
Hot topics
MEDIC
AL
BASIC S
CIENCE
GUIDELI
NES/REPORTS
REGIONAL
ICU
OBSTETRICS
PAEDS
ENT/MAXFAC/A
IRW
AY
RESUS/CRIT
INC
PAIN
GEN/VASC/G
YN/UROL
CARDIAC/T
HORACIC
NEURO/NIC
U
ORTHO/TRAUM
A/TRAN...
DAY SURG
0
5
10
15
20
25
30
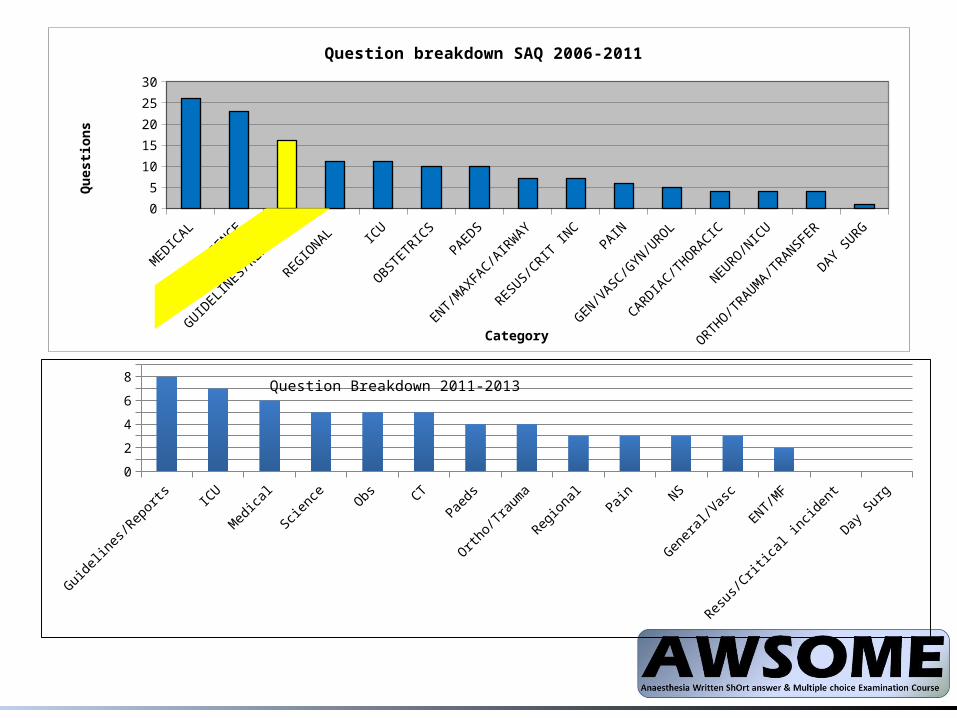
Question breakdown SAQ 2006-2011
Category
Qu
esti
on
s
Guide-lines/
Reports
ICU Medical Science Obs CT Paeds Ortho/Trauma
Regional Pain NS General/Vasc
ENT/MF Resus/Critical incident
Day Surg0
1
2
3
4
5
6
7
8
9Question Breakdown 2011-2013
Poorly answered questions Feb14
• Phaeochromocytoma• Antiplatelet therapy (CEACCP 2010)• Day case surgery in children (CEACCP 2011)• TCI Propofol• Drug errors (SALG, MHRA)• #NOF (NICE, AAGBI)
High yield resources• RCoA
– Chairman’s report– Their books– The website; 120 MCQs/30 SBAs– The Gas newsletter– The Candidate newsletter
• CEACCP• Guidelines & publications:
– SALG – AAGBI– National Audit Projects– NICE– NCEPOD
Continuing Education in Anaesthesia, Critical Care and Pain (CEACCP)
• The RCOA writes the exam and is involved in the production of CEACCP
• > 70 topics a year in CEACCP• Topical and pitched at final FRCA level• Now has podcast (as does BJA)

CEACCP 2013 – 6 topics asked from this journal
• Posterior fossa tumours• Anaesthesia for
shoulder surgery• Burns• Sympathetic blocks• Cerebral Palsy• Awareness
CEACCP 2012 – 6 topics asked from this journal
• Chemotherapy• Ultrasound• EVARs• Pulmonary Embolism• Nutrition• Head and facial injuries
POTENTIAL TOPICS
Guidelines & Reports• NICE:
– Head injury – IV fluids in hospital– AF management– Neuropathic pain– Acute Kidney Injury– Depth of anaesthesia
• NHS England– Never events
• NCEPOD– Tracheostomy care– Sepsis (in-progress)– Alcohol– Subarachnoid
haemorrhage
• National Audit Projects– 3: regional – 4: airway– 5: awareness– 6: anaphylaxis
Guidelines & Reports• NICE:
– Head injury – IV fluids in hospital– AF management– Neuropathic pain– Acute Kidney Injury– Depth of anaesthesia
• NHS England– Never events
• NCEPOD– Tracheostomy care– Sepsis (in-progress)– Alcohol– Subarachnoid
haemorrhage
