
Highlights from the Medical Literature:Top 10 Cardiovascular Articles from 2012
Michael J Bloch, MD, FACP, FVM, FASHDepartment of Medicine,
University of Nevada School of Medicine

Faculty Disclosures
Michael J. Bloch, M.D.• Consultant: Astra-Zeneca; Takeda; Aegerion• Speaker’s Bureau/Honoraria: AstraZeneca,
Takeda, Boeringer-Ingellheim, Daiichi-Sankyo, Liposcience

Learning Objective
At the conclusion of this session, the learner should be able to:
•Explore specific findings that have been published in the cardiovascular literature within the past 12 months in order to apply relevant findings to his or her clinical practice

Studies In Clinical Hypertension

Bedtime dosing of antihypertensive medications reduces cardiovascular risk in
chronic kidney disease
Hermida RC, et al. J Am Soc Nephrol. 2011;22(12):2313 2321.

Nocturnal Dosing BP Rx
Background:•Previous studies with ambulatory BP monitoring (ABPM) have demonstrated that the mean sleep-time BP is a better predictor of CV events than is the mean daytime or 24-hr BP.•BP Rx has traditionally been dosed primarily in the morning.•Some recent studies have suggested that restoration of the normal circadian “dipping” pattern of nocturnal BP by giving some of the antihypertensive rx at bedtime may lead to lower CV risk•Nocturnal hypertension common in CKD

Nocturnal Dosing BP Rx
Question:
In hypertensive patients with CKD, does giving at least one of the HTN medications at bedtime reduce CV risk compared to giving all medications upon waking?

Nocturnal Dosing BP Rx
Methods:•661 hypertensive patients with mild CKD (about ½ with Cr Cl >60 ml/min but + microalbuminuria)•About 2/3 were “nondippers” (BP did not exhibit normal circadian drop at night)
•All patients were on once daily BP Rx. •Randomized to take at least one BP rx at bedtime or to continue taking them all upon awaking.•ABPM was done for 48 hours at baseline and at least yearly.•Median follow-up was 5.4 years •Primary outcome was total CV events (CV death, MI, and stroke)

Nocturnal Dosing BP Rx
Results:
•The adjusted hazard ratio for major CV events was 0.28 for nocturnal vs morning dosing
•Major CV events were 1.45%/yr for the AM dosing vs 0.51%/yr for bedtime dosing

Nocturnal Dosing BP Rx
Results:
•The awake BP mean was no different between the groups
•However, the sleep systolic BP mean was 6 mmHg lower in the bedtime dose group, and a greater number reverted to a “dipping” pattern (59% vs 29% in AM dose group at end of study)

Nocturnal Dosing BP Rx
Conclusions:
•In hypertensive patients with mild CKD on once daily BP medications, moving at least one of the doses to bedtime reduces CV morbidity
Caveats:•Clinic BPs in both groups at end of study were above accepted targets (mean 146/80). •It is unclear if the magnitude of benefit would be as great if all patients had been more aggressively treated.

Nocturnal Dosing BP Rx
Clinical Implications:
•While awaiting further data:• In patients with mild CKD (and possibly others), it’s
reasonable to switch at least one of their BP rx to bedtime dosing (unless the patient is at high risk for falls in the night or for decreased compliance)
• What about other hypertensive populations?
• Do we need to do more ABPM?

Intensive BP and/or Glucose Control Did Not Reduce Microvascular Events in
Hypertensive Type 2 DiabeticsPost-Hoc Analysis of ACCORD BP
Ismail-Beigi F, et al, Kidney Int. 2012;81:586-94.

ACCORD BP - Microvascular
Background:•From the ACCORD BP study we know that in patients with hypertension and type 2 diabetes more intensive treatment of BP (goal <120) did not reduce the incidence of macrovascular events as compared to less intensive treatment of BP (goal <140)
Question:•What about microvascular events?

