My Baltimore HIV/AIDS Scholar Experience
Presented by Katerina Lescouflair

Generation Tomorrow (GT)★ Initiated in October 2013 by
the Johns Hopkins Center for AIDS Research (JHU CFAR)
★ GT trains students and
community members (peers) in
HIV and hepatitis C virus (HCV)
education, testing, and
counseling
★ Collaborates with Hopkins
associated outreach programs
and community agencies to
provide a field experience to
students

Generation Tomorrow Community PartnersAnd Johns Hopkins Associated Outreach Programs
STAR TRACK
Older Women Embracing Life
Johns Hopkins Emergency Medicine
ALIVE Study
Project Re__Baltimore City Health Department
STD ClinicVaccine is PreventionSisters Together and Reaching (STAR)
Viral Hepatitis Center at JHH Blalock
(Specialty) Clinic

★ Faith-based community organization founded in 1991 to address the health disparities surrounding HIV+ and affected African-American women and their families in Baltimore City.
★ Defines “Optimal Health” as providing spiritual support, linkage to care, direct services, treatment and prevention education.
★ Provides several AIDS & faith-related services to the youth, men and women of Baltimore City to educate and support . To name a few:
○ The Block Mobile Outreach Project○ Black Male Wellness Project
○ Minority AIDS Outreach ○ Ryan White Part A: Minority AIDS
initiative○ Case management for HIV+/HCV+ clients
Sisters Together and Reaching
(STAR)
http://www.sisterstogetherandreaching.org/#!about/cjg9

★ I joined STAR’s Mobile Testing (HIV/HCV) Van Outreach Program on Thursday nights @ “The Block” and other destinations
★ I enjoyed working with STAR because it really gave me an opportunity to learn more about the Baltimore community and provide HIV/HCV counseling and education for people who really needed it
My Field Placement with STAR

Johns Hopkins Emergency Medicine
★ Implemented an HIV testing program in 2005.
★ Has identified 200+ previously unknown HIV+ patients and linked them to care
★ Offers and performs free routine HIV screening to all patients ages 15-65.
★ Post-test counseling is performed with all tested patients
★ Assist with linkage to care for new HIV diagnoses, or for HIV positive patients that are not currently in care.
★ Testing is available to eligible ED patients 16 hours a day (8am-12a), 7 days per week.
Source: http://source.jhu.edu/programs-and-events/hiv-counseling-and-testing-program/ParticipationRequirements20152016.pdf

My Field Placement with JHH ED ★ I assisted with the JHH ED HIV Program and provided free
HIV testing, facilitation, and post-test counseling○ Working here really taught me how to deal with the
emotional dispositions of patients (varying from friendly
to irate) and help educate/counsel them about HIV
prevention & infection at the same time
★ Unfortunately (or fortunately), I did not encounter a new HIV+ patient, so I was unable to directly link a patient to care, but I was able to link patients to other free HIV testing sites in Baltimore and counsel patients on how to stay HIV-.

Research Background- Hepatitis C Basics★ What is it? Hepatitis C is a
contagious liver disease ★ Where does it affect? The liver. ★ How does HCV spread? Contact with
the blood of an infected person. In the US, the most common way to get infected is IDU. Blood transfusions used to be a common way to get infected, but is rare now in the US since blood screening became available in 1992)
★ HCV can be cured with all-oral regimens
Information courtesy of CDC: http://www.cdc.gov/hepatitis/hcv/cfaq.htm#cFAQ11
★ Who is at risk?○ Current IDU○ Past IVDU (including those who
injected only one time or many years ago)
○ Recipients of donated blood, blood products, and organs, people who received a blood product for clotting problems made before 1987
○ Hemodialysis patients or persons who spent many years on dialysis for kidney failure
○ People who received body piercing or tattoos done with non-sterile instruments
○ People with known exposures to HCV, such as health care workers injured by needlesticks and recipients of blood or organs from a donor who tested positive for HCV,
○ HIV+ people○ Children born to HCV+ mothers

Why is HCV important?It can cause liver damage, liver failure, liver cancer, or even death. It is the leading cause of cirrhosis and liver cancer and the most common reason for liver transplantation in the US. ~19,000 people die
every year from HCV-related liver disease.

