1
California State University, Fresno – Department of Kinesiology
Corrective Exercise to Address Common
Biomechanical Alterations throughout
Each Phase of the Throwing Motion
Stephanie D. Moore-Reed, PhD, ATC
California State University, Fresno
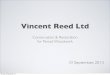
OBJECTIVES
• Six phases of the throwing motion
• Key breakdowns in the kinetic chain
• Assessment Techniques
• Corrective Exercises
1.Windup
2.Early Cocking (Stride)
3.Late Cocking
4.Acceleration
5.Deceleration
6.Follow Through
SIX
PH
AS
ES
Meister, AJSM 2000
Terminology
• Lead/Stride leg:
contralateral to throwing arm
• Trail/Stance leg: ipsilateral to throwing
arm, used to balance
body during cocking phase
Importance of the
Kinetic Chain
• Pitching motion is not an upper extremity action (requires entire
body)
• Reduced stresses on shoulder �
reduced injury risk � increased durability and health of shoulder (career) (Seroyer, Sports Health 2010)
• Improved velocity (Matsuo et al, J Appl
Biomech 2001; Stodden et al, J Appl Biomech
2005; Werner et al, JSES 2008)

2
1.Windup
2.Early Cocking (Stride)
3.Late Cocking
4.Acceleration
5.Deceleration
6.Follow Through
Wind-up
• Start: weight shift from
stride leg to trail leg
• End: maximum knee lift
of stride leg
• Preparation phase –
establishes rhythm
(Meister, AJSM 2000; Dillman et al, JOSPT 1993)Seroyer et al, Sports Health 2010
Wind Up Considerations
• Keep Center of Gravity over trail leg
– Premature movement forward � KC disruption � more stress on UE (Burkhart et al,
Arthroscopy 2003)
• Trail leg characteristics
– Balance/postural control
– Hip abduction strength
• Good peak hip abductor activity � proper throwing mechanics and reduced risk of injury (Yamanouchi,
Kurume Med J 1998)
Seroyer et al, Sports Health 2010
Maintain COG over stance leg
Hip ABD strength
1.Windup
2.Early Cocking (Stride)
3.Late Cocking
4.Acceleration
5.Deceleration
6.Follow Through
Early Cocking (Stride)• Start: Maximum knee lift of stride leg &
ball removed from glove
• End: Stride foot contact
• Generate & transfer momentum up
through the kinetic chain (Stodden et al, J Appl
Biomech 2005)

3
Early Cocking Considerations
• Foot position at stride foot contact
– Foot should point toward home plate (slightly inward)
– Necessary for optimal rotation of hips, pelvis & trunk (Dillman et al, JOSPT 1993)
– Deviation may lead to problems
Stride foot lands in closed position
– Must throw across body
– Slows down rotation of the torso, reducing body’s momentum
�throw delivered entirely by arm
Stride foot lands in open position
– Arm lags behind body
– Pelvic rotation occurs too early �increased stress to anterior shoulder and elbow
Seroyer et al, Sports Health 2010
Early Cocking Considerations
• Quality of stride foot contact
– Hyperextension of knee while planting the stride foot OR landing on the heel � sudden
deceleration of the body (Meister, AJSM 2000)
• Proper pelvic orientation at stride foot contact requires sufficient hip:
– ER ROM of lead leg
– IR ROM of trail leg
– Decreased hip ROM associated with
decreased velocity and poor throwing mechanics (Robb et al AJSM 2010)
Early Cocking Considerations
• Timing of trunk rotation
– Initiation of trunk rotation before stride foot contact � higher elbow valgus
torques (Aguinaldo & Chambers, AJSM 2009)
– Proper timing of pelvis rotation followed
by upper trunk rotation maximizes KC
• Improper stride foot angle or position �early rotation of pelvis � additional force
on shoulder and medial elbow (Fortenbaugh et
al, Sports Health 2009)
1.Windup
2.Early cocking (Stride)
3.Late Cocking
4.Acceleration
5.Deceleration
6.Follow Through

4
Late Cocking
• Start: stride foot
contact
• End: shoulder in
max ER (170-185º)
• Scapula retracts to
assist with
achieving this
position & forms a
stable base
Late Cocking Considerations
• Loss of Scapular Muscle Control
– Scapula: base for muscle attachment and link to transfer forces from trunk to arm (Kibler, AJSM
1998)
• Increased protraction
– Hyperangulation in cocking and follow through (Kibler, AJSM 1998)
– SubAC Impingement risk increases
– Disrupts Kinetic Chain
• 20% decrease in energy delivered from trunk�arm requires 33% increase in rotational velocity at the shoulder to deliver same amount of resultant force (Kibler, AJSM 1998)
• Consequence of increased protraction
• Complain of pain at late cocking and early
acceleration
• Posterior inferior supraspinatus tendon
impinged
Internal Impingement
1.Windup
2.Early cocking (Stride)
3.Late Cocking
4.Acceleration
5.Deceleration
6.Follow Through
Acceleration
• Start: maximum ER
• End: ball release
• Scapula begins to protract (controlled!)
• Arm internally
rotates 7000-9000
deg/sec (Dillman et al,
JOSPT 1993; Pappas et al, AJSM 1985)
• Stride leg stabilizing

