Francesco Paolo Russo
Department of Surgery, Oncology and Gastroenterology Multivisceral/ Gastroenterology Section
University Hospital Padova
IL TRAPIANTO DI FEGATO: QUALE FUTURO CON LE NUOVE TERAPIE PER LE
MALATTIE EPATICHE?
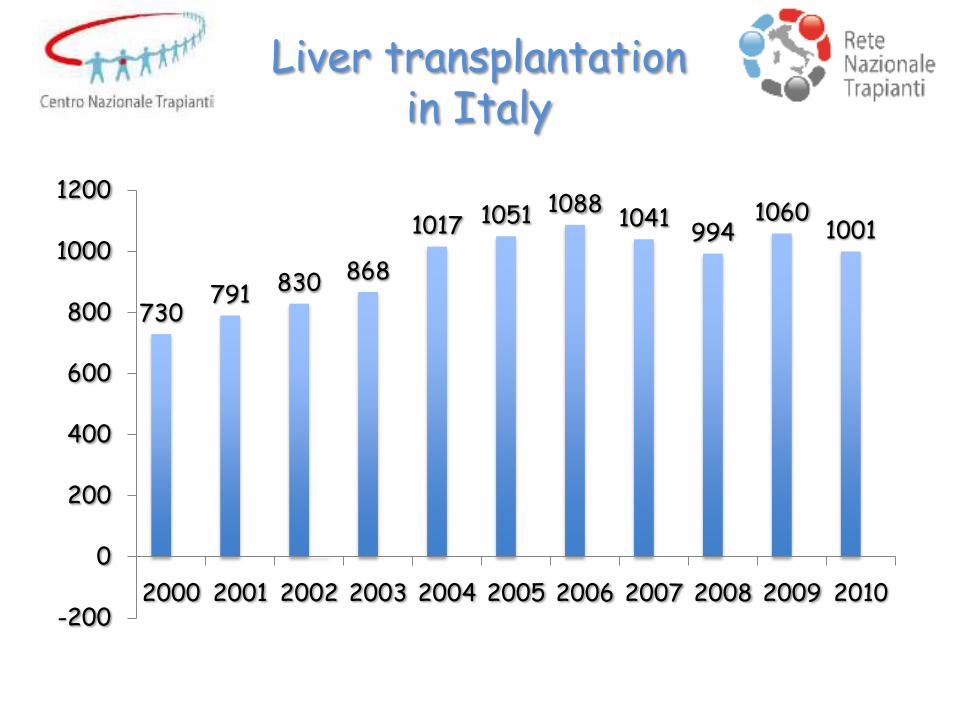
730 791 830 868
1017 1051 1088 1041
994 1060
1001
-200
0
200
400
600
800
1000
1200
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010
Liver transplantation in Italy
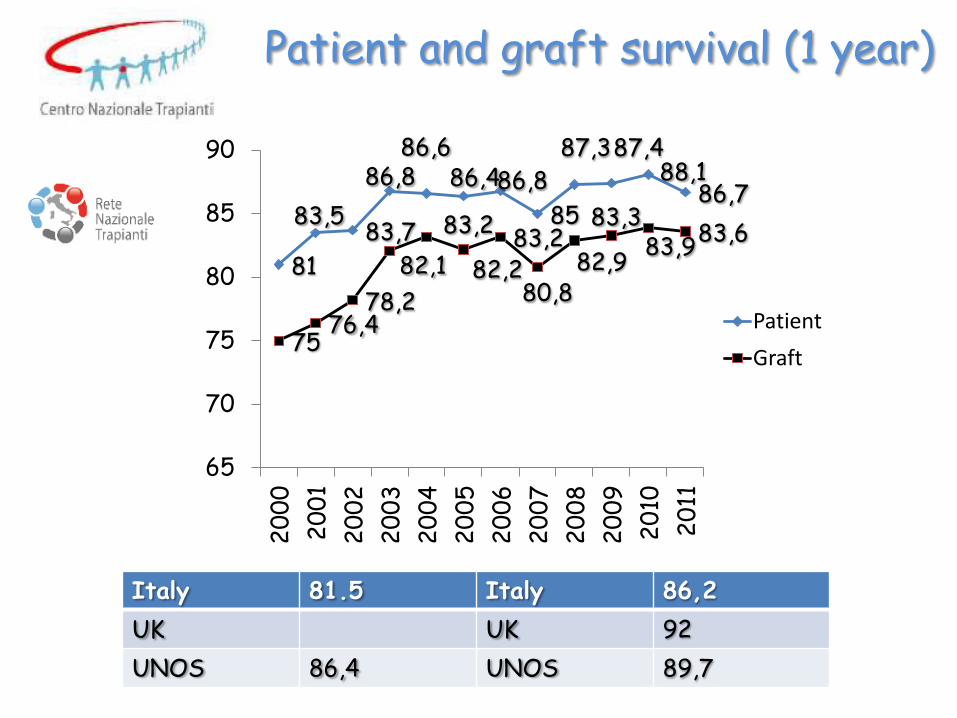
81
83,5 83,7
86,8 86,6
86,4 86,8
85
87,3 87,4 88,1
86,7
75 76,4
78,2
82,1
83,2
82,2 83,2
80,8 82,9
83,3 83,9
83,6
65
70
75
80
85
90
20
00
20
01
20
02
20
03
20
04
20
05
20
06
20
07
20
08
20
09
20
10
20
11
Patient
Graft
Italy 81.5 Italy 86,2
UK UK 92
