Don P. Wilson, M.D., FNLAFellow, American Board of Clinical Lipidology
Director, Pediatric Cardiovascular Risk Prevention Clinic
Pediatric EndocrinologyCook Children’s Medical Center
Fort Worth, Texas
Guidelines for Cardiovascular Health and Risk Reduction in Children and Adolescents

1. Atherosclerotic CVD is the #1 cause of death in the US and other developed counties.
2. This process begins in childhood.3. The cardiovascular risk factors that lead to
the development of atherosclerosis:a. Can be identified in childhood.b. Their number and intensity relate to the
development and progression of atherosclerosis, beginning in childhood.
c. Track from childhood into adult life.d. Interventions exist for their management.
Rationale

Pediatric Screening Guidelines
1992
Population ApproachTargeted Screening Pediatrics 1992;89:525–584
2008
Population ApproachTargeted ScreeningRisk Factors - ObesityRisk Conditions
Circulation 2006;114:2710-38Circulation 2007;115:1948-1967Pediatrics 2008;122:198-208
2011
Population ApproachTargeted ScreeningRisk Factors - ObesityRisk ConditionsUniversal Screening 9 – 11 yrs of age
Pediatrics 2011;128:Supp 213-256
1998
Population ApproachTargeted ScreeningRisk Factors
Pediatrics 1998;101:141-147

In 2006, the National Heart, Lung and Blood Institute (NHLBI) convened a panel of experts to develop comprehensive evidence-based guidelines addressing the known risk factors for CVD.
Goal:Assist primary pediatric careproviders in the prevention of:• Risk factor development – primordial
prevention.• Future CVD by effective management of
identified risk factors – primary prevention.The full report is available at: http://www.nhlbi.nih.gov/guidelines/cvd_ped/index.htm

Risk Factor Tracking

Unique Aspects of CVD Risk in Children:• The extended interval between identification
of risk factors and disease expression.• The ability of the child and family to
understand and implement medical advice.• The need for recommendations that are
specific to the age and developmental stage of the child.
• The necessity for regular updates to the medical history, since the family history evolves as a child matures.

Dietary RecommendationsInfants
• Exclusive breast-feeding for the first 6 - 12 months of life.
• If breastfeeding is not possible, feeding human milk by bottle is 2nd best, with formula – feeding as the 3rd choice.

Dietary Recommendations Children > 2 yr of age
*% of daily kcal/EER

NOTE: Values given are in mg/dL; to convert to SI units, divide the results for TC, LDL-C, HDL-C and non-HDL-C by 38.6; for TG, divide by 88.6.Values for plasma lipid and lipoprotein levels are from the National Cholesterol Education Program (NCEP) Expert Panel on Cholesterol Levels in Children. Non-HDL-C values from the Bogalusa Heart Study are equivalent to the NCEP Pediatric Panel cut points for LDL-C. Values for plasma apo-B and apoA-1 are from the National Health and Nutrition Examination Survey III.
Acceptable, Borderline-High, and High Plasma Lipid, Lipoprotein and Apolipoprotein Concentrations (mg/dL) For Children and Adolescents
Values represent approximately the *75th and **95th percentiles.

Acceptable, Borderline-High, and High Plasma Lipid, Lipoprotein and Apolipoprotein Concentrations (mg/dL) For Children and Adolescents
*Low cut points for HDL-C and apoA-1 represent approximately the 10th percentile.

Cholesterol Levels and Age• Increase for the first 2 years
of life.
• TC and LDL-C levels:– Plateau between 9 – 11 yrs– Fall as much as 10-20% or
more during puberty.
• Based on this normal pattern of change with growth and maturation, age 10 years (range age 9-11 years) was selected for the ideal time for Universal Lipid Assessment.

Who to screen:1.Children 2-18 years of age:
a. In whom 1 or both parents are known to have hypercholesterolemia or are receiving lipid lowering medications;
b. Who had a family history of premature cardiovascular disease (men < 55 years of age; women < 65 years of age);
c. Whose family history is unknown (e.g. children who were adopted).
Screening Guidelines

Who to screen: (continued)d. Children with moderate to high risk for premature
CVD.
Screening Guidelines
*Systemic Lupus Erythematosus, Juvenile Rheumatoid Arthritis

Who to screen:2. All children (Universal Screening)
regardless of general health or the presence / absence of CVD risk factors, who are:a. 9 – 11 years of age.b. 17 – 21 years of age.
Screening Guidelines

What to order:• Fasting or non-fasting lipid panel*.
• For non fasting lipid profiles, a non-HDL-C** is recommended for the initial screening test.
Screening Guidelines
*Total cholesterol / triglycerides / HDL-c / LDL-c**Non HDL-cholesterol = Total cholesterol – HCL-c

