5/12/2018 Management of Hypertension in Clinical Dentistry - slidepdf.com
http://slidepdf.com/reader/full/management-of-hypertension-in-clinical-dentistry 1/16
Management of Hypertension in Clinical Dentistry
Dr. Jin Y. Kim and Dr. E. Barrie Kenney
PIC Homepage | Member Homepage
DEFINITION
y Hypertension is a persistently raised blood pressure resulting from increased
peripheral arteriolar resistance. This condition is also known as hypertensivecardiovascular disease and hypertensive heart disease (HHD).
y The cause of hypertension is unknown in most cases and the disorder istherefore termed essential hypertension.
y P rimary hypertension, and idiopathic hypertension are synonymous and
interchangeable terms, meaning that no cause other than genetics can be
found.
Dental management in hypertensive patients can be complicated, since any
procedure causing stress can further increase the blood pressure and can precipitateacute complications such as a cardiac arrest or a cerebrovascular accident. Chronic
complications of hypertension, especially impaired renal function, can affect dental
management.
The diagnosis of hypertension is made at an arbitrary point when the blood
pressure at rest exceeds 160 mm Hg systolic pressure or where diastolic pressureexceeds 95 mm Hg (World Health Organization), or where systolic is above 140
mm Hg and diastolic above 90mm Hg (American Heart Association). By these
criterion some 10 per cent or more of the population in the U.S. are hypertensive.
A more recent consensus report of the Fifth Joint National Committee (JNC-V) hasset arbitrary limits for resting and seated arm blood pressure, which defines
hypertension to be systolic pressure above 140 mm Hg, and diastolic pressure
above 90 mm Hg. This classification also includes a systolic component, unlike the
previous guideline by the same committee (JNC-IV, 1988) which definedhypertension as mean diastolic pressure of 90 mm Hg or greater , with no regard toa systolic component. The newer 1993 guideline has set 4 stages of hypertension
which emphasize the seriousness and severity of the condition.

5/12/2018 Management of Hypertension in Clinical Dentistry - slidepdf.com
http://slidepdf.com/reader/full/management-of-hypertension-in-clinical-dentistry 2/16
A rise in diastolic blood pressure is much more significant than a rise in systolic
pressure, since the higher diastolic pressure translates to a prolonged greater
baseline arterial pressure, and therefore may precipitate arteriosclerosis and other
end-organ pathology.
CLASSIFICATION OF BLOOD PRESSURE IN ADULTS 18OR OLDER
SYSTOLIC DIASTOLIC
Category Pressure (mm HG) Pressure (mm Hg)
Normal BP < 130 < 85
High Normal BP 130-139 85-89
Hypertension
Stage I 140-159 90-99
Stage II 160-179 100-109
Stage III 180-209 110-119
Stage IV > 210 > 120
From the Joint National Committee on Detection, Evaluation , and Treatment of
High Blood Pressure. The fifth report of the Joint National Committee on
Detection, Evaluation, and Treatment of High Blood Pressure. Arch Intern
Med 153:154-83,
1993
The blood pressure is easily measured with a sphygmomanometer. Since the blood pressure increases with anxiety, measurements should be made with the patientrelaxed and fully at rest. Generally, the first three readings tend to be highest. But
in an office practice, taking two values and averaging is recommended.
TABLE 3: TECHNIQUE FOR RECORDING THE BLOOD PRESSURE
1. Seat and relax the patient.2. Place sphygmomanometer cuff on right upper arm with about 3cm of skin
visible at the antecubital fossa. ( P roper cuff size should be chosen; too small
cuff on an obese or large, muscular arm falsely elevates the reading; toolarge cuff on a small arm gives a falsely low reading.)
3. Palpate radial pulse.
5/12/2018 Management of Hypertension in Clinical Dentistry - slidepdf.com
http://slidepdf.com/reader/full/management-of-hypertension-in-clinical-dentistry 3/16
4. Inflate cuff to about 200 to 250 mmHg, or until the radial pulse is no longer
palpable.
5. Deflate cuff slowly while listening with stethoscope over the brachial artery
over skin on inside of arm below cuff.6. Record the systolic pressure as the pressure when the first tapping sound
(Korotkoff sound) appear.7. Deflate cuff further until the tapping sounds become muffled (diastolic
pressure).
