LeucemiaLeucemia MieloideMieloide AcutaAcutaTerapieTerapie Innovative Innovative
Adriano Venditti
Ematologia Universita’ Tor Vergata, Roma

LeucemiaLeucemia MieloideMieloide AcutaAcutaTerapieTerapie Innovative Innovative
Adriano Venditti
Ematologia Universita’ Tor Vergata, Roma

AML.Current outcome of therapy
10 (10 mo) 25 20 50 >60
35 (24 mo) 10 45 75 <60
OS % (med) ED% DFS %CR %Age, y

New strategies in AML
• Cell surface antigens− Anti-CD33 MoAbs
• Drug-resistance− MDR1 modulators
• Cellular signaling pathways− Kinase inhibition (FLT3, mTOR)− FT inhibition (RAS)− Induction of apoptosis (anti-bcl-2)− Proteasome inhibition
• Angiogenesis− Lenalidomide− Bevacizumab
• Epigenetic events− Hypomethylating agents, HDACi
• Others− Vaccines (WT1)
• Nucleoside analogues− Clofarabine− Troxacitabine− Ester of ARAc
• Alkylating agents− Cloretazine
• Inhibitors of Ribonucleotidereductase− Triapine
Novel cytotoxic drugs Targeted therapy

Fludarabine Cladribine Clofarabine
ClofarabineResistant to Deamination & Phosphorolysis

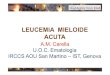
Metabolism and mechanism of action
Clofarabine
Clofarabine
Clofarabine
Clofarabine
P
P P
P P PRNR
DNAPolymerases
dCyd kinase
dNTP pool
DNA incorporation
Inhibition of DNA synthesis
CELL DEATH
Apoptosome

Clofarabine in AML
657Untreated37Clo + D + GO
616Rel/Untreated23Clo + Hd-AC
635Untreated42Clo + Ld-AC
604Untreated60Clo + Id-AC
413Rel/Ref29Clo + Id-AC
442Untreated66Clo (Biov-121)
321Rel/Ref31Clo
CR+CRi%PopulationNRegimen
1Kantarjian et al, Blood 2003; 2Burnett et al, ASH 2006; 3Faderl et al, Blood 2005; 4Faderl et al,Blood 2006; 5Faderl et al, ASH 2005; 6Agura et al, ASH 2006; 7Burnett et al, ASH 2006

AML16 intensive: Outline
*Randomise 2 vs 3 courses if at least PR after course 1 Mini-allo after course 2
D + Ara-C
D+Clofarabine
D + Ara-C
D+Clofarabine
Demethylation(Azacytidine)
No Treatment
R2CR/PR vs
Course 1 Course 2
+ Mylotarg
+ Mylotarg
D + Ara-C
No Rx
Demethylation(Azacytidine)
No Treatment

Cloretazine
• Novel sulfonylhydrazine alkylating agent
• Phase I dose-finding study in advanced AML(MDACC)
− 38 pts (28 AML, 5 MDS)
− 600 mg/m2 single iv infusion recommended dosefor phase II
−Minimal extramedullary toxicity
− 1 CR
• Phase II study in poor risk relapsed AML (MDACC)
− 53 pts (1st relapse AML; median age 62y)
− 600 mg/m2 single iv infusion
− 2 CR (4%)

Cloretazine
Phase II multicenter study in elderly untreated poor risk patientswith de novo AML or High Risk MDS
♣N=104♣600 mg/m2 single iv infusion♣Risk factors included ≥60 yrs, ECOG PS , secondary AML,
unfavorable cytogenetics, and organ dysfunction
Results:
• Currently being evaluated in a multicenter phase III trial incombination with Ara-C in 1st relapse AML
22%941Age+2
34%1029Age+ ≥3
32%722Age+1
58%712Age+0
CR/CRp(%)
CR/CRp(N=33)
# ofpatients
Risk Factors
Giles et al, JCO 2007

