
July 2012 Webinar• PDSA Sharing• Month 1 Reporting• CCI Practice: Byrnes Family Medicine
• Conduct the test with one provider in the office, or with one patient
• Conduct the test over a short time period• Test the change with the members of the
team that helped develop the plan• Test the change on a small group of
volunteers• Minimize confusion, frustration until bugs
are worked out, then spread
Testing on a Small Scale
PDSA Sharing• Pre-visit planning: Eastbrook, Oyster Point, Green Hill• Use of diabetes template: Seneca• Population alerts: Warren, Corry, General Internal
Medicine• Outreach for overdue patients: Manor, Mountville• Data capture/reporting: Hamilton Health• Patient education/Self management support: Oil Valley,
Hamilton Health• Complication screening (feet, eyes, kidneys): Carlisle,
Sandrowicz, Oyster Point
Super Strategies• Staff education/training• Staff meetings• Standing orders• Process auditing• Small, rapid PDSA cycles
PDSA Assistance, Reporting• Talk with your practice facilitator about your
PDSAs – they are there to help you!• South Central – Sharon Adams
814-344-2222, [email protected]• North West – Patty Stubber
814-217-6029, [email protected]
• Please fill out your entire PDSA worksheet, including what you’re learning (not just what you plan to do).
• Submit your PDSA worksheets ongoing or with your monthly reports.
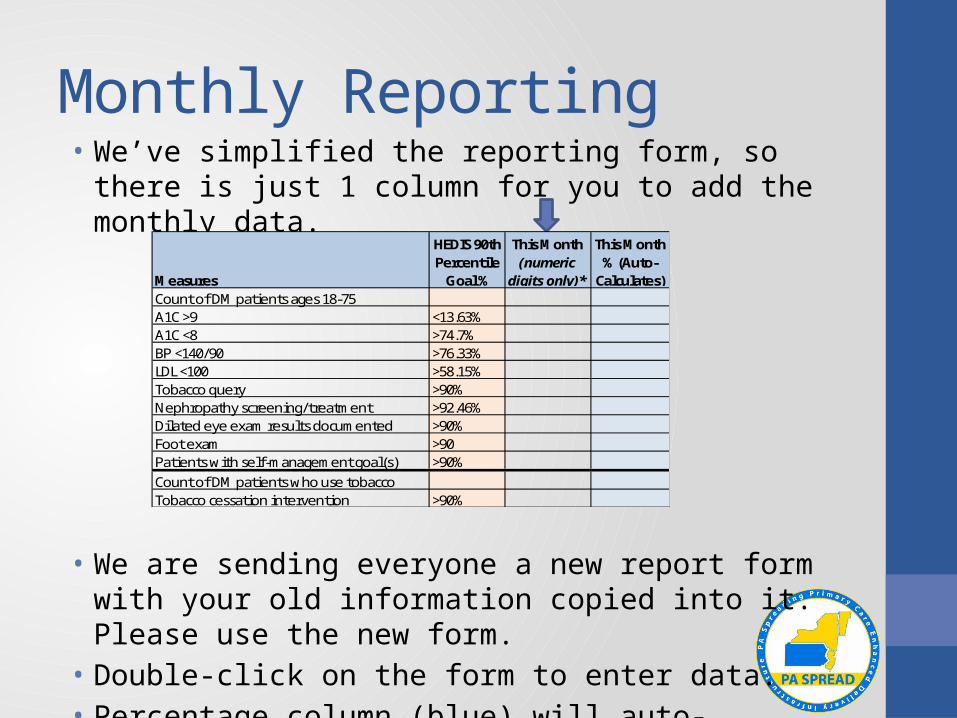
Monthly Reporting• We’ve simplified the reporting form, so there is just 1 column
for you to add the monthly data.
• We are sending everyone a new report form with your old information copied into it. Please use the new form.
• Double-click on the form to enter data.• Percentage column (blue) will auto-calculate.
