3/12/2018
1
Intravenous Fluid Therapy in Critical Illness
GINA HURST, MD
DIVISION OF EMERGENCY CRITICAL CARE
HENRY FORD HOSPITAL
DETROIT, MI
Objectives
▪ Establish goals of IV fluid therapy
▪ Review fluid types and availability
▪ Understand the concept of balanced solutions
▪ Discuss potential effects of hyperchloremia in the critically ill
3/12/2018
2
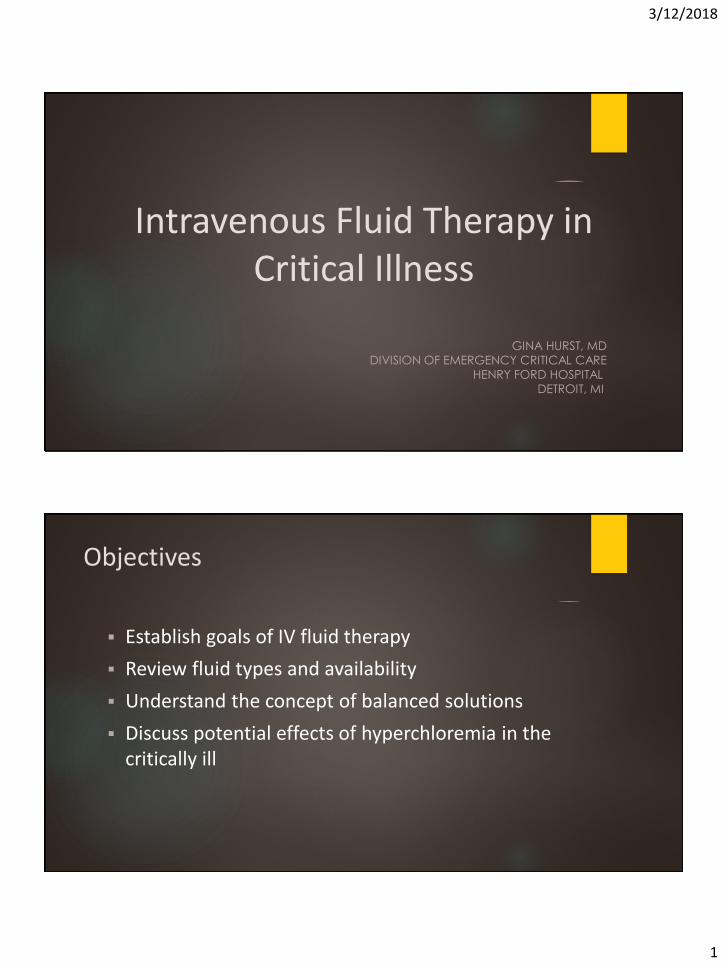
▪ Therapeutic efficacy
▪ Predictable response
▪ Low side effect profile
▪ Safety
▪ Suitability
▪ Ease of administration
▪ Cost
Intravenous Fluids
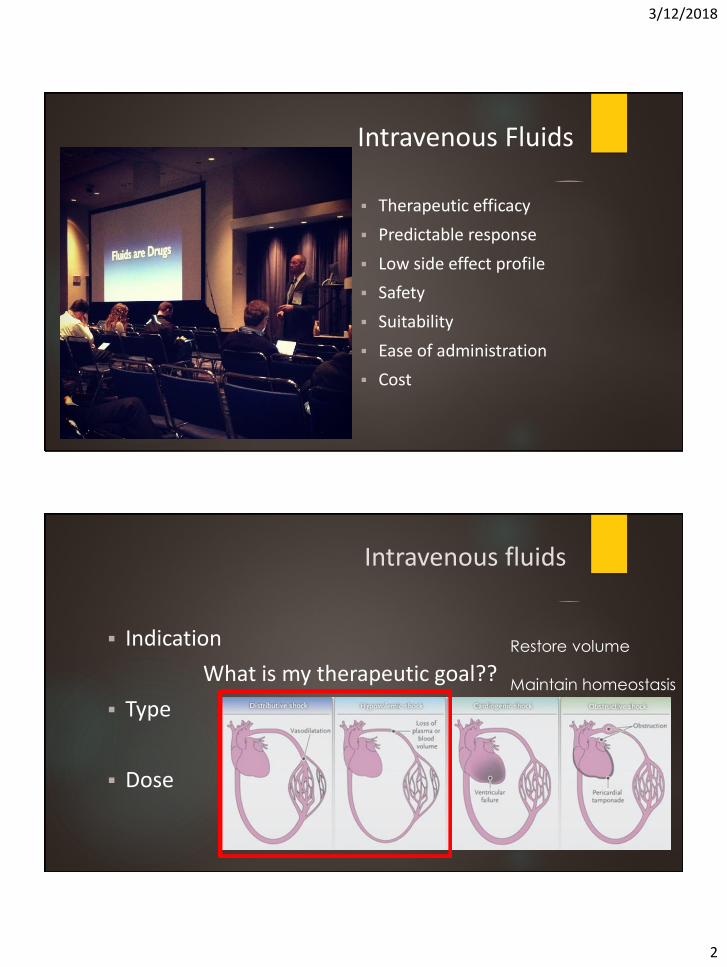
Intravenous fluids
▪ Indication