8. Repeat. Record blood pressure as systolic/diastolic pressure.
PATHOGENESIS AND RISK ASSESSMENT
Essential hypertension becomes more common as age advances and genetic
influences, obesity, excessive salt intake and a variety of other factors arecontributory. Hypertension is secondary to defined diseases, particularly renal or endocrine disorders, in about 10-20 percent of hypertensive cases and occasionally
can be secondary to the use of oral contraceptives.
Acute emotion, particularly anger and anxiety, can cause transient rises in blood
pressure by release of catecholamines (epinephrine and norepinephrine) and about40 percent of hypertensive patients have raised levels of circulating catecholamines
(epinephrine and norepinephrine) and may therefore have abnormal sympathetic
activity.
When the patient has a history of hypertension there is the possibility of both
congestive heart failure or angina pectoris. It is natural to think of stroke first whenconfronted with a history of hypertension, and it is true that hypertension, diabetes,
and cerebral hemorrhage are commonly linked, but the fact is that 65 percent of
hypertensives die of heart disease, whereas 20 percent demonstrate predominantlycerebral complications, except in hypertensive African American persons. African
Americans tend to develop hypertension earlier in life. It is frequently more severe,
and resulting in a higher mortality at a younger age, more commonly from strokethan from coronary artery disease. Since hypertension is one of several
predisposing factors for premature coronary disease, it is important to look for
other factors that may add to that risk , especially hyperlipidemia and cigarettesmoking. Diabetes and physical inactivity likewise are important.
MANAGEMENT IN CLINICAL DENTAL SITUATIONS
5/12/2018 Management of Hypertension in Clinical Dentistry - slidepdf.com
http://slidepdf.com/reader/full/management-of-hypertension-in-clinical-dentistry 4/16
Dentists have a unique opportunity to detect cases of hypertension since patientvisits at routine intervals are encouraged. It is a professional responsibility of a
dental clinician to inform the patient of their hypertensive state and to offer
medical advice, including appropriate referrals.
There are no recognized oral manifestations of hypertension but antihypertensivedrugs can often cause side-effects, such as:
y xerostomia, y gingival overgrowth,
y salivary gland swelling or pain,
y lichenoid drug reactions,
y erythema multiforme,
y taste sense alteration, and
y paresthesia.
Dental clinician must focus on the actions, interactions and adverse effects of theantihypertensive medications, as well as the overall management of blood pressureof the patient in the dental chair. (see Medications)
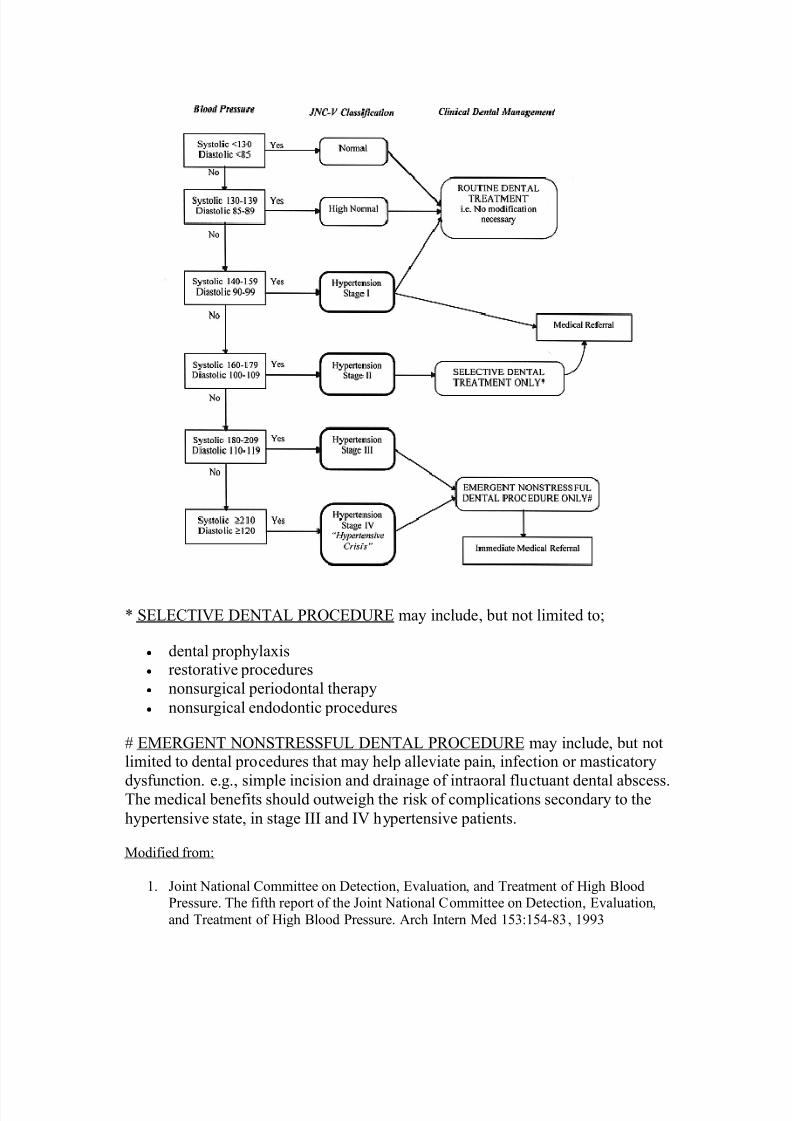
The appropriate modifications for differing stages of hypertension is outlined in the
algorithm presented below. (see ALGORITHM) There are, however , several areas
of general dental management to be considered in the hypertensive patients.