ACCORD BP - Microvascular
Methods:•Post-hoc analysis of ACCORD BP study•4733 patients 40-79 years of age with T2DM and HTN randomized to SBP goal <120 mmHg or <140 mmHg•Patients also randomized to hbA1C target of <6.0% or <7.0-7.9%•Mean f/u 4.7 years•Primary endpoint – composite of renal and retinal outcomes

ACCORD BP – Microvascular - Results
Outcomes Intensive BP Standard BP RRR (RRI) NNT (NNH)
Primary Composite 11.4% 10.9% +7.5% ns
Incident Microalbuminuria
21% 25% -14% 29
Incident macroalbuminuria
5.7% 7.1% -18% ns
The effect of BP control was not modified by intensity of glycemic control for any outcome

ACCORD BP - Microvascular
Conclusion:•Intensive BP control did not reduce macro- or micro-vascular events more than standard BP control in patients with T2DM and hypertension, regardless of intensity of glycemic control
Caveats•Event rates were low•Follow-up was relatively short•Subjects also had great glycemic, lipid, and tobacco control

ACCORD BP - Microvascular
Systolic BP Goal (mmHg)
Strength of Evidence
Most Patients with Diabetes
<140 Strong, based on primary endpoint
Diabetes Patients with Higher Stroke Risk*
<120# Less Strength, based on secondary
endpoint
*Defined as personal or family history of TIA/stroke, smoker, unable to tolerate statin therapy or antiplatelet therapy when approprioate, LVH or poor glycemic control #With close monitoring for bradycardia, hypotension, changes in electrolytes, and worsening renal function
Clinical Implications:

More Intensive BP Control May Not Be Advantageous in Chronic Kidney Disease
(CKD)The Kidney Early Evaluation Program
(KEEP)
Peralto CA, et al. Arch Intern Med 2012;172:41-47.

BP Goals in CKD - KEEP
Background:•Guidelines have long suggested BP goal <130/80 in patients with CKD•This recommendation is mostly supported by observational data and has been hard to support with RCTs
Question:•What is the optimal BP for a patient with CKD?

BP Goals in CKD - KEEP
Methods•Nation-wide, community based observational study enrolling adults with CKD or its major risk factors•As of 2000, KEEP included data on 16,121 persons with CKD (at least stage 3)•US Renal Data System was used to capture incidence of ESRD•Primary Endpoint: Incident ESRD•Follow-up = 2.7 years

BP Goals in CKD - KEEP
Results•Only 2% of patients progressed to ESRD•48% of patients had baseline SBP>140 or DBP>90•As compared to those with baseline SBP <130, only patients with SBP >150 had increased risk of ESRD•As compared to those with baseline DBP <75, only patients with DBP >90 had increased risk of ESRD•Patients with albuminuria represented only 20% of the cohort, but accounted for 88% of ESRD
– Presence of albuminuria did not effect results of KEEP but has been demonstrated to be a marker of response to intensive BP control in other studies

BP Goals in CKD - KEEP
Conclusions:•In patients with CKD, the hypothesis that more intensive control of SBP to a goal of <130 mmHg decreases the incidence of ESRD remains unproven
Caveats•Short follow-up•Cardiovascular events not meaured•Observational study – hypothesis generating only •Effect of albuminuria unclear and not consistent with previous trials
BP Goals in CKD - KEEP
Clinical Implications•BP is poorly controlled in patients with CKD•BP target of <140/90 probably reasonable for most patients with CKD•Consider more aggressive therapy in those with higher risk of progression to CKD, including young age or presence of albuminuria•Await results of NIH sponsored SPRINT study
– >9000 at risk patients with hypertension randomized to SBP<140 vs SBP<120
– More than 40% of patients expected to have CKD

Renal Sympathetic Denervation for Treatment of Drug Resistant HypertensionOne Year Results from Symplicity HTN-2
INVESTIGATIONAL
Esler MD, et al. Circulation 2012;126:2976-82.

Symplicity HTN-2
Background:•Renal sympathetic nerve activation contributes to the pathogenesis of hypertension•Sympathectomy has been demonstrated to be effective in treating resistant HTN, but with considerable adverse events
Question:•What is the benefit and risk of catheter based renal denervation in patients with treatment resistant hypertension?