Measures
HEDIS 90th Percentile
Goal %
This Month (numeric
digits only)*
This Month % (Auto-
Calculates)Count of DM patients ages 18-75A1C >9 <13.63%A1C <8 >74.7%BP <140/90 >76.33%LDL <100 >58.15%Tobacco query >90%Nephropathy screening/treatment >92.46%Dilated eye exam results documented >90%Foot exam >90Patients with self-management goal(s) >90%Count of DM patients who use tobaccoTobacco cessation intervention >90%
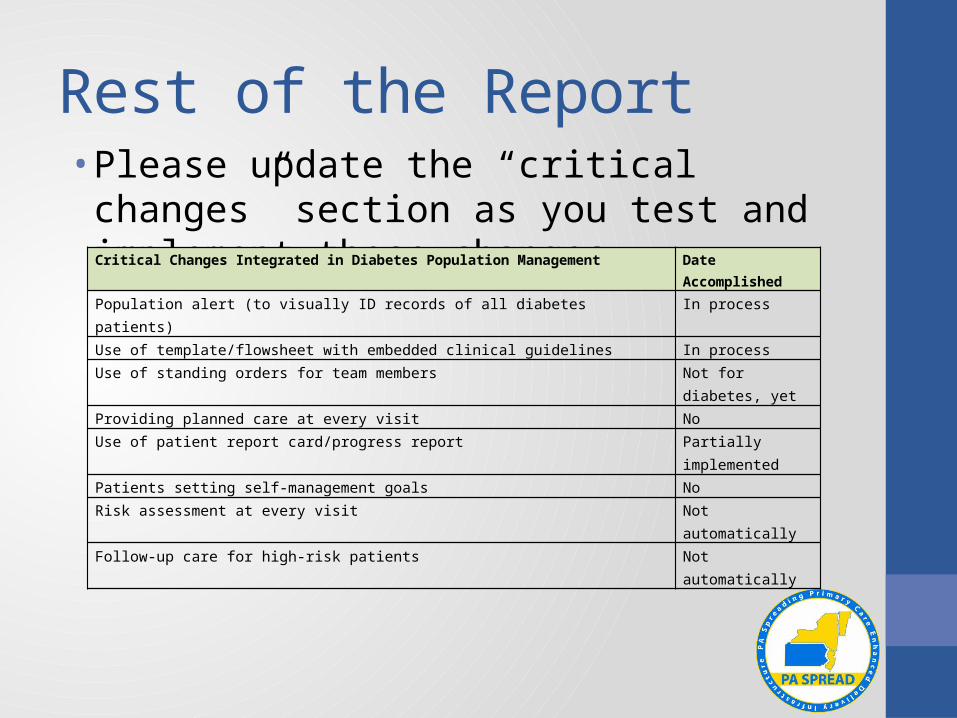
Rest of the Report• Please update the “critical changes” section as
you test and implement these changes.Critical Changes Integrated in Diabetes Population Management Date AccomplishedPopulation alert (to visually ID records of all diabetes patients) In processUse of template/flowsheet with embedded clinical guidelines In processUse of standing orders for team members Not for diabetes, yetProviding planned care at every visit NoUse of patient report card/progress report Partially
implementedPatients setting self-management goals NoRisk assessment at every visit Not automaticallyFollow-up care for high-risk patients Not automatically
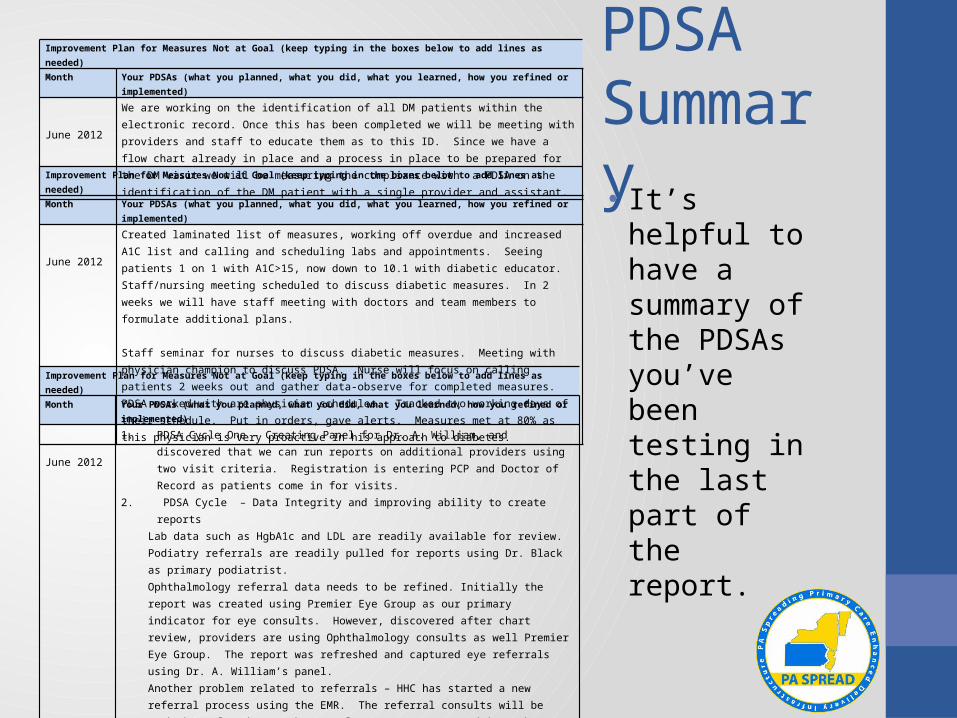
PDSA Summary• It’s helpful to
have a summary of the PDSAs you’ve been testing in the last part of the report.