UNOS 86,4 UNOS 89,7
Patient and graft survival (1 year)
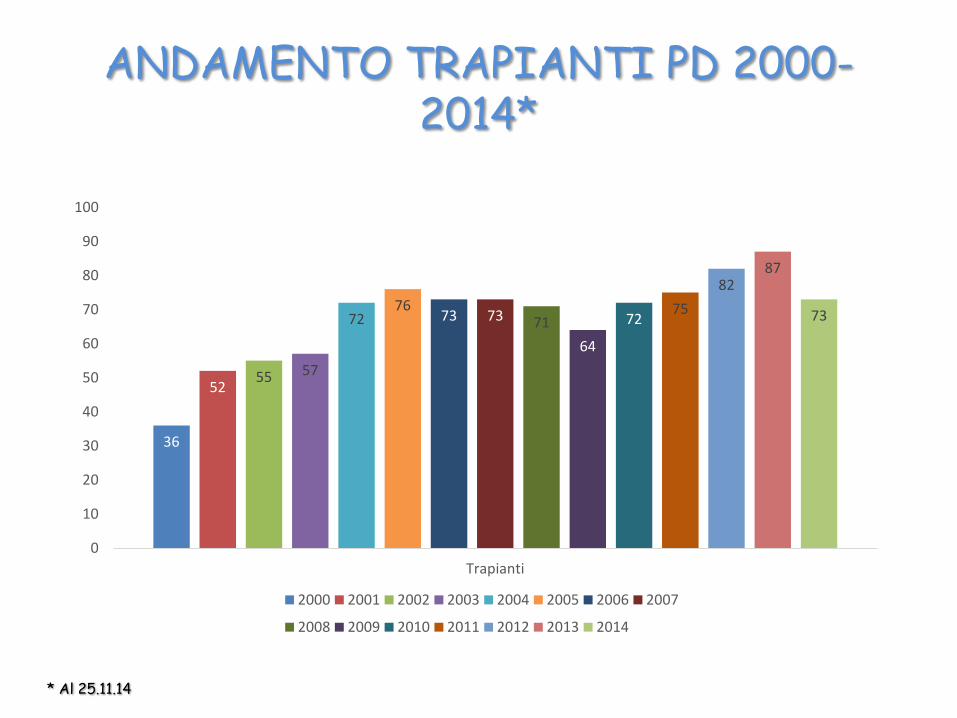
ANDAMENTO TRAPIANTI PD 2000-2014*
36
52 55 57
72 76
73 73 71
64
72 75
82 87
73
0
10
20
30
40
50
60
70
80
90
100
Trapianti
2000 2001 2002 2003 2004 2005 2006 2007
2008 2009 2010 2011 2012 2013 2014
* Al 25.11.14
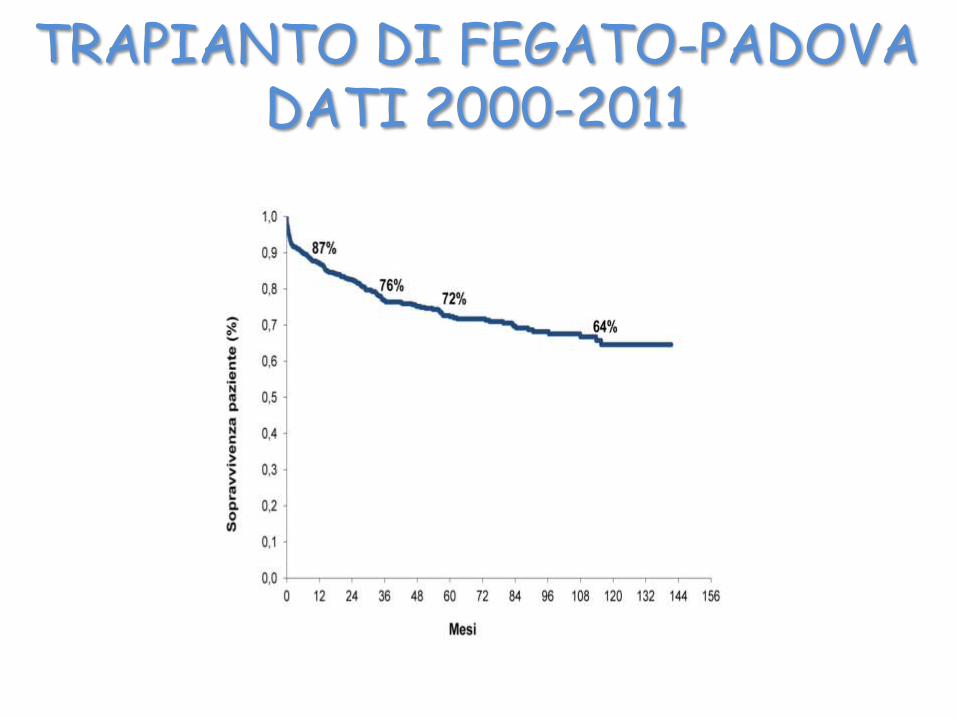
TRAPIANTO DI FEGATO-PADOVA DATI 2000-2011
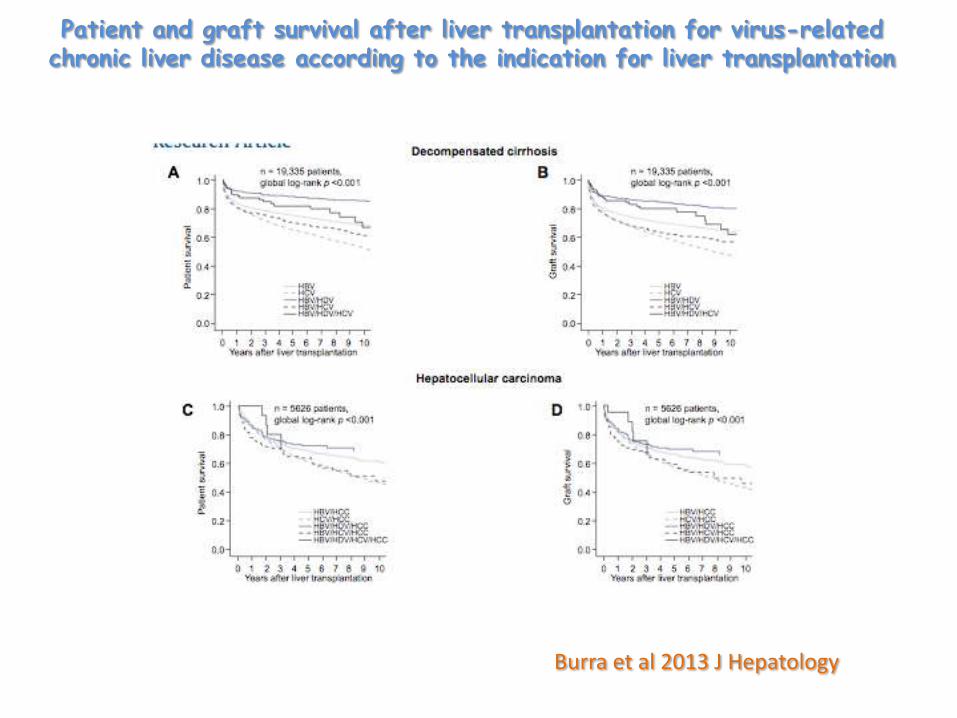
Patient and graft survival after liver transplantation for virus-related chronic liver disease according to the indication for liver transplantation
Burra et al 2013 J Hepatology
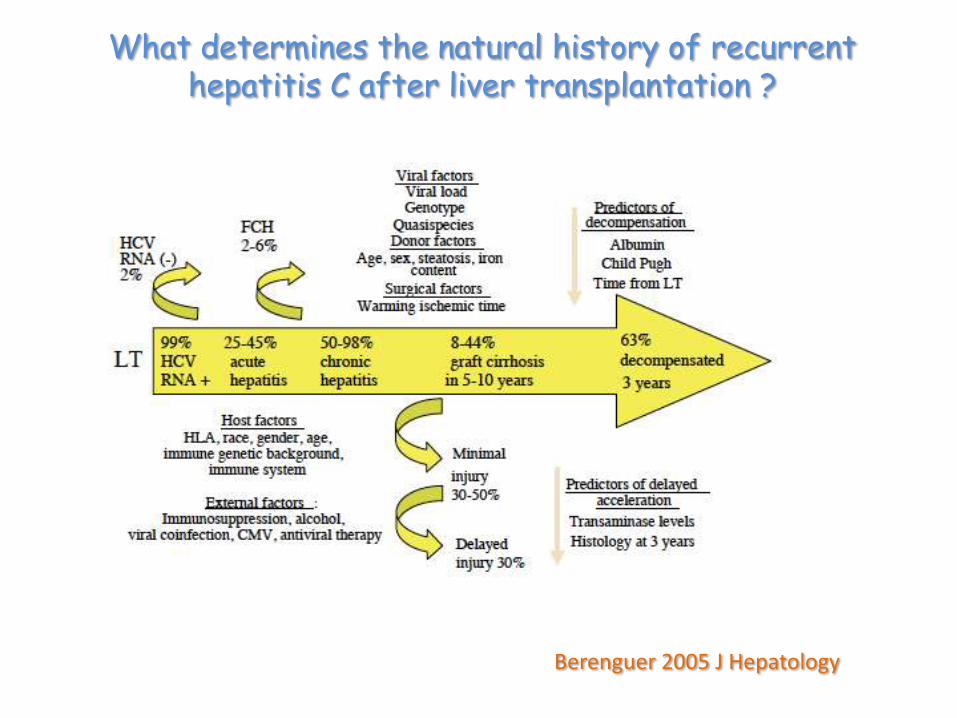
What determines the natural history of recurrent hepatitis C after liver transplantation ?
