
LE UNITA’ DI VALUTAZIONE ALZHEIMER: DALLA COMPLESSITA’ ALLA PIANIFICAZIONE DEI PERCORSI.
UNO SGUARDO AL FUTURO.
Lamezia Terme, 16 aprile 2012
I NUOVI CRITERI DIAGNOSTICI PER LA MALATTIA DI ALZHEIMER:
PERCORSI INTEGRATI PER LA DIAGNOSI
GB Frisoni Vice Direttore Scientifico
LENITEM - Laboratorio di Neuroimmagine e UITRR - Unità per il Trasferimento della Ricerca
IRCCS Fatebenefratelli. Brescia
www.centroAlzheimer.org

The Pathophysiological Model of Alzheimer’s
Evidence of validity of the model
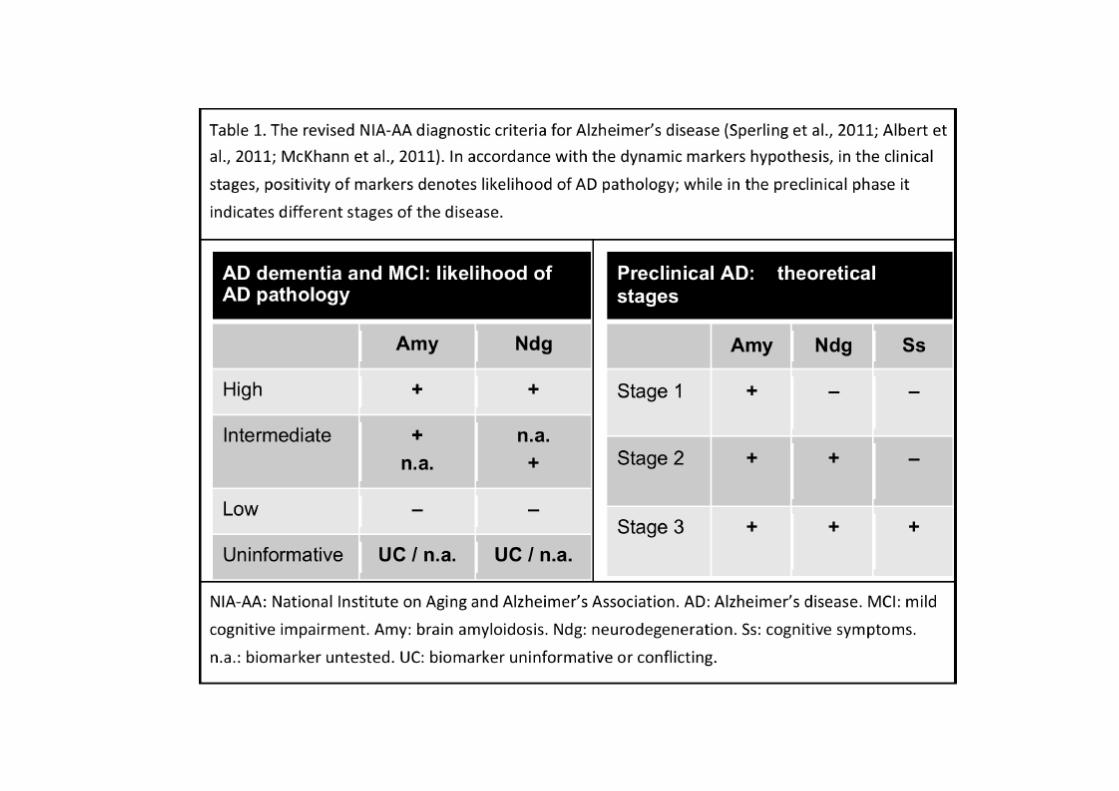
Biological markers in the context of the new diagnostic criteria
Instances of clinical application in MCI
Future challenges

The amyloid cascade from plaques to tangles, neurodegeneration, and symptoms
AMYLOID NEURODEGE-
NERATION ATROPHY SYMPTOMS PLAQUES TANGLES
Encoding episodic & spatial
memories
Encoding semantic memories ?
Smell
discrim.
Aphasia
Apraxia
Agnosia
Spared SM
and visual
functions
Braak & Braak , Courtesy of Frisoni et al., Frisoni et al., Acta Neuropath 1991 P. Giannakopoulos J Neurol 2009 J Neurol 2009

