
Impact of extending Social Health Insurance for the poor on facility-based
deliveries in the Philippines
카를로파레데스Karlo Paolo P. [email protected]
서울대학교보건대학원Seoul National University | Graduate School of Public Health
August 2015
COHRED | Global Forum on Research and Innovation for Health

Contents
• Introduction and Background of the Study
•Philippines’ Health System
• The UHC/KP policy
•Objectives
•Methods
•Key Messages
보건대학원 | Graduate School of Public Health

Background
• Channeling increased funding flows through the National Health Insurance schemes offers the best avenue to improve (1) the supply of services, (2) access to health services and (3) delivering quality health care, especially in low-income countries (WHO, 2005)
• Strong calls for Universal Health Coverage has prompted countries to institute / expand health insurance and prioritize health (WHO, 2008, 2010, 2013)
• However, recent studies have no consensus on the impact of health insurance especially among the poor, with no strong evidence of an impact on utilization, financial risks and health status (Acharya et al., 2013)
보건대학원 | Graduate School of Public Health

Background
• Philippines – premium sharing for the poor (National and Local) has not increased coverage under Philhealth (Before UHC/KP policy) (Chakraborty 2013)
보건대학원 | Graduate School of Public Health
Extension of SHI for
the poor
Voluntary
Free
Discounted Fees
• Strategy in the Philippines has shifted from a premium sharing scheme for the identified poor by LGUs (Pre-policy) to Full National Government subsidy to the proxy-tested poor in 2011 (post-policy) (DOH 2011, Philhealth revised IRR, 2013).
• Since then, there has been a marked increase in the number of SHI indigent members from 22% in 2010 to 46% in 2014 (More than the employed members at 40% in 2014) (Philhealth, 2010, 2014)
Strategies in expanding SHI for the poor

Philippines’ Health System
• 1991 – Health System was Devolved• Local Chief Executives (LCEs) role critical in Local Health
development after Devolution
• DOH – Remained (National Health Agency)
• DOH Regional Agency – Center for Health Development Offices
• DOH Retained Hospitals / Specialty centers
• 1995 – Creation of the National Health Insurance
• 1999 – Health Sector Reform Agenda
• 2005 – FOURmula 1 for Health (Financing, Service Delivery, Regulation & Governance)
• 2011 – UHC (Kalusugang Pangkalahatan)Levels of Health Service Delivery
Source: Melgar, J. D. (2010). Organizing Health Services towards Universal Health Care. Acta
Medica Philippina, Volume 44 No. 4(Universal Health Care for Filipinos: A Proposal), 36-42.
보건대학원 | Graduate School of Public Health

UHC/KP policy in the Philippines
• Enrollment of 5.2 Million Poor Filipinos to the National Health Insurance (Philhealth)
• Training and Mobilization of Community Health Teams (CHTs) to increase utilization of health services / use of Philhealth
• Reduction of unmet needs for Maternal and Child Health
• Health Facilities Enhancement Program – to Improve capacities of Health Facilities
보건대학원 | Graduate School of Public Health
3 Thrusts of UHC in the PhilippinesSource: Kalusugan Pangkalahatan Execution Plan and Implementation Arrangements (2011).
Aquino Health Agenda – Universal health Care (2010)
KalusuganPangkalahatan
(UHC) Framework for Implementation