Berenguer 2005 J Hepatology

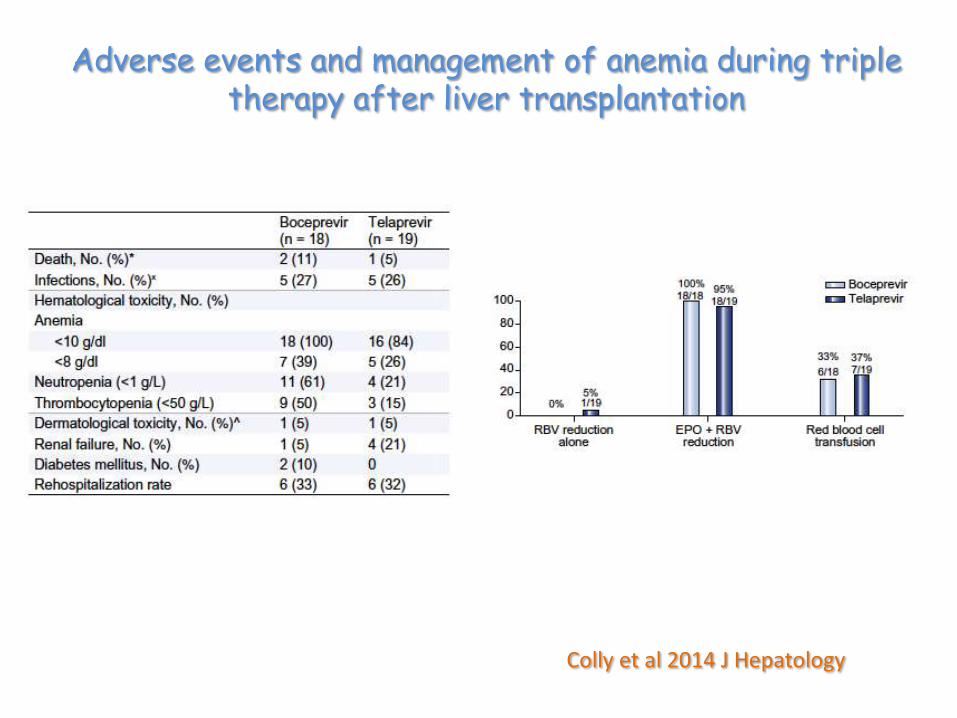
Colly et al 2014 J Hepatology
Adverse events and management of anemia during triple therapy after liver transplantation
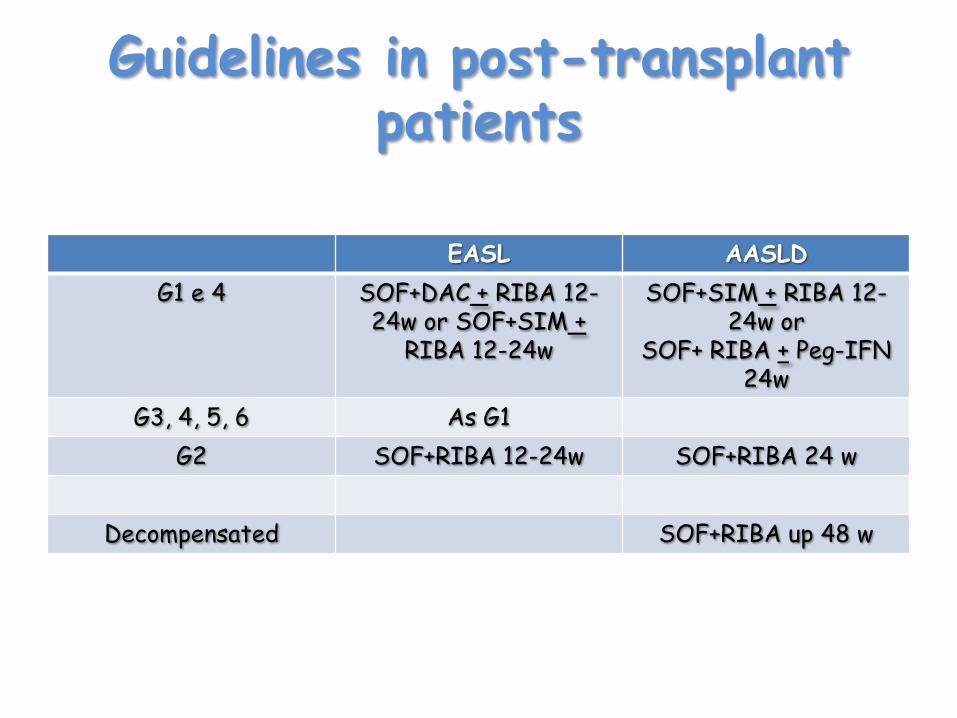
Guidelines in post-transplant patients
EASL AASLD
G1 e 4 SOF+DAC + RIBA 12-24w or SOF+SIM +
RIBA 12-24w
SOF+SIM + RIBA 12-24w or
SOF+ RIBA + Peg-IFN 24w
G3, 4, 5, 6 As G1
G2 SOF+RIBA 12-24w SOF+RIBA 24 w
Decompensated SOF+RIBA up 48 w
• Positives – Higher response rates → more cures – SVR rates similar to non transplantation
patients
• Negatives – Greater adverse effects, requiring high
intensity of monitoring – Significant DDIs with CNIs/mTORi → kidney
toxicity, rejection risk – Limited eligibility for treatment
First-Generation PI Triple Therapy in Transplantation Recipients
Opportunities and Challenges Prior to Transplant
• We now have pre-OLT therapy that can prevent reinfection of graft
• No dose adjustment of SOF required
• Anemia with RBV more problematic in more advanced liver disease
• Data thus far only in Childs A/B with CTP 7, MELD < 22, HCC within Milan criteria
– Unknown: MELD > 22, CTP > 7
• Duration of therapy 24-48 wks can make timing of transplant difficult for some centers
– SVR (SOF/SIM) may be a more cost-effective goal than suppression (SOF/RBV)
– Elimination of RBV also more effective
• Additional data required in those with more advanced disease
– Ascites and encephalopathy may improve
Kwo Clinical Care Options

Pre-Transplant
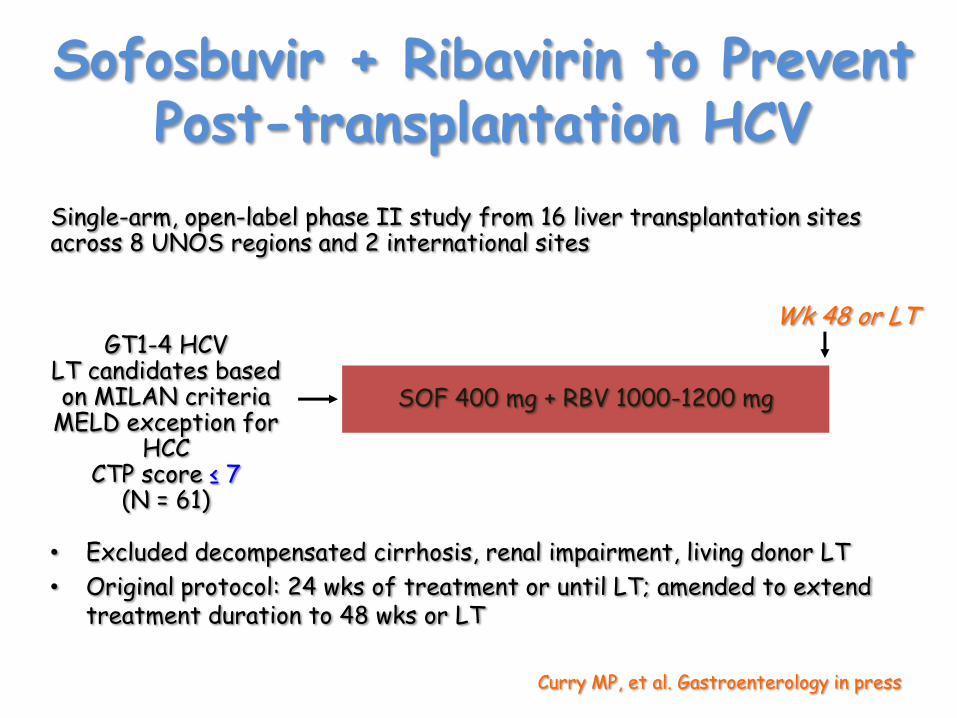
Sofosbuvir + Ribavirin to Prevent Post-transplantation HCV
• Excluded decompensated cirrhosis, renal impairment, living donor LT
• Original protocol: 24 wks of treatment or until LT; amended to extend treatment duration to 48 wks or LT
SOF 400 mg + RBV 1000-1200 mg
Wk 48 or LT GT1-4 HCV
LT candidates based on MILAN criteria
MELD exception for HCC
CTP score ≤ 7 (N = 61)