THE DYNAMIC MARKER HYPOTHESIS
Amyloidosis- and Neurodegeneration-associated markers change over time in a stereotyped fashion
Markers of amyloid
deposition
Markers of cortical
Entorhinal hypometabolism Cortex atrophy & synaptic
dysfunction Hippocampal
& post cing. atrophy
Temporal
Neocortex atrophy
Whole brain atrophy
-20 -15 -10 -5 0 5 10 15 20
Years from AD diag..

The Pathophysiological Model of Alzheimer’s
Evidence of validity of the model
Biological markers in the context of the new diagnostic criteria
Instances of clinical application in MCI
Future challenges

The course of atrophy is non linear…
Frisoni et al., J Neurol 2009 6
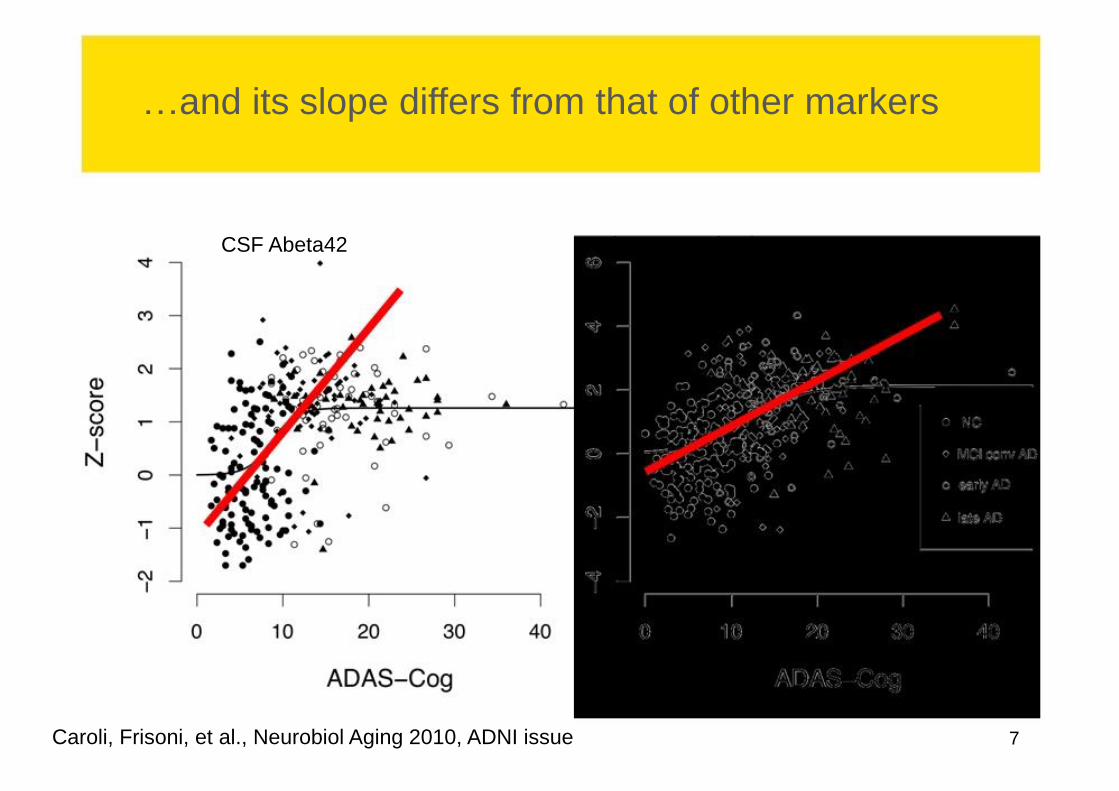
…and its slope differs from that of other markers
CSF Abeta42 Hippocampal volume
Caroli, Frisoni, et al., Neurobiol Aging 2010, ADNI issue 7