What is my therapeutic goal??
▪ Type
▪ Dose
Restore volume
Maintain homeostasis
3/12/2018
3
Intravenous fluids
▪ Indication
What is my therapeutic goal??
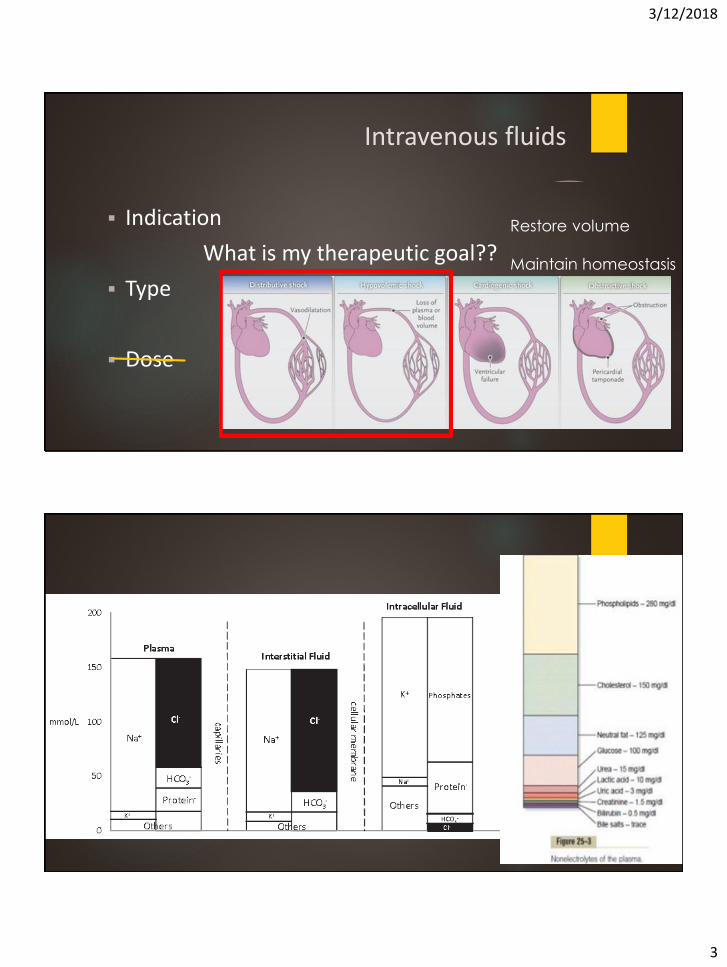
▪ Type
Ideal: close chemical composition to circulating plasma
▪ Dose
Restore volume
Maintain homeostasis
Plasma Composition ▪
3/12/2018
4
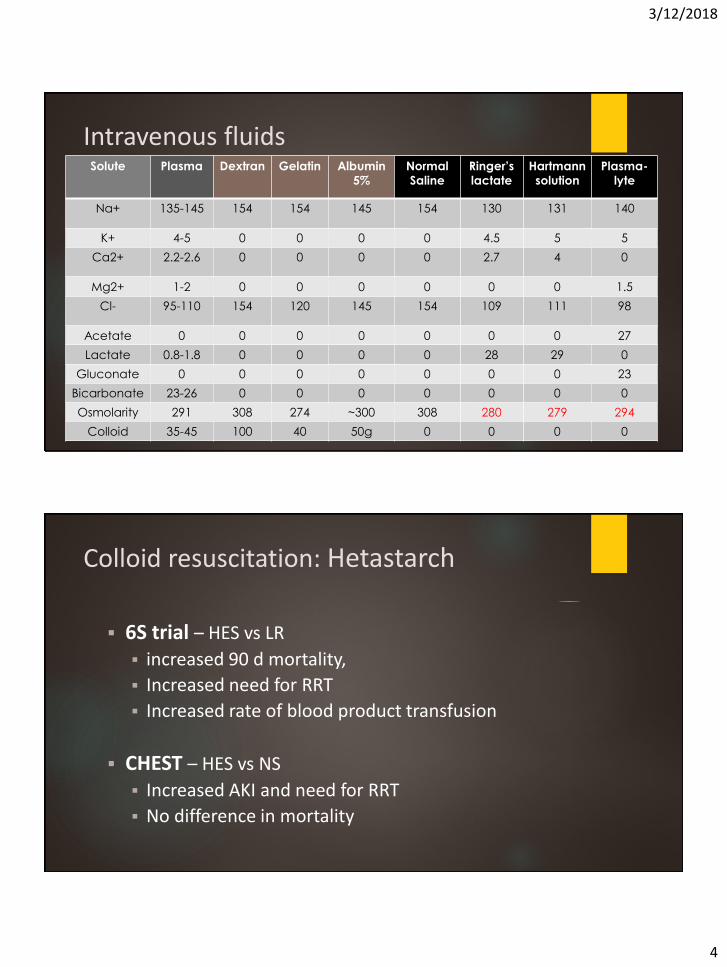
Intravenous fluids Solute Plasma Dextran Gelatin Albumin
5%
Normal
Saline
Ringer’s
lactate
Hartmann
solution
Plasma-
lyte
Na+ 135-145 154 154 145 154 130 131 140
K+ 4-5 0 0 0 0 4.5 5 5
Ca2+ 2.2-2.6 0 0 0 0 2.7 4 0
Mg2+ 1-2 0 0 0 0 0 0 1.5
