270 American Family Physician www.aafp.org/afp Volume 93, Number 4 ◆ February 15, 2016
Anemia, defined as a hemoglobin level two standard deviations below the mean for age, is prevalent in infants and children worldwide. The evaluation of a child with anemia should begin with a thorough history and risk assessment. Characterizing the anemia as microcytic, normocytic, or macrocytic based on the mean corpuscular volume will aid in the workup and management. Microcytic anemia due to iron deficiency is the most common type of anemia in children. The American Academy of Pediatrics and the World Health Organization recommend routine screen-ing for anemia at 12 months of age; the U.S. Preventive Services Task Force found insufficient evidence to assess the benefits vs. harms of screening. Iron deficiency anemia, which can be associated with cognitive issues, is prevented and treated with iron supplements or increased intake of dietary iron. The U.S. Preven-tive Services Task Force found insufficient evidence to recommend screening or treating pregnant women for iron deficiency anemia to improve maternal or neonatal outcomes. Delayed cord clamping can improve iron status in infancy, especially for at-risk populations, such as those who are preterm or small for gestational age. Normocytic anemia may be caused by congenital membranopathies, hemoglobin-opathies, enzymopathies, metabolic defects, and immune-mediated destruction. An initial reticulocyte count is needed to determine bone marrow function. Macrocytic anemia, which is uncommon in children, warrants subsequent evaluation for vitamin B12 and folate deficiencies, hypothyroidism, hepatic disease, and bone marrow dis-orders. (Am Fam Physician. 2016;93(4):270-278. Copyright © 2016 American Academy of Family Physicians.) IL
LUST
RA
TIO
N B
Y J
ENN
IFER
E. F
AIR
MA
N
Iron Deficiency and Other Types of Anemia in Infants and ChildrenMARY WANG, MD, University of California–San Diego, San Diego, California
Worldwide, anemia affects up to one-half of children younger than five years.1 Anemia is defined as a
hemoglobin level that is two standard devia-tions below the mean for age.2,3 After children reach 12 years of age, the hemoglobin norm can be further divided into gender-specific ranges.3 Table 1 lists age-based hemoglobin levels.3,4 Anemia can be categorized as micro-cytic, normocytic, or macrocytic. Microcytic iron deficiency anemia is a common cause of childhood anemia, whereas macrocytic ane-mia is rare in children. Table 2 summarizes the causes of anemia.3,5
EpidemiologyThe World Health Organization reports that the overall rate of infant and childhood (six to 59 months of age) anemia in the United
States in 2011 was low at 6%.6 The exception is in children in low-income families. A 2010 report of data from federally funded pro-grams serving low-income children found that the prevalence of anemia in this popula-tion increased from 13.4% in 2001 to 14.6% in 2010. The highest prevalence (18.2%) was among children 12 to 17 months of age.7
Screening for AnemiaThe American Academy of Pediatrics (AAP) and the World Health Organization recom-mend universal screening for anemia at one year of age. However, the U.S. Preventive Services Task Force (USPSTF) found insuffi-cient evidence to assess the benefits vs. harms of screening.1,2,8 The AAP also recommends selective screening at any age in children with risk factors for anemia, such as feed-ing problems, poor growth, and inadequate
CME This clinical content conforms to AAFP criteria for continuing medical education (CME). See CME Quiz Questions on page 264.
Author disclosure: No rel-evant financial affiliations.
Downloaded from the American Family Physician website at www.aafp.org/afp. Copyright © 2016 American Academy of Family Physicians. For the private, noncom-mercial use of one individual user of the website. All other rights reserved. Contact [email protected] for copyright questions and/or permission requests.

