British Journal of Ophthalmology 1996;80:536-540
Indocyanine green angiographic findings inserpiginous choroidopathy
A Giovannini, C Mariotti, E Ripa, B Scassellati-Sforzolini
AbstractAims-Analysis of the choroidal findingsin patients affected by serpiginous chor-oidopathy (SC).Methods-Thirteen patients (23 eyes; 11males and two females; age range 50-68years; mean age 59.1 years) affected by SCwere examined with fluorescein angiogra-phy (FA) and indocyanine green angio-graphy (ICGA). The follow up periodwas 7-33 months.Results-Using ICGA the disease could bedivided into the the following stages: (1)subclinical or choroidal stage (hypofluo-rescent lesions without FA evidence);(2) active stage (with ICGA and FAevidence); (3) subhealing stage (slight latehyperfluorescent lesions with ICGA, withno evidence on FA); (4) inactive or healedstage (hypofluorescent areas with ICGAand hyperfluorescent areas with FA).Conclusions-Although FA showed a cleardistinction between active and healedstages, ICGA allowed a greater subdivi-sion of the disease. In particular, ICGAallowed: (1) better staging ofSC, revealingchoroidal alterations when there was noophthalmoscopic or FA evidence; (2) bet-ter identification of the active lesionswhich appear to be larger at the choroidallevel in comparison with the correspondingretinal lesions; and (3) revealed a persis-tence of choroidal activity even when thesigns of retinal activity had disappeared.Thus, ICGA should be a particularly usefulclinical and therapeutic monitoring toolofSC.(BrJ Ophthalmol 1996;80:536-540)
Serpiginous choroidopathy (SC) usually ex-tends from the optic disc outwards in alldirections'-'; initial spreading from the maculararea is occasional and at first free of anyperipapillar activity (serpiginous maculopa-thy).4 5SC, known also as geographic helicoidperipapillary choroidopathy' is a chronic,recurrent, progressive, usually bilateral disor-der, that extends from the choroid to theretinal pigment epithelium (RPE) and ulti-mately to the retina. In the acute stage it iscommon to observe the concomitant expres-sion of new and old lesions. The active lesionsare greyish white or yellow in colour, with faintedges and are sometimes associated with aserous detachment of the neuroepitheliumand/or less frequently of the RPE.6 SC can befurther complicated by choroidal neovasculari-sation (CNV), usually occurring at the edge of
an old lesion, which may represent a furthercause of visual impairment in such patients.Other findings include retinal vasculitis,7 gen-erally at the site of an active lesion and venousbranch occlusion.8 The healed stage is charac-terised by well defined, irregularly pigmentedatrophic chorioretinal areas. Visual prognosisof SC depends on the extent of foveal involve-ment.The active lesions are hypofluorescent dur-
ing the early phases of fluorescein angiographyand hyperfluorescent in the late phases withlate diffusion. The healed lesions, on the otherhand, initially appear as an area ofhypofluores-cence, along with clearly visible residual largechoroidal vessels, secondary to choriocapillarisand RPE atrophy. As a result of fluoresceinspreading from the choriocapillaris and scleralstaining, the area of healing becomes hyper-fluorescent, with well defined edges.The causes of this disorder are still under
investigation. However, there are theories sug-gesting that either inflammatory"' or vascularfactors are involved." 12 Data collected fromthe limited histopathological studies per-formed to date 10 13 tend to favour theinflammatory hypothesis; indeed extensivelymphocyte choroidal infiltrates were found atthe margin of thelesion, but a coagulation dis-order (increase in factor VIII) has beenobserved in some cases." The distribution ofthe lesions may suggest a choroidal arterialocclusion and its vascular character wouldmake it possible to unify the two theories.
Indocyanine green (ICG) angiographyallows a better investigation of the choroidalcirculation: ICG has the highest point ofabsorption and the maximum emission in thenear infrared, and so allows us to overcome thescreen represented by the RPE and xantho-phyll. Good visualisation of the vascularchoroidal system (even if there are still limits inthe exploration ofthe choriocapillaris) is due tothe fact that 98% of ICG is linked to plasmaproteins, with a consequent poor diffusion out-side the choroidal and/or retinal normal vesselwalls. ICG angiography (ICGA), because ofthe possibilities it offers and the choroidalnature of SC, is undoubtedly helpful in assess-ing the possible pathogenesis of the disease.The aim of our study was to compare
fluorescein angiography (FA) and ICGA chor-oidal findings in order to improve the stagingand the evaluation of the therapeutic responseof SC.