UHC/KP policy in the Philippines
보건대학원 | Graduate School of Public Health
National Household Targeting System for Poverty Reduction
(NHTS-PR)
Proxy Means Test (PMT); Identification of the poorest of the poor Filipinos (5.2 M)
DOH / PhilhealthEnrollment to SHI
(Sponsored category)
Poor household: How were they enrolled under the UHC/KP?
보건대학원 | Graduate School of Public Health
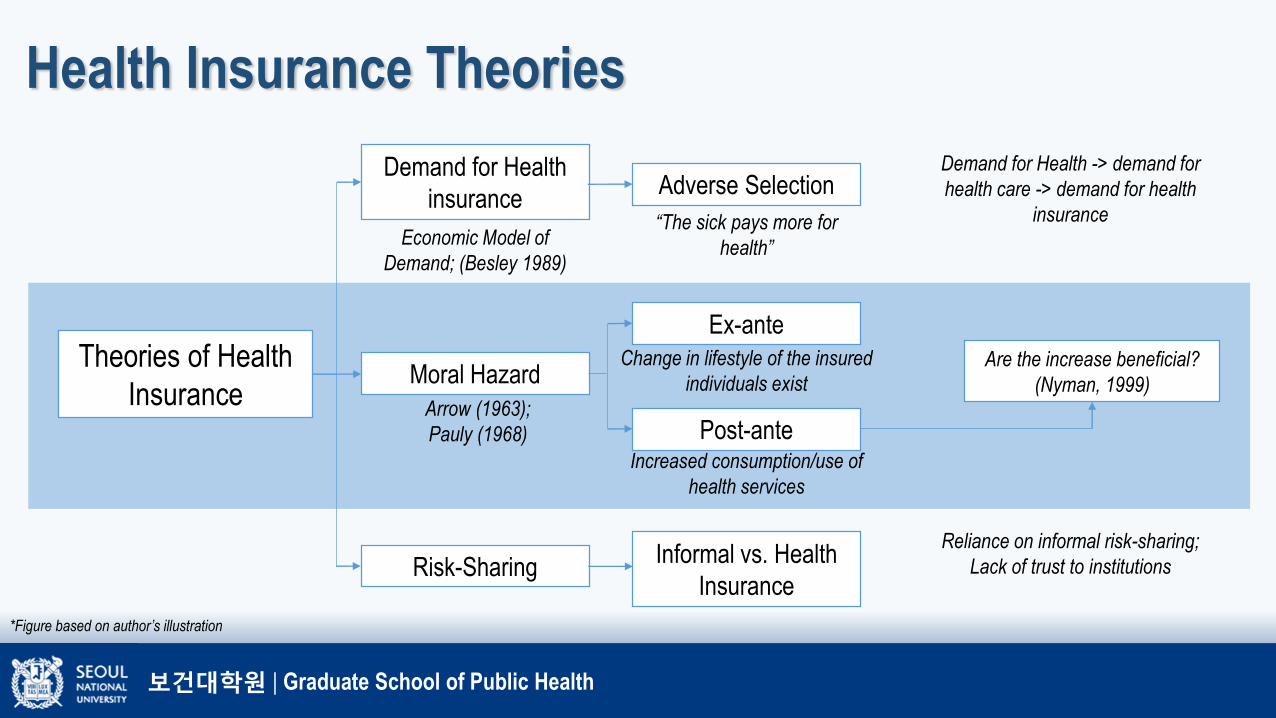
Health Insurance Theories
Theories of Health
Insurance
Demand for Health
insurance
Moral Hazard
Risk-Sharing
Adverse Selection
Ex-ante
Post-ante
Informal vs. Health
Insurance
Economic Model of
Demand; (Besley 1989)
“The sick pays more for
health”
Demand for Health -> demand for
health care -> demand for health
insurance
Change in lifestyle of the insured
individuals exist
Increased consumption/use of
health services
Are the increase beneficial?
(Nyman, 1999)
Reliance on informal risk-sharing;
Lack of trust to institutions
Arrow (1963);
Pauly (1968)
*Figure based on author’s illustration

보건대학원 | Graduate School of Public Health
Value of Health Insurance
Nyman (1999): Value of Health Insurance
Health
Insurance
Risk Aversion Value
Access Value
The access value of health insurance is related to the
value of the consumer of medical care that the person
would not otherwise be able to afford.
“If the insurance is the only way to gain access to
expensive health care, then the value of insurance for that
care is the expected consumer surplus from health care
that would otherwise be inaccessible”
Moral Hazard as otherwise implied, is not necessarily
inefficient if the increase in health service use was brought
by the access value of insurance to necessary services
that were previously inaccessible.
In the context of low-income countries, where levels of
unmet needs tends to be substantial, increased in
consumption are not necessarily problematic (Jowett,
2004)

