How to Read a CT Head
Opening Patient information; orientation; contrast vs non-contrast
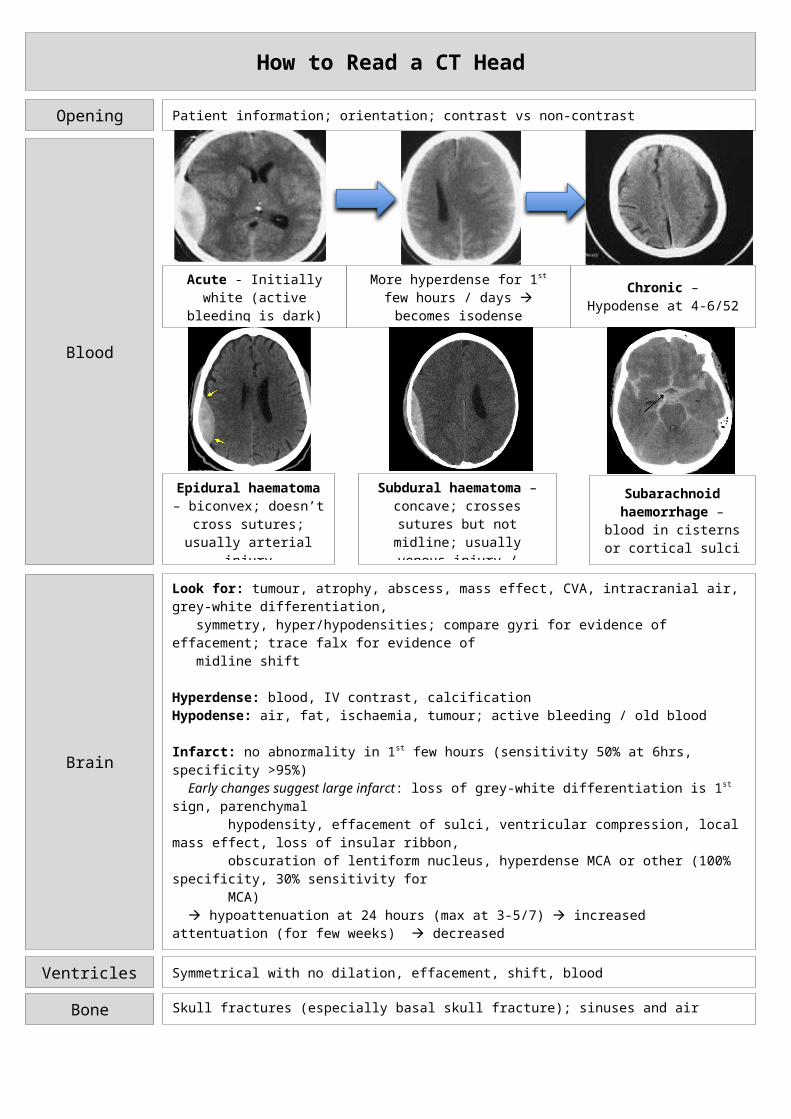
Blood
Acute - Initially white (active bleeding is dark)
More hyperdense for 1st few hours / days becomes isodense (subacute)
at 1-4/52
Chronic – Hypodense at 4-6/52
Epidural haematoma – biconvex; doesn’t cross sutures; usually arterial
injury
Subdural haematoma – concave; crosses sutures but not midline; usually venous injury /
bridging vessels
Subarachnoid haemorrhage – blood in cisterns or cortical sulci
Brain
Look for: tumour, atrophy, abscess, mass effect, CVA, intracranial air, grey-white differentiation, symmetry, hyper/hypodensities; compare gyri for evidence of effacement; trace falx for evidence of midline shift
Hyperdense: blood, IV contrast, calcificationHypodense: air, fat, ischaemia, tumour; active bleeding / old blood
Infarct: no abnormality in 1st few hours (sensitivity 50% at 6hrs, specificity >95%) Early changes suggest large infarct: loss of grey-white differentiation is 1st sign, parenchymal hypodensity, effacement of sulci, ventricular compression, local mass effect, loss of insular ribbon, obscuration of lentiform nucleus, hyperdense MCA or other (100% specificity, 30% sensitivity for MCA) hypoattenuation at 24 hours (max at 3-5/7) increased attentuation (for few weeks) decreased attenuation with mass effect and