Anemia in Children
dietary iron intake.2 When screening is positive for anemia, follow-up is essential. One study showed that 25% of patients who screened positive for anemia had no docu-mented follow-up testing.9
Initial EvaluationMost infants and children with mild ane-mia do not exhibit overt clinical signs and symptoms. Initial evaluation should include a thorough history, such as questions to determine prematurity, low birth weight, diet, chronic diseases, family history of ane-mia, and ethnic background. A complete blood count is the most common initial diagnostic test used to evaluate for anemia, and it allows for differentiating microcytic, normocytic, and macrocytic anemia based
Table 1. Age-Based Hemoglobin Levels in Children and Adolescents
Age Mean hemoglobin level –2 standard deviations
Birth (term infant) 16.5 g per dL (165 g per L) 13.5 g per dL (135 g per L)
1 month 13.9 g per dL (139 g per L) 10.7 g per dL (107 g per L)
2 months 11.2 g per dL (112 g per L) 9.4 g per dL (94 g per L)
3 to 6 months 11.5 g per dL (115 g per L) 9.5 g per dL (95 g per L)
6 months to 2 years 12 g per dL (120 g per L) 10.5 g per dL (105 g per L)
2 to 6 years 12.5 g per dL (125 g per L) 11.5 g per dL
6 to 12 years 13.5 g per dL 11.5 g per dL
12 to 18 years
Males 14.5 g per dL (145 g per L) 13 g per dL (130 g per L)
Females 14 g per dL (140 g per L) 12 g per dL
Information from references 3 and 4.
Table 2. Causes of Anemia in Children
Age
Type of anemia
Microcytic Normocytic Macrocytic
Neonates Three gene deletion α-thalassemia
Acute blood loss
Isoimmunization (antibody-mediated hemolysis)
Congenital hemolytic anemias (spherocytosis, glucose-6-phosphate dehydrogenase deficiency)
Congenital infections (including parvovirus B19)
Congenital aplasia
Infants and toddlers Iron deficiency anemia
Concurrent infection
Thalassemia
Concurrent infection
Acute blood loss
Iron deficiency anemia*
Sickle cell disease
Red blood cell enzyme defects (glucose- 6-phosphate dehydrogenase deficiency, pyruvate kinase deficiency)
Red blood cell membrane defects (spherocytosis, elliptocytosis)
Acquired hemolytic anemia
Autoimmune hemolytic anemia
Hypersplenism
Transient erythroblastopenia of childhood
Bone marrow disorders (leukemia, myelofibrosis)
Vitamin B12 or folate deficiency
Hypothyroidism
Hypersplenism
Congenital aplasia
Older children and adolescents
Iron deficiency anemia
Anemia of chronic disease
Thalassemia
Acute blood loss
Iron deficiency anemia*
Anemia of chronic disease
Acquired hemolytic anemia
Sickle cell disease
Bone marrow disorders (leukemia, myelofibrosis)
Vitamin B12 or folate deficiency
Hypothyroidism
NOTE: Causes are listed in approximate order of prevalence.
*—Iron deficiency anemia is most commonly microcytic.
Information from references 3 and 5.

Anemia in Children
272 American Family Physician www.aafp.org/afp Volume 93, Number 4 ◆ February 15, 2016
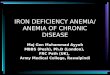
on the mean corpuscular volume. Figure 1 is an algorithm for the evaluation of children with low hemoglobin levels.5
Microcytic Anemia DIAGNOSIS OF IRON DEFICIENCY ANEMIA
Microcytic anemia due to iron deficiency is the most common type of anemia in chil-dren. The U.S. prevalence of iron deficiency anemia in children one to five years of age is estimated to be 1% to 2%.10 A child with microcytic anemia and a history of poor dietary iron intake should receive a trial of iron supplementation and dietary counsel-ing. Iron deficiency anemia is likely if the hemoglobin level increases by more than 1.0 g per dL (10 g per L) after one month of pre-sumptive treatment.
Although iron deficiency anemia is usually microcytic, some patients may have normo-cytic red blood cells.11 Further testing may also be necessary if suspected iron deficiency anemia does not respond to treatment. Fer-ritin measurement is the most sensitive test for diagnosing iron deficiency anemia.2,10 Ferritin is a good reflection of total iron storage and is also the first laboratory index to decline with iron deficiency.3 It may be less accurate in children with infectious or inflammatory conditions because ferritin is also an acute phase reactant.