Improvement Plan for Measures Not at Goal (keep typing in the boxes below to add lines as needed)
Month Your PDSAs (what you planned, what you did, what you learned, how you refined or implemented)
June 2012
1. PDSA Cycle One – Creating Panel for Dr. A. William, and discovered that we can run reports on additional providers using two visit criteria. Registration is entering PCP and Doctor of Record as patients come in for visits.
2. PDSA Cycle – Data Integrity and improving ability to create reportsLab data such as HgbA1c and LDL are readily available for review.Podiatry referrals are readily pulled for reports using Dr. Black as primary podiatrist.Ophthalmology referral data needs to be refined. Initially the report was created using Premier Eye Group as our primary indicator for eye consults. However, discovered after chart review, providers are using Ophthalmology consults as well Premier Eye Group. The report was refreshed and captured eye referrals using Dr. A. William’s panel.Another problem related to referrals – HHC has started a new referral process using the EMR. The referral consults will be marked completed once the actual reports are scanned into the EMR by HIS. Our referral numbers may be low until this process is perfected and all reports have arrived. Plan to monitor Unit Clerks using the Order Tracking Tab in the EMR. For the referrals without a completion date, the Unit Clerks are to call the patients to inquire if appointment was kept and the report needs to be sent from the referral office or if the patient requires rescheduling, Data Analyst reviewing ability to create reports for self- management goals. Clinical staff not using the Diabetic Goal Template consistently. Self- Management requires further investigation and planning for documentation of self- management goals. Assessment of smoking status is readily available and Medical Assistants assesses and documents upon rooming of patient.Assessment of Smoking intervention requires consensus on which areas of documentation to be used consistently for documentation of smoking intervention and cessation. Periodically providers are documenting in text form and not using medcin findings. We need to fully investigate the orders for medications, and recommendations for Nicotine patch and Nicotine Gum.Problem – upon refreshing data, syntax errors occur, and require Data Analyst to edit the formulas. Reports take a very long time to run on whole clinic.Need to request Data Analyst to create baseline report for Eye consults and retrieve monthly data for micro albumin. The ability to run individual reports for Dr. A. William panel is much quicker than running for whole clinic using multiple measures.Plan at this point in time to focus on first four measures and add measures as we move along.
3. PDSA – Self Management – Reviewed the self- management goals provided in EMR and the self- management goals on printed sheet utilized from a previous DM Collaborative. It was decided to use the goals from EMR and edit the hard copy with pictures with EMR Diabetic goals. Problem – Finding the ability to print the Diabetic goals for patients at the end of the visit. Presently being discussed, the MA will write the patients goals on the hard copy self -Management goals and provide to the patient. However, it needs to be investigated whether the goals will be printed on the clinical summary at the end of the patients visit. Continue discussion who will set the patient goals with the patient, MD, or Medical Assistant. Further education will be required for medical assistants for assessing and interviewing the patients.
Improvement Plan for Measures Not at Goal (keep typing in the boxes below to add lines as needed)
Month Your PDSAs (what you planned, what you did, what you learned, how you refined or implemented)
June 2012
Created laminated list of measures, working off overdue and increased A1C list and calling and scheduling labs and appointments. Seeing patients 1 on 1 with A1C>15, now down to 10.1 with diabetic educator. Staff/nursing meeting scheduled to discuss diabetic measures. In 2 weeks we will have staff meeting with doctors and team members to formulate additional plans. Staff seminar for nurses to discuss diabetic measures. Meeting with physician champion to discuss PDSA. Nurse will focus on calling patients 2 weeks out and gather data-observe for completed measures. PDSA worked with are physician schedules. Tracked two working days of their schedule. Put in orders, gave alerts. Measures met at 80% as this physician is very proactive in his approach to diabetes.