• National Audit Projects– 3: regional – 4: airway– 5: awareness– 6: anaphylaxis
• AAGBI– Post anaesthetic recovery guidelines– Perioperative Care of the Elderly (esp. delirium)– Regional anaesthesia in pts with abnormal coag.– Dental damage (SALG)
• RCoA– Remote site anaesthesia– Child protection– Safe sedation– Diabetes
• AAGBI– Post anaesthetic recovery guidelines– Perioperative Care of the Elderly (esp. delirium)– Regional anaesthesia in pts with abnormal coag.– Dental damage (SALG)
• RCoA– Remote site anaesthesia– Child protection– Safe sedation– Diabetes
CEACCP- Advance Access• Iatrogenic airway injury• LA toxicity• Anaesthesia in patients with established SCI• Perioperative SVT• Placental structure, function and drug transfer• Smoke inhalation• End-of-life care• Fire safety• Tracheostomy management• Awake intubation• Inherited disorders coagulation
CEACCP- Advance Access• Iatrogenic airway injury• LA toxicity• Anaesthesia in patients with established SCI• Perioperative SVT• Placental structure, function and drug transfer• Smoke inhalation March ‘13• End-of-life care• Fire safety• Tracheostomy management March ‘14• Awake intubation• Inherited disorders coagulation
CEACCP- Advance Access• Iatrogenic airway injury• LA toxicity• Anaesthesia in patients with established SCI• Perioperative SVT• Placental structure, function and drug transfer• Smoke inhalation March ‘13• End-of-life care• Fire safety• Tracheostomy management March ‘14• Awake intubation• Inherited disorders coagulation
CEACCP- Main Journal• Major spinal surgery• Paracetamol• Rhabdomyolysis • ICU management of the morbidly obese• Chronic pain and depression• Awake craniotomy• Assessment of high risk patient• Intrathecal drug delivery• COPD and anaesthesia• Traumatic brain injury• Post op cognitive dysfunction in cardiac surgery• Acute spinal cord injury
CEACCP- Main Journal• Major spinal surgery• Paracetamol• Rhabdomyolysis • ICU management of the morbidly obese• Chronic pain and depression• Awake craniotomy• Assessment of high risk patient• Intrathecal drug delivery• COPD and anaesthesia• Traumatic brain injury• Post op cognitive dysfunction in cardiac surgery• Acute spinal cord injury