Up stream
AMYLOID NEURODEGENERATION TANGLES ATROPHY SYMPTOMS
PLAQUES
Down stream
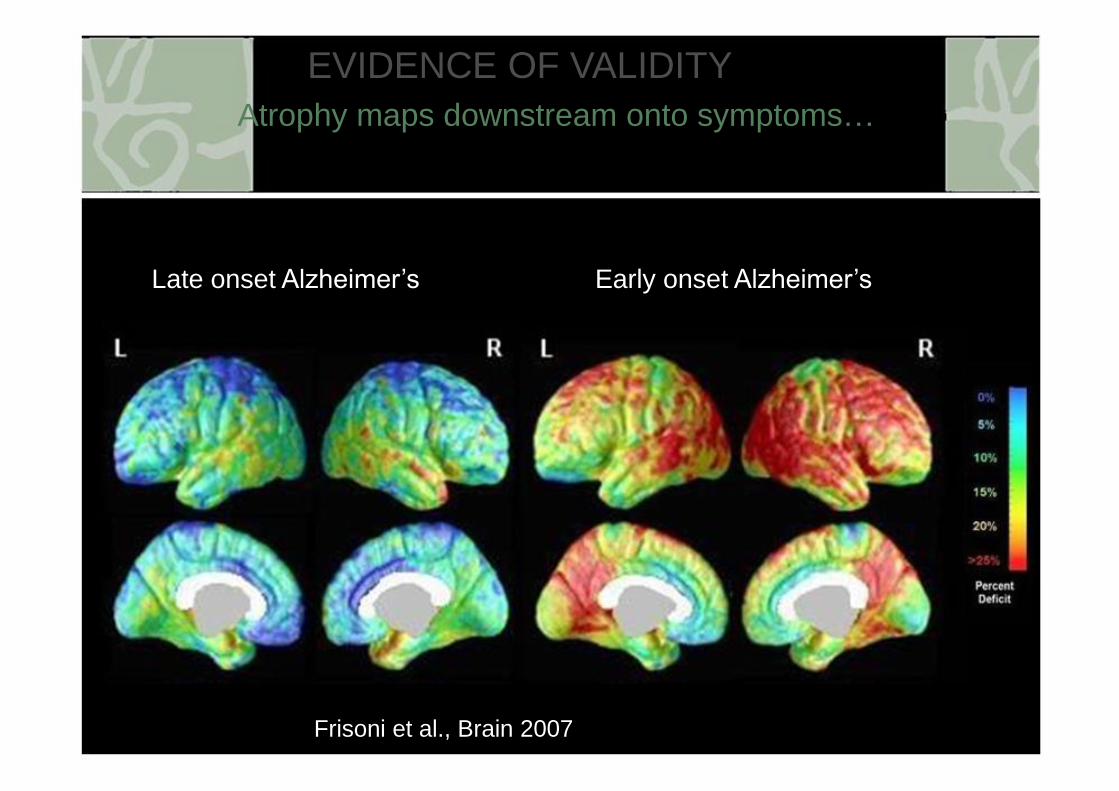
EVIDENCE OF VALIDITY
Atrophy maps downstream onto symptoms…
Late onset Alzheimer’s Early onset Alzheimer’s
Frisoni et al., Brain 2007 9
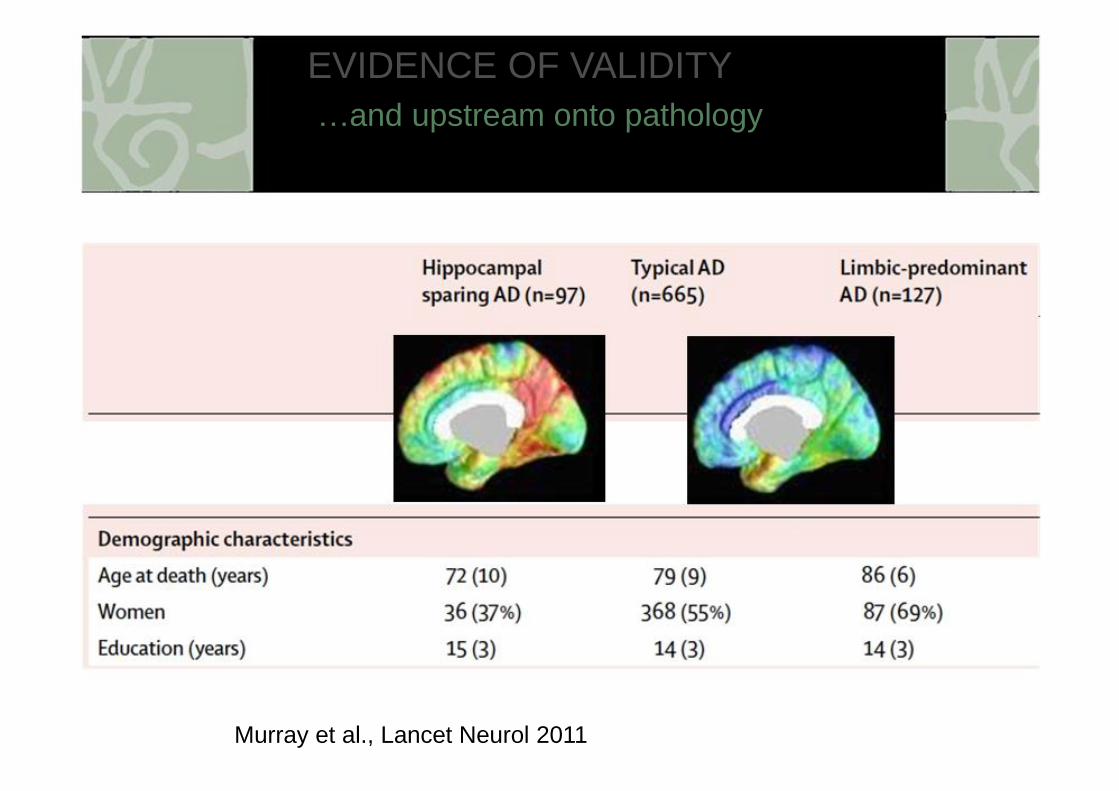
EVIDENCE OF VALIDITY
…and upstream onto pathology
Murray et al., Lancet Neurol 2011