보건대학원 | Graduate School of Public Health
Related studies
Studies measuring SHI impact to the poor (targeted)
Country Study objectives Results
Colombia(Trujillo, Portillo, &
Vernon, 2005)
Measurement of the impact of the subsidized
health insurance for the poor in Colombia (PSM
and IV Estimations)
The subsidized health insurance program greatly
increased medical care utilization among the poor
Colombia(Miller, Pinto, and
Vera-Hernandez,
2009)
Determination of how the SR enrollment is
associated with financial risk protection and
efficiency in health service use (IV estimation)
The SR has been successful in financially protecting
the poor from financial risk associated with medical
costs of unexpected illnesses; Increase in utilization of
the previously underutilized preventive services.
Vietnam(Wagstaff, 2010)
Measuring the impact of VHCFP on health
service use and financial risk protection using
VHLS surveys (Difference-in-differences)
VHCFP had no impact on use of health services. ATT
of health insurance did not show statistically significant
results for out-patient or in-patient visits; VHCFP
substantially reduced OOP spending.

보건대학원 | Graduate School of Public Health
Related studies
Studies measuring SHI impact to the poor (targeted)
Country Study objectives Results
Vietnam(Axelson et al, 2009)
Evaluation of the short-term impacts of VHCFP
on utilization and out of pocket expenditure using
VHLS survey (PSM and double differencing)
Small, positive impact on overall healthcare
utilization; statistically significant result in out-patient
strong negative impact on out-of-pocket expenditure;
the insured had lower OOP expenditure for in-patient care
Georgia(Bauhoff, Hotchkiss,
and Smith, 2011)
Measuring the impact of the medical insurance
for the poor using a dedicated survey of 3500
households (RDD estimation)
There was no impact seen on utilization; lower
expenditure was only seen on the elderly group, all others
with no robust evidence. Lower expenditure among the
insured for inpatient care.
Georgia(Zoidze, Rukhazde,
Chkhatarashvili, and
Gotsadze, 2013)
Mix-method study of Georgia’s health insurance
for the poor, using secondary data analysis and
health expenditure and utilization surveys of
2007-2010 (DID)
MIP has positive impact in terms of reduced
expenditure for IP services; Consequently, the MIP had
almost no significant effect on health services
utilization.

Did health insurance made health services more accessible to the poor?
보건대학원 | Graduate School of Public Health

보건대학원 | Graduate School of Public Health
Methods3.1 Research Design SHI Impact and Health
Service Utilization
I. Quasi-Experimental
- Impact of extending
SHI for the poor
Data Source Description Percentage of Insured HH (Income
quintile 1&2)
NDHS 2013 (Post-policy) NHDS survey data conducted in the Philippines after the
UHC/KP policy in 201144.24% of total households covered
NDHS 2008 (Pre-policy) NDHS survey data conducted in the Philippines before the
initiation of the UHC/KP policy in 201115.75% of total households covered
Department of Health /
Philhealth / National
Statistical Board
Information about regional/provincial community-level variables
to be used in the analysisWealth Index: Samples are categorized
using an index which is equal to 1 for the
poorest to 5 for the richest

보건대학원 | Graduate School of Public Health
Methods
Why NDHS?
DHS Year Total Households
Covered
Total population
(Women, Children,
Household Members)
Total Women
Respondents
Total number of
Children <5
% of Poor and next
poor samples (Q1 &
2)
2013 14,804
(43% in Q1&2)
70,100
(45% in Q1&2)
16,155
(40% in Q1&2)
7,216
(54% in Q1&2)
40% of total sample
2008 12,469
(45% in Q1&2)
60,901
(45% in Q1&2)
13,594
(40% in Q1&2)
6,572
(55% in Q1&2)
40% of total sample

