#IGOffenderHealth17
James Bamford
Team Manager
BGSW (Bristol, Gloucestershire,
Somerset, Wiltshire) CRC
Probation
and
Dr Sue SmithSpeech & Language Therapist and
Professional Lead for Autism in Swindon
AWP

Understanding Autism Project -Developing an effective approach to
supporting people with Autism in Criminal Justice Services
Dr Sue Smith- Professional Lead for Autism
James Bamford- Probation Team Manager

Today’s purpose
• Briefly explain what autism is, and why we are concerned about people with autism in the criminal justice system
• Describe our project
• Provide an idea of the adaptations that could be made for people with autism in criminal justice services

What is an Autism Spectrum Condition? (ASC)
• Autism is a condition: affects the way a person sees the world, processes information and interacts with people.
• Autism is a different way of thinking, that someone will have had all their life
• Terms like Asperger Syndrome, High Functioning Autism, Classical Autism all describe different presentations of an Autism Spectrum Condition

A few facts
• Autism is NOT a mental health condition
• Autism is NOT a learning disability
• People with Autism can have both learning disability and mental health conditions
• More than 50% of people with autism do NOT have a learning disability (Asperger Syndrome)
• People with autism are at greater risk of developing a mental health condition

Prevalence in Criminal Justice System
• At least as high as in the ordinary population approximately 1% of population (King and Murphy 2014)
• In high secure settings is known to be overrepresented- 4% of population.
• Smaller scale studies (Bates 2017) and clinical experience suggest general CJS nearer 4%

Specific Issues in CJS for people with autism
• Poor victim empathy- harder to see other person’s view (not lack of caring)
• Poor social deception-e.g. less able to pretend to be ‘sorry’ or see why this makes sense
• Intense focus- e.g. cannot move on from an issue and read wider situation
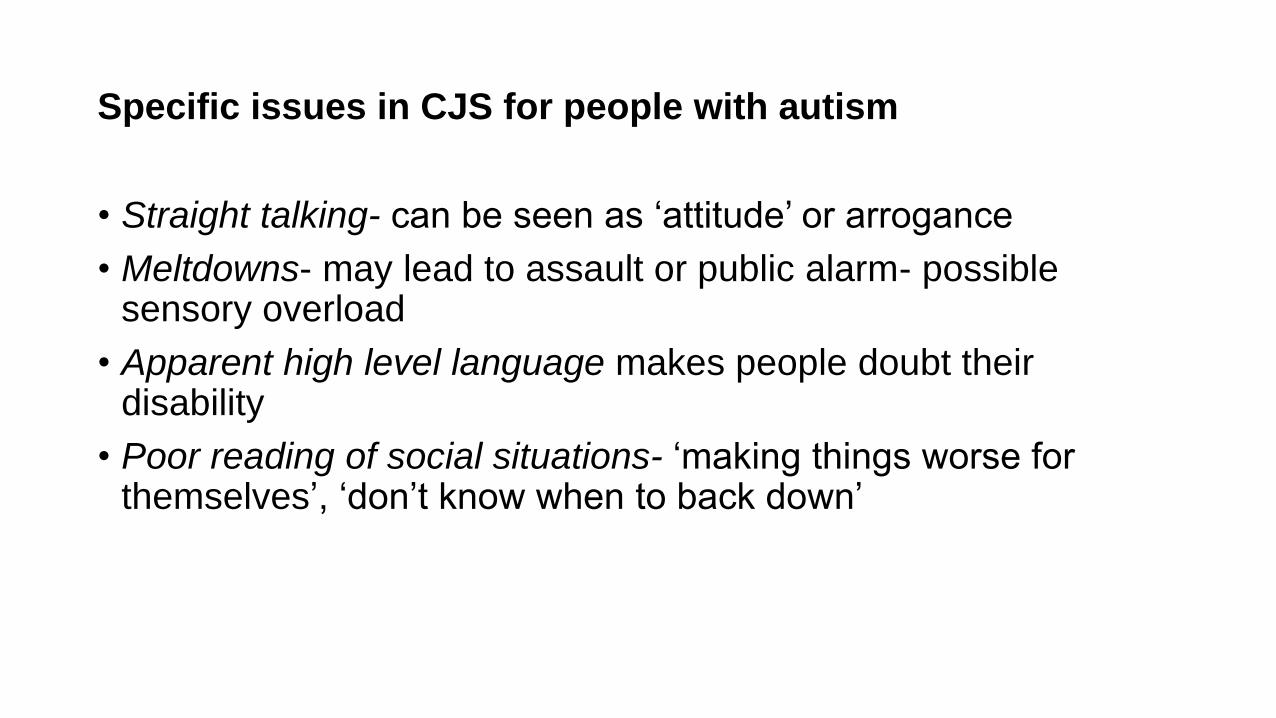
Specific issues in CJS for people with autism
• Straight talking- can be seen as ‘attitude’ or arrogance
• Meltdowns- may lead to assault or public alarm- possible sensory overload
• Apparent high level language makes people doubt their disability
• Poor reading of social situations- ‘making things worse for themselves’, ‘don’t know when to back down’