Amyloid markers predict dementia and cognitive deterioration in healthy elderly persons
N Desig F-U Pre- Outcome Associa- n dictor tion
Skoog et al., DGCD 35 Popu- 3 yrs Ab42 Dementia OR 8.2 2003 lation
Hansson et al., 53 Volunt 4-6 Ab42 Conversion to Sens 91% Lancet Neurol 2006 eers yrs MCI Spec 81%
Stomrud et al. 57 Volun- 3 Ab42 Subj mem imp + Sens 71% DGCD 2007 teers +tau decreased QoL Spec 76%
Gustafson et al., 55 Popu- 10 yrs Ab42 MMSE -5 pts OR 2.2 JNNP 2007 lation or dementia ♀
Fagan et al., Arch 61 Popu- 1-8 Tau/ CDR 0 gg 0.5+ OR 5.2 Neurol 2007 lation yrs Ab42
Li et al., Neurology 129 Volun- 42 Tau/ Conversion to OR 4.5 2007 teers mos Ab42 MCI

EVIDENZA DI VALIDITA’ DEL MODELLO FISIOPATOLGICO
Specificity to AD of cortical atrophy pattern

The Pathophysiological Model of Alzheimer’s
Evidence of validity of the model
Biological markers in the context of the new diagnostic criteria
Instances of clinical application in MCI
Future challenges