Symplicity HTN-2

Symplicity HTN-2
Methods•Eligible patients were on at least 3 BP meds and had a baseline SBP >160mmHg•Randomized to catheter based renal denervation or medical management•This report includes one year results of those patients originally randomized to renal denervation and patients who crossed over after 6 months due to poorly controlled BP

Symplicity HTN-2
Mean BP Immediate Renal Denervation (n=49)
Cross-Over Group (n=35)
Before Procedure 178/96 190/99
6 Months After Procedure
146/84 166/91
12 Months After Procedure
150/87 n/a
Results:
Complications included one renal artery dissectionNo significant changes in eGFR or cystatin c

Symplicity HTN-2
Conclusion•Catheter based renal artery denervation led to significant and sustained reductions in BP in patients with poorly controlled resistant HTN at baseline with limited potential for adverse events
Caveats•Short follow-up, particularly for adverse events•Unblinded

Symplicity HTN-2
Clinical Implications•Catheter based renal denervation is an investigational procedure that may have a role in the treatment of uncontrolled resistant hypertension in the future•May be other indications, including heart failure•Long term safety issues unknown•Await results of Symplicity HTN-3
• RCT that includes sham renal denervation as control group and include ABPM

Clinical Implications of Latest BP Trials
• Switching at least 1 BP med to night-time administration may improve nocturnal BP control and reduce CV events, at least in CKD
• Systolic BP goal of <140 mmHg may be reasonable for most patients with T2DM
• Systolic BP goal of <140 mmHg may be reasonable for most patients with CKD
• Catheter-based renal denervation is an investigational procedure that may prove to be safe and effective in treatment of poorly controlled resistant HTN
• Eagerly await future near-term publications in clinical hypertension, including SPRINT, Symplicity HTN-3, and JNC8

Studies In Clinical Lipidology

Another Investigational CETP Inhibitor Fails to Demonstrate Reduction in Events in Patients
with Recent ACSDal-OUTCOMES
INVESTIGATIONAL
Schwartz GG, et al. New Engl J Med 2012;367:2089-99.

Dal-OUTCOMES
Background•In observational analyses, higher HDL-C is associated with lower risk of CHD events•CETP inhibitors raise HDL-C significantly, but their effects on CV outcomes is unclear•Torcetrapib increased HDL-C, but failed to reduce CV events, perhaps due to mild increase in BP and aldosterone
Question:•Would use of the CETP inhibitor dalcetrapib reduce CHD events in patients with recent ACS?

Dal-OUTCOMES
Methods•15,871 patients with recent ACS•Best available background risk reduction therapy including target LDL-C of around 70 mg/dl with statin therapy•Randomized to dalcetrapib 600 mg daily or placebo•Primary endpoint = composite of fatal and nonfatal CHD•Mean follow-up = 31 months
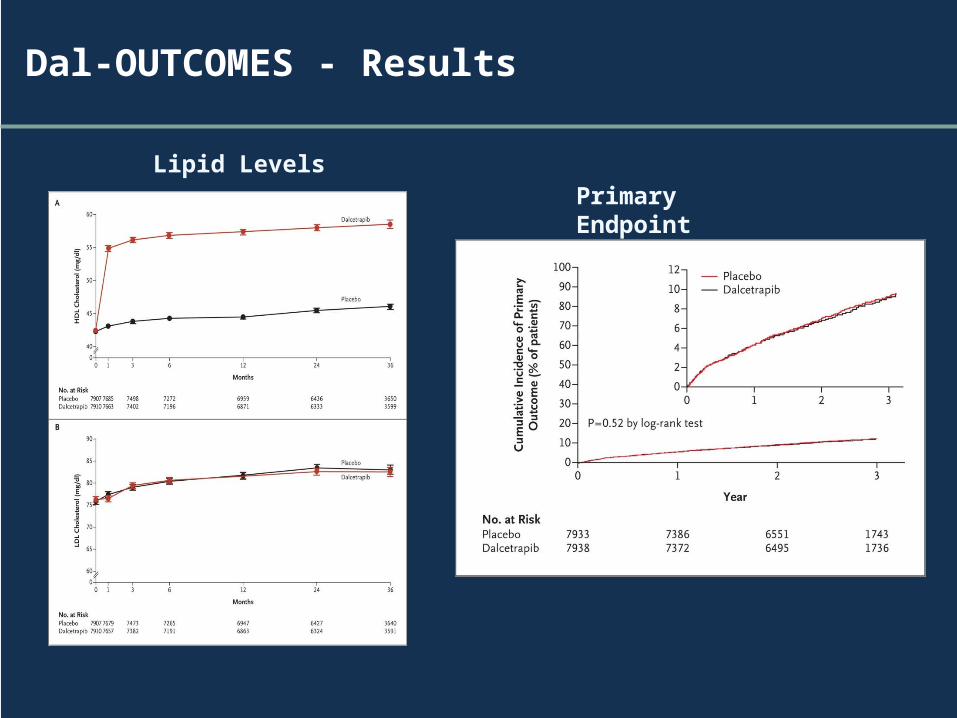
Dal-OUTCOMES - Results
Lipid LevelsPrimary Endpoint