5
Shoulder Abduction & Lateral Trunk Tilt
• 90-100º
• Altered shoulder
abduction
– Decreased ball velocity (MacWilliams AJSM
1998)
– Increased varustorque at elbow (Matsuo,
J Appl Biomech 2001;
Aguinaldo & Chambers, AJSM
2009)
Arm Slot Variations
• Sidearm delivery �higher elbow valgus torques compared to overhand arm slot (Matsuo et al 2000;
Aguinaldo & Chambers, AJSM 2009)
Sidearm 3/4
Aguinaldo & Chambers, AJSM 2009
Submarine
Increased ball velocity associated with…
• Greater knee extension motion & velocity (Matsuo
et al, 2001; Escamilla et al, Sports Biomech 2002; Werner et al, JSES
2008)
• Greater forward trunk tilt (Stodden, J Appl Biomech 2005;
Escamilla et al, Sports Biomech2002)
…at ball release
Seroyer et al, Sports Health 2010
1.Windup
2.Early cocking (Stride)
3.Late Cocking
4.Acceleration
5.Deceleration
6.Follow Through
Deceleration
• Start: Ball
release
• End: Max IR
• Reversal of
earlier phases
• Most “violent”
phase – greatest
joint loads
Deceleration Characteristics
• Velocity -500,000 deg/sec2 (Pappas et al,
1985; Dillman et al, 1993)
• Distraction forces as high as 81% BW (Werner et al, JSES 2007)
– Compressive force >1000 N-m (Fleisig et al, 1995;
Dillman et, JOSPT 1993)
• Posterior musculature working
eccentrically to slow down arm
• Hip abductors of stride leg maintain
balance

6
Deceleration Considerations
• Tightness of posterior shoulder
musculature
— Decreased Internal Rotation
— Decreased Horizontal Adduction
Infraspinatus
Teres minor
Posterior deltoid
Posterior Deltoid
Deceleration Considerations
• Posterior Capsule Tightness
• Decreased internal rotation
• Decreased horizontal adduction
• Decreased flexion
• Decreased abduction
(Tyler et al, AJSM 2000; Burkhart et al,
Arthroscopy 2003)
1.Windup
2.Early cocking (Stride)
3.Late Cocking
4.Acceleration
5.Deceleration
6.Follow Through
Follow Through
• Body moves forward with the arm
• Rebalancing phase
• Culminates in pitcher in fielding position (Fleisig, AJSM 1995)

7
1.Windup
2.Early Cocking (Stride)
3.Late Cocking
4.Acceleration
5.Deceleration
6.Follow Through
SIX
PH
AS
ES
KEY POINTS OF BREAKDOWN IN THE KINETIC CHAIN
Key Breakdowns – Lower
Extremity
1. Trail leg hip abductor weakness
2. Premature forward motion
3. Stride leg foot placement & quality
4. Limited hip ER/IR ROM
5. Too much knee flexion @ ball release
Key Breakdowns – Trunk
1. Timing of pelvis and trunk rotation
2. Decreased forward trunk tilt
3. Weakness in core strength
Key Breakdowns – Upper
Extremity
• Shoulder Abduction varies from 90-100º
• Scapular Muscle Imbalance/Scapular
Dyskinesis
• Increased scapular protraction
• Diminished max ER ROM
• Tightness of posterior capsule &
musculature
ASSESSMENT

8
Assessment
• LE & Trunk
– Hip IR/ER ROM
– Hip abductor strength
– Single-leg stance & squat
– Three plane core assessment
• UE
– Glenohumeral ER/IR ROM
– Horizontal Adduction ROM
– Humeral Retroversion
– Scapular Dyskinesis
Hip IR/ER ROM
Laudner et al, AJSM 2010
Hip Abduction MMT
Laudner et al, AJSM 2010
Correct Trunk
Pelvis & Hip
Hip & Knee
SIN
GLE
LE
G S
QU
AT
3 - 5 repetitions
Cro
ssle
y e
t a
l, A
JS
M 2
011
Three Plane Core Assessment
Sagittal Plane Testing
Evaluates eccentric
strength of abdominals, quads, and hip flexors
Concentric strength of
hip and spine extensors
Frontal Plane
Testing
Evaluates eccentric strength of QL, hip
abductors
Transverse Plane
Testing
Evaluates abdominals, hip rotators, spine
extensors
Kibler et al, Sports Med 2006
• Decreased internal rotation (IR) with
concomitant external rotation (ER) gain
(Bigliani AJSM 1997; Ellenbecker JOSPT 1996)
• Total arc of motion
(IR+ER) similar bilaterally (Borsa MSSE 2006; Ellenbecker MSSE 2002)
Typical Motion Alterations in
Overhead Athletes
Consequences of repetitive
throwing
Seroyer et al, Sports Health 2009