Single-arm, open-label phase II study from 16 liver transplantation sites across 8 UNOS regions and 2 international sites
Curry MP, et al. Gastroenterology in press
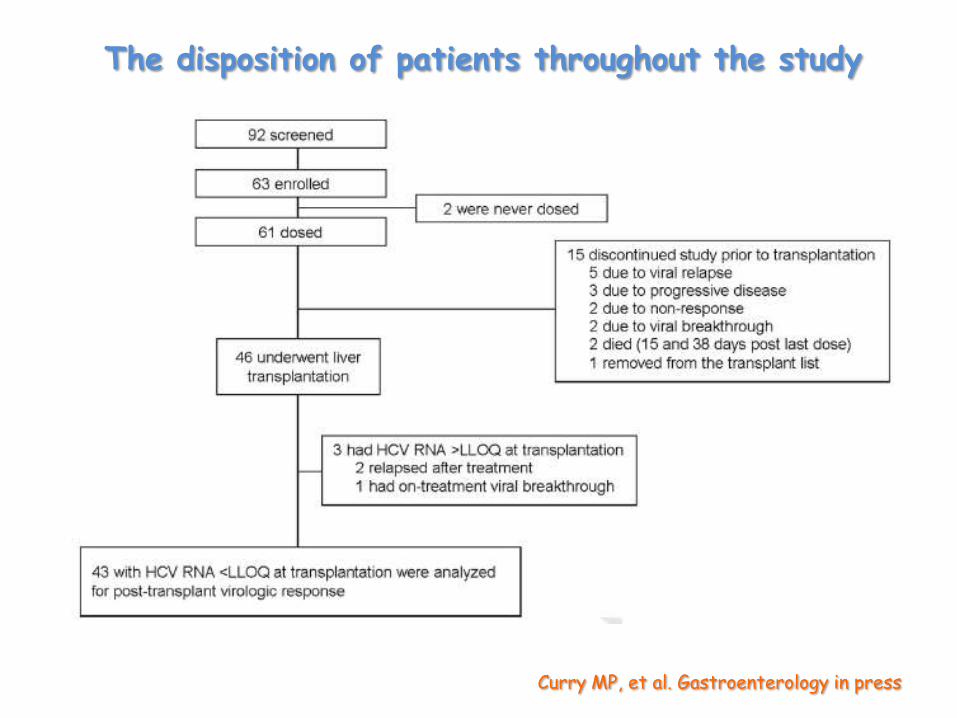
The disposition of patients throughout the study
Curry MP, et al. Gastroenterology in press
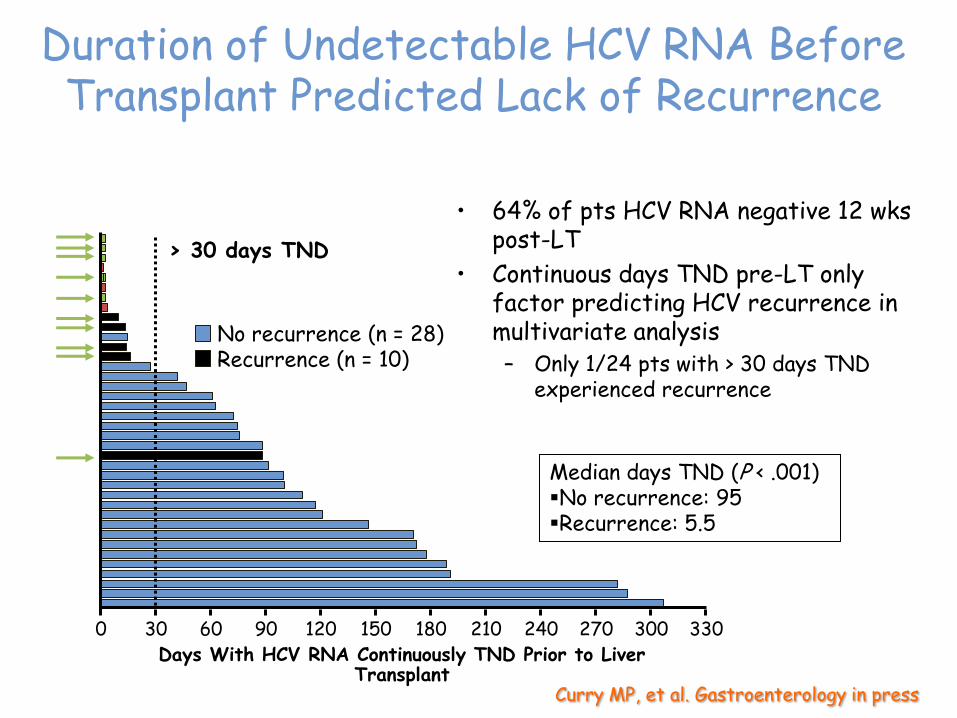
Duration of Undetectable HCV RNA Before Transplant Predicted Lack of Recurrence
• 64% of pts HCV RNA negative 12 wks post-LT
• Continuous days TND pre-LT only factor predicting HCV recurrence in multivariate analysis – Only 1/24 pts with > 30 days TND
experienced recurrence
330 0 30 60 90 120 150 180 210 240 270 300 Days With HCV RNA Continuously TND Prior to Liver
Transplant
> 30 days TND
No recurrence (n = 28) Recurrence (n = 10)
Median days TND (P < .001) No recurrence: 95 Recurrence: 5.5
Curry MP, et al. Gastroenterology in press
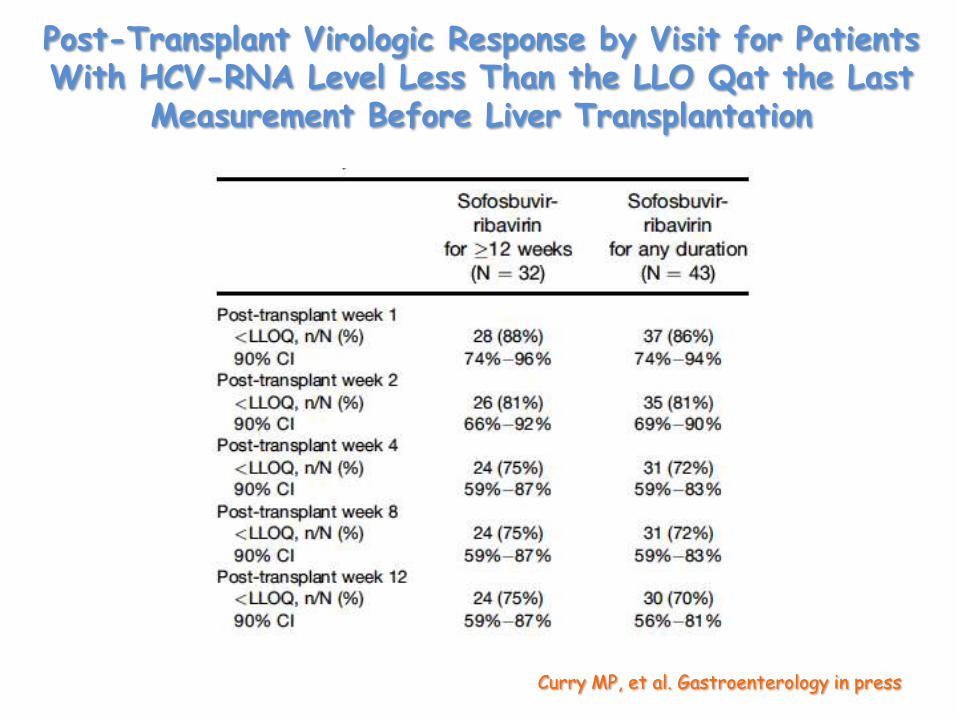
Post-Transplant Virologic Response by Visit for Patients With HCV-RNA Level Less Than the LLO Qat the Last
Measurement Before Liver Transplantation
Curry MP, et al. Gastroenterology in press
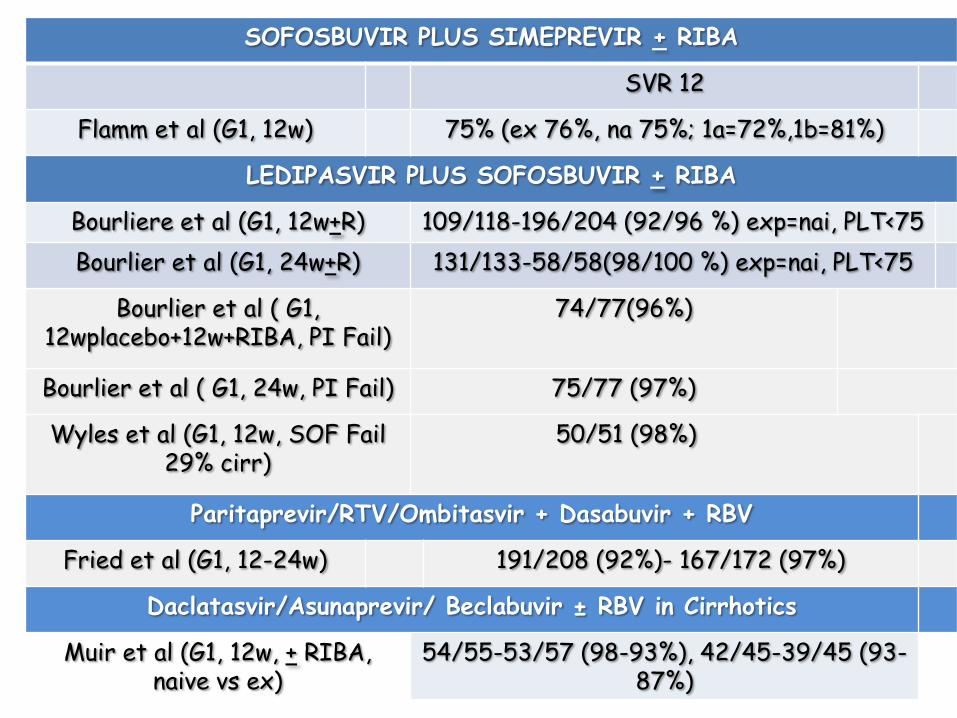
SOFOSBUVIR PLUS SIMEPREVIR + RIBA
SVR 12
Flamm et al (G1, 12w) 75% (ex 76%, na 75%; 1a=72%,1b=81%)
LEDIPASVIR PLUS SOFOSBUVIR + RIBA
Bourliere et al (G1, 12w+R) 109/118-196/204 (92/96 %) exp=nai, PLT<75
Bourlier et al (G1, 24w+R) 131/133-58/58(98/100 %) exp=nai, PLT<75
Bourlier et al ( G1, 12wplacebo+12w+RIBA, PI Fail)
74/77(96%)
Bourlier et al ( G1, 24w, PI Fail) 75/77 (97%)
Wyles et al (G1, 12w, SOF Fail 29% cirr)
50/51 (98%)
Paritaprevir/RTV/Ombitasvir + Dasabuvir + RBV
Fried et al (G1, 12-24w) 191/208 (92%)- 167/172 (97%)
Daclatasvir/Asunaprevir/ Beclabuvir ± RBV in Cirrhotics
Muir et al (G1, 12w, + RIBA, naive vs ex)
54/55-53/57 (98-93%), 42/45-39/45 (93-87%)
Fried MW, et al. AASLD 2014. Abstract 81. Reproduced with permission.