CEACCP- Main Journal• Major spinal surgery• Paracetamol• Rhabdomyolysis • ICU management of the morbidly obese• Chronic pain and depression• Awake craniotomy• Assessment of high risk patient (crossover with NELA)• Intrathecal drug delivery• COPD and anaesthesia• Traumatic brain injury (crossover with NICE)• Post op cognitive dysfunction in cardiac surgery• Acute spinal cord injury
TOPICS
Traumatic Brain Injury
• NICE guidelines, cover following:– ‘bypass’ criteria for head injury– Indication and timing of CT in ED– Cost effectiveness of strategies to image cervical
spine– Information provided to pt & relatives after
discharge
Depth of anaesthesia/Awareness
• NICE guidance recommends use of EEG-based DoA monitoring in pts at risk of:– Adverse effects of deep anaesthesia– Higher risk of awareness
• Rate of awareness probably higher than previously quoted
• NMB most implicated risk factor• MAC >0.7 considered protective• Benzos/N2O NOT protective
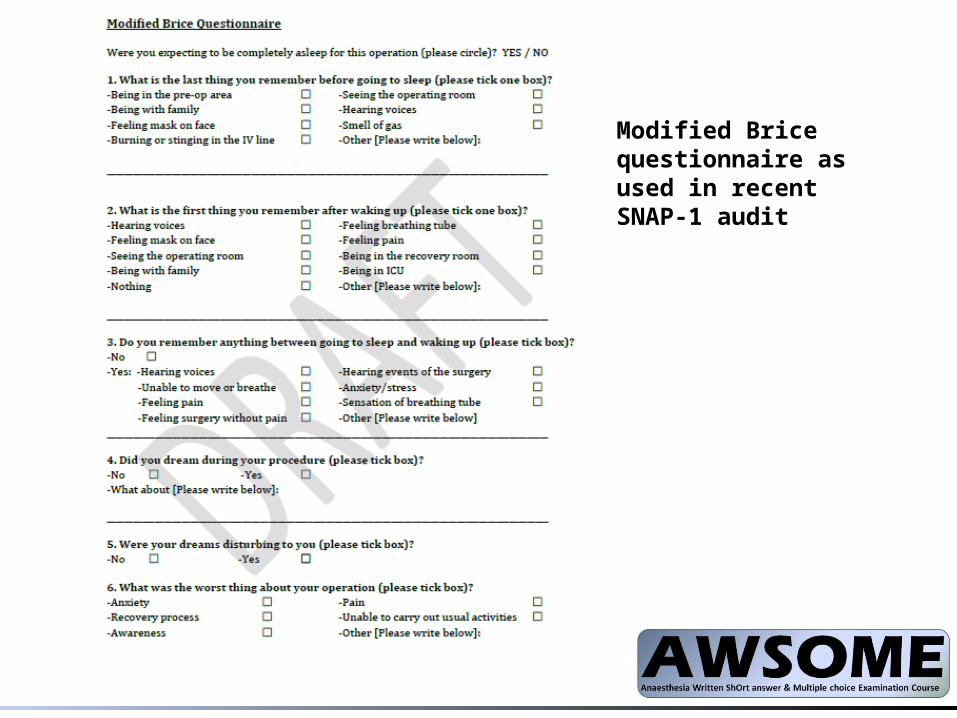
Modified Brice questionnaire as used in recent SNAP-1 audit
IV fluid therapyNICE Dec 13 (NCEPOD 1999)1. Assessment
– history, clinical examination, current medications, clinical monitoring and laboratory investigations
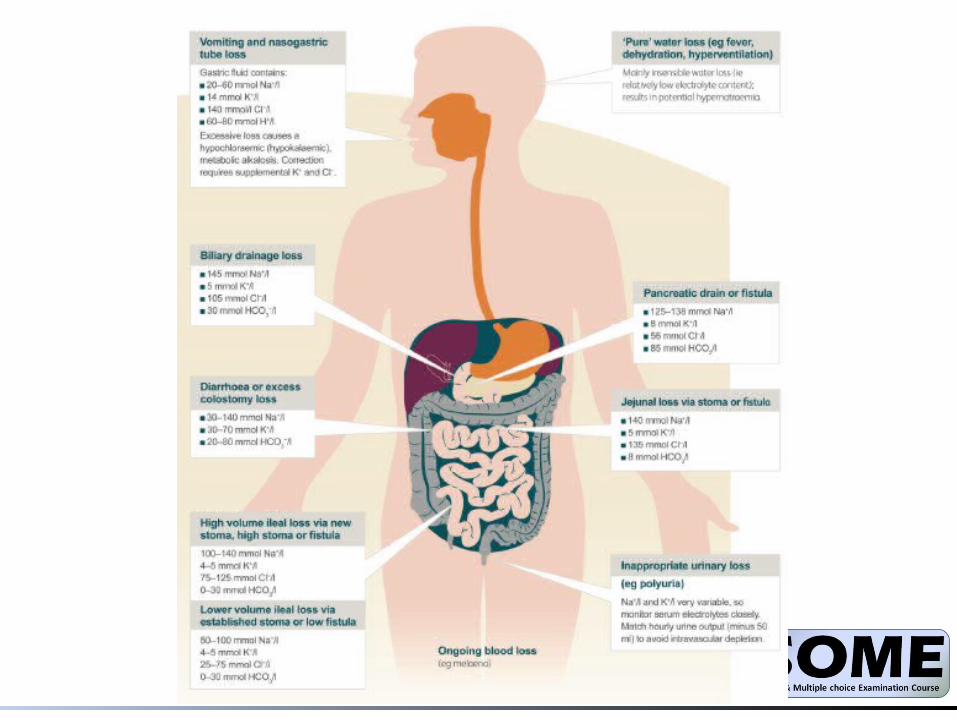
– Monitoring of urinary sodium may be helpful in patients with high-volume gastrointestinal losses
2. Routine maintenance– 25–30 ml/kg/day of water and– approximately 1 mmol/kg/day of K+, Na+ & Cl- and– approximately 50–100 g/day of glucose to limit
starvation ketosis (50g in 1l of 5% dex)
3. Fluid resuscitation– crystalloids with Na 130–154 mmol/l– bolus of 500 ml over less than 15 minutes– Do not use tetrastarch for fluid resuscitation. – Consider HAS 4–5% for fluid resuscitation only in
patients with severe sepsis
4. Replacement & redistribution– Adjust prescription to account for existing fluid
and/or electrolyte deficits or excesses, ongoing losses or abnormal distribution.