9
Bony Contribution
• Humeral retroversion: angle of the axis of the humeral head in a medial and
posterior direction relative to the axis of the elbow joint (Reagan et al, AJSM 2002; Kronberg et
al, CORR 1990, Gordon et al, JSES 2000)
• At birth = MORE retroverted, diminishes over time (Gordon et al, JSES 2000)
Bony Contribution
• Larger angle of retroversion associated with greater ER motion (Kronberg CORR 1990)
• May be advantageous for achieving max ER and ball velocity
More humeral retroversion
Less humeral retroversion
Pieper AJSM 1998
Glenohumeral Internal Rotation
Deficit (GIRD)
– 15°loss of IR compared
to non-dominant arm
and
– 10°loss of total arc of
motion compared to
non-dominant arm
Association of Limited ROM with
Injury
• Secondary subacromial impingement (Tyler et al, AJSM 2000; Warner et al, AJSM 1990)
• Superior labral lesions (Burkhart et al, Arthroscopy 2003; Huffman et al, AJSM 2006)
• Internal impingement (Myers et al, AJSM 2006; Tyler et al, AJSM 2010)
• Ulnar Collateral Ligament tears(Garrison et al, AJSM 2012)
Passive Rotational ROM
Internal
Rotation ROM
• Internal and External Rotation
• Total Arc of Motion
• Supine
• 90°shoulder abduction
• 90°elbow flexion
• Humerus supported to maintain alignment
• Scapula stabilized at coracoid (Wilk, Sports
Health 2009)
0º
Passive Horizontal Adduction
Laudner, JAT 2006
• Supine
• Begin in 90°shoulder abduction and neutral rotation
• Stabilize scapula at lateral border with downward force
• Move humerustoward midline of
body
0º
Angle created by the end
position of the humerus with respect to 0°horizontal
adduction (vertical dotted line).
(-)(+)

10
True Glenohumeral MotionScapula stabilized
Scapula stabilized
Scapula unstabilized
Scapula unstabilized
Internal Rotation
ROM
Horizontal Adduction
ROM
Clinical Assessment of Humeral
Retroversion
Dominant (right) armMore resting ER
Non-Dominant (left) arm
Normal Scapular Kinematics• During humeral elevation:
– Upward rotation
– External rotation
– Posterior tilt
POSTERIOR TILTUPWARD ROTATION EXTERNAL ROTATION
Normal Scapular Kinematics
• During humeral elevation:– Elevation– Retraction (adduction + ER)
Force Couples at Scapulothoracic Joint
Serratus anterior –
trapezius
Upper trapezius – lower
trapezius
SICK Scapula
• Scapular malposition
• Inferior medial border
prominence
• Coracoid pain &
malposition
• dysKinesis of scapular
movementBurkhart et al, Arthroscopy 2003

11
Scapular Examination: Observation
Static resting position:
• Elevation/depression
• ABD/ADD
• Up/downward rot
• Winging
– Med border
– Inferior angle
• Atrophy
Dynamic movement:
• Scapulohumeralrhythm
• Concentric &
eccentric phases
• Repetition
• With load
Scapular Testing/Strengthening
• Trapezius
– Upper
– Middle
– Lower
• Serratus anterior
• Rhomboids
• Latissimus dorsi/teres major
• Levator scapulae
Scapular Assistance Test
Positive test �issue with muscular balance
during scapular upward rotation
1. Unassisted active humeral elevation
– Rate pain
2. Assist scapular upward rotation during active
humeral elevation
– Rate pain
• Positive test = ↓pain
– Implications?
Force Couples at Scapulothoracic Joint
Serratus anterior –
trapezius
Upper trapezius – lower
trapezius
Scapular Retraction Test
1. Resisted elevation (isometric) in
scaption
– Note strength & pain
2. Add manual scapular retraction
– Note strength & pain
• Positive test = ↑strength or ↓pain
– Implications?
Posterior Shoulder Endurance Test (PSET)
• Metronome with verbal cues
• 2% of body weight
• 90 degree arc of motion
• Repetitions to fatigue

12
CORRECTIVE EXERCISE TECHNIQUES
Lower Extremity
Lateral Slide Supported SL Squats
Monster Walks
Trunk / Core
Chop Lift
Ellenbecker & Cools BJSM 2010