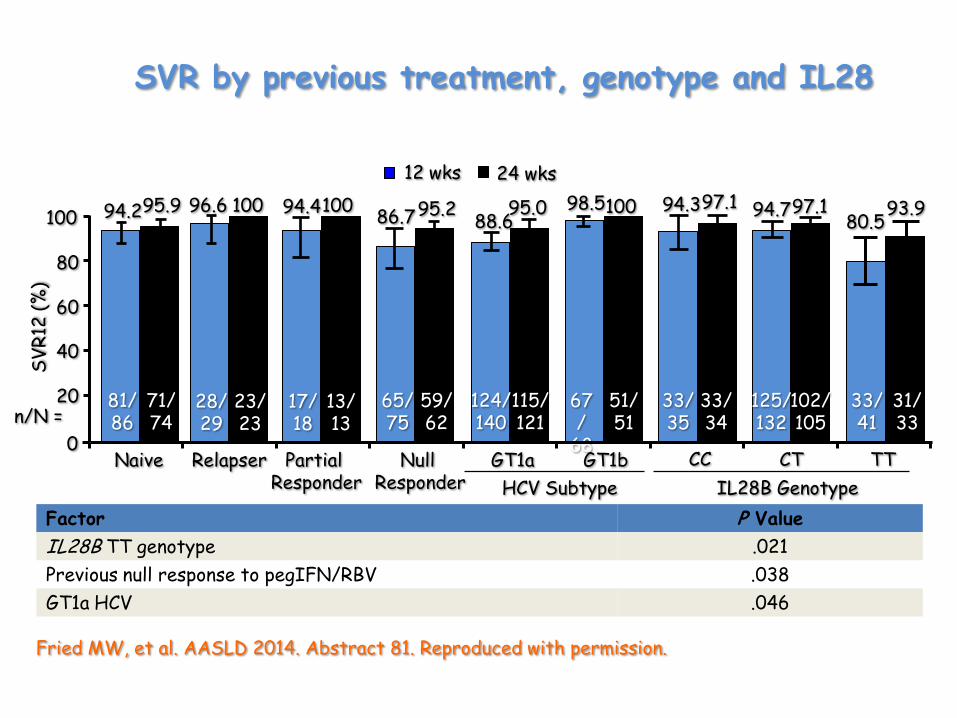
12 wks 24 wks
97.1 94.7 97.1 93.9
CT TT GT1a GT1b
124/ 140
67/
68
115/ 121
51/ 51
88.6 95.0 98.5 100
125/ 132
33/ 41
102/ 105
31/ 33
HCV Subtype
CC
33/ 35
33/ 34
94.3 80.5
IL28B Genotype
SV
R12
(%
)
Null Responder
65/ 75
59/ 62
100
80
60
40
20
0
86.7 95.2
Factor P Value
IL28B TT genotype .021
Previous null response to pegIFN/RBV .038
GT1a HCV .046
Partial Responder
Relapser Naive
17/ 18
13/ 13
94.4 100
28/ 29
23/ 23
96.6 100
81/ 86
71/74
94.2 95.9
n/N =
SVR by previous treatment, genotype and IL28
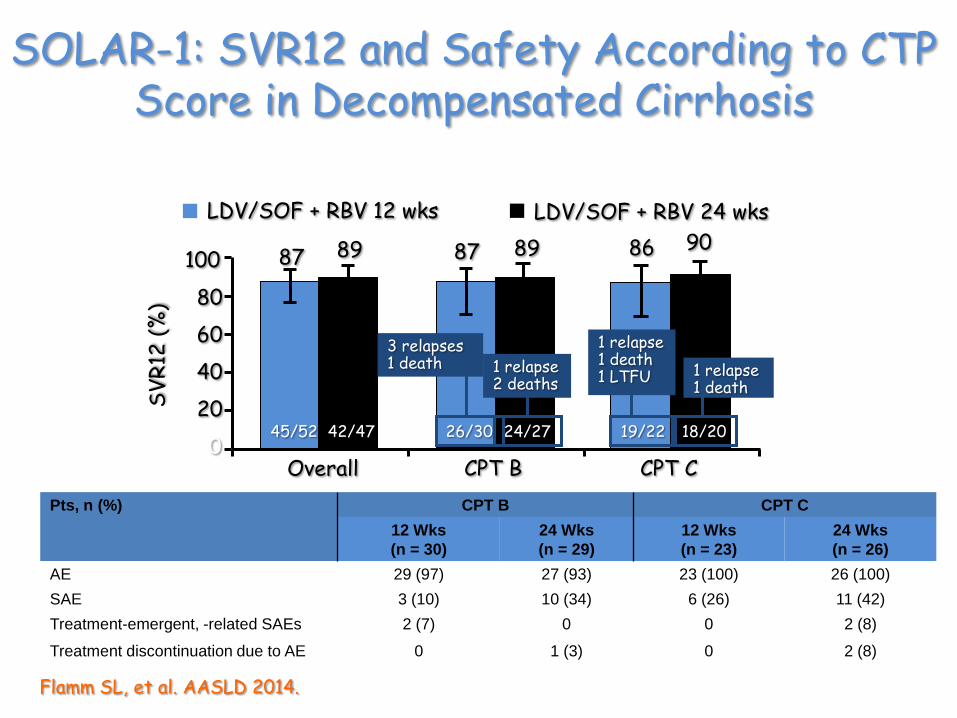
SOLAR-1: SVR12 and Safety According to CTP Score in Decompensated Cirrhosis
Flamm SL, et al. AASLD 2014.