An elevated red blood cell distribution width index can also be a sensitive test to dif-ferentiate iron deficiency anemia from other types of microcytic anemia if ferritin and iron studies are not available.12,13
Evaluation of Low Hemoglobin Levels in ChildrenLow hemoglobin level
Confirm level and add indices; evaluate MCV
Low MCV Normal MCV High MCV
Microcytic anemia Normocytic anemia (see Figure 2)
Macrocytic anemia (see Figure 3)
Is anemia mild, and are history and indices consistent with iron deficiency anemia?
NoYes
Treat presumptively; retest in one month
Perform iron studies, hemoglobin electrophoresis, lead level measurementHemoglobin increased by > 1.0 g per dL (10 g per L)?
Yes
No
Diagnosis confirmed; counsel about cow’s milk consumption; and continue treatment for an additional one to two months
Iron deficiency anemia (not responsive to oral therapy)
Anemia of chronic disease Thalassemia No cause found
Test for gastrointestinal bleeding; refer to pediatric gastroenterologist
Treat underlying disease Counsel or refer as needed
Refer to pediatric hematologist
Figure 1. Algorithm for the evaluation of low hemoglobin levels in children. (MCV = mean corpuscular volume.)
Adapted with permission from Janus J, Moerschel SK. Evaluation of anemia in children. Am Fam Physician. 2010;81(12):1468.

February 15, 2016 ◆ Volume 93, Number 4 www.aafp.org/afp American Family Physician 273
PREVENTION OF IRON DEFICIENCY ANEMIA
During Pregnancy and Delivery. Up to 42% of pregnant women worldwide will have anemia, with a prevalence of 6% in North America.1 The iron requirement increases with each trimester and should be supported by higher maternal iron intake.14 Between 60% and 80% of the iron storage in a new-born occurs during the third trimester,2,14 but it is unclear whether treatment of mater-nal anemia prevents anemia in newborns and infants. The USPSTF found insuffi-cient evidence to recommend screening for or treating iron deficiency anemia in preg-nant women to improve maternal or neo-natal outcomes.15 Although two Cochrane reviews found that maternal hemoglobin levels improve with antepartum iron supple-mentation, studies have not demonstrated statistically significant benefits in clinical outcomes (e.g., low birth weight, preterm birth, infection, postpartum hemorrhage) for mothers or newborns.16,17
Delayed umbilical cord clamping (approx-imately 120 to 180 seconds after delivery) is associated with improved iron status (fer-ritin levels) at two to six months of age.18,19
This benefit may be especially important in those vulnerable to iron deficiency, such as infants who were premature or small for gestational age. A Cochrane review looking at the effects of the timing of cord clamp-ing during preterm births showed a reduc-tion of blood transfusions when clamping was delayed (24% vs. 36%).20 The effects of delayed cord clamping do not appear to per-sist beyond the first 12 months.21
Iron Supplementation During Infancy. Iron is the most common single-nutrient defi-ciency. Preterm infants (born at less than 37 weeks’ gestation) who are exclusively breast-fed should receive 2 mg per kg per day of
elemental iron supplementation from one to 12 months of age,2 except for those who have had multiple blood transfusions. In healthy full-term infants, iron storage from in utero is adequate for the first four to six months of life.22 The AAP recommends that full-term, exclusively breastfed infants start 1 mg per kg per day of elemental iron supplementa-tion at four months of age until appropri-ate iron-containing foods are introduced.2,3 Table 3 includes daily iron supplementation and requirements for children.2,3,5 Various oral iron formulations and dosing for supple-mentation and treatment of anemia are listed in Table 4.3 Formula-fed infants often receive adequate amounts of iron (average formula contains 10 to 12 mg per L of iron) and thus rarely require further supplementation.2
Ideally, the estimated 7-mg daily iron requirement for children one to three years of age should be met through consump-tion of iron-rich foods.2 Consumption of large quantities of non–iron-fortified cow’s
Table 3. Elemental Iron Supplementation or Requirement in Children
Age Iron supplementation or requirement
Preterm (< 37 weeks’ gestation) infants: 1 to 12 months
2 mg per kg per day supplementation if exclusively breastfed
1 mg per kg per day supplementation if using iron-fortified formula
Term infants: 4 to 6 months to 12 months
1 mg per kg per day supplementation if exclusively breastfed
Supplementation not needed if using iron-fortified formula
Toddlers 1 to 3 years Requires 7 mg per day; modify diet and/or supplement if anemic
Children 4 to 8 years Requires 10 mg per day; modify diet and/or supplement if anemic
Information from references 2, 3, and 5.