– Seek expert help if:• gross oedema• severe sepsis • hyponatraemia or hypernatraemia • renal, liver and/or cardiac impairment• post-operative fluid retention and redistribution• malnourished /refeeding
Subarachnoid haemorrhage
• NCEPOD document 2013 – “Managing the Flow”
• CEACCP article in 2013• Neurocritical Care Society issued consensus
guidelines of critical care management of aneurysmal SAH in 2011
• 85% caused by aneurysmal rupture• Other causes: AV malformations, trauma• F > M, age 40-60• Investigations:
– Non contrast CT (>95% sensitivity on day 0)– MRI– LP (after 12 hours)
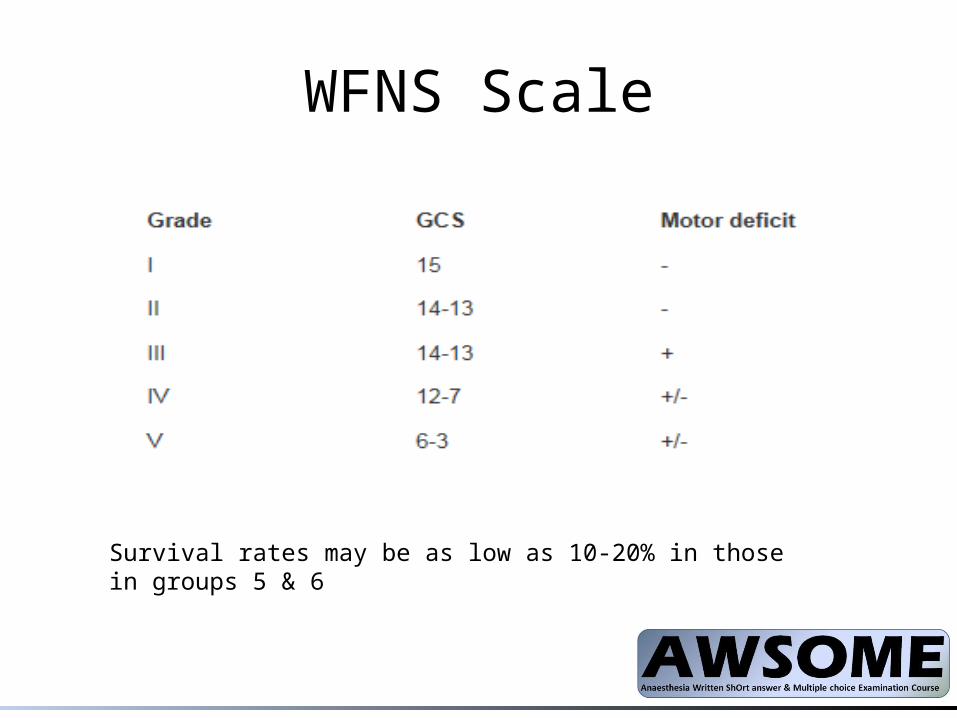
WFNS Scale
Survival rates may be as low as 10-20% in those in groups 5 & 6
Anaphylaxis
• 6th National Audit Project
• 2013 CEACCP article
• AAGBI guidelines 2009
• Allergic/non-allergic (term ‘anaphylactoid’ now obsolete)
• Previous exposure is not required in non-allergic anaphylaxis
• Atopy is a risk factor for NMBA sensitivity• Sensitization from non-anaesthetic agents
(DetergentsNMBD, Pholcodeine Suxamethonium, smoking antibiotics, fruit latex)
Investigation
• MCT – ASAP, 1-2 hours, 24 hrs or later• Skin testing 4-6 weeks (skin prick vs intradermal –
more sensitive)• Drug challenge is only way to exclude clinical allergy• Future anaesthesia –
– Written information, MDT, Alert bracelet, Yellow card, AAGBI database,
– Safe options- regional, volatiles, BZP, Remi, – Full monitoring, IV access, Pre-O 2, vasopressors ready
Emergency Laparotomy / NELA• ASGBI – Issues in Professional Practice – Emergency
General Surgery 2012• NELA – National Emergency Laparotomy Audit Dec
2012 – ongoing• Mortality in High Risk Emergency General Surgical
Admissions BJS 2013. Symons et al• Emergency surgery – Standards for unscheduled