Dal - OUTCOMES
Conclusion•Despite an approximately 35% increase in HDL-C, dalcetrapib did not reduce the risk of recurrent CHD events in patients with recent ACS with well controlled LDL-C
Clinical Implications:•HDL-C is complicated•Endpoint studies needed for lipid lowering drugs, particularly those that have their primary effect on HDL-C or LDL size

Studies In Anti-Platelet and Anticoagulant Therapy

Novel Anticoagulant Now Indicated to Reduce Risk of Recurrent Venous
Thromboembolic Events
EINSTEIN DVT and PE Studies
Pooled Analysis As Presented at American Society of Hematology 2012 Annual Meeting
(Harry Buller, MD)
Einstein Investigators. N Engl J Med. 2010;363:2499-510. Einstein Investigators. N Engl J Med. 2012;366:1287-1297

Einstein DVT and PE
Background•Three novel anticoaglulants (dabigratran, rivaroxaban, and apixaban) are approved as alternatives to warfarin to prevent stroke and systemic embolism in patients with non-valvular atrial fibrillation•DVT/PE is another indication for anticoagulation
Question•How does the factor Xa inhibitor rivaroxaban compare to warfarin in efficacy and safety for patients with a history of venous thromboembolism (DVT or PE)?
Einstein DVT and PE
Methods
•Patients with a history of PE (n = 4832) or symptomatic DVT (n = 3449)
•Randomized to– Rivaroxaban 15 mg twice daily for 3 weeks followed by 20 mg daily
OR
– Standard therapy with enoxaparin followed by dose adjusted warfarin with INR goal 2-3
•Primary efficacy endpoint = symptomatic recurrent thromboembolic event (DVT or PE)
•Primary safety endpoint = major or clinically relevant non-major bleeding

Einstein DVT and PE – Pooled Results
Outcome Rivaroxaban (%) Standard Therapy (%)
Hazard Ratio (HR) with 95% CI
Recurrent VTE 2.1 2.3 0.89 (0.66-1.19)
Major or Clinically Relevant Bleeding
9.4 10.0 0.93 (0.81-1.06)
Major Bleeding 1.0 1.7 0.54 (0.37-0.79
Subgroup analysis favored rivaroxaban in patients with cancer

Einstein DVT and PE
Conclusion•Rivaroxaban in non-inferior to standard therapy with enoxaparin/warfarin in preventing recurrent DVT/PE with similar risk of bleeding
Caveats and Clinical Implications•Rivaroxaban is approved for reducing recurrence of VTE in patients with DVT/PE as an alternative to warfarin•Offers an opportunity for easy out patient management•Does not require monitoring•Cost an issue•Duration of anticoagulation unchanged

Low Dose Aspirin After Completed Course of Anticoagulation Reduces Risk of
Recurrent VTE
ASPIRE
Brighton TA, et al. New Eng J Med 2012;367:1979-87

ASPIRE
Background•Even after completed a traditional course of oral anticoagulation (3-6 months), patients with a history of unprovoked DVT have a relatively high long-term risk of recurrent VTE (around 25% at 5 years)
Question•Would aspirin be effective in preventing a recurrence of VTE in patients with first episode of unprovoked VTE who have completed a traditional course of anticoagulation?