Cl- 95-110 154 120 145 154 109 111 98
Acetate 0 0 0 0 0 0 0 27
Lactate 0.8-1.8 0 0 0 0 28 29 0
Gluconate 0 0 0 0 0 0 0 23
Bicarbonate 23-26 0 0 0 0 0 0 0
Osmolarity 291 308 274 ~300 308 280 279 294
Colloid 35-45 100 40 50g 0 0 0 0
Colloid resuscitation: Hetastarch
▪ 6S trial – HES vs LR
▪ increased 90 d mortality,
▪ Increased need for RRT
▪ Increased rate of blood product transfusion
▪ CHEST – HES vs NS
▪ Increased AKI and need for RRT
▪ No difference in mortality
3/12/2018
5
Colloid resuscitation: Albumin
▪ SAFE – Albumin vs NS
▪ Albumin better in sepsis
▪ No difference in mortality
▪ CRISTAL – Colloid vs NS
▪ No difference in 28 d mortality
▪ Possible increase in 90 d mortality with colloid
3/12/2018
6
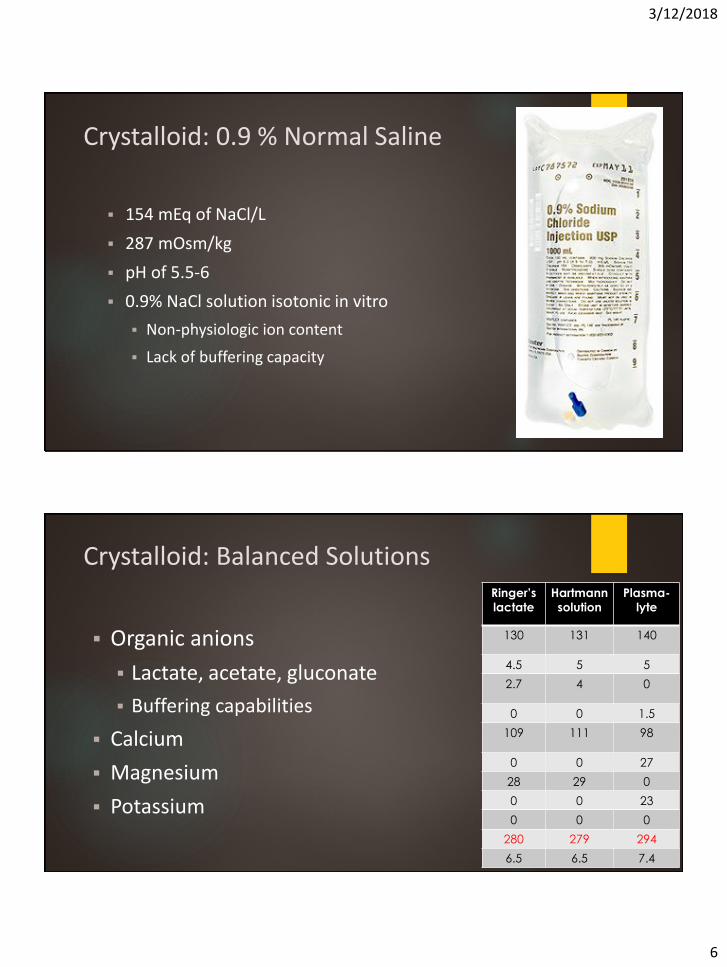
Crystalloid: 0.9 % Normal Saline
▪ 154 mEq of NaCl/L
▪ 287 mOsm/kg
▪ pH of 5.5-6
▪ 0.9% NaCl solution isotonic in vitro
▪ Non-physiologic ion content
▪ Lack of buffering capacity
Crystalloid: Balanced Solutions
▪ Organic anions
▪ Lactate, acetate, gluconate
▪ Buffering capabilities
▪ Calcium
▪ Magnesium
▪ Potassium
Ringer’s
lactate
Hartmann
solution
Plasma-
lyte
130 131 140
4.5 5 5
2.7 4 0
0 0 1.5
109 111 98
0 0 27
28 29 0
0 0 23
0 0 0
280 279 294