보건대학원 | Graduate School of Public Health
Methods
Measuring impact of sponsored SHI on health service use (Facility-based delivery)
Impact of Health insurance to
Service Utilization
Level 2: Community-level
characteristics
(1) Women (Q1&2) who
delivered in the last 24 months
(NDHS 2013)
Insured under UHC/KP
(treatment)
Uninsured (control)

보건대학원 | Graduate School of Public Health
Methods
Determination of the impact of SHI for the poor
will be determined controlling both for
individual and community factors.
Variable Name Coding Definition
Dependent Variable
fbd - Women who last delivered
in a facility (Facility-Based
Delivery)
0, 1 Identified women who delivered in a health facility (government / private)
Dependent variable in a binary form
Facility Delivery (Q1 & Q2)
Year
2008 2013
Yes 290 (24%) 679 (51%)
No 928 (76%) 651 (49%)

보건대학원 | Graduate School of Public Health
MethodsModel: DID under Linear Probability Model
(LPM), with cluster-robust standard errors
Interaction terms in the DID model using a
Non-linear model will not be able to show
the ATT of the interaction variable (A &
Norton, 2003; Athey & Imbens, 2006)
Difference-in-Differences Estimation

보건대학원 | Graduate School of Public Health
MethodsModel: DDD under Linear Probability Model
(LPM), with cluster-robust standard errors
Identification of post-policy effect of SHI on
utilization with consideration of urban/rural
community types
Assumption: individuals from urban
community types have more access to
health facilitiesTriple Differences Estimation

보건대학원 | Graduate School of Public Health
ResultsMLR HLM
Interaction variables Model 1 Model 2 Model 3 Model 4 Model 5 Model 6 Model 7 Model 8 Model 9 Model 10
Interaction (DD) -0.07 -0.01 -.09 -0.02 -0.07 -0.01 -0.01 -0.09 -0.03 -0.03
Interaction (DDD) 0.05 0.01 0.08 0.04 0.04
Insured 0.06 0.06 0.07* 0.06 0.05 0.05 0.05 0.06 0.05 0.05
Post-policy 0.29* .26 * 0.31* 0.28 0.30* 0.27* 0.26* 0.33* 0.30* .30 *
Insured*postpolicy -0.07 -0.01 -.09* -0.02 -0.07 -0.01 -0.01 -0.09 -0.03 -0.03
Community Type 0.14* 0.08 .13* .08* .08*
Community Type * Post policy -.10* -0.08 -0.13* 0-.12* -.13*
Insured*Community Type 0.02 0.04 0.00 0.02 0.03
Independent Variables (x)
Education 0.08* .08 * 0.08 0.08 0.08* 0.08*
Number of HH Members -0.01* -.01 * -0.01 -0.01* -0.01 -0.01*
Head of HH Sex -0.04 -0.04 -0.04 -0.04 -0.04 -0.04
Head of HH Age 0.00* 0.00 * .002301 * 0.00* 0.00* .00*
Wealth Index Decile (5 decimals) 1.45e-06*
1.36e-06 * 0.00 1.20e-06*
1.21e-06 *
1.17e-06 *
Total number of Children -0.01* -.01 * -0.01 -.01 * -0.01 -0.01
Union Status -0.04 -0.03 -0.02 -0.02 -0.02 -0.02
Partners' Educational Attainment .06* 0.06 0.05 .05* 0.05* 0.05
Age group 0.00 0.00 0.00 0.00 0.00 0.00
Level 2 Variables (Regions)
MD to Population Ratio 0.00 0.00
RN to Population Ratio 0.00 0.00
MW to Population Ratio 0.00 0.00
Number of Government Hospitals -0.01* -0.01*
Number of Private Hospitals -0.01* -0.01*
Number of RHUs / Lying-in 0.00 0.00
Number of Philhealth Accredited Hospitals 0.01 .01 *
n=2,257
• The models yielded insignificantresults.
• This suggests that despite the fact that FBDs increased (2008-2013), there is no significant evidence to say that the increase was brought by the “insured” status of the poor (from UHC/KP policy).