ASPIRE DVT
Methods•822 patients who completed initial anticoagulation therapy after a first episode of unprovoked VTE (DVT or PE)•Randomized to aspirin 100 mg daily or placebo•Primary Endpoint: Recurrent symptomatic VTE•Mean Follow-Up = 37.2 months•Results pooled with another similar previously reported studied (WARFASA)

ASPIRE DVT - Results

ASPIRE DVT
Conclusions•For patients with history of first unprovoked VTE, after completion of a course of anticoagulation, use of aspirin 100 mg daily decreased the incidence of recurrent VTE and CV events with minimal increased risk of bleeding
Caveats and Clinical Implications•Safe, inexpensive intervention•What about provoked DVT?•What is the role of d-dimer and repeat duplex in determining the duration of anticoagulation?
Warfarin Dose Assessment Every 4 Weeks Versus Every 12 Weeks in Patients With Stable International Normalized Ratios
Schulman S, et al. Ann Intern Med. 2011;155:653-659.

INR Testing Frequency
Background:•Clinical guidelines differ on the optimal interval for INR monitoring (limited data)•A 1998 British guideline suggests that monitoring can be done up to every 12 weeks for very stable patients•Underpowered Italian study stated no difference between 4 and 6 week testing
Question: Is assessment of warfarin dosing every 12 weeks as safe as assessment every 4 weeks?

INR Testing Frequency
Methods
•250 patients with unchanged warfarin dosing for at least 6 months randomized to assessment at 4 week or 12 week intervals (noninferiority trial)
•Both groups had nurse visits every 4 weeks
•Nurses following those in the 12 week group were given sham INR results (in range) in 2 of the 3 four week visits
•Primary Outcome = % of time in therapeutic range
•Secondary Outcome = Number of extreme INRs, changes in maintenance dose, major bleeding events, objectively verified thromboembolism, and death
INR Testing Frequency - Results
The percentage of time in the therapeutic range:•74.1% in the 4-week group •71.6% in the 12-week group•This met the requirement for noninferiority
•Secondary outcomes: – No difference between groups– Fewer dosage changes, and fewer extreme
INRs that were >4.5 or <1.5 in 12 week group

INR Testing Frequency
Conclusion:•Assessment of warfarin dosing every 12 weeks seems to be safe and noninferior to assessment every 4 weeks
Caveat and Clinical Implications•This study used sham INR and had monthly RN visits in extended follow-up group•These results demonstrate that the frequency of assessing warfarin dosing may be substantially reduced in stable patients

Addition of Clopidogrel to Aspirin in Patients with History of Lacunar Stroke
SPS 3
SPS3 Investigators. New Eng J Med 2012;367:817-825

SPS-3
Background•Lacunar strokes are a frequent type of stroke caused by cerebral small vessel disease and hypertension usually•Aspirin is the standard of care post lacunar stroke•Addition of clopidogrel to aspirin has been found to be effective in patients with atrial fibrillation and ACS•Combined therapy with clopidorgrel and aspirin is associated with a greater risk of bleeding than with either agent alone
Question•In patients with history of lacunar infarction would the addition of clopidogrel decrease the risk of recurrent stroke?