Table 4. Oral Iron Formulations and Dosing
Formulation Dosing (elemental iron)
Ferrous fumarate Tablet: 90 (29.5) mg, 324 (106) mg, 325 (106) mg, 456 (150) mg
Ferrous gluconate Tablet: 240 (27) mg, 256 (28) mg, 325 (36) mg
Ferrous sulfate Drops and oral solution: 75 (15) mg per mL
Elixir and liquid: 220 (44) mg per 5 mL
Syrup: 300 (60) mg per 5 mL
Tablet: 300 (60) mg, 324 (65) mg, 325 (65) mg
Extended-release tablets: 140 (45) mg, 160 (50) mg, 325 (65) mg
Polysaccharide-iron complex and ferrous bisglycinate chelate
Capsule: elemental iron (50 mg, 150 mg with or without 50 mg vitamin C)
Elixir: elemental iron (100 mg per 5 mL)
Information from reference 3.

Anemia in Children
274 American Family Physician www.aafp.org/afp Volume 93, Number 4 ◆ February 15, 2016
milk increases the risk of iron deficiency.23 Although iron supplementation may achieve more significant improvements in hemoglo-bin concentration, children are more likely to tolerate iron-fortified foods.24 Table 5 lists common childhood foods and their elemen-tal iron content.2 If achieving daily iron sup-plementation is difficult, intermittent iron supplementation still improves hemoglobin concentration and reduces the risk of iron deficiency.25
COGNITIVE ISSUES WITH IRON DEFICIENCY ANEMIA
Iron is important for the neurologic devel-opment of infants and children. Iron is required for proper myelinization of neu-rons, neurogenesis, and differentiation of brain cells that can affect sensory systems, learning, memory, and behavior.2,26-29 Iron is also a cofactor for enzymes that synthesize neurotransmitters.26,27
A landmark study of Costa Rican chil-dren concluded that iron deficiency anemia increases the risk of long-lasting develop-mental disadvantages.30 However, whether iron supplementation can affect psycho-motor development or cognitive function in children is unclear. A Cochrane review concluded that there is no evidence that iron supplementation improves psychomotor or
cognitive development in young children with iron deficiency anemia after 30 days of treatment.31 Furthermore, a systematic review showed that iron supplementation in children who were iron deficient but nonane-mic did not positively influence developmen-tal scores at one to five years of age.32 Thus, screening for iron deficiency in nonanemic infants is not recommended.1,2 A recent sys-tematic review for the USPSTF found no studies showing an association between iron supplementation and clinical outcomes in a population relevant to the United States.33
THALASSEMIA
Thalassemia, a hemoglobinopathy with an α-globin or β-globin production defect, should be considered in a child with micro-cytic anemia if the history or laboratory studies are inconsistent with iron deficiency. α-Thalassemia occurs most often in persons of African and Southeast Asian descent, and β-thalassemia is most common in persons of Mediterranean, African, and Southeast Asian descent.12,34 Because of the presence of hemoglobin F at birth, newborns with thal-assemia are likely to be asymptomatic until hemoglobin A becomes predominant at six months of age.34 The Mentzer index (mean corpuscular volume/red blood cell count) uses the complete blood count to differenti-ate thalassemia from iron deficiency anemia. A Mentzer index of less than 13 suggests thalassemia, and an index of more than 13 suggests iron deficiency.5,12,34
Thalassemia can be confirmed using hemoglobin electrophoresis. Patients with one or two α-gene deletions (silent carrier or trait) may be asymptomatic with nor-mal hemoglobin electrophoresis, whereas patients with three α-gene deletions (hemoglobin H disease) will have moder-ate to severe anemia. The presence of four α-gene deletions (hemoglobin Bart’s or α-thalassemia major) is usually incom-patible with neonatal survival.3,34 Infants and children with β-thalassemia trait or β-thalassemia minor may have increased hemoglobin A2 and hemoglobin F on elec-trophoresis, with asymptomatic, mild ane-mia. Those with β-thalassemia intermedia
Table 5. Iron Content in Common Foods
Food (serving size)Amount of elemental iron (mg)
Soybeans: cooked (1/2 cup) 4.4
Lentils: cooked (1/2 cup) 3.3
Spinach: cooked/boiled, drained (1/2 cup) 3.2
Beef: cooked (3 oz) 2.5
Beans (lima, navy, kidney, pinto): cooked (1/2 cup) 1.8 to 2.2
Baby food brown rice cereal: dry (1 tbsp) 1.8
Baby food green beans (6 oz) 1.8
Baby food oatmeal cereal: dry (1 tbsp) 1.6
Turkey and chicken: dark meat (3 oz) 1.1 to 2.0
Baby food lamb or chicken (2.5 oz) 1.0 to 1.2
Baby food peas (3.4 oz) 0.9
Information from reference 2.