보건대학원 | Graduate School of Public Health
Key Messages
1. Measuring the impact of the recent policy change in the Philippines, insuring
the poor does not seem to have an immediate effect of increasing use of
health services.
2. Further studies to explore other barriers to health use despite the
“insured” status of the poor should be further investigated which may be
related to the following:
• Availability of health facilities (for delivery) where the poor is located
• Awareness of the nationally sponsored poor of their health insurance benefits
• Ease of Use (of insurance benefits) in facilities
• OOP payments above insurance coverage (from patient experience), etc.

보건대학원 | Graduate School of Public Health
Key Messages
3. Many countries now are using subsidies to achieve UHC – it is important
therefore to note that while health insurance is important to enable the
poor to access services, other supply- / demand-side barriers beyond
financing services should be considered.
4. Medium- and long-term evaluation is recommended for thorough policy
evaluation and future health policy development.

보건대학원 | Graduate School of Public Health
Thank You!
Maraming Salamat!
감사합니다!
Karlo Paredes

References (In slides)Acharya, A., Vellakkal, S., Taylor, F., Masset, E., Satija, A., Burke, M., & Ebrahim, S. (2013). The Impact of
Health Insurance Schemes for the Informal Sector in Low- and Middle-Income Countries: A Systematic Review. The World Bank Research Observer, 28(2), 236-266. doi: 10.1093/wbro/lks009
Andersen, R. M. (2008). National Health Surveys and the Behavioral Model of Health Services Use. Medical Care, 46(7), 647-653 610.1097/MLR.1090b1013e31817a31835d.
Arrow, K. J. (1963). Uncertainty and the Welfare Economics of Medical Care. The American Economic Review, 53(5), 941-973. doi: 10.2307/1812044
Axelson, H., Bales, S., Minh, P. D., Ekman, B., & Gerdtham, U. G. (2009). Health financing for the poor produces promising short-term effects on utilization and out-of-pocket expenditure: evidence from Vietnam. Int J Equity Health, 8, 20. doi: 10.1186/1475-9276-8-20
Babitsch, B., Gohl, D., & von Lengerke, T. (2012). Re-revisiting Andersen’s Behavioral Model of Health Services Use: a systematic review of studies from 1998–2011. GMS Psycho-Social-Medicine, 9, Doc11. doi: 10.3205/psm000089
Bauhoff, S., Hotchkiss, D. R., & Smith, O. (2011). The impact of medical insurance for the poor in Georgia: a regression discontinuity approach. Health economics, 20(11), 1362-1378. doi: 10.1002/hec.1673
Besley, T. (1989). The Demand for Health Care and Health Insurance. Oxford Review of Economic Policy, 5(1), 21-33.
Chakraborty, S. (2013). Philippines' Government Sponsored Health Coverage Program for the Poor Households. UNICO Studies Series 22. Retrieved October 25, 2014, from https://openknowledge.worldbank.org/bitstream/handle/10986/13295/75010.pdf?sequence=1
Culyer, A. J., & Wagstaff, A. (1993). Equity and equality in health and health care. Journal of Health Economics, 12(4), 431-457. doi: http://dx.doi.org/10.1016/0167-6296(93)90004-X
Kalusugan Pangkalahatan Execution Plan and Implementation Arrangements (2011). Doorslaer, E. v., & O’Donnell, O. (2008). Measurement and Explanation of Inequity in Health and Health
Care in Low-Income Settings. WIDER Discussion Papers, World Institute for Development Economics (UNU-WIDER), 2008/04.
Duan, N. (1983). Smearing Estimate: A Nonparametric Retransformation Method. Journal of the American Statistical Association, 78(383), 605-610. doi: 10.1080/01621459.1983.10478017
Duan, N., Manning, W. G., Morris, C. N., & Newhouse, J. P. (1984). Choosing Between the Sample-Selection Model and the Multi-Part Model. Journal of Business & Economic Statistics, 2(3), 283-289. doi: 10.1080/07350015.1984.10509396