6.5 6.5 7.4
3/12/2018
7
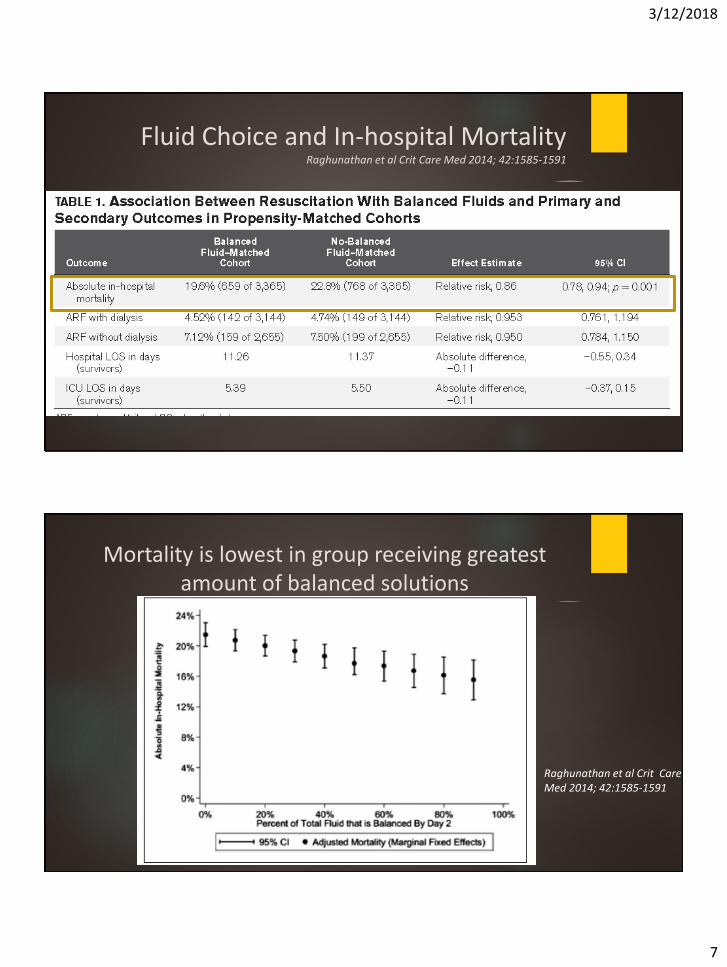
Fluid Choice and In-hospital MortalityRaghunathan et al Crit Care Med 2014; 42:1585-1591
Mortality is lowest in group receiving greatest amount of balanced solutions
Raghunathan et al Crit Care Med 2014; 42:1585-1591
3/12/2018
8
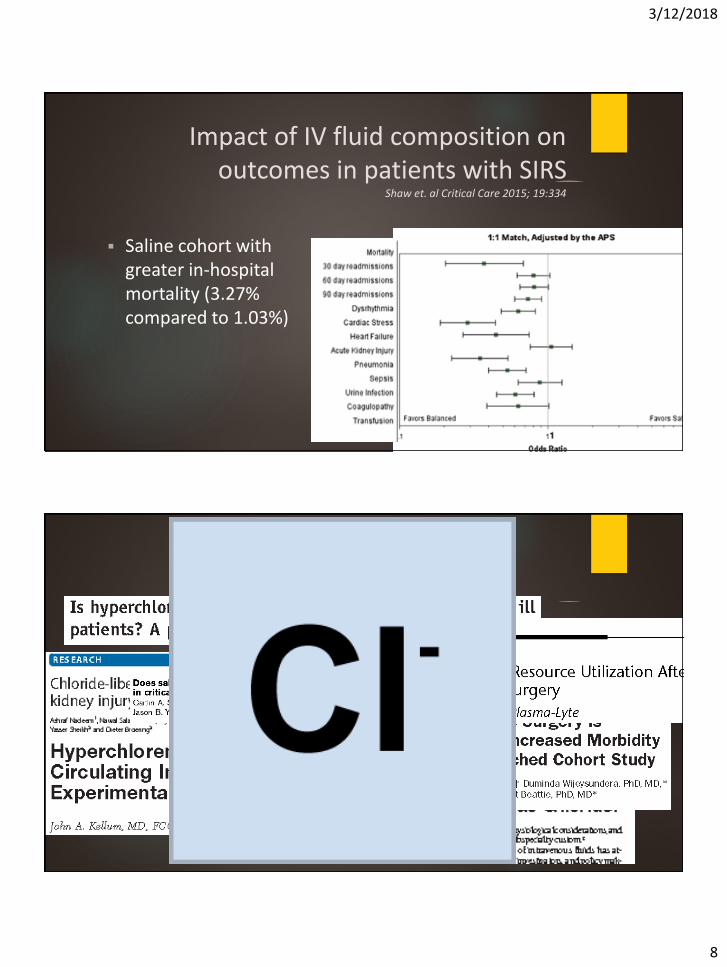
Impact of IV fluid composition on outcomes in patients with SIRS
Shaw et. al Critical Care 2015; 19:334
▪ Saline cohort with greater in-hospital mortality (3.27% compared to 1.03%)
Balanced vs. 0.9 NS
3/12/2018
9
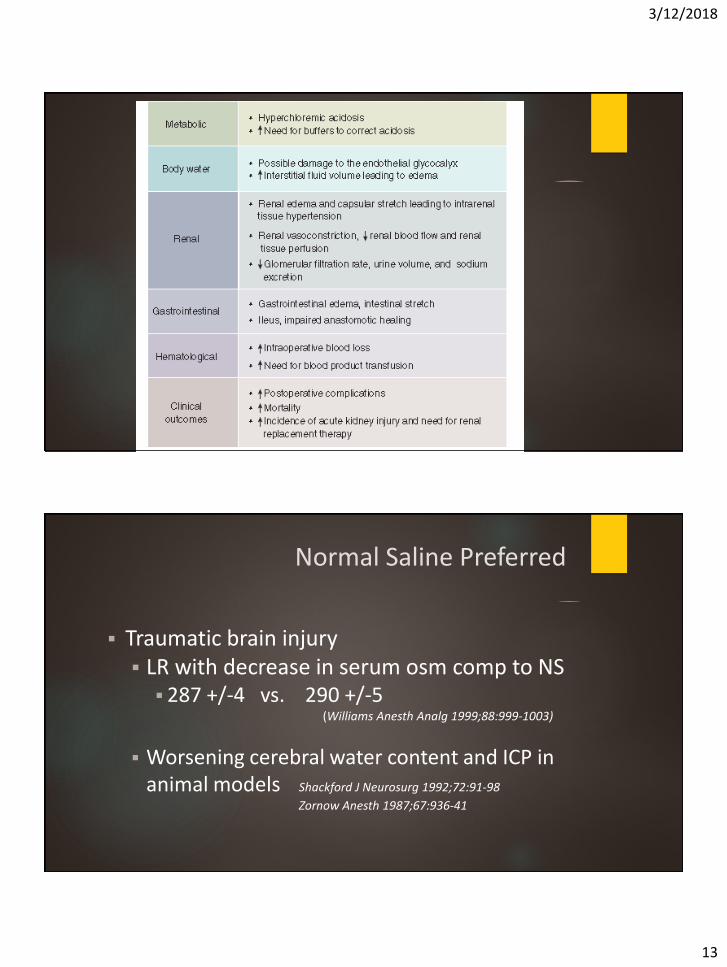
Claims against hyperchloremia