Materials and methodsWith high definition videoangiography (Top-con IMAGEnet H1024) we examined 13
Clinica Oculistica dell'UniversitA di Ancona,Nuovo OspedaleRegionale di Torrette,Ancona, ItalyA GiovanniniC MariottiE RipaB Scassellati-Sforzolini
Correspondence to:A Giovannini, ClinicaOculistica dell' Universita diAncona, Nuovo OspedaleRegionale di Torrette, 60020Ancona, Italy.
Accepted for publication11 March 1996
536

Indocyanine green angiographic findings in serpiginous choroidopathy
patients affected by SC (23 eyes; 11 males andtwo females; age 50-68 years; mean age 59.1years): six patients (nine eyes) at the activestage viewed with ophthalmoscopy (yellowplaque at the level of the RPE) and FA, sevenpatients (14 eyes) at the inactive stage. Thepatients were followed up for 7-33 months.
All patients underwent complete ophthalmicexamination: colour and red-free fundusphotography, FA, and ICGA. ICGA was per-formed using 25 mg/patient of ICG (Car-diogreen, Hynson,Westcott and Dunning, Inc,Baltimore, MD, USA) injected into a periph-eral arm vein which was followed immediatelyby a 5 ml flush of sterile saline via a three waystopcock.
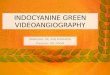
Figure 1 Subclinical stage. (A) Indocyanine greenangiography (ICGA) shows hypofluorescent choroidallesions with faint edges (arrows). (B) The lesions are notevident onfluorescein angiography (FA). (C) Two monthslater the lesions are seen even on FA , in an areacorresponding to the choroidal lesions seen with ICGA.
ResultsOf the 23 eyes examined, nine presented signsof ophthalmoscopic and FA activity. In four ofthem we observed more than one recurrence(one case presented two recurrences, two casesthree recurrences, and one case four recur-rences).FA signs of activity (early hypofluorescence
with late leakage of the focus) have been welldescribed by Schatz et al,13 Hamilton andBird,'4 and Laatikainen and Erkkila. 5The findings provided by ICGA in the active
stage, after the observation of all recurrences,can be summarised as follows:
(1) In seven eyes we found a correspondencebetween ICG and FA findings, characterisedby early hypofluorescent areas with late hyper-fluorescence and faint edges.
(2) In 10 eyes ICGA showed in allangiographic phases an area of hypofluores-cence with ill defined margins and a sizegreater than that seen in FA.
(3) A third pattern of activity was observedonly with ICGA: a hypofluorescent area(distant from the area observed in FA) with illdefined margins in all phases (three eyes).
(4) ICGA showed, in our series, choroidalhyperfluorescence only in the late phases, afterthe active focus appeared to have healed whenviewed with an ophthalmoscope and FA (twoeyes). In these cases only ICGA revealed chor-oidal permeability alterations.ICGA alsorevealed delayed choroidal filling
(a time longer or equal to 8 seconds from the
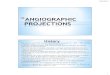
Figure 2 Active stage. (A) Fluorescein angiographyshows an active focus, hyperfluorescent in the late phases(arrow). (B) In the indocyanine green angiograms theactive area appears hypofluorescent with faint edges and nolate hyperfluorescence (arrows).
537

Giovannini, Mariotti, Ripa, Scassellati-Sforzolini
Figure 3 Active stage. (A) (B) Fluorescein angiographyreveals the classic early hypofluorescence with latehyperfluorescence of the active focus (arrows). (C) (D) Thebehaviour of the active focus in the indocyanine greenangiogram is comparable (arrows). (E) Note the markedlate leakage (arrow).
moment of the choroidal blush till the full cho-roidal filling)'6 17 in 42.1% of cases of SC at theactive stage. Moreover, ICGA showed hyper-fluorescence with late leakage of the activelesions in 47.4% of cases secondary to choroi-dal permeability alterations. We observed a
reduction or regression of activity of theinitially active lesions after systemic steroids(1 g intravenous methylprednisolone for 5consecutive days) in 11 eyes presenting signs ofactivity or recurrences threatening the fovea.