Burnett AK et al. ASH 2006. Abstract 13
MRC AML 15 Schema
DA 3+10
± GO
FLAG-Ida± GO
DA 3+8
FLAG-Ida
MACE
± GOMidAc
AraC 3g/m2
± GO
Ara-C
3g/m2
AraC1.0g/m2
ADE
8+3+5
Ara-C1.5g/m2
± GO
Ara-C1.5g/m2
Stoptherapy
Course 1 Course 2 Course 3 Course 4
R
Course 5
ADE
10+3+5
± GO
RISK
ASSESSMENT
R

CR
MRC AML 15 trial: study design
*Consolidation arms included gemtuzumab + chemotherapy.
Patients withuntreated AML
< 60 years of age
(N = 1115)
ADE ± GO(n = 160)
DA ± GO(n = 474)
FLAG-Ida ± GO(n = 479)
Induction:Course 1
ADE
DA
FLAG-Ida
Induction:Course 2
Risk assessment
Secondrandomization,thenconsolidation*
Burnett AK, et al. ASH 2006. Abstract 13.
To compare threeinduction schedules(namely ADE, DA and
FLAG-Ida)
To assess the value of GOduring induction when usedin combination with ADE or
DA or FLAG-Ida

MRC AML 15 trial: relapse and DFS
60
50
40
30
20
10
03 Years From CR
Rel
apse
(%
)
P = .027
54
39
Relapse
60
50
40
30
20
10
03 Years From CR
Dis
ease
Fre
e (%
)
P = .007
38
49
DFS
No gemtuzumab Gemtuzumab
Burnett AK, et al. ASH 2006. Abstract 13.



MRC AML 15 trial: preliminary results
• Similar rates of postinduction CR with gemtuzumab +induction vs induction chemotherapy alone
− 84% vs 86%
• Similar mortality, resistant disease rate in both groups
− 8% to 7%
• Gemtuzumab increased DFS in patients with favorableor intermediate cytogenetics (P < .02) withoutimprovement in overall survival
• Treatment generally tolerable with similar rates ofadverse events in each arm
• Addition of gemtuzumab to induction chemotherapymay benefit those with favorable/intermediatecytogenetics
Burnett AK, et al. ASH 2006. Abstract 13.

Studies of MDR modulation in AML
No benefitDA ± PSC-833PSC-833HOVON*
No benefitMEC ± PSC-833PSC-833ECOG
No benefitADE ± PSC-833PSC-833GALGB*
No benefitME ± CSPCSPHOVON
No benefitADE ± CSPCSPMRC
RFS/OS ImprD/HiDAC ± CSPCSPSWOG
OUTCOMEREGIMENMODULATORGROUP
*De novo > 60 yrs

Inhibition of MDR: zosuquidar
• Selective P-gp inhibitor1
• Binds to P-gp with high affinity1
• In vitro concentrations of 50-100nM circumvent P-gp-mediatedresistance 2,3
• Does not alter pharmacokinetics ofco-administered drugs2
• Phase II trial in poor-risk AMLCR/CRi 61%4
• Can be combined with inductionchemo5
1Sato Cancer Res, 1991; 2Dantzig Cancer Res, 1996; 3Green Biochem Pharmacol, 2001;4Cripe ASH, 2002 (abstr); 5Gerrard Haematologica, 2004

ECOG protocol E3999: daunorubicin + cytarabine+/- zosuquidar in older adults
Induction Consolidation I
CRorMR
Cytarabine
Consolidation II
EVALUATE
Cripe L et al. ASH 2006
Daunorubicin
Cytarabine
Zosuquidar
Daunorubicin
Cytarabine
Placebo Daunorubicin
Cytarabine
Zosuquidar
Daunorubicin
Cytarabine
Placebo