▪ Metabolic Acidosis
▪ Increased inflammatory cytokines
▪ Renal vasoconstriction
▪ Decreased renal blood flow/diuresis/natiuresis
▪ Increased interstitial edema
▪ Possible coagulopathy
Metabolic acidosisInflammatory cytokines
▪ Hyperchloremia with acidosis due to change in strong ion difference
▪ SID=[(Na+K+Mg+Ca) – (Cl+lactate)]
▪ Animal studies correlate increasing hyperchloremia with worsening hemodynamic profile and inflammation
3/12/2018
10
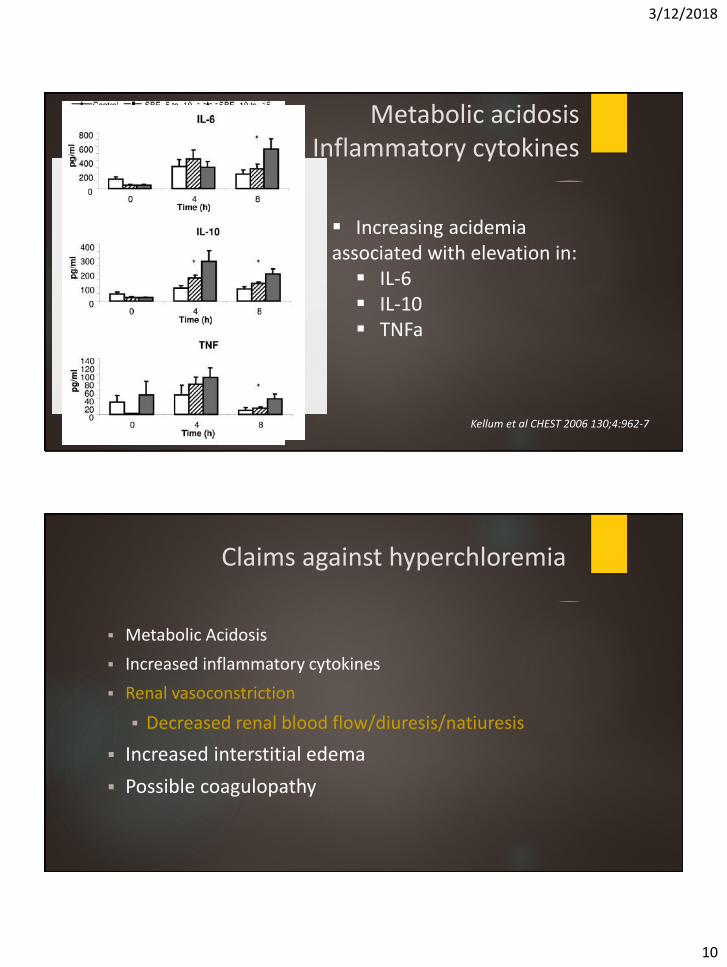
Metabolic acidosisInflammatory cytokines
▪ Increasing acidemiaassociated with elevation in:
▪ IL-6▪ IL-10▪ TNFa