Improvement Plan for Measures Not at Goal (keep typing in the boxes below to add lines as needed)
Month Your PDSAs (what you planned, what you did, what you learned, how you refined or implemented)
June 2012
We are working on the identification of all DM patients within the electronic record. Once this has been completed we will be meeting with providers and staff to educate them as to this ID. Since we have a flow chart already in place and a process in place to be prepared for the DM visit we will be measuring the compliance with a PDSA on the identification of the DM patient with a single provider and assistant.
Comments at the End• Feel free to add comments or questions at the end of the
report. (Please date them.)• Challenges you are facing.• Areas where you need support or resources.• Things you want to learn more about.
Example:July 20121. Discussion concerning Self -Management goals and innovative ways to incorporate group visits.2. Data integrity and creating reports remains a challenge for a number of measures but we are improving the quality of the reports.
Patient Centered Medical HomeBuilding the System
Mary Beth Byrnes, MSN, RN
PA SPREAD PCMH Initiative
July 26, 2012
Richard Byrnes, D.O. Family Practice Established 1974 Serving Upper Bucks & Montgomery Counties Suburban – Semi-Rural Patient Population 2100 97% English Speaking Caucasian Farming – Light Industry 7.2% Community Unemployment Rate Staff – 1 RN (CNS), 2 MA, 1 CRNP (temporary)