Anemia in Children
February 15, 2016 ◆ Volume 93, Number 4 www.aafp.org/afp American Family Physician 275
or major usually have moderate to severe anemia complications, including hyper-splenism, endocrinopathies, cardiac compli-cations, and hypercoagulopathy due to iron overload from repeated transfusions.34
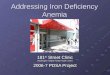
Normocytic AnemiaIron deficiency anemia and acute blood loss are the most common causes of nor-mocytic anemia in infants and children. Evaluation of normocytic anemia (Figure 2) starts with a history, reticulocyte count, and peripheral blood smear.5 A high reticulo-cyte count indicates increased red blood cell turnover. A high reticulocyte count along with laboratory markers of hemolysis (i.e., increased bilirubin, increased lactate dehy-drogenase, and decreased haptoglobin) may help confirm hemolytic anemia.3 Hemolytic anemia has many causes, including congeni-tal membranopathies, hemoglobinopathies,
enzymop athies, metabolic defects, and immune-mediated destruction.3,35 Other testing, such as an osmotic fragility test for hereditary spherocytosis and a glucose-6-phosphate dehydrogenase assay to check for a deficiency, may also be useful.3,36
Sickle cell disease, caused by a genetic defect in the β-globin, is a hemoglobinopa-thy that results in normocytic anemia. In the United States, it is typically diagnosed through newborn screening.3,37 A review of the management of sickle cell anemia was recently published in American Family Physician.38
A low reticulocyte count with normo-cytic anemia in infants and children sug-gests impaired bone marrow function. This can be due to anemia of chronic inflamma-tion; acquired red blood cell aplasias; and bone marrow disorders, such as leukemia.5 Acquired aplasias can have an infectious
Evaluation of Normocytic Anemia in ChildrenNormocytic anemia
Review patient history for underlying disease; obtain reticulocyte count and peripheral blood smear
Reticulocyte count low (indicating bone marrow hypofunction)
Reticulocyte count high (indicating increased red blood cell turnover)
Perform laboratory testing for hemolysis (bilirubin, lactate dehydro-genase, and haptoglobin levels)Medical disease
suspectedUnderlying inflammation
Abnormal smear
Consider iron studies for diagnosis of anemia of chronic disease
Consider bone marrow disorders (e.g., leukemia, myelofibrosis)
Perform laboratory testing for renal, hepatic, or thyroid disease
Cause unknownRefer to pediatric hematologist
Positive Negative
Consider enzyme defects, autoimmune disorders, hemoglobinopathies, or membrane disorders; test accordingly
Consider blood loss, hypersplenism, or mixed disorder
Cause unknown
Figure 2. Algorithm for the evaluation of normocytic anemia in children.
Adapted with permission from Janus J, Moerschel SK. Evaluation of anemia in children. Am Fam Physician. 2010;81(12):1469.