SPS-3
Methods•3020 patients with recent symptomatic lacunar infarction identified by MRI•All patients on aspirin 325 mg daily •Randomized to clopidogrel mg daily or placebo•Primary Efficacy Endpoint = recurrent stroke•Primary Safety Endpoint = major extracranial hemorrhage •Mean Follow-Up = 3.4 years

SPS-3 - Results
Recurrent Stroke Risk
Safety1)Risk of major hemorrhage doubled with dual therapy (2.1%/yr vs 1.1%/yr) 2)Risk of death increased with dual therapy (113 deaths vs 77 deaths)

SPS-3
Conclusion•Among patients with recent lacunar stroke, the addition of clopidogrel to aspirin did not significantly reduce the risk of stroke but did increase the risk of bleeding and death

SPS3
Clinical Implications and Caveats•Dual anti-platelet therapy should be used only in rare instances and with caution for secondary prevention of lacunar infarction•Does not tell us which is the preferred anti-platelet agent in monotherapy•Does not necessarily apply to other stroke etiologies•Await results of SPS-3 BP arm where patients randomized to SBP goal <130 mmHg vs 130-150 mmHg

Subclinical atrial fibrillation
and the risk of stroke
Healey JS, et al. N Engl J Med. 2012 Jan 12;366:120.

Subclinical Atrial Fibrillation
Background
•25% of all ischemic strokes are cryptogenic, and subclinical atrial fibrillation is suspected to be a possible cause in many of these•The prevalence and prognosis of subclinical atrial fibrillation has been difficult to assess•More than 400,000 pacemakers and ICDs implanted each year in North America •These have the capacity to record episodes of atrial tachyarrhythmia•The significance of pacemaker detected subclinical atrial fibrillation is unknown

Subclinical Atrial Fibrillation
Question:
•In patients with pacemakers or ICDs, does the detection of subclinical atrial tachyarrhythmia signify an increased risk of stroke?

Subclinical Atrial Fib
Methods
•2,580 patients with HTN who had pacemaker (95%) or ICD (5%) placed
•Episodes of atrial rate >190 lasting at least six minutes recorded for 1st three months followup for 2.5 years for ischemic stroke or systemic embolism

Subclinical Atrial Fibrillation - Results
• By 3 months, subclinical atrial tachy had occurred in 10.1% of patients.
• Over the next 2.5 years, the risk of stroke was doubled in these patients compared to those without atrial tachy
• Those who had episodes lasting >17.7 hours had a higher risk of stroke (4.89% per year) than those in lower quartiles of duration
• Risk of developing clinical atrial fibrillation also 5x higher in those with subclinical atrial fibrillation

Subclinical Atrial Fibrillation - Results
CHADS2
Score
Stroke risk this study
%/yr
Stroke risk in clinical AF study
%/yr
1 0.56 2.8
2 1.29 4.0
≥ 3 3.78 >6.4*
For subclinical atrial fibrillation:
Risk of Stroke increased with CHADs2 score
However, the risk was not as great as in studies of clinical atrial fibrillation:

Subclinical Atrial Fibrillation
Conclusions•Patients with asymptomatic subclinical atrial fibrillation identified on PPM or ICD had
– Increased risk of stroke (related to CHADs2 score but less risk than with clinical atrial fibrillation)
– Increased risk of developing clinical atrial fibrillation
Caveats:•Does not tell us whether or not these patients would benefit from anticoagulation

Subclinical Atrial Fibrillation
Clinical Implications:
•Patients who exhibit atrial tachy on quarterly pacemaker reports should:
Be followed for development of clinical atrial fibrillation
Perhaps anticoagulation should be considered in those with a CHADs@ score of 3 or greater or with episodes lasting over 17 hours(hypothesis should be tested in an RCT)
•These data could have important implications for work-up of patients with ‘cryptogenic’ stroke
Clinical Implications of Latest Trials in Antiplatelet and Anticoagulant Therapy
• Consider novel anticoagulants as an alternative to warfarin in patients with DVT/PE
• Consider use of aspirin after completing recommended course of anticoagulation in patients with DVT/PE
• Consider decreasing the frequency of INR monitoring in patients with very stable INRs
• Avoid use of dual antiplatelet therapy in patients with lacunar stroke
• Be aware of implications of subclinical atrial fibrillation in patients with PPMs, ICDs, and history of cryptogenic stroke
• Eagerly await future studies to help clarify and strengthen these recommendations

Questions & Answers
??
Recommended

