PACCI – 2010Why Participate in Initiative Expert Guidance Challenge Financial
No Cost Meaningful Use IBC – Incentive Payment
Better Patient Outcomes
Decision Support Clinical Guidelines Imbedded in EMR & Registry Stepped Care Protocol – Medications Standing Orders – Team Members
Labs, Eye Exam, Diabetic Education, Influenza & Pneumococcal Vaccinations, Mammograms, Colonoscopy
Risk Stratification – Identify highest risk patients Created a Care Management Process
Patient Centered Communication Proven Education Methods – Barrier to Care/Confidence
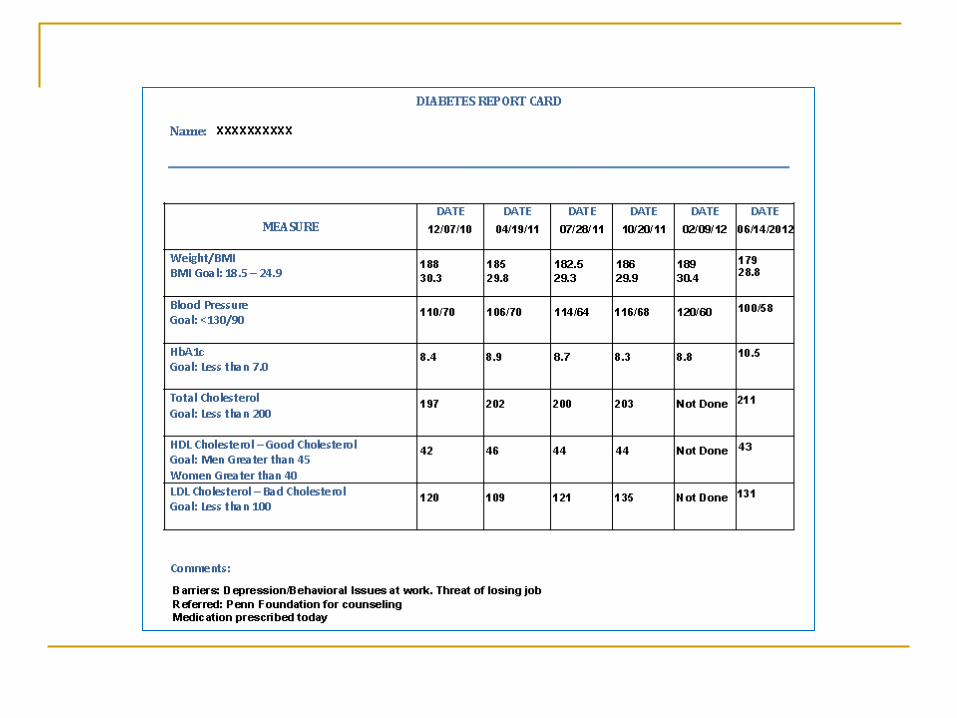
Patient Support & Report Cards Sharing Guidelines – Outcomes with Patients
Patient Education Material & Resources
Delivery System Design
Planned Care at Every Visit PDSA’s
How to implement elements from Decision Support Written Policy for PDSA’s Implemented Job Descriptions related to the new policy
Developed a Strategy Mapped Office Visits
Delivery System DesignPlanned Care at Every Visit Formed Team & Identified Roles & Responsibilities Evaluated Method of Communication
Motivational Interviewing Techniques Self Management
Report Card & Self Management Goals Readiness & Confidence Rulers Action Plan
System to Identify & Document High Risk Patients Develop Care Plan for Highest Risk Patients
Huddles, Tag Team, Warm Hand Off
Delivery System Design Redefined Roles & Work Flows Put more responsibility on staff
How to Read Charts Tracking