EVIDENZA DI VALIDITA’ DEL MODELLO FISIOPATOLGICO
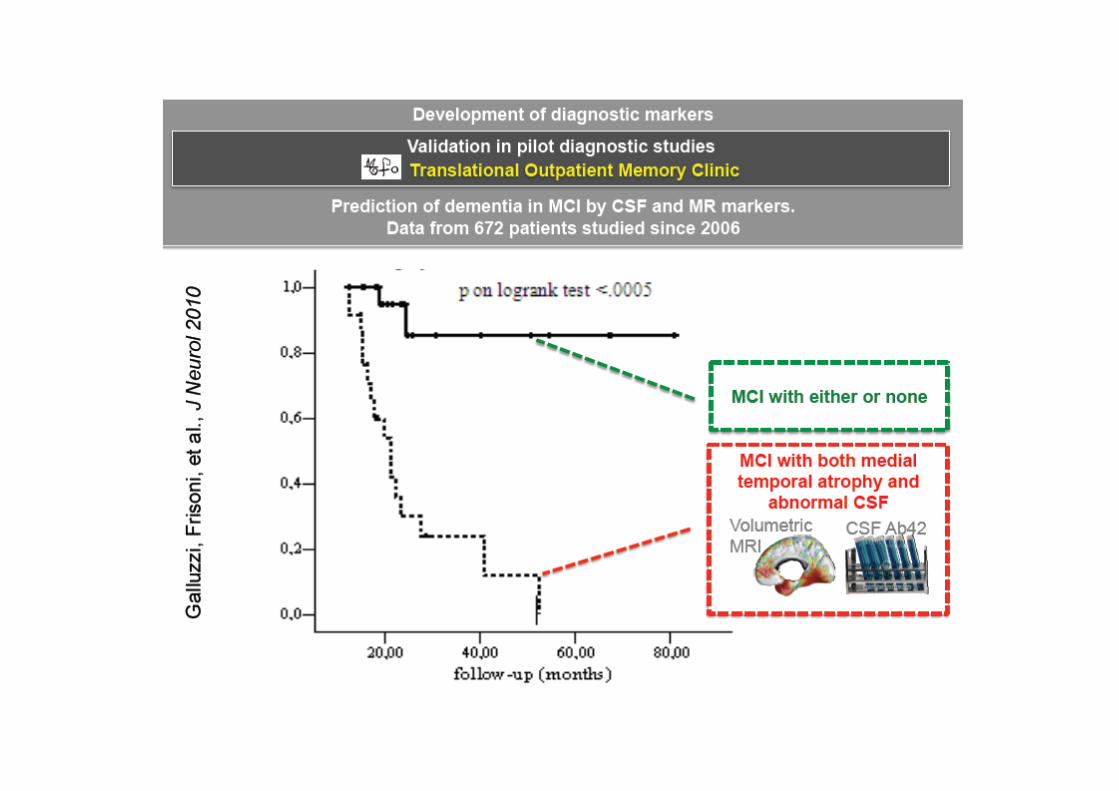
Marker combination predicts dementia in MCI
587 persons with no
cognitive impairment @ baseline
211 persons with MCI
@ baseline
Bennett et al., Neurology 2002;59:198-205

EVIDENZA DI VALIDITA’ DEL MODELLO FISIOPATOLGICO
Marker combination predicts dementia in MCI
MCI-NC MCI-AD p
n=51 n=24
Age 70.9+7.1 72.2+7.1 .57
Sex (female) 28 (55%) 17 (71%) .38
Education 7.7+3.6 8.8+4.6 .39
MMSE 26.3+1.9 26.4+1.6 .24


In vivo β amyloid imaging with PET


The Pathophysiological Model of Alzheimer’s
Evidence of validity of the model
Biological markers in the context of the new diagnostic criteria
Instances of clinical application in MCI
Future challenges

Patient R.F.
Clinical & demograph. features
● Age 78, educ 13, onset 6 mos ● Lives alone, no relatives ● MMSE 29/30
● Fails ONLY 1 memory test ● Fully functional in daily life
● Asks whether she has Alzheimer`s
Frisoni et al., Alzheimer Dis Assoc Disord. 2010;24:108-14. Porteri et al., Can J Neurol Sci. 2010;37:67-75

Patient F.C.
Clinical & demograph. features
● Age 75, educ 18, onset 18 mos ● Lives alone, 1+1 daughters ● MMSE 29/30
● Poor performance ONLY in memory tests
● Fully functional in daily life
● Daughters ask whether she has Alzheimer`s to arrange future care
Frisoni et al., Alzheimer Dis Assoc Disord. 2010;24:108-14. Porteri et al., Can J Neurol Sci. 2010;37:67-75