Median OS (months)MDR status and treatment arm
11.4 (n=31)
11.7 (n=32)
11.4 (n=63)
MDR -
0.08
0.5
0.08
P value
7.8 (n=318)All Patients
9.2 (n=158)Placebo
7.0 (n=160)Zosuquidar
MDR +
P = .523
Cripe L et al. ASH 2006
•Schedule modified to eliminate neurologic toxicity•No difference in OS or CR was seen overall between treatmentgroups

FLT3 inhibition in AML
• FLT3 is expressed at high levels in 70% to100% of cases of AML
• FLT3-activating mutations− Internal tandem duplication (ITD) and point
mutations occur in ~30% of patients with AML
− Lead to constitutive activation of the tyrosinekinase
− Stimulate proliferation and inhibit apoptosis of AMLcells
• Important negative prognostic factor
Gilliland DG, et al. Blood. 2002;100:1532.

FLT3 inhibitors currently in clinical trials in AML
• MLN-518 (Tandutinib, quinazoline)
• PKC412 (Staurosporine)
• SU11248 (Indolinone)
• CEP701 (Lestaurtinib, indolocarbazole)

Studies of FLT3 inhibitors in AML
Antileukemicactivity in 5/8
mutated
50-700 mg
twice daily
Adult unfit
Mutated/Wild
MLN5182
Phase I
PR in 4/4 mut
PR in 2/15 wild
50-70 mgdaily
Adult refractory
Mutated/Wild
SU112481
Phase I
HI in 3/5 Mut
HI in 5/22 Wild
60(80) mgtwice daily
Elderly unfit
Mutated/Wild
CEP7014
Phase II
HI in 14/2075 mg 3times daily
Refractory/Relapsed
Mutated
PKC4123
Phase II
OUTCOMEREGIMENPOPULATIONSTUDY
1Fiedler et al, BLOOD 2005; 2De Angelo et al, BLOOD 2006; 3Stone et al, BLOOD 2005;4Knapper et al, BLOOD 2006;
COMBINATION
THERAPY
CEP701 is synergistic withstandard therapy only if usedsimultaneously or immediatelyfollowing chemo
Levis et al, BLOOD 2004
PKC412 can be given safely insimultaneous and sequentialcombination with DHARAc
Stone et al, ASH 2005

Why Target Ftase?
• Ftase is an enzyme that modifies proteins forlocalization to cell membrane
• Many proteins are farnesylated, some of whichare important in cancer development
• Transforming activity of RAS proteins depends onfarnesylation
• Activating mutations of RAS in 15-30% of AMLs
• Blocking farnesylation may have therapeuticpotentialTipifarnib, lonafarnib
Targeting signaling pathways

Phase II study of tipifarnib in AML
• Poor risk and elderly with untreated AML
• 158 patients enrolled
• Age range: 34-85 years (median: 74)
• 600 mg twice a day for 21 days
• CR in 14%
• PR or HI 9%
• 7,3 mos median duration of CR
• 18 mos median duration of OS in responders
Lancet, et al. Blood. 2007
ORR = 23%

Phase II study of tipifarnib in AML
• Refractory/relapsed AML
• 252 patients enrolled
• Age range: 34-85 years (median: 62)
• 600 mg twice a day for 21 days
• CR/CRi in 4%
• HI in 7%
• 12 mos median duration of OS in responders
Harousseau, et al. Blood. 2007
ORR = 11%

♣ Alteration of the heritable state of gene expressioncausing loss of function (gene silencing)
♣ Gene silencing mediated by:− DNA methylation (DNA Methyltransferase)
− Histone de-acetylation (Histone deacetylase)
− RNA interference (post-transcriptional)
− MicroRNA
♣ Epigenetic events reversible
♣ Hypomethylating agents and HDACi in clinical use− Azacytidine, Decitabine
− Valproic acid, SAHA, Depsipeptide
Targeting epigenetic events
Epigenetics

Decitabine
Incorporates into RNAPro-drug for decitabine
5-Azacytidine
Incorporates into DNA
HO O
N
N
NH2
O
HO
N
OH
O
N
N
NH2
OHO
HO OH