Removed any “Crutch” which blocked change Redefined Flow of Patient Visit - Mapping
Team Effort Team Member Responsibilities
Written Policy Updated Job Descriptions
Focused on Patient Education Tag Team
Written Policy Based on Successful PDSA’s
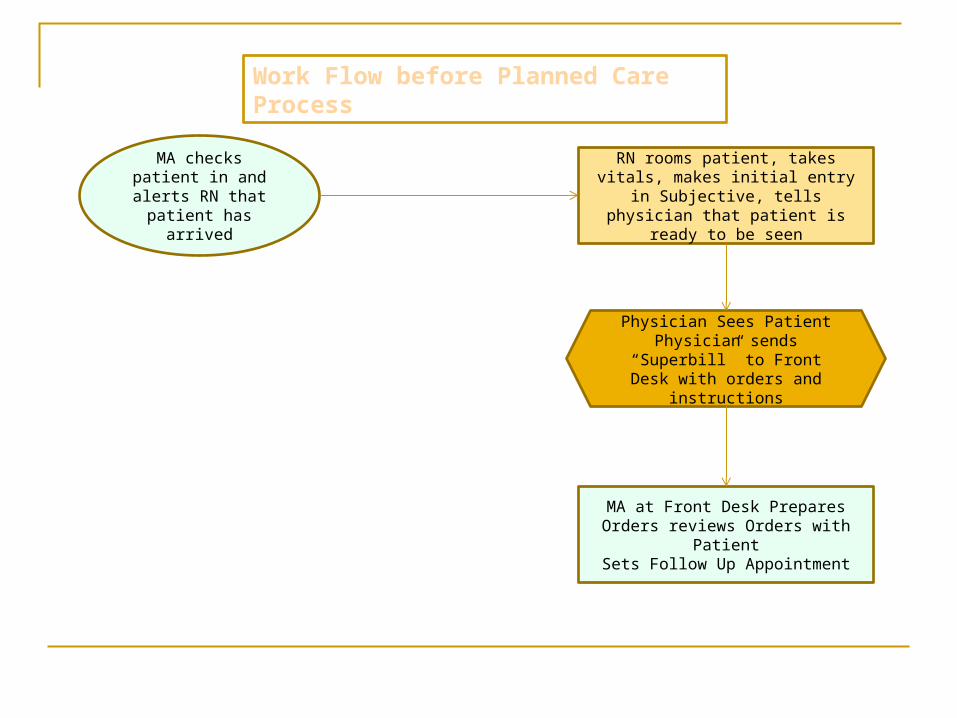
MA checks patient in and alerts RN that patient has arrived
RN rooms patient, takes vitals, makes initial entry in Subjective, tells
physician that patient is ready to be seen
MA at Front Desk Prepares Orders reviews Orders with PatientSets Follow Up Appointment
Physician Sees PatientPhysician sends “Superbill” to
Front Desk with orders and instructions
Work Flow before Planned Care Process
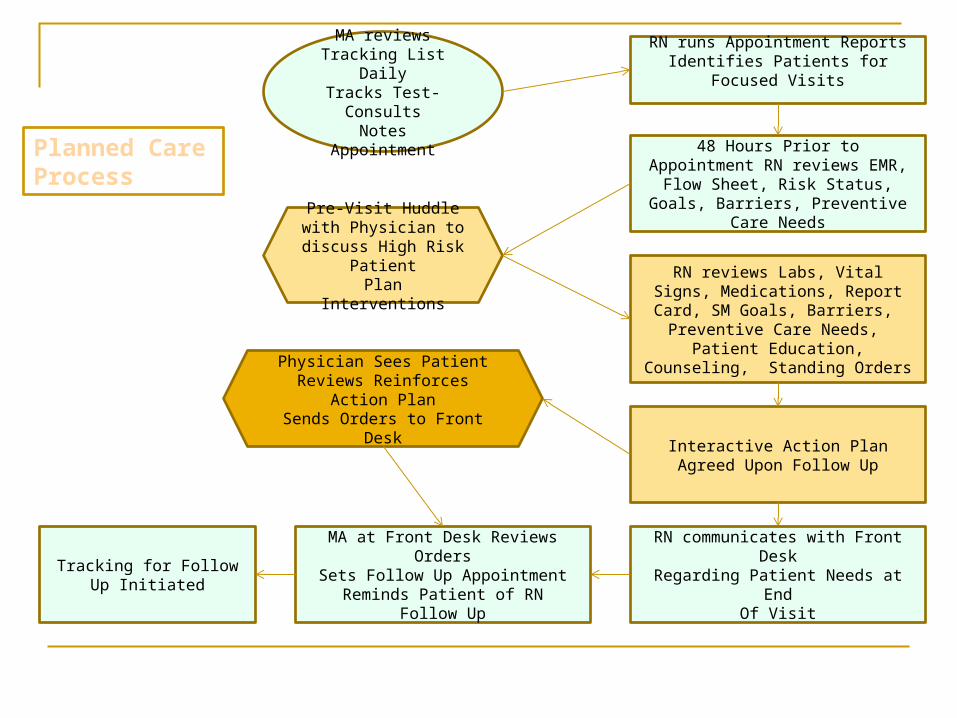
MA reviews Tracking List Daily
Tracks Test-ConsultsNotes Appointment
RN runs Appointment ReportsIdentifies Patients for Focused Visits
48 Hours Prior to Appointment RN reviews EMR, Flow Sheet, Risk
Status, Goals, Barriers, Preventive Care Needs
RN reviews Labs, Vital Signs, Medications, Report Card, SM Goals,
Barriers, Preventive Care Needs, Patient Education, Counseling, Standing
Orders
Interactive Action PlanAgreed Upon Follow Up
RN communicates with Front DeskRegarding Patient Needs at End
Of Visit
MA at Front Desk Reviews OrdersSets Follow Up Appointment
Reminds Patient of RNFollow Up
Tracking for Follow Up Initiated
Pre-Visit Huddle with Physician to discuss
High Risk PatientPlan Interventions
Physician Sees PatientReviews Reinforces Action Plan