276 American Family Physician www.aafp.org/afp Volume 93, Number 4 ◆ February 15, 2016
cause, such as parvovirus B19 or transient erythroblastopenia of childhood.3,5 Tran-sient erythroblastopenia of childhood usu-ally resolves spontaneously within four to eight weeks3,5,39 with no recurrence or sub-sequent hematologic disorders at 15 years of follow-up.39 If bone marrow disorders are suspected, peripheral blood smear and bone marrow aspiration are indicated with a referral to a pediatric hematologist.
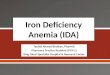
Macrocytic AnemiaThe evaluation of macrocytic anemia in children (Figure 3) begins with examination of a peripheral blood smear for hyperseg-mented neutrophils, which indicate mega-loblastic anemia.5 If megaloblastic anemia is shown, folate and vitamin B12 measure-ments are indicated. Low vitamin B12 levels may be nutrition/absorption related or con-genital and have neurologic consequences,
SORT: KEY RECOMMENDATIONS FOR PRACTICE
Clinical recommendationEvidence rating References
The American Academy of Pediatrics and the World Health Organization recommend universal screening for anemia at one year of age. However, the U.S. Preventive Services Task Force found insufficient evidence to assess the benefits vs. harms of screening.
C 1, 2, 8
Although iron deficiency anemia is associated with cognitive delays in children, it is unclear if iron supplementation improves cognitive outcomes.
C 2, 26-29
Screening for iron deficiency in nonanemic infants and children is not recommended.
A 1, 2
A = consistent, good-quality patient-oriented evidence; B = inconsistent or limited-quality patient-oriented evidence; C = consensus, disease-oriented evidence, usual practice, expert opinion, or case series. For information about the SORT evidence rating system, go to http://www.aafp.org/afpsort.
Evaluation of Macrocytic Anemia in ChildrenMacrocytic anemia
Order peripheral blood smear to evaluate for hypersegmented neutrophils (indicating megaloblastic anemia)
Megaloblastic anemia
Test folate and vitamin B12 levels
Vitamin B12 level low Folate level low Both levels low or normal
Consider treatment if clinically appropriate (or refer to a pediatric hematologist for further evaluation)
Refer to pediatric hematologist for consideration of bone marrow disorders
Nonmegaloblastic anemia
Obtain reticulocyte count
Low High
Evaluate for bone marrow disorders, hypothyroidism, or hepatic disease
Evaluate for hemolysis or hemorrhage
Cause unknownNo improvement
Figure 3. Algorithm for the evaluation of macrocytic anemia in children.
Adapted with permission from Janus J, Moerschel SK. Evaluation of anemia in children. Am Fam Physician. 2010;81(12):1470.

Anemia in Children
February 15, 2016 ◆ Volume 93, Number 4 www.aafp.org/afp American Family Physician 277
ranging from growth retardation to seizure disorders.40 Clinicians should have a low threshold to refer these patients to a pediat-ric hematologist. Nonmegaloblastic causes of macrocytic anemia in children include hemolysis, hemorrhage, bone marrow dis-orders, hypothyroidism, and hepatic disease.
Data Sources: I searched PubMed, the Cochrane data-base, Essential Evidence Plus, and the National Guideline Clearinghouse using the key words anemia in children, anemia in infants, iron deficiency, microcytic anemia, normocytic anemia, macrocytic anemia, and hemolytic anemia. We included publication dates between 1995 and October 2015. Search dates: July and October 2015.
This review updates a previous article on this topic by Janus and Moerschel.5
The Author
MARY WANG, MD, is an associate professor of family medicine and public health at the University of California–San Diego.
Address correspondence to Mary Wang, MD, University of California–San Diego, 9333 Genesee Ave., #200, San Diego, CA 92121 (e-mail: [email protected]). Reprints are not available from the author.
REFERENCES
1. World Health Organization. Worldwide prevalence of anaemia 1993-2005. 2008. http://whqlibdoc.who.int/publications/2008/978 924 1596 657 _eng.pdf. Accessed October 27, 2015.
2. Baker RD, Greer FR; Committee on Nutrition American Academy of Pediatrics. Diagnosis and prevention of iron deficiency and iron-deficiency anemia in infants and young children (0-3 years of age). Pediatrics. 2010;126(5):1040-1050.