Kellum et al CHEST 2006 130;4:962-7
Claims against hyperchloremia
▪ Metabolic Acidosis
▪ Increased inflammatory cytokines
▪ Renal vasoconstriction
▪ Decreased renal blood flow/diuresis/natiuresis
▪ Increased interstitial edema
▪ Possible coagulopathy
3/12/2018
11
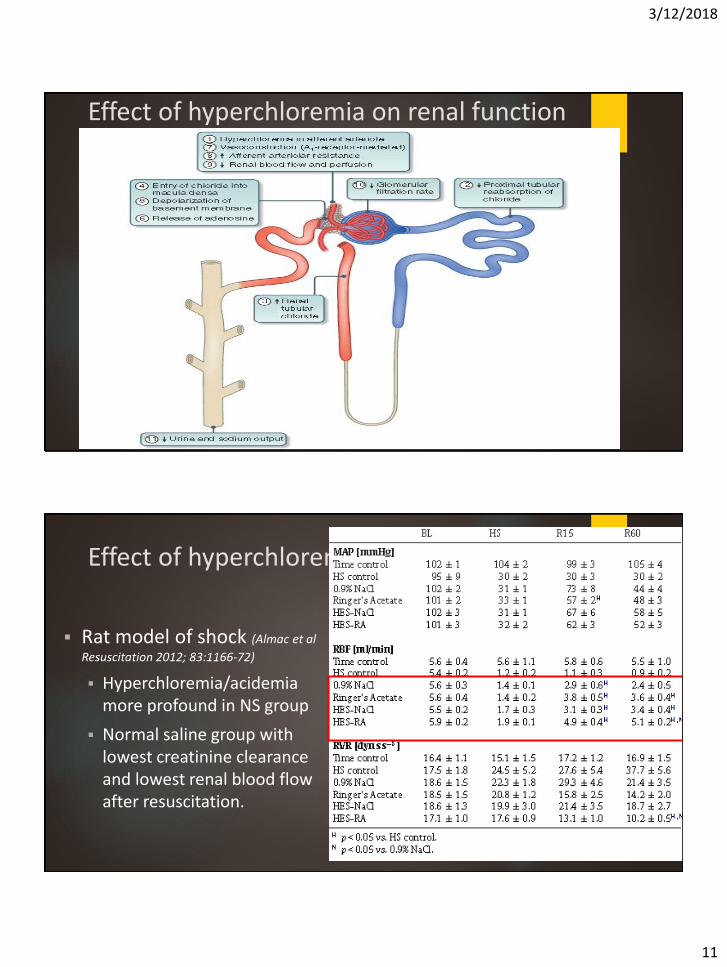
Effect of hyperchloremia on renal function
Effect of hyperchloremia on renal function
▪ Rat model of shock (Almac et al
Resuscitation 2012; 83:1166-72)
▪ Hyperchloremia/acidemiamore profound in NS group
▪ Normal saline group with lowest creatinine clearance and lowest renal blood flow after resuscitation.