surgical care 2011 RCS• Guidance on the provision of anaesthesia services for
emergency surgery 2013. RCoA
• Variability between trusts & between weekdays and weekends
• High 30 day mortality – 15.6%
• RCS - Dedicated team, prioritization over elective activity, audit and review, consultant lead in all specialties
• RCoA (organisational) : consultant lead at all times, equipment eg warming, cell saver, invasive monitoring, goal directed therapy (CQINN)
• Pre-op – optimization if appropriate, Formal risk assessment using eg p-POSSUM: if estimated mortality >10%-
– consultant delivered care
– post-op level 2 or 3
– Any emergency laparotomy OOH should get level 1 care
– Consultant decision making, pt centred, family communication
• Intra-op – Temp, thromboprophylaxis, antibiotics, CO monitor
• Post op – critical care/outreach/EWS
Paediatric Analgesia
• MHRA Guidance 2013 – Codeine should not be used in any child under 12
or in any child with OSA– Ultra-Fast metabolisers to morphine (genetic
variant of P450 CYP2D6) • APA guidelines re: alternative opioids in
children 2013• Alternative – Oral morphine 100mcg/kg
• MHRA : Dose greater than 75mg/kg/day constitutes an overdose requiring treatment
• APA and BNFc currently recommend 90mg/kg/day
• Summary :– in hospital up to 90mg/kg/day is fine– Out of hospital should be decreased to
75mg/kg/day (i.e 18.75mg/dose QDS)– IV paracetamol maximum doses 60mg/kg/day or
30mg/kg if <10kg.
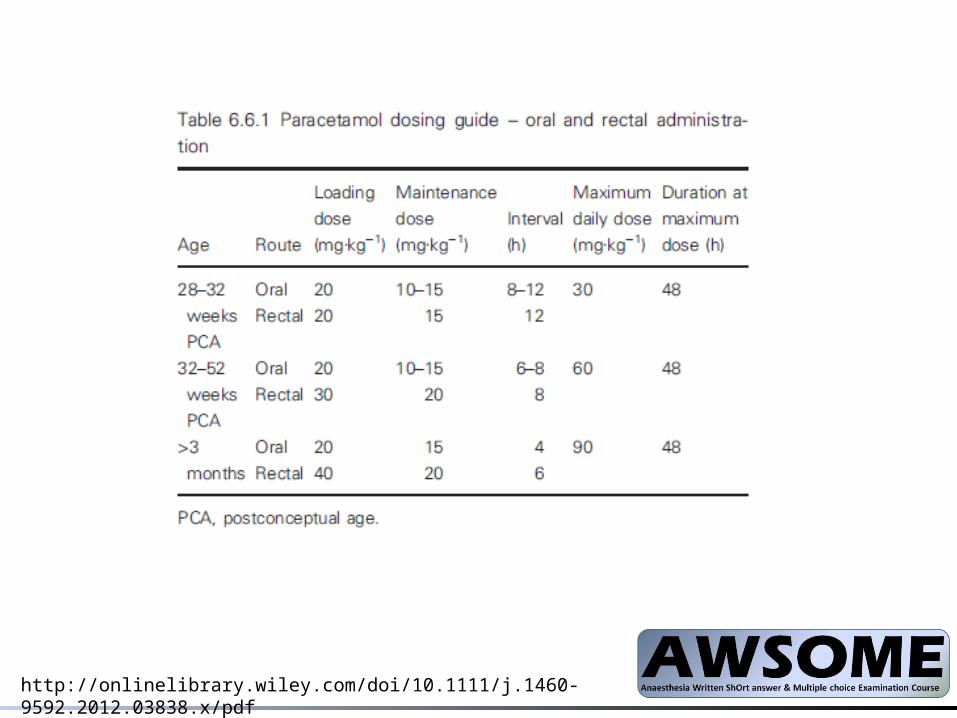
http://onlinelibrary.wiley.com/doi/10.1111/j.1460-9592.2012.03838.x/pdf
Alcohol• Sources:
– NCEPOD – Measuring the Units 2013– Anaesthesia for patients with liver disease 2010
(CEACCP)– NICE guidelines – acute upper GI bleeding June 2012.