Pazienti RF e FC La biologia
RF FC
Cognitività MMSE 29/30 29/30
CDR 0.5 0.5
Disabilità IADL, funz perse 0/8 0/8
Barthel 100/100 100/100
consapevolezza GRAD 4/4 4/4
(piena consapevol.) (piena consapevol.)
CIRS 0/8 0/8
(piena consapevol.) (piena consapevol.)
Umore Depressione (BSI) 0.33/4 0.33/4
(assente) (assente)
Ansia (BSI) 0.04/4 0.33/4
(assente) (assente)
Frisoni et al., Alzheimer Dis Assoc Disord. 2010;24:108-14. Porteri et al., Can J Neurol Sci. 2010;37:67-75

RF FC
Raw Perc. Raw Perc.
LEARNING
3 objects 3 places (Prestia 2006) 8/9 -- 7/9 --
Logical memory (Spinnler 1987) 1.5/28 <5th 15.5/28 >50th
Rey figure del. recall (Caffarra 2002) 8.5/36 10-25th 8/36 25-50th
SHORT TERM MEMORY
Digit span 5 25-50th 6 >50th
Spatial span (Spinnler 1987) 4 10-25th 4 10-25th
LANGUAGE
Token test (Spinnler 1987) 30/36 10-25th 33/36 >50th
Letter fluency (Novelli 1986) 27/3 min 25-50th 26/3 min 25-50th
Semantic fluency (Spinnler 1987) 22/3 min 10-25th 24/3 min <10th
VISUO-SPATIAL ABILITIES
Rey figure copy (Caffarra 2002) 34/36 >50th 28/36 <10th
FRONTAL/EXEC
Raven's coloured PM (O.S. 1985) 26/36 25-50th 33/36 >50th
TMT B-A (Giovagnoli, 1996) 132 sec 10-25th 40 sec >50th
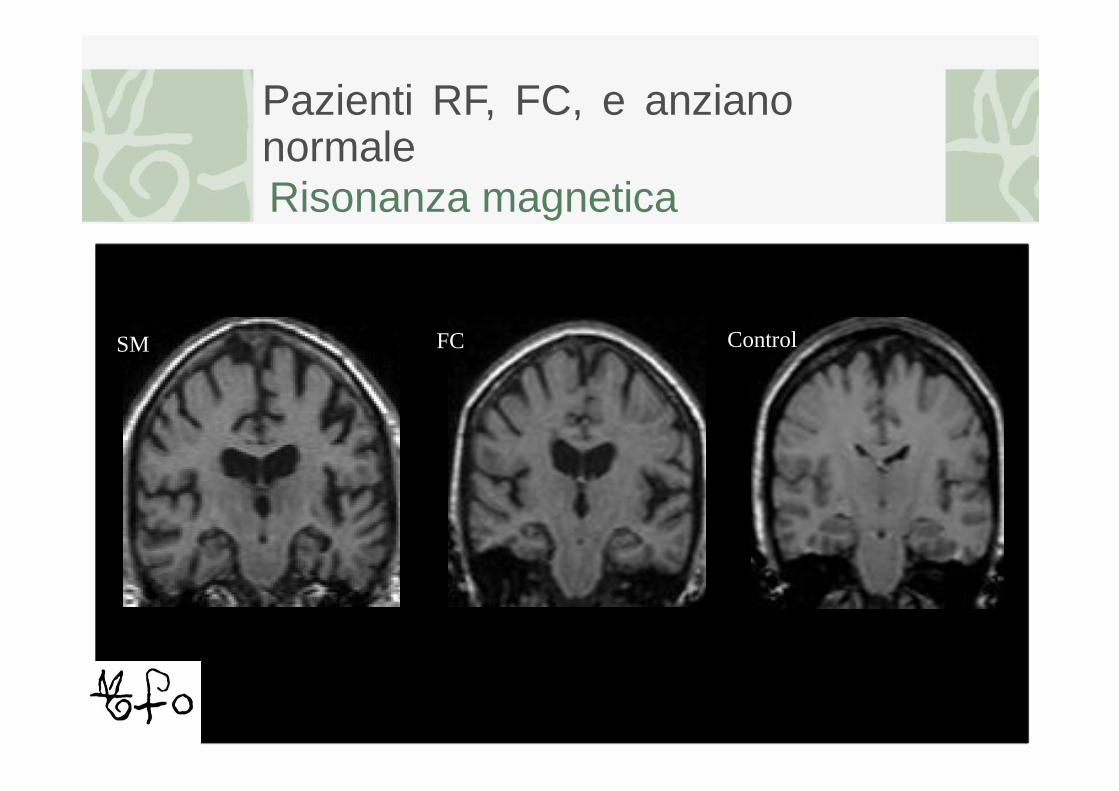
Pazienti RF, FC, e anziano normale
Risonanza magnetica
FC Control SM