Pts, n (%) CPT B CPT C
12 Wks
(n = 30)
24 Wks
(n = 29)
12 Wks
(n = 23)
24 Wks
(n = 26)
AE 29 (97) 27 (93) 23 (100) 26 (100)
SAE 3 (10) 10 (34) 6 (26) 11 (42)
Treatment-emergent, -related SAEs 2 (7) 0 0 2 (8)
Treatment discontinuation due to AE 0 1 (3) 0 2 (8)
100
80
60
40
20
0
SV
R12
(%
)
Overall CPT B CPT C
LDV/SOF + RBV 12 wks LDV/SOF + RBV 24 wks
87 89
45/52 42/47
87 89 86 90
26/30 24/27 19/22 18/20
3 relapses 1 death 1 relapse
2 deaths
1 relapse 1 death 1 LTFU 1 relapse
1 death

Post-Transplant
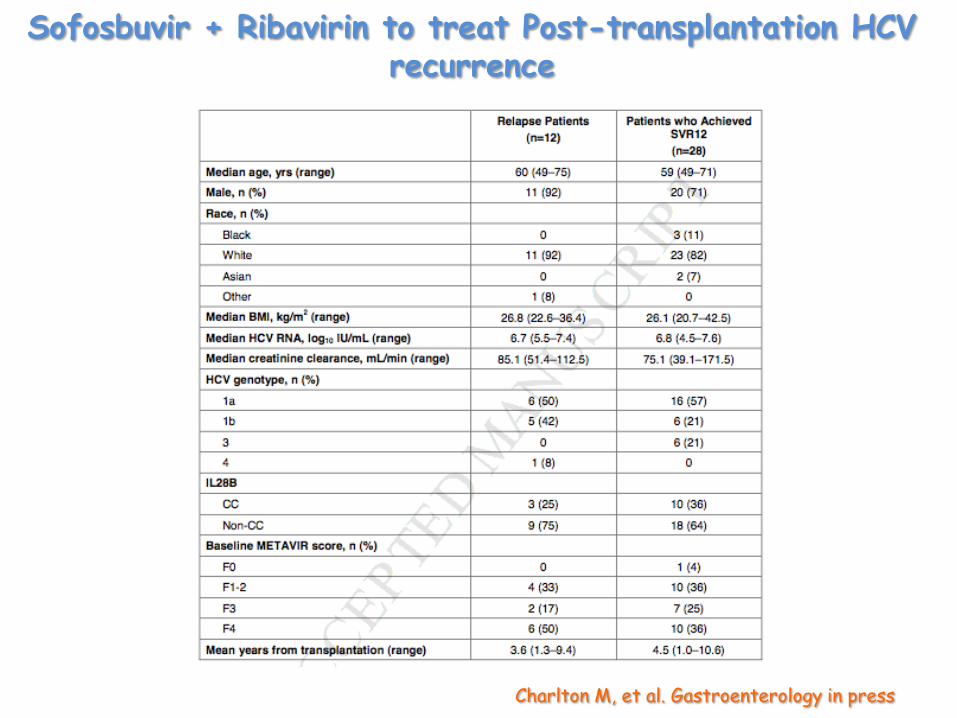
Charlton M, et al. Gastroenterology in press
Sofosbuvir + Ribavirin to treat Post-transplantation HCV recurrence
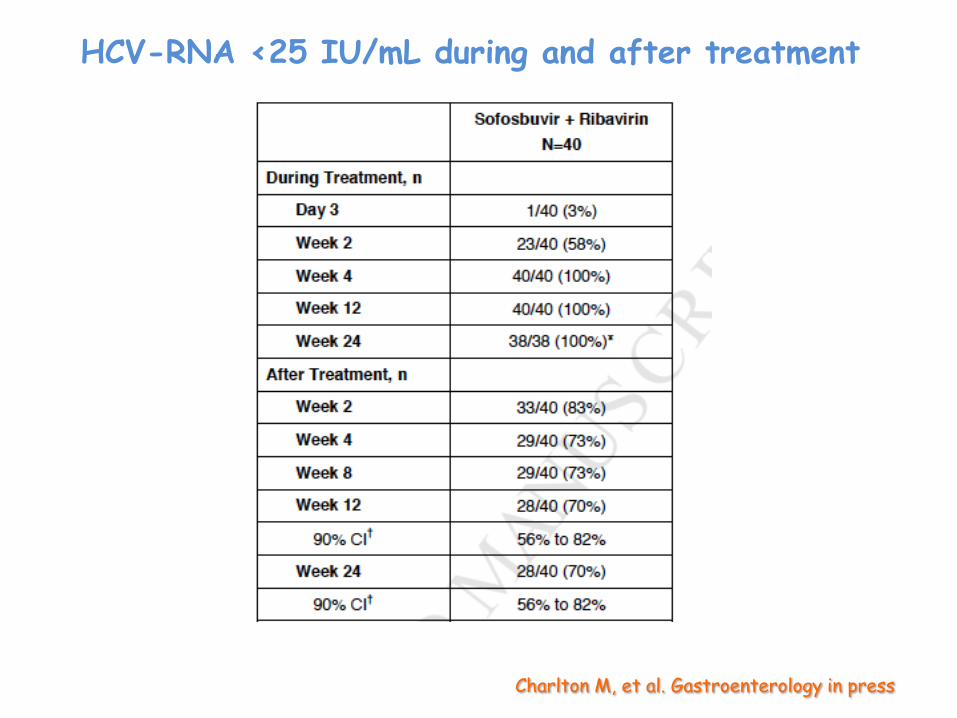
HCV-RNA <25 IU/mL during and after treatment
Charlton M, et al. Gastroenterology in press
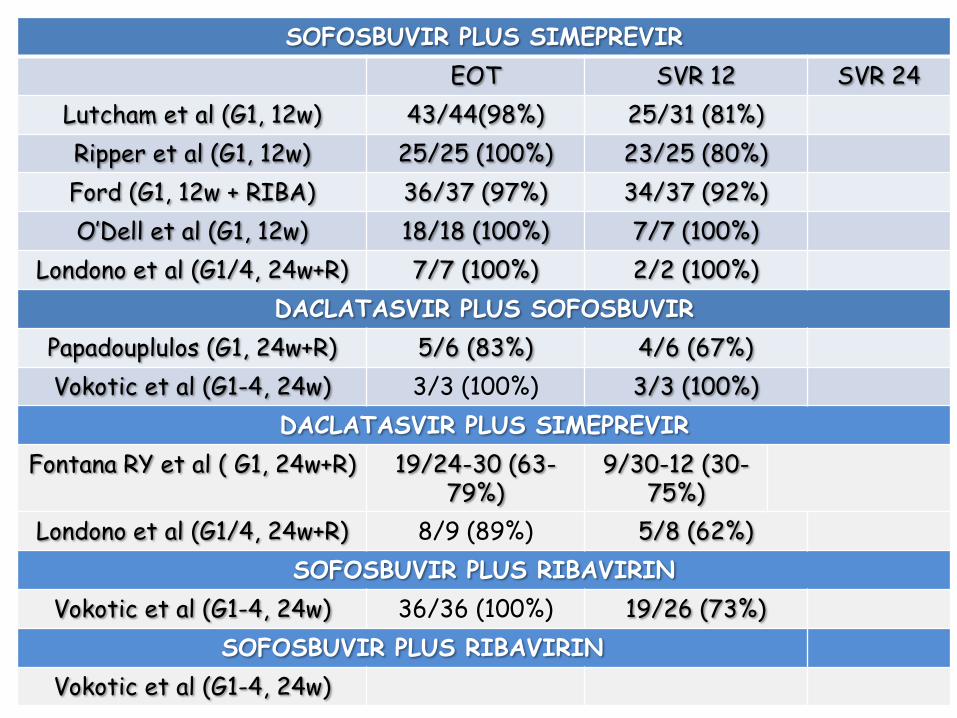
SOFOSBUVIR PLUS SIMEPREVIR
EOT SVR 12 SVR 24
Lutcham et al (G1, 12w) 43/44(98%) 25/31 (81%)
Ripper et al (G1, 12w) 25/25 (100%) 23/25 (80%)
Ford (G1, 12w + RIBA) 36/37 (97%) 34/37 (92%)
O’Dell et al (G1, 12w) 18/18 (100%) 7/7 (100%)
Londono et al (G1/4, 24w+R) 7/7 (100%) 2/2 (100%)
DACLATASVIR PLUS SOFOSBUVIR
Papadouplulos (G1, 24w+R) 5/6 (83%) 4/6 (67%)
Vokotic et al (G1-4, 24w) 3/3 (100%) 3/3 (100%)
DACLATASVIR PLUS SIMEPREVIR
Fontana RY et al ( G1, 24w+R) 19/24-30 (63-79%)
9/30-12 (30-75%)
Londono et al (G1/4, 24w+R) 8/9 (89%) 5/8 (62%)
SOFOSBUVIR PLUS RIBAVIRIN
Vokotic et al (G1-4, 24w) 36/36 (100%) 19/26 (73%)
SOFOSBUVIR PLUS RIBAVIRIN
Vokotic et al (G1-4, 24w)
Vukotic et al AASLD 2014
No rejection episodes