Routine measurement of the following are not recommended at this time:1. ApoB and ApoA-1.2. Lipoprotein (a)*3. Lipoprotein subclasses and their sizes by
advanced lipoprotein testing.
* Lp (a) is useful in the assessment of children with both hemorrhagic and ischemic stroke
Lipids and Lipoproteins in Children and Adolescents

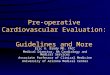
Universal ScreeningInterpreting the Results
*Non HDL cholesterol = Total cholesterol – HDL cholesterolFLP = Fasting Lipid Profile

Fasting Lipid Profile (FLP) x 2 – Average
Step #1 Refer to Lipid Specialist if:• LCL-c > 250 mg/dl• Tg > 500 mg/dl
Step #2 Exclude Secondary Causes
Step #3 Refer to a registered dietitian for family medical nutrition therapy.
• Start CHILD-1• Progress to CHILD-2 as needed
CHILD = Cardiovascular Health Integrated Lifestyle Diet

FHx = Family History; RF = Risk Factor


Patient Selection
• Algorithm and risk factor categories are used to select patients who are appropriate for statin therapy.
• Include preferences of patient and family in decision making.
• In general, do not start treatment with statins before age 10 years *
*Children with high-risk family history, high-risk conditions, or multiple risk factors might be considered for medication initiation at age 10 years or younger.

Initiation and Titration
• Choice of particular statin is a matter of preference.
• Start with the lowest dose once daily.

Initiation and Titration
If target LDL-C levels are not achieved:• Increase the dose by one increment (usually
10 mg) and repeat the lipid profile and LFTs in 4 weeks.
• If target LDL-C levels are still not achieved, dose may be further increased by one increment .
orAnother agent (bile acid sequestrant or cholesterol absorption inhibitor) may be added under the direction of a lipid specialist.

Monitoring

Monitoring

Monitoring

ConclusionsThe NHLBI Expert Panel’s Integrated Guidelines (2011) provide developmentally appropriate recommendations for:• Prevention of CVD risk factors in all
children.• As well as specific recommendations
for treatment, monitoring and follow-up for those at highest risk.

Given the impact of premature CVD on the well-being of future generations and its cost to society, it is important that such guidelines be understood and consistently implemented by primary care providers.
Conclusions

Although not without controversy, these guidelines help create an awareness about the burden of CVD as well as the opportunity for prevention, and in selected individuals, the benefits of early and effective medical intervention.
Conclusions

References1. Expert Panel on Integrated Guidelines for Cardiovascular Health and Risk
Reduction in Children and Adolescents, & National Heart, Lung, and Blood Institute. (2011). Expert panel on integrated guidelines for cardiovascular health and risk reduction in children and adolescents: summary report. Pediatrics, 128 Suppl 5, S213-56.
2. Daniels, S. R., Greer, F. R., & Committee on Nutrition. (2008). Lipid screening and cardiovascular health in childhood. Pediatrics, 122(1), 198-208.
3. American Academy of Pediatrics. Committee on Nutrition. (1998). American Academy of Pediatrics. Committee on Nutrition. Cholesterol in childhood. Pediatrics, 101(1 Pt 1), 141-147.
4. National Cholesterol Education Program (NCEP): highlights of the report of the Expert Panel on Blood Cholesterol Levels in Children and Adolescents. (1992). Pediatrics, 89(3), 495-501.
5. American Academy of Pediatrics. National Cholesterol Education Program: Report of the Expert Panel on Blood Cholesterol Levels in Children and Adolescents. (1992). Pediatrics, 89(3 Pt 2), 525-584.

Expert Panel Members• Stephen R. Daniels, MD, PhD, Panel Chair , Univ of Colorado, Denver, CO
• Irwin Benuck, MD, PhD., Northwestern Univ Feinberg, Chicago, Il
• Dimitri A. Christakis, MD, MPH, Univ of Washington , Seattle, WA
• Barbara A. Dennison, MD, New York State Department of Health , Albany, NY
• Samuel S. Gidding, MD, Alfred I du Pont Hospital for Children , Wilmington, DE
• Matthew W. Gillman, MD, MS , Harvard Pilgrim Health Care , Boston, MA
• Mary Margaret Gottesman, PhD, RN, CPNP, Ohio State Univ – CON, Columbus, OH
• Peter O. Kwiterovich, MD, Johns Hopkins Univ , Baltimore, MD
• Patrick E. McBride, MD, MPH, Univ of Wisconsin and Public Health, Madison, WI
• Brian W. McCrindle, MD, MPH, The Hospital for Sick Children, Toronto, ON
• Albert P. Rocchini, MD, C.S. Mott Children's Hospital, Ann Arbor, MI
• Elaine M. Urbina, MD, Cincinnati Children's Hospital Medical Center , Cincinnati, OH
• Linda V. Van Horn, PhD, RD, Northwestern Univ – Feinberg School of Medicine, Chicago, IL
• Reginald L. Washington, MD, Rocky Mountain Hospital for Children , Denver, CO
Recommended