ill defined margins isodense at 1-2/52 more decreased attenuation looks like CSF at few months Poor outcome with thrombolysis if: hypodensity >1/3 MCA territory (19% fatal haemorrhage vs 0%; 7% good 3/12 outcome vs 17%), sulcal effacement, mass effect, cerebral oedema
ICH: increased attenuation in 1st week (hypodense area may be active bleeding) decreased density and blurring of margins from periphery after 1/52 surrounding oedema (may contrast enhance mimicking cancer) loss of mass effect isodense at 3/52 hypoattentuation at 10/52 little residual change
Ventricles Symmetrical with no dilation, effacement, shift, blood
Bone Skull fractures (especially basal skull fracture); sinuses and air cells
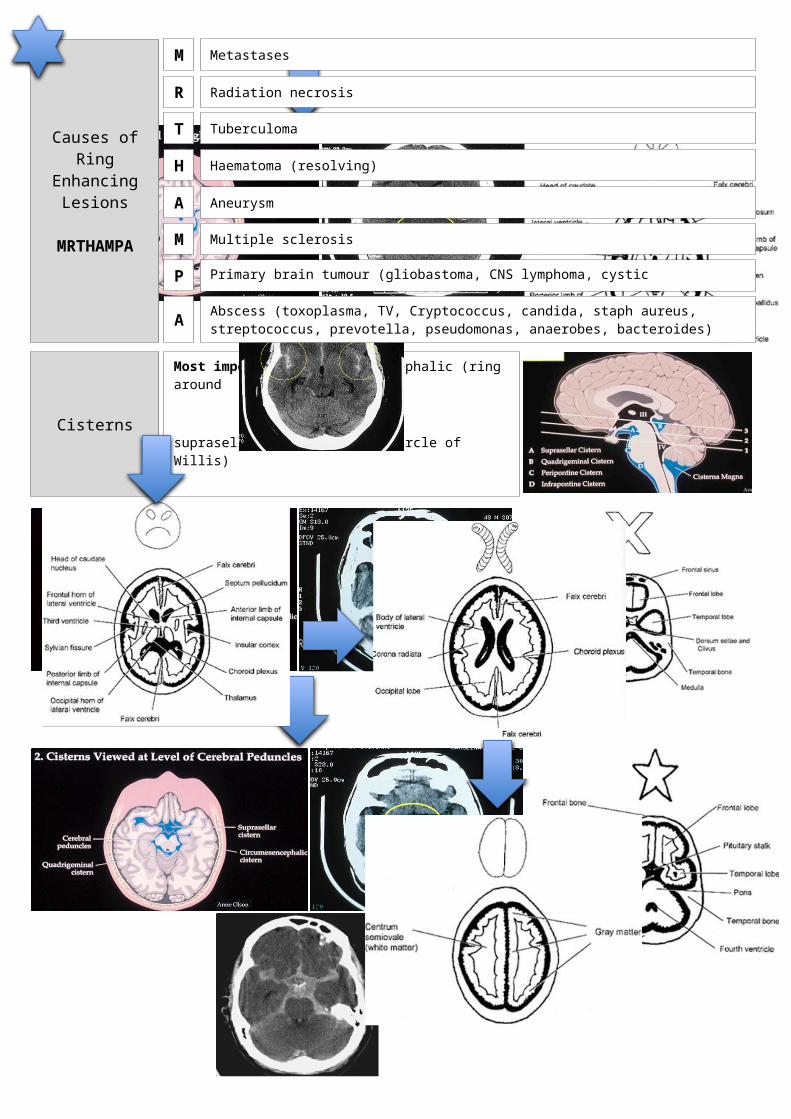
Cisterns
Most important: circummesencephalic (ring around midbrain) suprasellar (star shape at Circle of Willis) quadrigeminal (W shape – happy smile) sylvian (between temporal and frontal
lobes)
Look to see: if there’s blood, if the cisterns are open
Causes of Ring
Enhancing Lesions
MRTHAMPA
MetastasesM
R Radiation necrosis
T Tuberculoma
Haematoma (resolving)H
A Aneurysm
M Multiple sclerosis
P Primary brain tumour (gliobastoma, CNS lymphoma, cystic astrocytoma); post-op changes
A Abscess (toxoplasma, TV, Cryptococcus, candida, staph aureus, streptococcus, prevotella, pseudomonas, anaerobes, bacteroides)
Recommended

