3. Flerlage J, Engorn B, eds. The Harriet Lane Handbook: A Manual for Pediatric House Officers. 20th ed. Philadel-phia, Pa.: Saunder/Elsevier; 2015:305.
4. Short MW, Domagalski JE. Iron deficiency anemia: evaluation and management. Am Fam Physician. 2013;87(2):98-104.
5. Janus J, Moerschel SK. Evaluation of anemia in children. Am Fam Physician. 2010;81(12):1462-1471.
6. World Health Organization. The global preva-lence of anaemia in 2011. http://apps.who.int/iris/bitstream/10665/177094/1/9789 241 564 960 _eng.pdf?ua=1. Accessed November 16, 2015.
7. Dalenius K, Borland E, Smith B, Polhamus B, Grummer-Strawn L. Centers for Disease Control and Prevention. Pediatric Nutrition Surveillance 2010 Report. 2012. http: / /www.cdc.gov /pednss /pdfs / PedNSS_2010_Summary.pdf. Accessed October 27, 2015.
8. Siu AL; U.S. Preventive Services Task Force. Screening for iron deficiency anemia in young children: USP-STF recommendation statement. Pediatrics. 2015; 136(4):746-752.
9. Biondich PG, Downs SM, Carroll AE, et al. Shortcomings
in infant iron deficiency screening methods. Pediatrics. 2006;117(2):290-294.
10. U.S. Preventive Services Task Force. Iron deficiency anemia in young children: screening, September 2015. ht tp: / /www.uspreventiveser v icestaskforce.org / Page/Document/UpdateSummaryFinal/iron- deficiency- anemia-in-young-children-screening?ds=1&s=Iron%20 deficiency%20anemia%20screening%29. Accessed Jan-uary 11, 2016.
11. Bermejo F, García-López S. A guide to diagnosis of iron deficiency and iron deficiency anemia in digestive dis-eases. World J Gastroenterol. 2009;15(37):4638-4643.
12. Jain S, Kamat D. Evaluation of microcytic anemia. Clin Pediatr (Phila). 2009;48(1):7-13.
13. Sazawal S, Dhingra U, Dhingra P, et al. Efficiency of red cell distribution width in identification of children aged 1-3 years with iron deficiency anemia against traditional hematological markers. BMC Pediatr. 2014;14:8.
14. Scholl TO. Maternal iron status: relation to fetal growth, length of gestation, and iron endowment of the neo-nate. Nutr Rev. 2011;69 (suppl 1): S23-S29.
15. U.S. Preventive Services Task Force. Iron deficiency anemia in pregnant women: screening and supple-mentation. September 2015. http://www.uspreventive servicestaskforce.org/Page/Document/UpdateSumma-ryFinal /iron-deficiency-anemia-in-pregnant-women-screening-and-supplementation?ds=1&s= Iron%20deficiency%20anemia%20screening%29. Accessed January 11, 2016.
16. Peña-Rosas JP, Viteri FE. Effects and safety of preven-tive oral iron or iron+folic acid supplementation for women during pregnancy. Cochrane Database Syst Rev. 2009;(4):CD004736.
17. Pena-Rosas JP, De-Regil LM, Garcia-Casal MN, Dowswell T. Daily oral iron supplementation during pregnancy. Cochrane Database Syst Rev. 2015;(7):CD004736.
18. Hutton EK, Hassan ES. Late vs early clamping of the umbilical cord in full-term neonates: systematic review and meta-analysis of controlled trials. JAMA. 2007;297(11):1241-1252.
19. Andersson O, Hellström-Westas L, Andersson D, Domellöf M. Effect of delayed versus early umbilical cord clamping on neonatal outcomes and iron sta-tus at 4 months: a randomised controlled trial. BMJ. 2011;343:d7157.
20. Rabe H, Diaz-Rossello JL, Duley L, Dowswell T. Effect of timing of umbilical cord clamping and other strategies to influence placental transfusion at preterm birth on maternal and infant outcomes. Cochrane Database Syst Rev. 2012;(8):CD003248.