Severe adverse events (SAEs) occurred in 12 (16.9%):
• 4 deaths (5.6%) • 1 re-OLT (1.4%) • 7 hospitalizations (9.9%)
Safety
Kwo et al 2014 NEJM
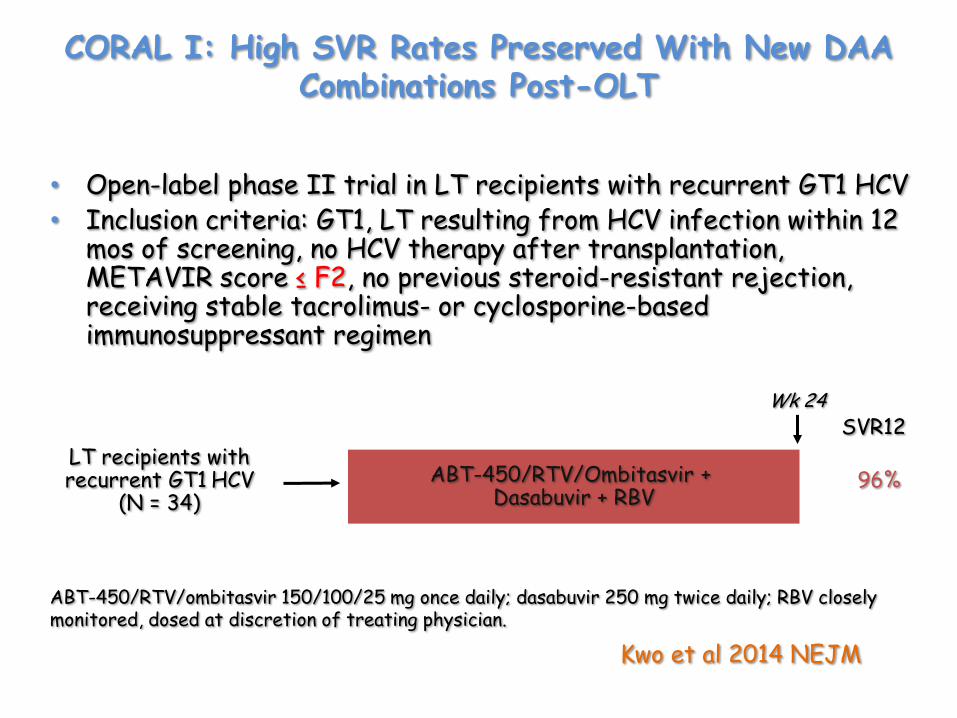
CORAL I: High SVR Rates Preserved With New DAA Combinations Post-OLT
• Open-label phase II trial in LT recipients with recurrent GT1 HCV • Inclusion criteria: GT1, LT resulting from HCV infection within 12
mos of screening, no HCV therapy after transplantation, METAVIR score ≤ F2, no previous steroid-resistant rejection, receiving stable tacrolimus- or cyclosporine-based immunosuppressant regimen
ABT-450/RTV/Ombitasvir + Dasabuvir + RBV
Wk 24
ABT-450/RTV/ombitasvir 150/100/25 mg once daily; dasabuvir 250 mg twice daily; RBV closely monitored, dosed at discretion of treating physician.
LT recipients with recurrent GT1 HCV
(N = 34)
SVR12
96%
Kwo et al 2014 NEJM
Calcineurin Inhibitor Dosing With ABT-450/RTV/Dasabuvir + Ombitasivr
• Phase I study: dosing tacrolimus or cyclosporine with the 3 DAA regimen compared with either alone resulted in:
– 7-fold increase in tacrolimus half-life
– 3-fold increase in cyclosporine half-life
• Based on these findings, recommended dosing during 3 DAA treatment was:
– Tacrolimus 0.5 mg once weekly or 0.2 mg every 3 days
– Cyclosporine 1/5 of the daily pre-3 DAA treatment dose given once daily
Kwo et al 2014 NEJM
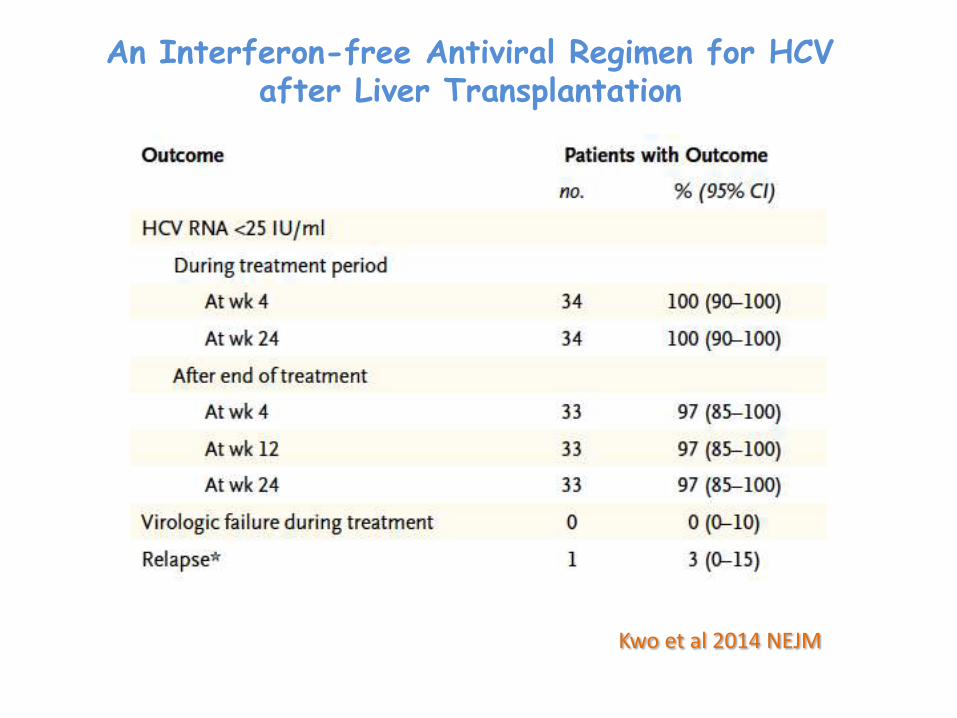
An Interferon-free Antiviral Regimen for HCV after Liver Transplantation
Reddy KR et al AASLD 2014 Abstract 8
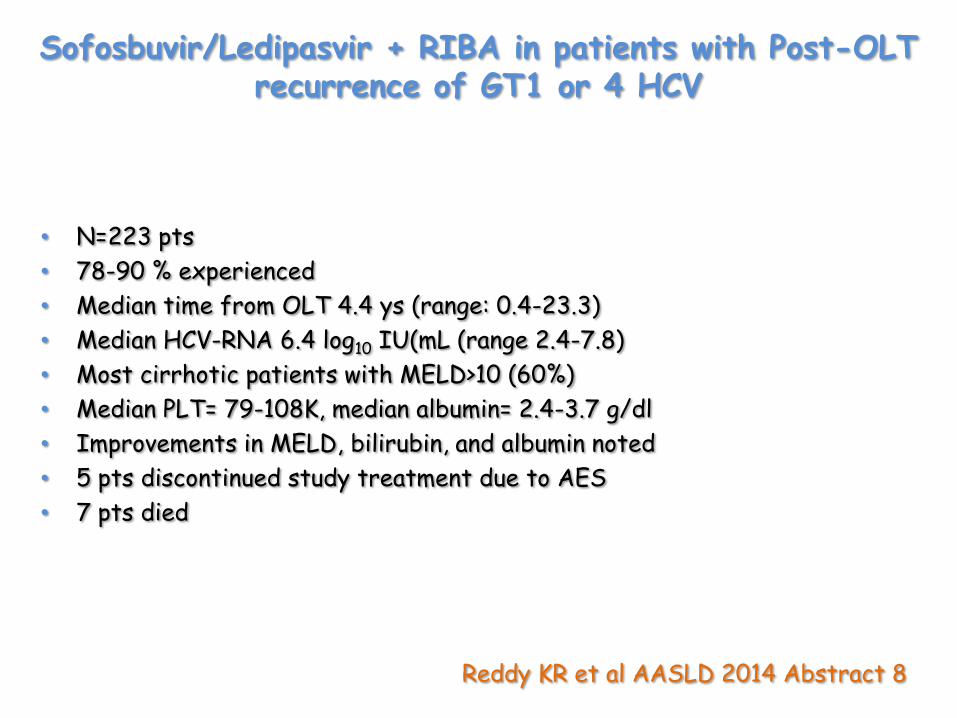
• N=223 pts