What might help?
• Clearer less ambiguous language
• Use of visual supports
• Environmental adaptations
• Communication tools- Talking Mats, Social Stories, Comic Strip Conversations
• Linking to local health and social care support services
• Advocating in mental health services

What do we do?
• Provide high quality, tailored awareness training
• Consultation and support to staff and assessment and intervention for service users
• Direction to statutory services and local resources

What do we do?
• Currently funded by Working Links to work in BGSW area (includes Wiltshire probation)
• Open to commissioning from other CJS services

Outcomes in Swindon Probation
• Fifteen service users with a diagnosis of autism. The rate of referral is increasing
• Three service users with learning disability, language disorder or other neurodevelopmental issues
• Over 200 staff trained
• Over 60 percent of staff attending training feeling that they had made direct practice changes for people with ASD

Outcomes in Swindon Probation
• Screening tools used routinely in service and a highlighted area in supervision
• Staff making adaptations that benefit service users with communication challenges, with and without autism
• Poor staff awareness of the autism alert card has now become excellent staff awareness

Any questions?
• Thanks for listening
For further information please contact
Dr Sue Smith on
Or
James Bamford on

#IGOffenderHealth17
Oneal ThomasHealthcare Manager
HM/YOI Feltham

Effectively Determining the Health Needs of Youth Offenders
Oneal Thomas
Head of Healthcare HM YOI Feltham

Social Demographics
• Young people 15-17 and young adults aged 18- 21
• Total population 535
• Both remand and sentenced prisoners
• Predominantly from the London area
• 70% of the YP’s & YA’s identify themselves as coming from a BME background
• Gang affiliation: 45 gangs with an active presence within the establishment.

Joint Enterprise Healthcare & Establishment
Project Board
Senior Management
Team
Risk & Performance
Meeting
Medicine Management
Meeting
Clinical Governance
Regional Public Health
Meeting
Patient Care