Pazienti RF, FC, e anziano normale
Volumetria ippocampale
4.000 4.000
3.500 3.500
3.000 3.000
2.500 2.500
2.000 2.000
RF
FC 1.500 1.500
20,00 40,00 60,00 80,00 100,00 20,00 40,00 60,00 80,00 100,00
Le linee rappresentano i percentili: 1°, 5°, 25°, 50°, 75°, 95°, 99°

Pazienti RF e FC Metabolismo cerebrale con FDG PET"
SM FC
Frisoni et al., Alzheimer Dis Assoc Disord. 2010;24:108-14. Porteri et al., Can J Neurol Sci. 2010;37:67-75

Pazienti RF e FC
Profilo liquorale 750
700
650
600 FC 550 SM
500
450
400
350
300
250
200
150
100
50
0
200 250 300 350 400 450 500 550 600 650 700 750 800 850
Abeta 42 (pg/ml)
Frisoni et al., Alzheimer Dis Assoc Disord. 2010;24:108-14. Porteri et al., Can J Neurol Sci. 2010;37:67-75
Pazienti RF e FC La comunicazione
• R.F.: lQualche segno di invecchiamento cerebrale
accelerato, potrebbe diventare Alzheimer, ma non
sappiamo quandoz. Terapia: donepezil 10 mg.
Rivalutazioni cliniche e npsy semestrali •
F.C.:
Paziente: lQualche segno di invecchiamento
cerebrale accelerato, facciamo cura per cercare
di arrestare la progressione, poi ci si rivedez.
Familiari: lQuasi certezza che si tratti di
Alzheimer, peggiorerà nel giro di mesi/
pochissimu anni, terapia solo sintomatica,
decorso disabilitante in 10 anni circaz. Terapia
donepezil 10 mg.
ETHICS
Related to clinical issues
• Was it justified to answer patient`s and
relatives` requests for early diagnosis? •
Was it justified to diagnose an almost
asymptomatic disease when therapy is
poorly effective?
• What should have patients been told?
Whole truth or almost so?
• Should have relatives been told
anything at all?

Cognitività dopo 1 anno I numeri indicano la variazione % rispetto alla prima valutazione clinica
VISUO- FRONTAL- LEARNING WORKING
20 SPATIAL EXECUTIVE MEMORY LANGUAGE
0
-20
SM -40
FC
-60
-80
-100

The Pathophysiological Model of Alzheimer’s
Evidence of validity of the model
Biological markers in the context of the new diagnostic criteria
Instances of clinical application in MCI
Future challenges