75%–85%Of people who become infected with HCV will develop chronic infection.
Information courtesy of CDC: http://www.cdc.gov/hepatitis/hcv/cfaq.htm#cFAQ11

2.7-3.9 M People in the US have chronic Hepatitis C
Information courtesy of CDC: http://www.cdc.gov/hepatitis/hcv/cfaq.htm#cFAQ11

70-80%Of people with acute Hepatitis C do not have any symptoms, warranting the name, “The Silent Killer.”
Information courtesy of CDC: http://www.cdc.gov/hepatitis/hcv/cfaq.htm#cFAQ11

Treatment: Interferon vs DAAs (direct acting antivirals)★ Peginterferon (PEG increases interferon
half-life in the body) + ribavirin combo regimen
○ 1-3 injections/week○ Must refrigerate○ 50% success rate○ Multiple side effects: Flu-like symptoms
(headache, fever, chills, muscle aches), insomnia, depression and mood changes, irritability, nausea and vomiting, skin rashes, extreme tiredness, loss of appetite, weight loss
○ Cost: range of $8,400 for a 12-week course and $16,800 for a 24-week course
○ Medicaid, Medicare and private insurance cover the cost when treatment is approved
★ DAAs (Sovaldi, Harvoni, Daklinza and Viekira Pak, etc.) directly attack enzymes related to HCV replication
○ All once or twice daily oral regimens
○ 90-100% success rate○ Few side effects seen in small
percentage of study populations○ Cost: ~$95k for 12 weeks○ Medicaid, Medicare and private
insurance cover the cost when treatment is approved
Sources: https://www.verywell.com/what-is-a-pegylated-drug-1760130 , http://hepc.liverfoundation.org/treatment/the-basics-about-hepatitis-c-treatment/advances-in-medications/

Why are so many people falling through the cracks? Could it be that new DAAs (direct acting antivirals) are not well enough advertised? Cost?
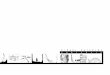
Diagram courtesy of Yehia et al. Hepatitis C Virus Infection in the United States
HIV Care Cascade

So why are there still persistent LTC (Linkage to Care) barriers, and how can we solve them?

Research Methods
★ 1. Document what currently happens to get patients linked to care
○ Met with LTC Coordinators at the VHC and the JHH ED
★ 2. Conduct in-depth interviews with patients and providers (case managers, clinicians, outreach specialists) to define any barriers to LTC and possible solutions

Research Results-Barriers Identified by Providers★ “I feel okay right now, so the disease isn’t bothering me and if I mess
with it, I’ll make things worse.”
★ Not a high priority given the highly-stressful external factors that much
of the Baltimore population faces everyday: homelessness, substance abuse,
taking care of family, and death
★ Do not know risks of untreated HCV or how it can affect the body
★ Fear that insurance companies will not cover the cost of the HCV medical
treatment (~$94.5k for 3 months) if patient’s liver disease stage (F0-F4)
not being dire enough
★ Fear of adverse side effects, in relation to the previous HCV treatment,
Interferon

Research Results-Barriers Identified by Patients
★ Do not want friends or family to see them visiting clinic or their medication★ Fear of adverse side effects, in relation to the previous HCV treatment, Interferon★ Fear of being isolated from family & friends★ Fear that the disease will mean putting one’s life on hold: work, romantic
relationships, substance abuse★ Distance to HCV clinic★ Transportation to clinic★ Cost of medication without insurance coverage★ Too many other things going on: family--kids & elderly parents, incarceration,
substance abuse★ Highly stressful jobs that do not enable patient to make appointments and stay in
regular HCV care★ Shame about diagnosis★ Denial about what will happen if HCV goes untreated

Research Results-Why Patients Are Lost to Care
★ Not emotionally/mentally ready to start treatment★ External factors including, but not limited to:
homelessness, transient housing, disconnected phone number, incarceration/prison, substance abuse, food issues, relationship issues (esp. domestic abuse), death
★ If insurance does not cover medical costs and the patient is ineligible for HCV clinical trials, a sense of hopelessness can make the patient feel like “Why should I bother coming to my appointments anymore? I can’t get cured.”

Research Conclusions
★ Educating the public about HCV on a larger scale so that people know just as much about HCV as they do HIV is crucial.
★ Enacting insurance policy reform. There is no other disease where a patient is ignored/sent away because their condition “is not bad enough.” Have you ever heard a doctor say to a cancer patient to come back when they have Stage 3 or 4 cancer? No. And that’s the problem.
★ Ending stigma is still an issue. PCPs still focus on how patients contracted HCV, instead of focusing on how to cure them.

Special Thanks ★ CFAR
○ Jordan White, Chris Beyrer
★ Generation Tomorrow○ Dr. Risha Irvin, Zackiya Grant, and GT Students
Sarah and Deawodi
★ STAR○ Donald, Mr. OD, Will, Earl, Kayla, Deqwan
★ JHH ED○ Lucas, Tekiyah, Danielle and all the kind ED nurses
and staff
★ VHC○ Eniola, Rachel, Jillian, Tracy, Stacy, Joseph, and
all the HCV patients that were interviewed
Recommended