Respiratory Viruses
Viruses Associated with Respiratory Infections
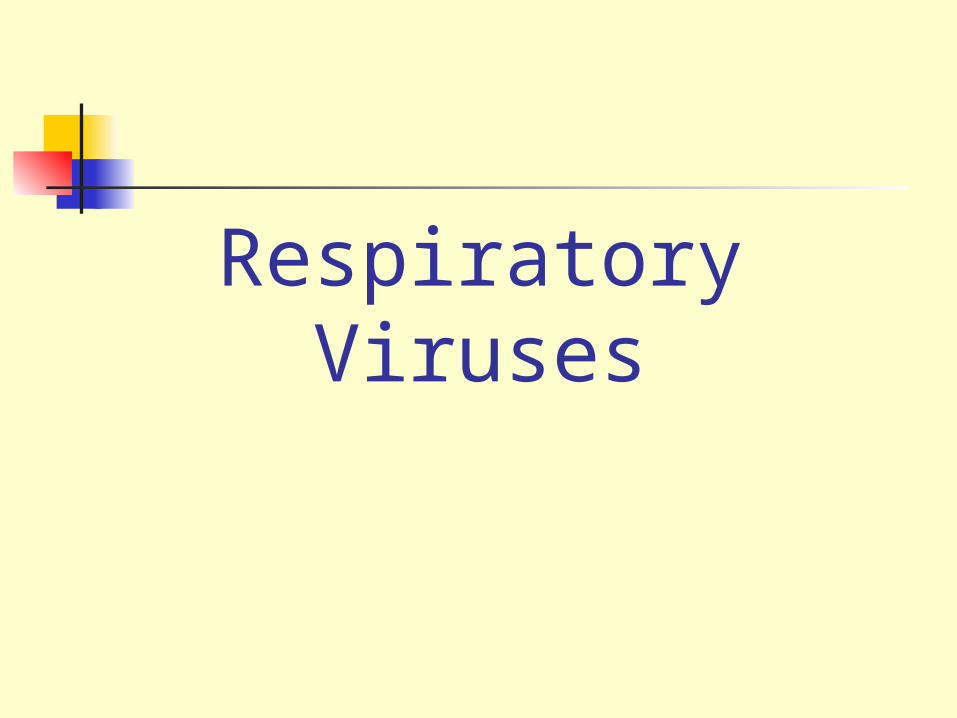
Syndrome Commonly Associated Viruses
Coryza Rhinoviruses, Coronaviruses
Influenza Influenza viruses
Croup Parainfluenza viruses
Bronchiolitis RSV
Bronchopneumonia
Influenza virus, RSV, Adenoviruses
Influenza Virus
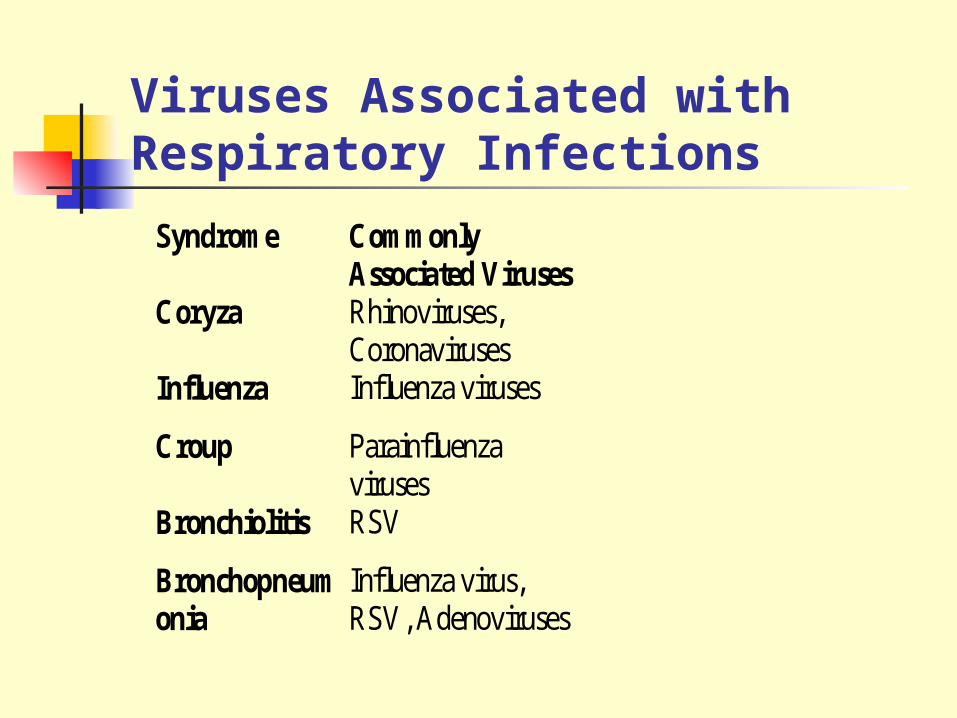
RNA virus Enveloped virus, with haemagglutinin
(HA) and neuraminidase (NA) spikes 3 types: A, B, and C Type A undergoes antigenic shift and
drift. Type B undergoes antigenic drift only Type C is relatively stable
(Courtesy of Linda Stannard, University of Cape Town, S.A.)

