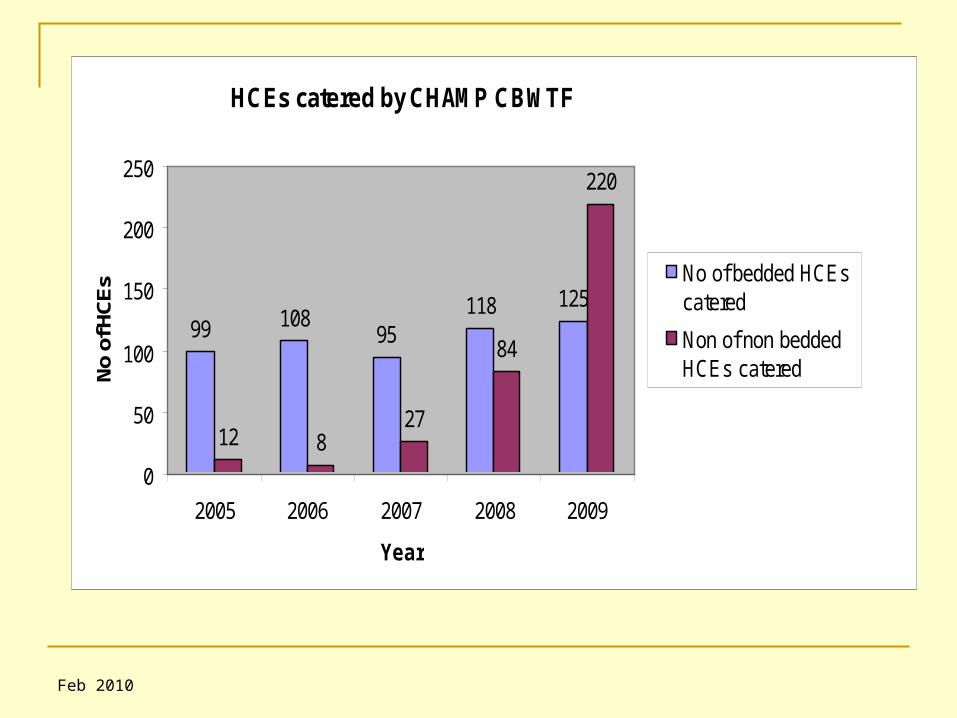
HCEs catered by CHAMP CBWTF
99 10895
118 125
12 827
84
220
0
50
100
150
200
250
2005 2006 2007 2008 2009
Year
No
of H
CE
s No of bedded HCEscatered
Non of non beddedHCEs catered
Feb 2010
Segregation of waste at source is improving but needs to be combined with improvement of collection and segregated treatment
Although the hospital staff in Govt. hospitals and Maternity homes are trained and aware about BMWM practices but they are not able to implement the practices properly due to lack of resources, facilities and motivation among the seniors in the HCEs
None of the hospitals were found disposing their liquid wastes properly
Emphasis on procedures for chemical disinfection for glass and immunization waste in rural areas, disposing of liquid waste in the urban and rural areas and training programmes for all Healthcare Workers (HCWs) is strongly recommended
Conclusion
Feb 2010
Recommended

