Jowett, M. (2004). Theoretical insights into the development of health insurance in low-income countries. University of York Centre for Health Economics(Discussion Paper 188).
Melgar, J. D. (2010). Organizing Health Services towards Universal Health Care. Acta Medica Philippina, Volume 44 No. 4(Universal Health Care for Filipinos: A Proposal), 36-42.
Miller, G., Pinto, D., & Vera-Hernandez, M. (2009). High-powered Incentives in Developing Country Health Insurance: Evidence from Colombia's Regimen Subsidiado. NATIONAL BUREAU OF ECONOMIC RESEARCH(NBER Working Paper Series).
National Statistics Office (NSO) [Philippines], a. I. C. F. M. (2009). National Demographic and Health Survey 2008.
Nyman, J. A. (1999). The value of health insurance: the access motive. Journal of Health Economics, 18(2), 141-152. doi: http://dx.doi.org/10.1016/S0167-6296(98)00049-6
O'Donnel, O., Doorslaer, E. v., Wagstaff, A., & Lindelow, M. (2008). Analyzing Health Equity Using Household Survey Data. Washington DC: The World Bank.
Pauly, M. V. (1968). The Economics of Moral Hazard: Comment. The American Economic Review, 58(3), 531-537. doi: 10.2307/1813785
Acharya, A., Vellakkal, S., Taylor, F., Masset, E., Satija, A., Burke, M., & Ebrahim, S. (2013). The Impact of Health Insurance Schemes for the Informal Sector in Low- and Middle-Income Countries: A Systematic Review. The World Bank Research Observer, 28(2), 236-266. doi: 10.1093/wbro/lks009
Andersen, R. M. (2008). National Health Surveys and the Behavioral Model of Health Services Use. Medical Care, 46(7), 647-653 610.1097/MLR.1090b1013e31817a31835d.
Arrow, K. J. (1963). Uncertainty and the Welfare Economics of Medical Care. The American Economic Review, 53(5), 941-973. doi: 10.2307/1812044
Axelson, H., Bales, S., Minh, P. D., Ekman, B., & Gerdtham, U. G. (2009). Health financing for the poor produces promising short-term effects on utilization and out-of-pocket expenditure: evidence from Vietnam. Int J Equity Health, 8, 20. doi: 10.1186/1475-9276-8-20
Babitsch, B., Gohl, D., & von Lengerke, T. (2012). Re-revisiting Andersen’s Behavioral Model of Health Services Use: a systematic review of studies from 1998–2011. GMS Psycho-Social-Medicine, 9, Doc11. doi: 10.3205/psm000089
Bauhoff, S., Hotchkiss, D. R., & Smith, O. (2011). The impact of medical insurance for the poor in Georgia: a regression discontinuity approach. Health economics, 20(11), 1362-1378. doi: 10.1002/hec.1673
Besley, T. (1989). The Demand for Health Care and Health Insurance. Oxford Review of Economic Policy, 5(1), 21-33.
Chakraborty, S. (2013). Philippines' Government Sponsored Health Coverage Program for the Poor Households. UNICO Studies Series 22. Retrieved October 25, 2014, from https://openknowledge.worldbank.org/bitstream/handle/10986/13295/75010.pdf?sequence=1
Culyer, A. J., & Wagstaff, A. (1993). Equity and equality in health and health care. Journal of Health Economics, 12(4), 431-457. doi: http://dx.doi.org/10.1016/0167-6296(93)90004-X
Kalusugan Pangkalahatan Execution Plan and Implementation Arrangements (2011). Doorslaer, E. v., & O’Donnell, O. (2008). Measurement and Explanation of Inequity in Health and Health
Care in Low-Income Settings. WIDER Discussion Papers, World Institute for Development Economics (UNU-WIDER), 2008/04.
Duan, N. (1983). Smearing Estimate: A Nonparametric Retransformation Method. Journal of the American Statistical Association, 78(383), 605-610. doi: 10.1080/01621459.1983.10478017