21. Andersson O, Domellöf M, Andersson D, Hellström-Westas L. Effect of delayed vs early umbilical cord clamping on iron status and neurodevelopment at age 12 months: a randomized clinical trial. JAMA Pediatr. 2014;168(6):547-554.
22. Uijterschout L, Vloemans J, Rövekamp-Abels L, Feitsma H, van Goudoever JB, Brus F. The influences of factors associated with decreased iron supply to the fetus dur-ing pregnancy on iron status in healthy children aged 0.5 to 3 years. J Perinatol. 2014;34(3):229-233.
23. Brotanek JM, Halterman JS, Auinger P, Flores G, Weitzman M. Iron deficiency, prolonged bottle-feeding, and racial/ethnic disparities in young children. Arch Pediatr Adolesc Med. 2005;159(11):1038-1042.
24. Rosado JL, González KE, Caamaño Mdel C, García OP,

Anemia in Children
278 American Family Physician www.aafp.org/afp Volume 93, Number 4 ◆ February 15, 2016
Preciado R, Odio M. Efficacy of different strategies to treat anemia in children: a randomized clinical trial. Nutr J. 2010;9:40-50.
25. De-Regil LM, Jefferds ME, Sylvetsky AC, Dowswell T. Intermittent iron supplementation for improving nutri-tion and development in children under 12 years of age. Cochrane Database Syst Rev. 2011; (12): CD009085.
26. Iannotti LL, Tielsch JM, Black MM, Black RE. Iron sup-plementation in early childhood. Am J Clin Nutr. 2006; 84(6): 1261-1276.
27. Beard JL. Why iron deficiency is important in infant development. J Nutr. 2008;138(12):2534-2536.
28. Domellöf M. Iron requirements in infancy. Ann Nutr Metab. 2011; 59(1): 59-63.
29. Domellöf M, Braegger C, Campoy C, et al.; ESPGHAN Committee on Nutrition. Iron requirements of infants and toddlers. J Pediatr Gastroenterol Nutr. 2014; 58(1):119-129.
30. Lozoff B, Jimenez E, Wolf AW. Long-term developmen-tal outcome of infants with iron deficiency. N Engl J Med. 1991;325(10):687-694.
31. Wang B, Zhan S, Gong T, Lee L. Iron therapy for improving psychomotor development and cognitive function in children under the age of three with iron deficiency anaemia. Cochrane Database Syst Rev. 2013; (6):CD001444.
32. Abdullah K, Kendzerska T, Shah P, Uleryk E, Par-kin PC. Efficacy of oral iron therapy in improving the developmental outcome of pre-school children with
non-anaemic iron deficiency: a systematic review. Pub-lic Health Nutr. 2013;16(8):1497-1506.
33. McDonagh MS, Blazina I, Dana T, Cantor A, Bougat-sos C. Screening and routine supplementation for iron deficiency anemia: a systematic review. Pediatrics. 2015;135(4):723-733.
34. Muncie HL Jr, Campbell J. Alpha and beta thalassemia. Am Fam Physician. 2009;80(4):339-344.
35. Murray NA, Roberts IA. Haemolytic disease of the newborn. Arch Dis Child Fetal Neonatal Ed. 2007; 92(2):F83-F88.
36. Christensen RD, Henry E. Hereditary spherocyto-sis in neonates with hyperbilirubinemia. Pediatrics. 2010;125(1):120-125.
37. Quinn CT. Sickle cell disease in childhood: from new-born screening through transition to adult medical care. Pediatr Clin North Am. 2013; 60(6):1363-1381.
38. Yawn BP, Joylene JS. Management of sickle cell disease: recommendations from the 2014 expert panel report. Am Fam Physician. 2015; 92(12):1069-1076.
39. van den Akker M, Dror Y, Odame I. Transient erythro-blastopenia of childhood is an underdiagnosed and self-limiting disease. Acta Paediatr. 2014;103(7):e288-e294.
40. Demir N, Koc A, Üstyol L, Peker E, Abuhandan M. Clinical and neurological findings of severe vitamin B12 deficiency in infancy and importance of early diag-nosis and treatment. J Paediatr Child Health. 2013; 49(10):820-824.
Recommended