Influenza A Virus
Antigenic shift is an abrupt change of the HA due to genetic reassortment: results in pandemics
Antigenic drift is a gradual change in the HA and NA proteins: results in epidemics

Reassortment
Avian H3 Human H2
Human H3
Reassortment of the H and N genes between human and
avian influenza viruses through a third host.
Epidemiology
Epidemics Epidemics of influenza A and B arise due to minor
antigenic drifts as a result of mutation
Pandemics Due to antigenic shift a virus with a new
haemagglutinin subtype emerges The population has no immunity against the new strain Three antigenic shifts occurred in the 20th century
Past Antigenic Shifts
1918 H1N1 “Spanish Influenza” 20-40 million deaths
1957 H2N2 “Asian Flu” 1-2 million deaths
1968 H3N2 “Hong Kong Flu” 700,000 deaths
1977 H1N1 Re-emergence No pandemic
At least 15 HA subtypes and 9 NA subtypes occur in nature. Up until 1997, only viruses of H1, H2, and H3 are known to infect and cause disease in humans.

Influenza Virus Replication
Avian InfluenzaH5N1 An outbreak of Avian Influenza H5N1 in Hong Kong in
1997 The source of the virus was probably infected chickens Was controlled by a mass slaughter of chickens in the area
H9N2 Several cases of human infection occurred in Hong Kong
and Southern China in 1999 The disease was mild and all patients made a complete
recovery

Symptoms Usually much more severe than, the "common cold." “Incubation period." 1-2 days Fever (up to 104° F) Chills Muscle aches and pains Sweating Dry Cough Nasal congestion Sore throat Headache Malaise & Fatigue Some or all of these symptoms may be present Illness can last for up to 1-2 weeks, although fever generally
lasts only 3-8 days.

Complications Bacterial pneumonia Influenza can damage the lining of the
respiratory tract and bacteria establish an infection
Streptococcus pneumoniae and Staphylococcus aureus are the common causes.
Pneumonia caused by the virus itself is less common

Laboratory DiagnosisSpecimens Nasopharyngeal aspirates & throat washings Detection of Antigen By IFT and ELISA: a rapid diagnosis
Virus IsolationSerology CFT most widely used. EIA detect type-specific antibodies
Management
Amantidine Rimantidine Ribavirin Neuraminidase
inhibitors
Prevention Vaccination with an inactivated
trivalent vaccine, consisting of one A H3N2 strain, one A H1N1 strain, and one B strain
May be 30-90% protective Given to debilitated, elderly and
immunocompromized individuals Amantidine prophylaxis WHO Global Surveillance
Nasal Spray
Common Cold Viruses Common colds: one-third to one-half of all
acute respiratory infections in humans
Rhinoviruses (30-50%) Coronaviruses (10-30%)
Others: Adenoviruses Enteroviruses RSV Influenza, and parainfluenza viruses