• Poor care identified in terms of :– Fluid management– Inadequate intervention to stop bleeding– Over-sedation leading to aspiration– Failure to escalate to critical care in patients with
acute deterioration
• NICE guidance (bleeding)–Early endoscopy – all patients with ARLD who present with
bleeding should be given antibiotics and terlipressin (3/5 days) until the outcome of their endoscopy is known.
–Consider TIPSS if variceal bleeding not controlled by band ligation
• Best prognostic scores once on ICU are SOFA or acute physiology based scores rather than traditional liver scores.
RA and patients with abnormalities of coagulation
• Lists acceptable time intervals after anticoagulant drugs for RA
• Pre-eclampsia/ thrombocytopaenia: – 75-100 increased risk– >100 low risk
• Need to consider risk of block as well as pt’s coag
• Other abnomalities of coagulation “special circumstances”– Trauma– Sepsis– Massive Transfusion– Uraemia– Liver Failure– DIC
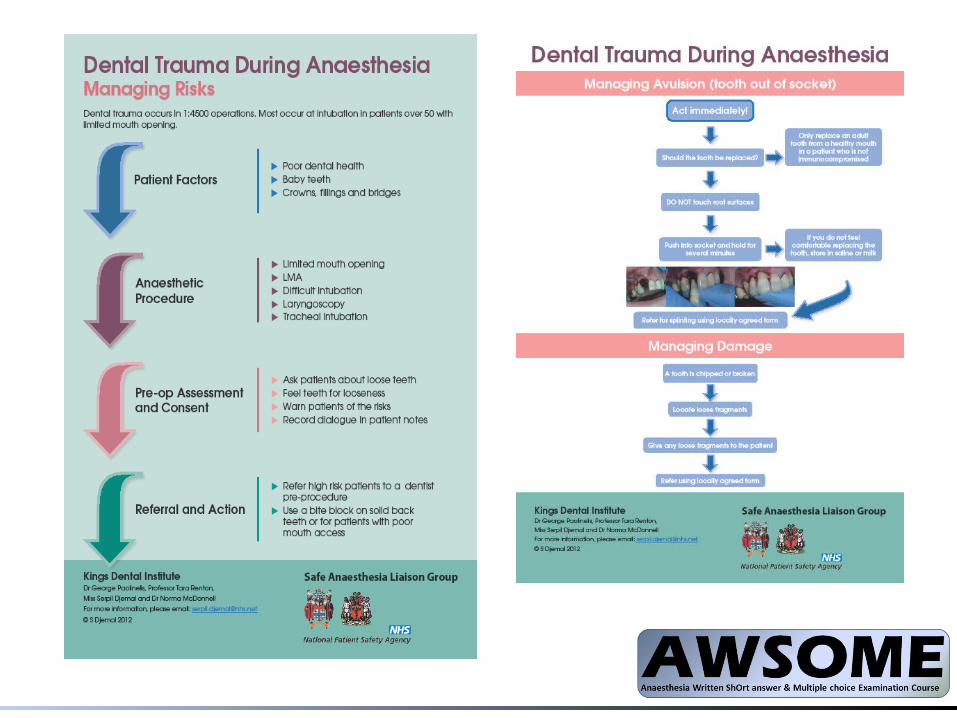
Dental damage under anaesthesia
• SALG has members from RCoA, AAGBI and NHS England (NPSA)
• Dental damage during anaesthesia guidelines issued in July 2012
• Previous SAQ (2009) poorly answered
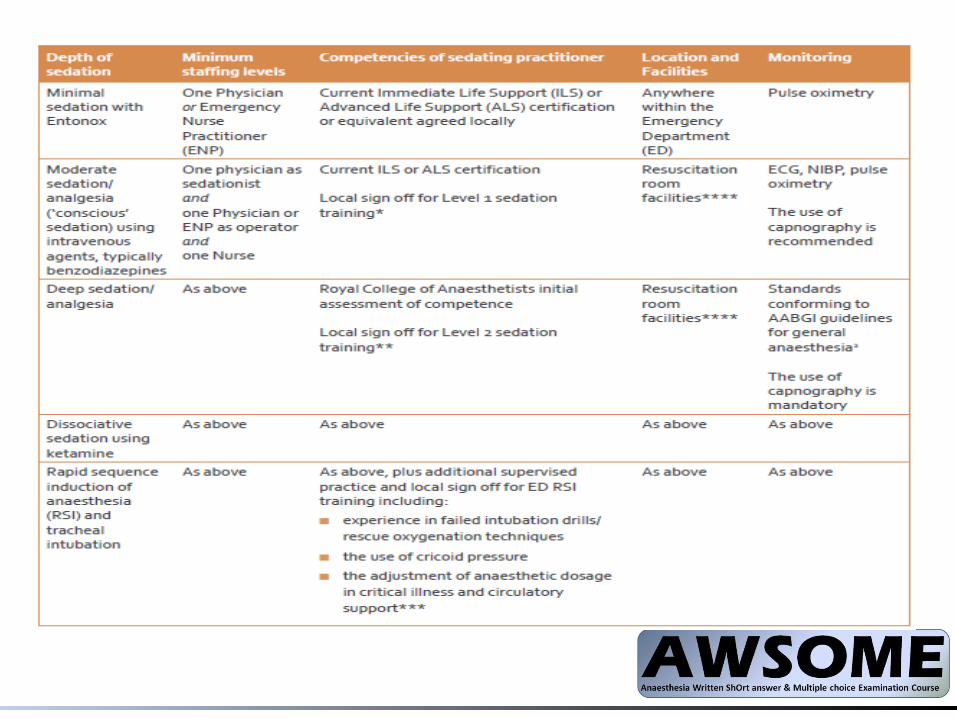
Safe Sedation
• RCoA guidance 2012– Appropriate training– Trained assistant– Define level of sedation aiming for– Oxygen, ETCO2/ AAGBI monitoring– Specific recovery monitoring– Discharge criteria
Anaesthesia in patients with SCI• Autonomic dysreflexia
– Caused by stimulation below level of lesion– Commoner in higher lesions eg above T6, and
complete (cf incomplete)– Presentations
• Inc BP >20%• Headache/flushing/sweating/chills
– Consequences• Raised ICP• Seizures• Cardiac eg MI
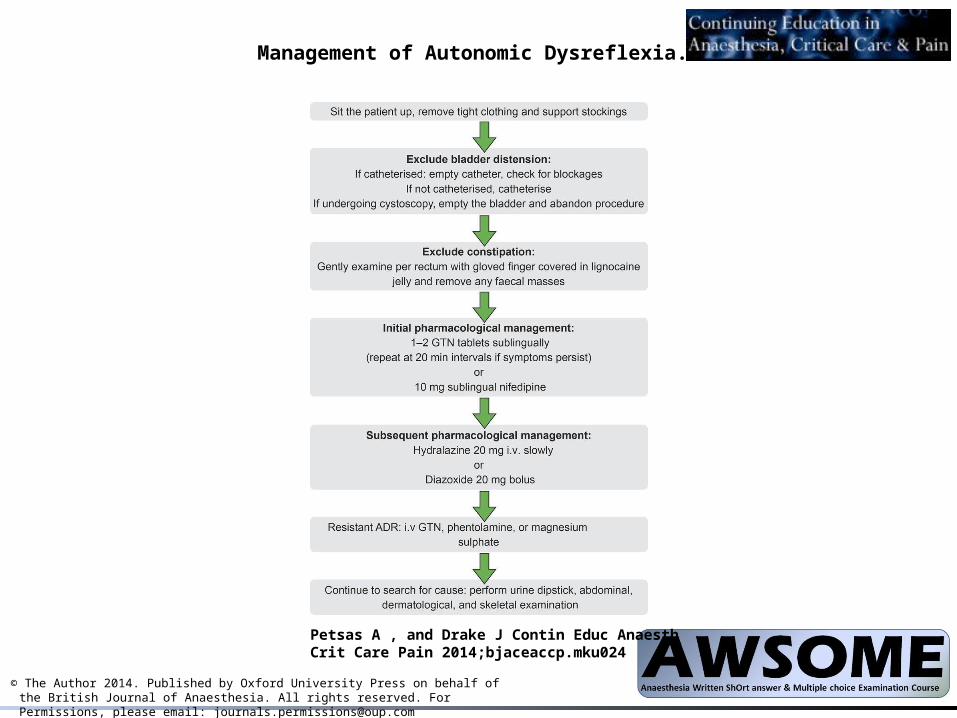
Management of Autonomic Dysreflexia.