13
Posterior Shoulder Stretching:
Patient AppliedSleeper Stretch (Oyama AT and Sports Healthcare 2010; Laudner JAT
2008)
1 2
3
Posterior Shoulder Stretching:
Patient Applied
Cross-Body Stretch (McClure, JOSPT 2007; Manske, Sports Health, 2010)
Self-applied cross-body, scapula unstabilized
Self-applied cross-body, scapula stabilized
Posterior Shoulder Stretching:
Clinician Applied
Clinician-applied cross-body,
scapula stabilized
Clinician-applied internal rotation,
scapula stabilized
Pectoralis Major
Pectoralis Minor Quadratus Lumborum

14
Latissimus Dorsi T-Spine Mobility
Bow & Arrow Circle Stretches
Self-mobilizations
But what if static stretching isn’t
effective?!
Other interventions to consider…
• Hold-relax techniques
• Muscle Energy Techniques
• Soft tissue mobilization
• Massage
• Cross friction massage/Instrument
assisted mobilization
• Assess for altered arthrokinematics
• Joint mobilizations
Muscle Energy Techniques
MET for the Horizontal Abductors
• Parameters of
Application (Moore, JOSPT 2011)
→5 second isometric contraction (Horiz
Abd)
→30 second active
assistive stretch
(Horiz Add)
→3 repetitions total
Improved HA ROM 7±11º
IR ROM 4±5º
Muscle Energy Techniques
• Parameters of
Application • (Moore, JOSPT 2011)
→5 second isometric contraction (ER)
→30 second active assistive stretch (IR)
→3 repetitions total
MET for the External Rotators
Improved HA ROM 5±9º
Soft Tissue Mobilization
• Ischemic compression• Transverse friction massage
• Focused myofascial stretch• Instrument assisted (IASTM)• “Massage” ??
• Reduces pain and sensitivity of trigger points
(Chatchawan, J Bodywork and Mvmt Ther 2005;
Hong, J Musculoskeletal Pain 1993)
• Improves function and ROM (McKechnie, J Sport Sci and Med 2007; Hunter, BJSM 2006;
van den Dolder, Aust J Physio 2003)

15
Joint Mobilizations
• Posterior mobilizations directed at posterior
capsule (Manske, Sports Health 2010; Muraki, JOSPT 2011)
• Parameters of Application
– Grades III and IV
– 10 minute treatment
(Manske, Sports Health 2010)
Strengthening / Neuromuscular
Re-Education
• Arm fatigue while pitching is a risk factor
for shoulder and elbow pain in youth baseball pitchers (Lyman et al, MSSE 2001)
Scap
ula
r C
lock
Dynamic Low Row
Mid
Ro
w
Serratus Anterior – Punches
Serratus Anterior – Push Up Plus
Fe
nc
ing
Robbery

16
Shoulder Dump (Lawnmower Overhead)
Lawnmower
Eccentrics & Plyometric Deceleration
Sid
ely
ing
ER
Neg
ati
ves
Sidelying Ball Drops
Prone Ball Drops
1 2
3 4
Standing ER Plyos

17
IWTYC: “I Would Throw You a
Curveball”
Throw Like A Pro App
• 14 HS baseball players
• Age 16 ± 2 years
• Height 182 ± 8 cm
• Mass 75 ± 11 kg
• No recent UE injury
• Compliant to protocol
– attended 2/3 of sessionsSports Health 2009
Intervention: Clinic (20 weeks)
• UBE warm up
• Theraband
– Rows
– ER & IR at 90-90
– Prone ER
• PHA (“T”s)
• Sidelying ER neg
• Rebounder at 90-90
• Wrist curls
• Rice bucket
• 4 way hip
• Lateral step (80 ft)
• Hamstring curls (bilateral & single
neg)
• Calf raises
Intervention: Field (Weeks 1-10)
• Warm up run
• Theraband
– Rows
– ER & IR at 90-90
– Bicep curls
– Tricep extensions
– Chest press
– Twists
• Power cord
– Squats
– Lateral step
– Backward step
• Calf raises
• Abdominals

18
Intervention: Weight Room
(Weeks 11-20)
• Seated rows
• Lat pulls
• Calf raises
• Hamstring curls
• Leg press
• Squats
• Knee extensions
• Abdominals
• Warm up run
• Theraband
– Rows
– ER & IR at 90-90
– Bicep curls
– Tricep extensions
– Twists
• Supine chest press
Results
• Posterior shoulder endurance improved
– Baseline: 30 ± 14 reps
– 4 weeks: 66 ± 26 reps
– 20 weeks: 88 ± 36 reps
California State University, Fresno – Department of Kinesiology
Thank You!
Questions?
Stephanie Moore-Reed, PhD, ATC
Email: [email protected]
fresnostate.box.com/FWATA2015
Recommended