Rhinovirus
ssRNA virus Picornavirus family Acid-labile At least 100 serotypes are
known
Reconstructed Image of rhinovirus particle (Institute for Molecular Virology)
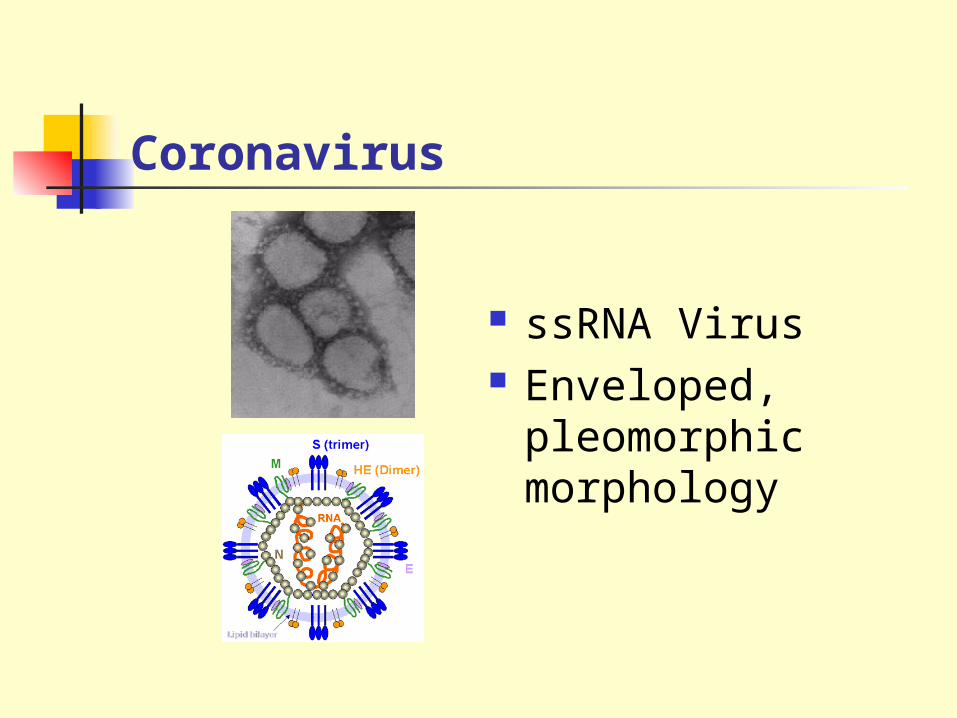
Coronavirus
ssRNA Virus Enveloped,
pleomorphic morphology
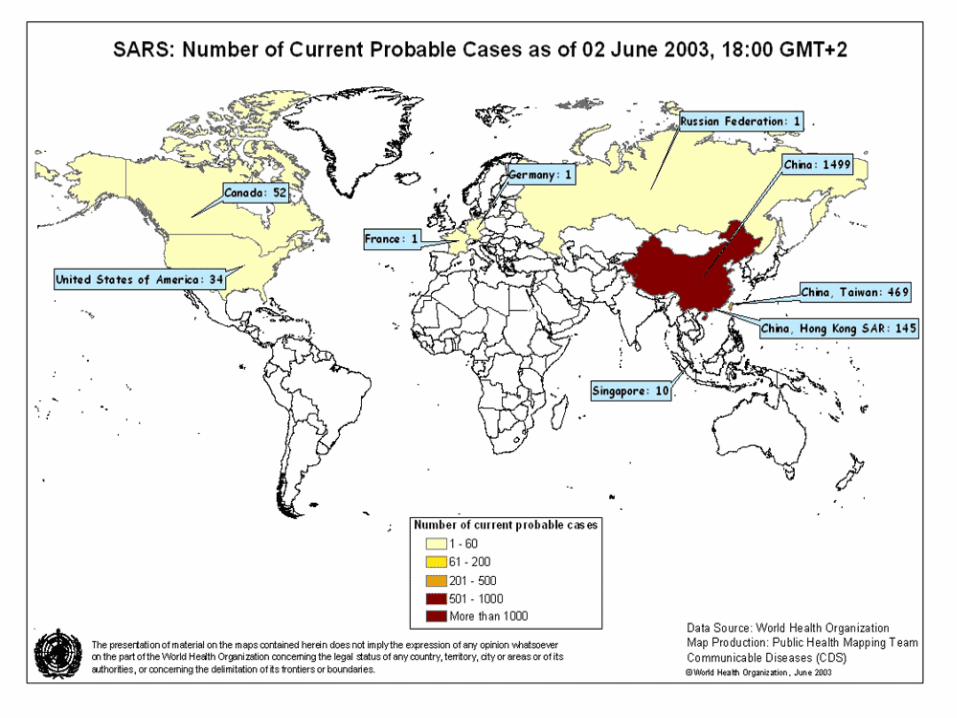
Severe Acute Respiratory Syndrome (SARS)
In late 2002: first observed in Southern China (Guangdong Province).
Now been reported in Asia, North America, and Europe
The initial outbreak of SARS peaked in April 2003 and by June had tailed off. By that time, there had been about 8,000 cases worldwide and 775 deaths.
SARS
Is characterized by: Fever above 38oC (100.4oF) headache,
general malaise and aches. Initially mild respiratory symptoms Dry non-productive cough & dyspnea Respiratory distress leads to death in
3-30% of cases.
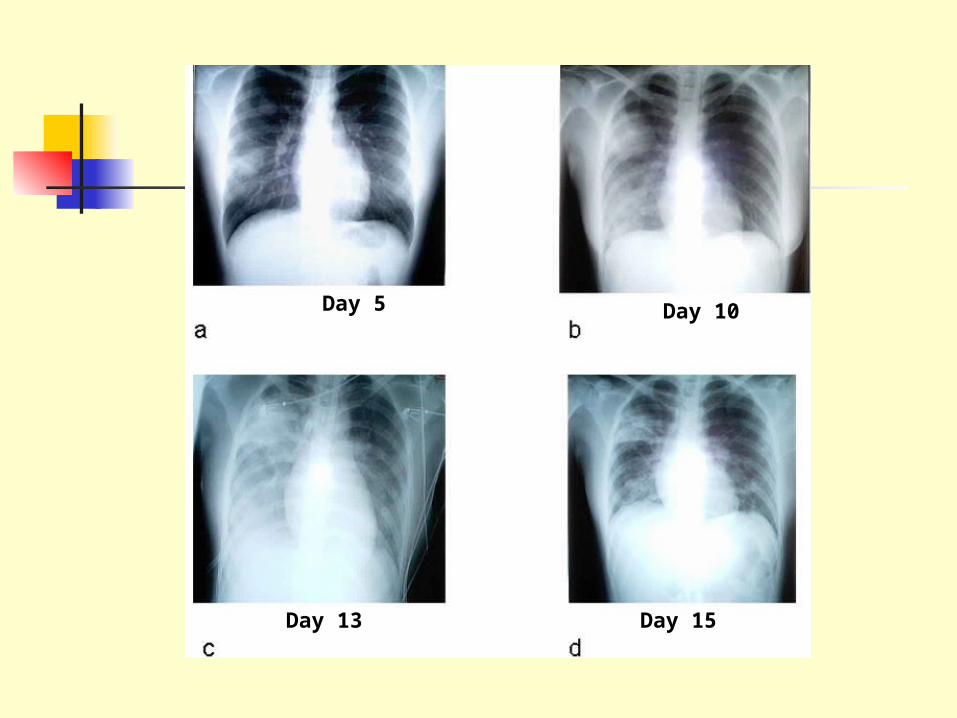
Day 5 Day 10
Day 13 Day 15