3/12/2018
12
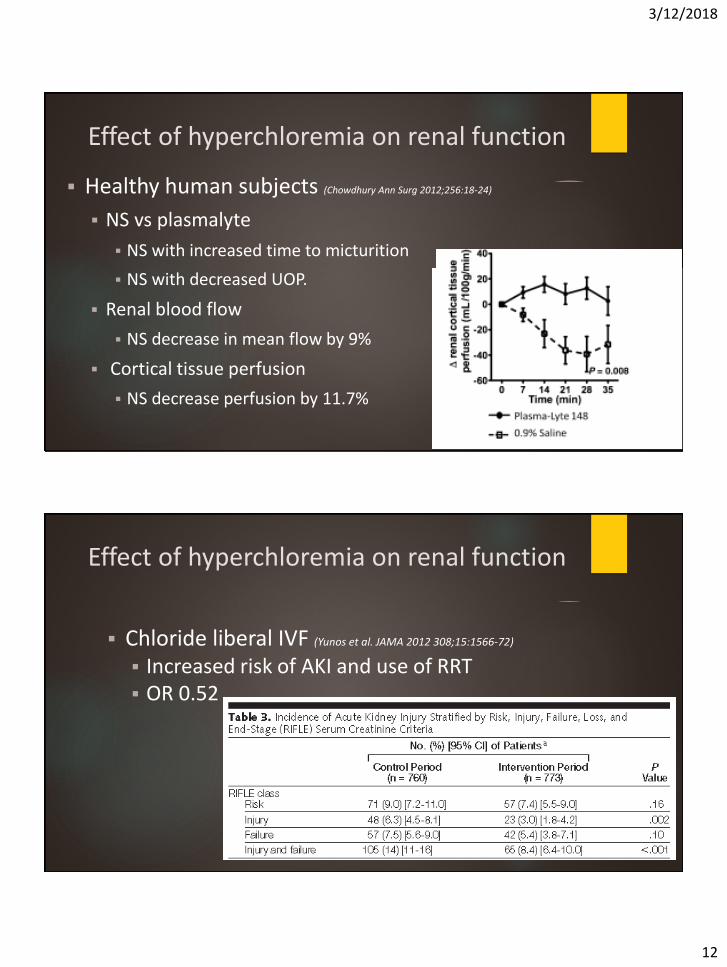
Effect of hyperchloremia on renal function
▪ Healthy human subjects (Chowdhury Ann Surg 2012;256:18-24)
▪ NS vs plasmalyte
▪ NS with increased time to micturition
▪ NS with decreased UOP.
▪ Renal blood flow
▪ NS decrease in mean flow by 9%
▪ Cortical tissue perfusion
▪ NS decrease perfusion by 11.7%
Effect of hyperchloremia on renal function
▪ Chloride liberal IVF (Yunos et al. JAMA 2012 308;15:1566-72)
▪ Increased risk of AKI and use of RRT ▪ OR 0.52
3/12/2018
13
Normal Saline Preferred
▪ Traumatic brain injury▪ LR with decrease in serum osm comp to NS
▪ 287 +/-4 vs. 290 +/-5 (Williams Anesth Analg 1999;88:999-1003)
▪ Worsening cerebral water content and ICP in animal models Shackford J Neurosurg 1992;72:91-98
Zornow Anesth 1987;67:936-41
3/12/2018
14
Summary
▪ Balanced IV fluids are preferred for large volume resuscitation
▪ Hyperchloremia is increasingly shown to be associated with morbidity and mortality
▪ TBI or other risk of ICP should be treated with NS
3/12/2018
15
Use your fluids wisely!
Recommended