DiscussionIf FA showed an unequivocal distinctionbetween the active and the inactive stages ofSC, ICGA seemed to enable us to make a more
accurate analysis of the disease. In ICGA theactive focus appeared as a hypofluorescent area
with faint edges, visible from the early phasesto the intermediate and late phases of theangiography. This image was frequently ac-
companied by a hyperfluorescent halo varyingin intensity, with diffusion in the late angio-
graphic phases, a possible sign of alteration inchoroidal permeability. The area ofhealing wasalways hypofluorescent with well defined mar-gins in all ICGA phases.rThe comparison of the data obtained from
FA and ICGA of our patients allow us to clas-sify SC into four distinct stages.
(1) The subclinical stage (choroidal stage ofthe disease) is characterised by hypofluores-cent lesions with faint edges, the manifestationof choroidal changes was detectable only withICGA; the RPE remains unaffected, indeedophthalmoscopy and FA indicate that no suchlesions are present. This aspect may continuefor a prolonged period of time withoutadditional manifestations. During the followup, new lesions may also be visible distant fromformer ones and on FA, alterations can bedetected at the same site previously seen onICGA (Fig 1).
(2) At the active stage, when the lesion dam-ages the RPE and therefore becomes evidenton ophthalmoscopic and FA examination(retinal stage), two ICG angiographic patternsare evident: (a) at the active stage, and in thepresence of the aforementioned sign of activity(early hypofluorescence with late leakage), theICGA reveals active areas of hypofluorescencewhich are similar in size, but are neverthelessusually larger compared with those observed inFA. No late hyperfluorescence is evident (Fig2); (b) occasionally the classic FA early hypof-luorescence with late leakage of the activefocus, corresponds to an early ICGA hypoflu-
538

Indocyanine green angiographic findings in serpiginous choroidopathy
Figure 4 Third stage. (A) Fluorescein angiography reveals no activity (arrow). (B) (C) Indocyanine green angiographyshows a hyperfluorescent halo with slight late leakage (arrows). (D) After 2 months ofsystemic steroids a regression of thehyperfluorescence can be observed (arrow).
oescence with faint edges and is associatedwith a marked hyperfluorescence with evidentdiffusion in the la,- 4hases. These manifesta-tions of altered permeability of the choroidalvessels are sign of increased aggressiveness ofthe disease (Fig 3).
(3) ICGA makes it possible to identify asubhealing stage characterised by activitywhich persists at the level of the choroid, afterthe focus itself appears to have healed at thelevel of the RPE. In such cases choroidalpermeability alterations, which are usuallyadjacent to a recently healed focus, can bedetected only by ICGA. These anomalies arecharacterised by a slight late diffusion withoutFA evidence. Systemic steroid therapy cancause the regression of such signs of choroidalactivity (Fig 4)
(4) The inactive or healed stage presents asan area of hypofluorescence with clearlydefined margins; this hypofluorescencebecomes more marked in the late phases.Within the area itself, images of greater hypof-luorescence emerge indicating irregular pig-mentation of the atrophic zones, together withthe remaining patent choroidal vessels (Fig 5).Note that the extension of the healed area isusually smaller than that at the active stage.After steroid therapy a reduction in the extentof the inactive hypofluorescent area comparedwith the initial active lesions is visible.