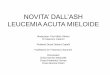
Complete response
Partial responseHematologic improvement
Response
Non responders
0
10
20
30
40
50
60
70
SubcutaneousAzacytidine
(n = 55)
IntravenousAzacytidine
(n = 25)
% o
f p
atie
nts
Azacytidine effective in AML
Silverman LR, et al. ASH 2005. Abstract 1848.
• Azacytidine evaluated inpatients meeting WHO IWGcriteria for AML
♣ Phase II/III studies
− CALGB 8421(IV administration)
− CALGB 8921 (S.C.administration)
− CALGB 9221 (S.C.administration)
− Dose schedule for alltrials: 75 mg/m2/day for7 days, every 28 days
• Median response: 279 days

Phase II decitabine in frontline AML
• Decitabine 20 mg/m2 given as IV infusion once dailyfor 5 days every 4 weeks
• 42 patients enrolled
• Median age=73.5 years
• 28 patients evaluable for response, 25 for safety
• Overall response: 29%; CR=2, CRc=2, CRi=4
• Grade 3/4 Adverse events: febrile neutropenia(32%), dyspnea (20%), hypokalemia (12%),pneumonia (28%), vomiting (8%)
Cashen A, et al. ASH 2006

Phase I-II study of 5-AZA, VPA and ATRAin AML/HRMDS
• Untreated/refractory/relapsed AML
• 53 patients enrolled (4 HRMDS), 19 in the phase I
• Age range: 5-84 years (median: 69)
• Schedule:
− 5-AZA 75 mg/m2 days 1-7, subcutaneously
− VPA 50, 62.5 and 70 mg/kg days 1-7, orally
− ATRA 45 mg/m2, days 3-5
• CR/CRi in 29%
• BM response in 13%
• 26 weeks median duration of responseSoriano, et al. Blood. 2007
ORR = 42%

Phase I study of DAC and VPA in AML
• 25 untreated/relapsed AML
• Age range: 37-83 years (median: 70)
• 14 pts treated with DAC alone (d 1-10)
− 8, 15 mg/m2/d
− 6, 20 mg/m2/d
• 11 pts treated with DAC at OBD + VPA (d 5-21)
− 3, 15 mg/kg
− 6, 20 mg/kg
− 2, 25 mg/kg
♣ ORR 52% (11 pts, 4 CR, 4 CRi, 3 PR)
Blum et al. JCO. 2007
OBD
To determine the OBD of DAC alone and MTD of VPA + DAC
encephalopathy

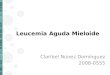
Critical pathways that may be targeted in leukemiastem cells
Differentiation
Quiescence
Self-renewal
Apoptosis
LSC
•PIK3/PTEN•JunB/AP-1 pathway•Wint/β-Catenin•HOX genes•Notch•BMI-1•Shh

UpstreamUpstream activatorsactivators
DownstreamDownstream effectorseffectors
Rapamycin/Analogs

A Phase I dose escalation study of the mTORinhibitor sirolimus and MEC chemotherapy in AML
Sirolimus combinations in AML Salvage: A Dose Finding Phase IStudy of Sirolimus + mitoxantrone/etoposide/ara-C
•sirolimus MTD (12 mg loading dose and then 4 mg daily)•MEC (M at 8 mg/m2 X 5d, E at1 00 mg/m2 X 5d, ara-C at1000 mg/m2 X 5d)•N=23
Preliminary Results:•CR = 4 (17%)•Therapeutic sirolimus levels safely achieved
Conclusions:•Sirolimus can be combined with chemotherapy•Myelosuppression and hepatoxicity (hyperbilirubinemia) isthe predominant toxicity•Phase II study will be required to test efficacy
Luger S, et al Blood 2006

Conclusive remarks
• AML still a challenge, particularly in elderly
• A wide range of novel agents available for phaseIII clinical trials (“multitargeted therapy”)
• New strategies should consider combinationtherapies
• LSC targeted therapy
Recommended