The virus was grown on monkey Vero E6 cells in tissue culture and a new coronavirus (SARS-coV) was identified
Reduction in lymphocyte numbers Raised aminotransferase activity which
indicates damage to the liver.
SARS
CDC recommendations: Chest radiograph Blood cultures Sputum Gram's stain and culture Testing for viral respiratory pathogens, notably
influenza A and B and RSV. Legionella and pneumococcal urinary antigen
testing
SARS: Lab Diagnosis

Treatment
Suspected SARS patient should be isolated and quarantined.
Management of symptoms No vaccine against the SARS virus. A major problem with live virus
vaccine is antigenic shift and unpredictable outcomes

Parainfluenza Virus
ssRNA virus Enveloped 5 serotypes: 1, 2, 3, 4a and 4b Closely related to Mumps
virus
(Linda Stannard, University of Cape Town, S.A.)
Clinical Manifestations
Croup (laryngotraheobroncitis) The most common manifestation
Bronchiolitis Pneumonia Flu-like tracheobronchitis Coryza-like illnesses
Laboratory Diagnosis Specimens Detection of Antigen Virus Isolation Serology
Symptomatic Treatment No vaccine is available.
Management
Respiratory Syncytial Virus (RSV)
ssRNA eveloped virus Paramyxovirus family Causes a sizable epidemic each year
Clinical Manifestations Most common cause of severe lower
respiratory tract disease in infants Bronchiolitis (50-90%) Bronchopneumonia (5-40% )
Croup (10% of all cases) Coryza-like illness or bronchitis: in older
children and adults
Laboratory Diagnosis
Specimens Nasopharyngeal aspirates & throat washings Detection of Antigen Virus IsolationSerology

Treatment and Prevention
Aerosolised ribavirin There is no vaccine available
RSV immunoglobulin for high risk group infants
Adenovirus
ds DNA virus non-enveloped At least 47 serotypes
(Linda Stannard, University of Cape Town, S.A.)
Clinical SyndromesPharyngitis Pharyngoconjunctival feverAcute respiratory disease of recruits Pneumonia Follicular conjunctivitis Epidemic keratoconjunctivitisPertussis-like syndrome Acute haemorrhaghic cystitis Acute infantile gastroenteritis IntussusceptionSevere disease in AIDS Meningitis
Laboratory Diagnosis
Specimens Nasopharyngeal aspirates, throat washings & fecesDetection of Antigen Virus IsolationSerology
Treatment and Prevention A vaccine is available against Adult
Respiratory Distress Syndrome. Consists of live adenovirus 4, 7, and 21 in
enterically coated capsules. Given to new recruits into various arm
forces around the world.
Recommended




![Respiratory Viruses -2013 (FN) [Compatibility Mode].pdf](https://img.pdfslide.net/doc/110x75/577cdd241a28ab9e78ac484f/respiratory-viruses-2013-fn-compatibility-modepdf.jpg)