Integrated Service Dimensions
Integrated Healthcare
Primary Care
Mental Health
Inpatient Care
Substance Misuse
Pharmacy
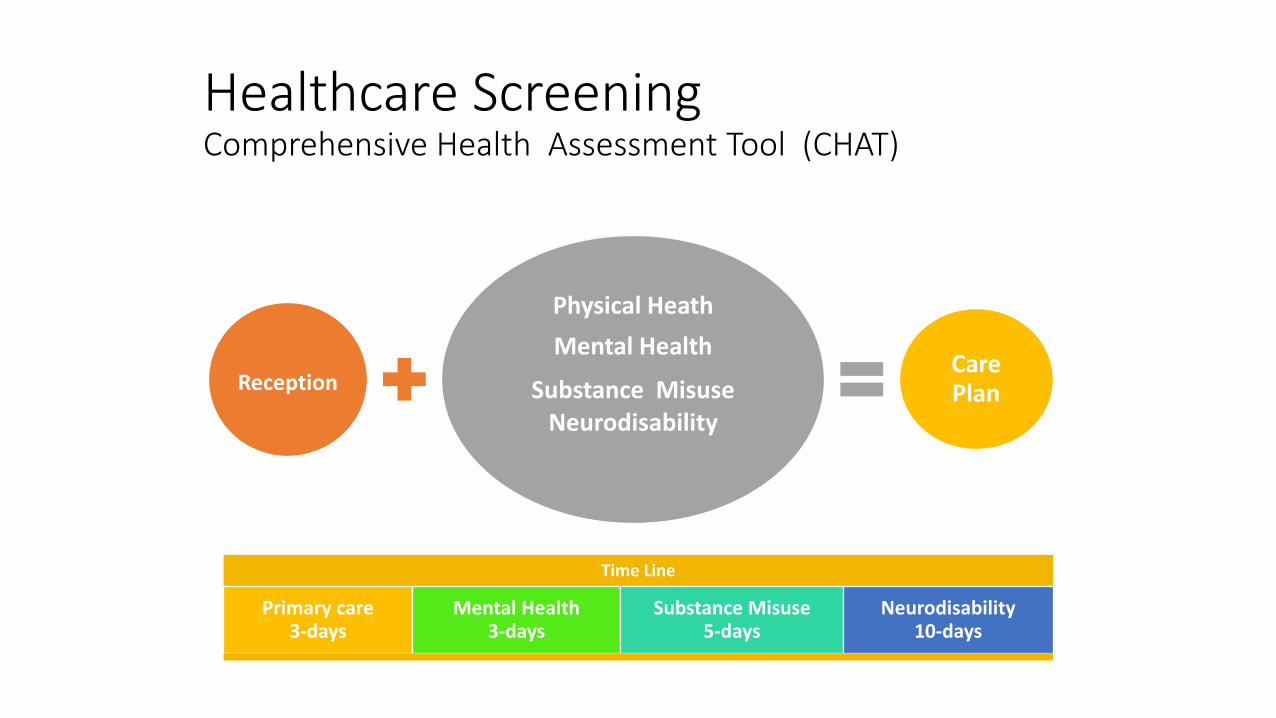
Healthcare Screening Comprehensive Health Assessment Tool (CHAT)
Reception
Physical Heath
Mental Health
Substance Misuse Neurodisability
Care Plan
Time Line
Primary care 3-days
Mental Health 3-days
Substance Misuse 5-days
Neurodisability 10-days

Primary Interventions
Primary Care
• GP Access ( 7 days)
• Nurse Led Clinics
• Sexual Health
• Smoking Cessation
• Dental Clinic
• Ophthalmic Care
• Proactive Outpatient Follow-up System
Mental Health
• Anger & Mood Management
• Trauma Clinic
• Harmful Sexual Behaviour Programme ( YP’s)
• Learning Difficulty Assessment/ Clinic
• Mental Health Assessments

Mental Health & Wellbeing Team
• Psychologist & Psychology Assistants • Speech & Language Therapist • RMHN’s• Occupational Therapist • CAMHS Consultant • Learning Disability Consultant • Forensic Psychiatrist
Substance Misuse Interventions
• Harm Reduction Service
• Specialist Pharmacological Intervention
• Psychosocial – Counselling
• Cognitive Behavioural Therapy
• Psychosocial – Motivational Interviewing
• Psychosocial – Relapse Prevention
• Psychosocial – Family Work

Primary Substances Misuse Data September/December 2016
New Episodes Active Cases
Alcohol unspecified 8 15
Cannabis herbal 23 54
Cannabis herbal (skunk) 1 5
Cannabis unspecified 22 37
Heroin illicit 1 1
Nicotine 8 8
NPS Other - 0 1
TOTAL 66 121

Clinical Activity – GP Trend

Systematic Focus on Risk & Performance
• Each service area holds weekly (RPM’s) the sole focus is on identifying risk and performance issues
• The process is designed to promote bottom up solutions
• The RPM process is based on Kanter’s nine symptoms of corporate decline

Key Challenges
• The re-alignment of mental health services for young people (Secure Stairs model)
• Ongoing work to support the continuity of care with community based services
• Sustaining and building on key patient data sets, e.g. GP registration and NHS numbers.
• Introduction of opt-out BBV testing.
Recommended