In the light of our observations and evidenceprovided by FA and ICGA we present a newclassification of SC. ICGA made it possible toobserve in more detail the various aspects ofthe disorder than did FA. In particular it
picture. (B) Indocyanine green i
hypofluorescent lesion with wellangiographic phases.
allowed: (1) better staging of SC, revealingchoroidal alterations without ophthalmoscopic
539

Giovannini, Mariotti, Ripa, Scassellati-Sforzolini
or FA evidence; (2) better identification of theactive lesions, which appear to be larger at thelevel of the choroid in comparison with thecorresponding retinal lesions; (3) to point out,at the active stage of the disease, a delayed cho-roidal filling in 42.1% of cases; and to indicatesigns of vasculitis (hyperfluorescence with lateleakage) of the active lesions in 47.4% of cases.Furthermore, a reduction in the extent of theinactive hypofluorescent areas, compared withthe initial active lesions, after systemic steroidtherapy was observed. All these elementswould therefore allow us to hypothesise a cor-relation between occlusive and inflammatorypathogenic theories; (4) to reveal a persistenceof choroidal activity even when the signs ofretinal activity have disappeared. The observa-tion of choroidal alterations without retinalchanges could be proof of the choroidal natureof the affection, as is supposed on the basis ofhistopathological studies by Gass" and Wuet al.9
In consideration of the above, ICGA couldbe a particularly useful tool for the clinicalmonitoring of SC and seems to provide a moresensitive method of investigation and apprecia-tion of the various stages of the disorder.Moreover, the ICG angiographic signs of sub-clinical activity could be helpful in developingmore accurate therapeutic schemes.
1 Weiss H, Annesley WH Jr, Shields JA, Tomer T, Christo-pherson K. The clinical course of serpiginous choroidopa-thy. Am J Ophthalmol 1979;87:133-42.
2 Schatz H, Maumenee AK, Patz A. Geographical helicoidperipapillary choroidopathy: clinical presentation and fluo-rescein angiographic findings. Trans Am Acad OphthalmolOtolaryngol 1974;78:747-61.
3 Chisholm IH, Gass JDM, HuttonWL. The late stage of ser-piginous (geographic) choroiditis. Am J Ophthalmol 1976;82:343-51.
4 Hardy RA, Schatz H. Macular geographic helicoid choroid-opathy. Arch Ophthalmol 1987;105:1237-42.
5 Mansour JM, Jampol LM, Packo KH, Hrisomalos NF.Macular serpiginous choroiditis. Retina 1988;8:125-31.
6 Wojno T, Meredith TA. Unusual findings in serpiginouschoroiditis. Am J Ophthalmol 1982;94:650-5.
7 Blumenkranz MJ, GassJDM, Clarkson JG. Atypical serpigi-nous choroiditis. Arch Ophthalmol 1982;100: 1773-5.
8 Erkkila H. Laatikainen L, Jokinen E. Immunological studiesofserpiginous choroiditis. GraefesArch Clin Exp Ophthalmol1982;219:131-4.
9 Wu JS, Lewis H, Fine SL, Grover DA, GreenWR. Clinico-pathologic findings in a patient with serpiginous choroiditisand treated choroidal neovascularization. Retina 1989;9:292-301.
10 Becquet F, Cohen SY, Coscas G. Choroidite serpigineuse. JFr Ophtalmol 1992;4:288-298.
11 King DG, GrizzardWS, Sever RJ, Espinoza L. Serpiginouschoroidopathy associated with elevated factor VII. VonWillebrand factor antigen. Retina 1990;10:97-101.
12 Gass JDM. Specific choroidal diseases causing disciformmacular detachment. In: Gass JDM, ed. Stereoscopic atlas ofmacular diseases: diagnosis and treatment, 3rd ed. St Louis:CV Mosby, 1987:136-44.
13 Schatz H, Maumenee AK, Patz A. Geographic helicoidperipapillary choroidopathy. Trans Am Acad OphthalmolOtolaryngol 1974;78:747-61.
14 Hamilton AM, Bird AC. Geographical choroidopathy. BrJOphthalmol 1974;58:784-97.
15 Laatikainen L, Erkkila H. Serpiginous choroiditis. Br J7Ophthalmol 1974;58:777-83.
16 De Laey JJ. Fluoro-angiographic study of the choroid inman. Bull Soc Belge Ophtalmol 1977;174:1-217.
17 Giovannini A, Mariotti C, Ripa E, Scassellati Sforzolini B,Tittareili R Choroidal filling in age-related maculardegeneration: indocyanine green angiographic findings.Ophthalmologica 1994;208:185-91.
540
Recommended