• 78-90 % experienced
• Median time from OLT 4.4 ys (range: 0.4-23.3)
• Median HCV-RNA 6.4 log10 IU(mL (range 2.4-7.8)
• Most cirrhotic patients with MELD>10 (60%)
• Median PLT= 79-108K, median albumin= 2.4-3.7 g/dl
• Improvements in MELD, bilirubin, and albumin noted
• 5 pts discontinued study treatment due to AES
• 7 pts died
Sofosbuvir/Ledipasvir + RIBA in patients with Post-OLT recurrence of GT1 or 4 HCV
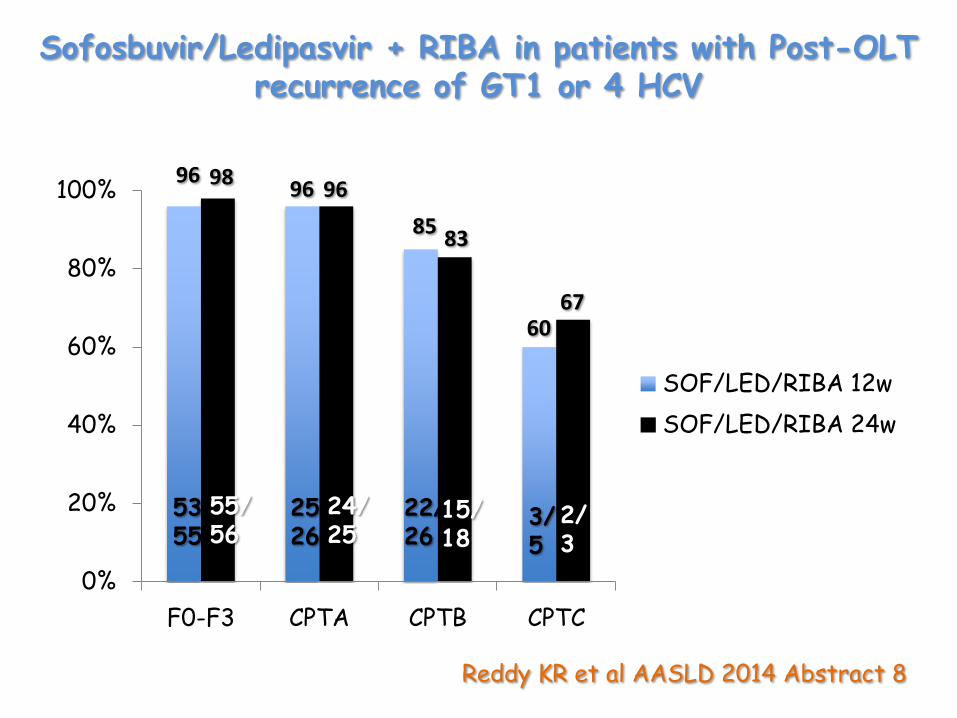
Reddy KR et al AASLD 2014 Abstract 8
Sofosbuvir/Ledipasvir + RIBA in patients with Post-OLT recurrence of GT1 or 4 HCV
0%
20%
40%
60%
80%
100%
F0-F3 CPTA CPTB CPTC
SOF/LED/RIBA 12w
SOF/LED/RIBA 24w
96 98
53/55
55/56
96 96
25/26
24/25
22/26
15/18
85 83
60 67
3/ 5
2/ 3
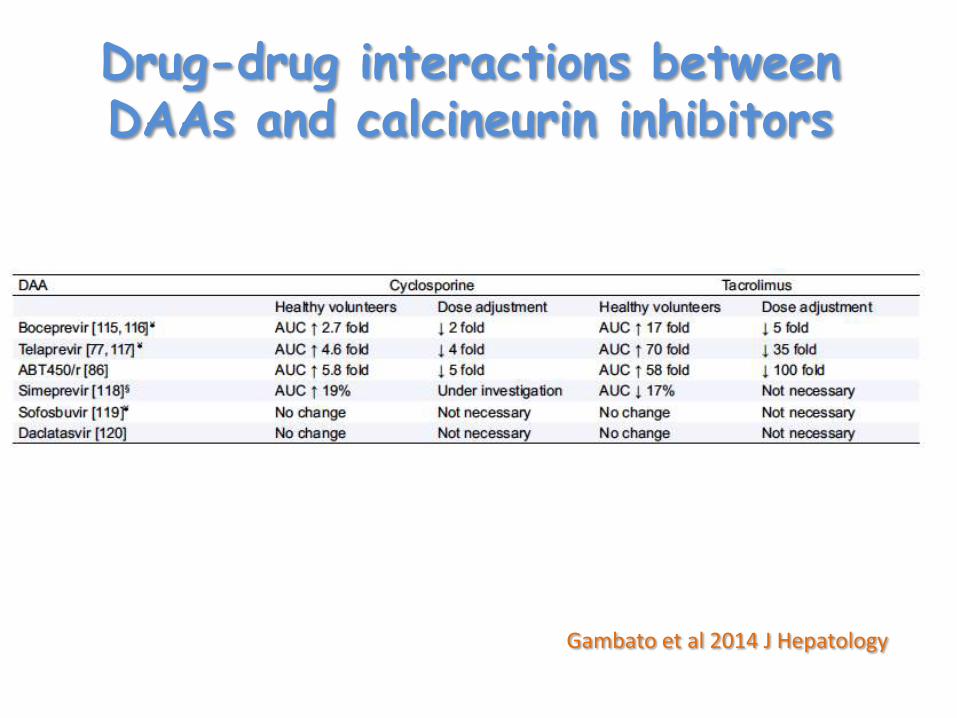
Drug-drug interactions between DAAs and calcineurin inhibitors
Gambato et al 2014 J Hepatology
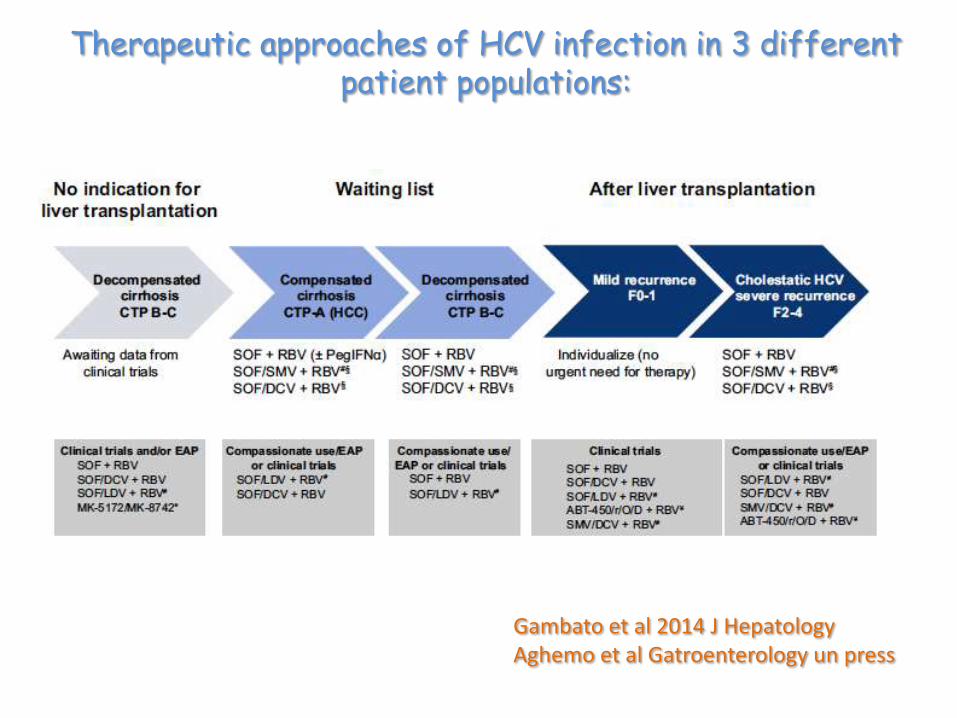
Gambato et al 2014 J Hepatology Aghemo et al Gatroenterology un press
Therapeutic approaches of HCV infection in 3 different patient populations:
CONCLUSION
• Current oral therapy limited to compassionate use of: – Sofosbuvir + ribavirin + Peg-IFN
– Sofosbuvir + simeprevir or daclatasvir + Ribavirin
• Additional all-oral therapies for GT1 will be approved in 2015-16 – ABT-450/RTV/ombitasvir + dasabuvir + Ribavirin
– Sofosbuvir/ledipasvir + Ribavirin
– Daclatasvir + asunaprevir or simeprevir+ Ribavirin
• Expect > 90% SVR, 12- to 24-wk duration
• Interferon will not be required
• RBV-free therapies also desirable
Recommended

