Sends Orders to Front Desk
Planned Care Process
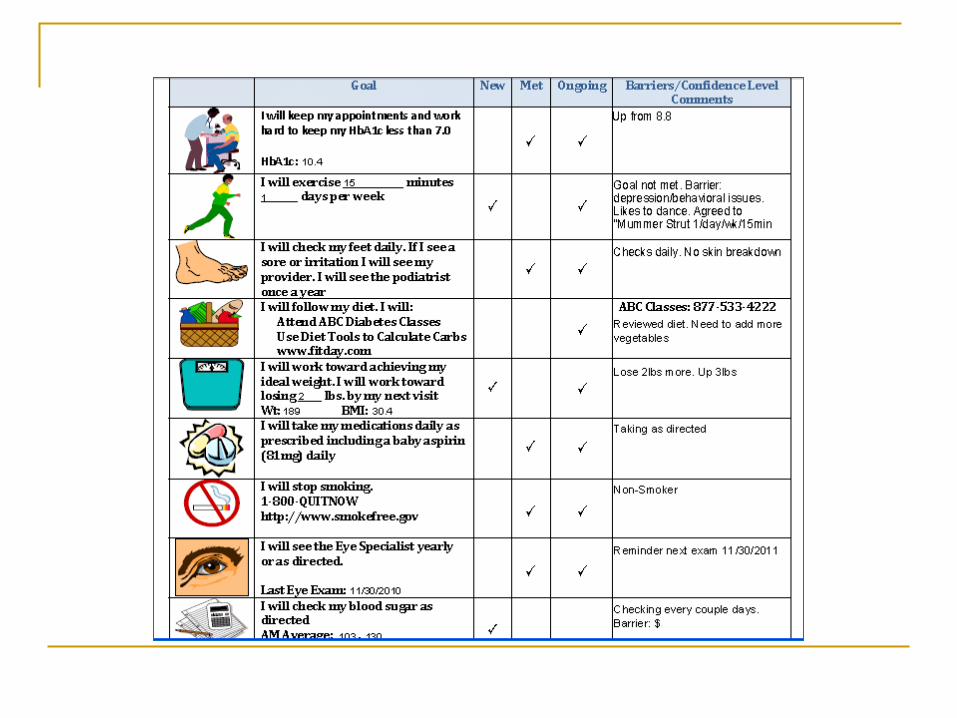
Self-Management Support
Changed Method of Communication Provider Self Assessment
Patient Report Card Clinical Measures
Self Management Goals Process Measures
Identify Barriers to Goals & Readiness to Change Action Plan
Impact of Self-Management Support Improved Patient Outcomes Patients Taking Control Patients Increased Confidence
Spreading their Knowledge Improved Patient Satisfaction
Improved Work Flow Improved Provider/Staff Satisfaction Development of Care Management Strategies
Developed Relationships with Insurance Carrier Care Managers and ABC Diabetes Education Program
Computer Information System The Tool Goal
Population Management Data Management Access and Continuity Monitor Performance
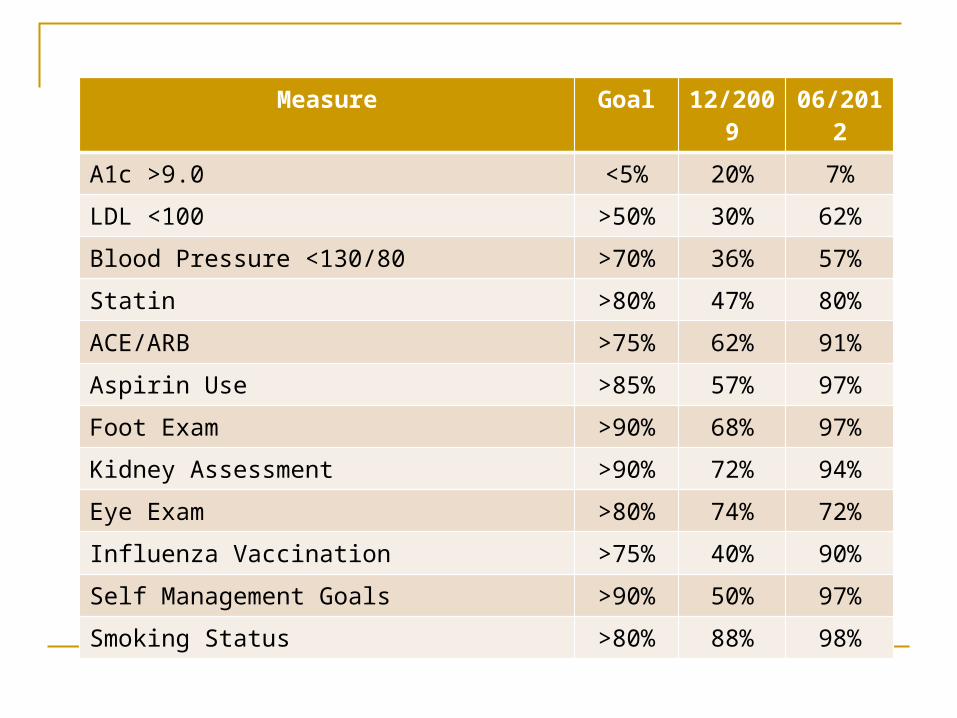
Measure Goal 12/2009 06/2012
A1c >9.0 <5% 20% 7%
LDL <100 >50% 30% 62%
Blood Pressure <130/80 >70% 36% 57%
Statin >80% 47% 80%
ACE/ARB >75% 62% 91%
Aspirin Use >85% 57% 97%
Foot Exam >90% 68% 97%
Kidney Assessment >90% 72% 94%
Eye Exam >80% 74% 72%
Influenza Vaccination >75% 40% 90%
Self Management Goals >90% 50% 97%
Smoking Status >80% 88% 98%
Advantage of Being a Small Practice
Small Practices can effect change faster than larger practices Less Inertia
Change that occurs can result in improved patient outcomes that are consistent with improved patient outcomes in large practices
Questions?
Recommended

