Duan, N., Manning, W. G., Morris, C. N., & Newhouse, J. P. (1984). Choosing Between the Sample-Selection Model and the Multi-Part Model. Journal of Business & Economic Statistics, 2(3), 283-289. doi: 10.1080/07350015.1984.10509396
Jowett, M. (2004). Theoretical insights into the development of health insurance in low-income countries. University of York Centre for Health Economics(Discussion Paper 188).
Melgar, J. D. (2010). Organizing Health Services towards Universal Health Care. Acta Medica Philippina, Volume 44 No. 4(Universal Health Care for Filipinos: A Proposal), 36-42.
Miller, G., Pinto, D., & Vera-Hernandez, M. (2009). High-powered Incentives in Developing Country Health Insurance: Evidence from Colombia's Regimen Subsidiado. NATIONAL BUREAU OF ECONOMIC RESEARCH(NBER Working Paper Series).
National Statistics Office (NSO) [Philippines], a. I. C. F. M. (2009). National Demographic and Health Survey 2008.
Nyman, J. A. (1999). The value of health insurance: the access motive. Journal of Health Economics, 18(2), 141-152. doi: http://dx.doi.org/10.1016/S0167-6296(98)00049-6
O'Donnel, O., Doorslaer, E. v., Wagstaff, A., & Lindelow, M. (2008). Analyzing Health Equity Using Household Survey Data. Washington DC: The World Bank.
Pauly, M. V. (1968). The Economics of Moral Hazard: Comment. The American Economic Review, 58(3), 531-537. doi: 10.2307/1813785
Pauly, M. V. (1968). The Economics of Moral Hazard: Comment. The American Economic Review, 58(3), 531-537. doi: 10.2307/1813785
Philippine Health Insurance Corporation. (2010). Stats and Charts. Retrieved February 11, 2015, from http://www.philhealth.gov.ph/about_us/statsncharts/snc2010.pdf
Philippine Health Insurance Corporation. (2013). Revised Implementing Rules and Regulation of the National Health Insurance Act (RA 7875 as ammended by RA 9241 and 10606). Manila, Philippines.
Philippine Health Insurance Corporation. (2014). Stats and Charts. Retrieved February 11, 2015, from http://www.philhealth.gov.ph/about_us/statsncharts/snc2014.pdf
Philippine Statistics Authority (PSA) [Philippines], & I.C.F. International. (2014). Philippines National Demographic and Health Survey 2013.
Sen, A. (2002). Why health equity? Health economics, 11(8), 659-666. doi: 10.1002/hec.762 Son, H. H. (2009). Equity in Health and Health Care in the Philippines. ADB Economics Working Paper
Series. Retrieved October 26, 2014, from http://unpan1.un.org/intradoc/groups/public/documents/apcity/unpan050000.pdf
Trujillo, A., Portillo, J., & Vernon, J. (2005). The Impact of Subsidized Health Insurance for the Poor: Evaluating the Colombian Experience Using Propensity Score Matching. International Journal of Health Care Finance and Economics, 5(3), 211-239. doi: 10.1007/s10754-005-1792-5
Wagstaff, A. (2010). Estimating health insurance impacts under unobserved heterogeneity: the case of Vietnam's health care fund for the poor. Health economics, 19(2), 189-208. doi: 10.1002/hec.1466
World Health Organization. (2008). Primary Health Care (Now more than ever) World Health Report. Geneva, Switzerland: World Health Organization.
World Health Organization. (2010). Health Systems Financing: The path to universal coverage. World Health Report. Geneva, Switzerland.
World Health Organization. (2013). Research for Universal Health Coverage. World Health Report. Retrieved October 27, 2014, from http://www.who.int/whr/2013/report/en/
Zoidze, A., Rukhazde, N., Chkhatarashvili, K., & Gotsadze, G. (2013). Promoting universal financial
protection: health insurance for the poor in Georgia – a case study. Health Research Policy and Systems.
Recommended











![[6] kesetimbangan partikel & fbd](https://img.pdfslide.net/doc/110x75/55920fd11a28abf47d8b4754/6-kesetimbangan-partikel-fbd.jpg)