Petsas A , and Drake J Contin Educ Anaesth Crit Care Pain 2014;bjaceaccp.mku024
© The Author 2014. Published by Oxford University Press on behalf of the British Journal of Anaesthesia. All rights reserved. For Permissions, please email: [email protected]
• Resp function– Lesions >C3 vent dependant– Lesions C3-5 variable need for vent– Lesions C6-8 may need NIV– Approx 5th of cervical SCI pts have tracheostomy
• Musculoskeletal– Spasticity (baclofen /pump)– Osteoporosis– Extrajunctional Ach receptors
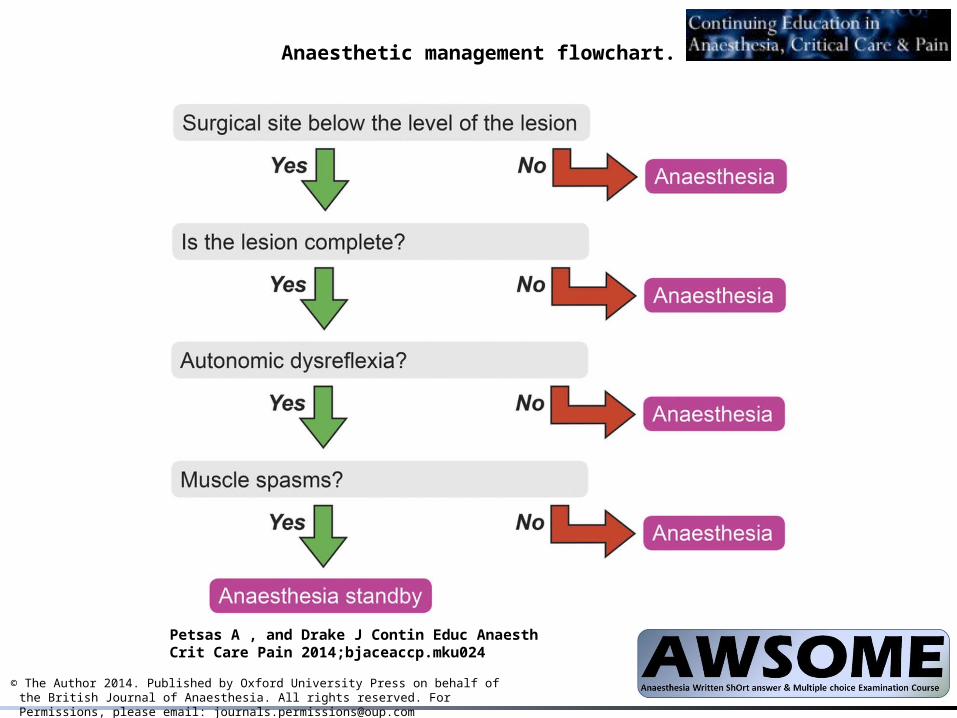
Anaesthetic management flowchart.
Petsas A , and Drake J Contin Educ Anaesth Crit Care Pain 2014;bjaceaccp.mku024
© The Author 2014. Published by Oxford University Press on behalf of the British Journal of Anaesthesia. All rights reserved. For Permissions, please email: [email protected]
Recommended

