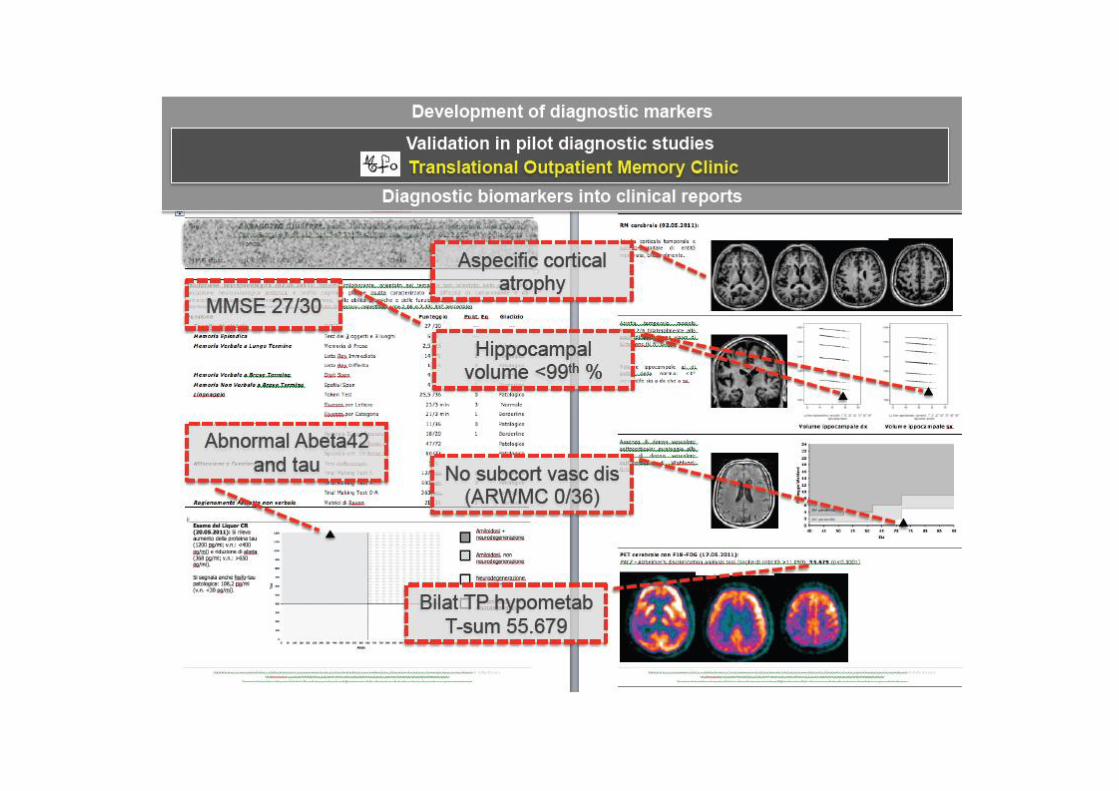
Development of diagnostic markers
Validation in pilot diagnostic studies
Translational Outpatient Memory Clinic
PATIENTS: MCIs, demented with uncertain features
CLINICAL DATA COLLECTION Clinical and Drug History, Neurol exam, Cogn & Mood screen (MMSE, BSI)
MARKER COLLECTION
HIGH RESOLUTION NEUROPSYCHOL 18F-FDG PET LUMBAR TAP
MR TESTING
PROCESSING OF DATA/MARKERS
Hppocampal volume T-sum for TP Age- and educ-
Subcortical micro- Abeta42, tau, p-tau hypometabolism corrected scores
vascular damage scale
DIAGNOSTIC REPORT to physician-in-charge
Frisoni et al., Alzheimer Dementia 2009

Development of diagnostic markers
Development of Standard Operating Procedures for Biomarker Assessment
Modality Measurement
Hippocampal 3D T1 MR
volume
Temporo- parietal FDG PET
hypometabolism
CSF Ab42 and Lumbar tau puncture
Cortical amyloid Amyloid SOPs developed by ligand manufacturers
deposition PET

NEXT STEPS TOWARDS TRANSLATION
Challenges to translation

NEXT STEPS TOWARDS TRANSLATION
Challenges to translation
1. Clinical factors: evidence on efficacy of combined
markers, SOPs, normative population and abnormality
thresholds, estimates of biomarker predictivity 2.
Health-care organization-related factors: primary
secondary tertiary care, panel/stand alone biomarkers;
3. Reimbursement-related factors 4. Market-related factors
5. Incremental diagnostic value
6. Cost/benefit ratio: cost/risk/feasibility/invasiveness 7. Patient/caregiver preferences: “wish to know”
NEXT STEPS TOWARDS TRANSLATION
Challenges to translation: understanding patient needs and wishes
CONCLUSIONI
La sequenza di eventi nella malattia di Alzheimer comprende deposizione di amiloide, neurodegenerazione e sintomi.
I biomarcatori diventano anomali secondo una sequenza precisa: prima di amiloidosi, poi funzionali, metabolici, strutturali, e infine cognitivi.
L’atrofia mappa a monte sulla
neurodegenerazione e a valle sui sintomi.
I marcatori di amiloidosi e di
neurodegenerazione permettono di riconoscere i pazienti MCI con neuropatologia Alzheimer.
Per essere utilizzati su larga scala, i biomarcatori devono essere standardizzati.
Recommended

