1. ANESTHESIA
A. Local Anesthesia
Dental patients with hypertension are best treated under local anesthesia being surethat the anesthesia is complete so that no anxiety induced elevation of blood
pressure occurs. The use of vasoconstrictors such as epinephrine in local anesthetic
agents is known to have negligible influences on blood pressure in hypertensive
patients, according to numerous clinical studies. Data in regard to epinephrine-containing local anesthetics has consistently shown that blood pressure and heart
rate are minimally affected by the typically low dose and short duration of the druguse in dentistry, both in healthy and those with existing cardiovascular conditions.
Nonetheless, the use of epinephrine-containing anesthetics in patients with
uncontrolled hypertension, and elective dental procedures are contraindicated.
According to Muzyka & Glick (JADA 1997),
" the benefits of the small doses of epinephrine used in dentistry, when administered properly,far outweigh the cardiovascular disadvantages"
5/12/2018 Management of Hypertension in Clinical Dentistry - slidepdf.com
http://slidepdf.com/reader/full/management-of-hypertension-in-clinical-dentistry 5/16
The use of aspirating syringes in local anesthetics is imperative to avoidintravenous, intrarterial, intraligamentary and intrabony injections, which could
potentially precipitate further anxiety and thus rise in pressure and possible
arrhythmias.
B. General Anesthesia
All antihypertensive drugs are potentiated by general anesthetic agents, especially barbiturates. General anesthesia tends to cause vasodilation. A severely reduced
blood supply to vital organs can be dangerous in healthy individuals, but in thehypertensive person with vascular disease there is greater risk as the tissues have
become adapted to a raised blood pressure which is needed to overcome the
resistance of the vessels and maintain adequate perfusion. A fall in blood pressure below the critical level needed for adequate perfusion of vital organs such as the
kidneys, can therefore be fatal. Hypokalemia as a result of diuretics may beassociated with arrhythmias. Some inhalant anesthetics (halothane, enfluane, andisoflurane) are similar in action to calcium slow channel antagonists and so reduce
blood pressure significantly.
2. ANXIETY CONTROL
The anxiety and stress associated with dental treatment typically causes a rise in blood pressure and may precipitate cardiac arrest or a cerebrovascular accident.
Preoperative reassurance and oral sedation may help in alleviating anxiety relatedrise in pressure. Use of sedatives the night before a procedure may also be used.
Relative analgesia technique using nitrous oxide (N2O) can also reduce both
systolic and diastolic pressure by up to 10-15mm Hg, after approximately 10
minutes of use, preoperatively. Use of oral sedation or nitrous oxide sedation mayreduce blood pressure to acceptable levels, allowing initiation of local anesthesia
(with or with vasoconstrictor).
3. TIMING OF DENTAL APPOINTMENTS
The increase of blood pressure in hypertensive patient is associated with the hourssurrounding awakening that peaks by midmorning. This fluctuation of blood
pressure tends to be less likely in the afternoon. Afternoon appointments are
recommended over mornings for this reason.

5/12/2018 Management of Hypertension in Clinical Dentistry - slidepdf.com
http://slidepdf.com/reader/full/management-of-hypertension-in-clinical-dentistry 6/16
4. ORTHOSTATIC HYPOTENSION
Orthostatic hypotension may be a problem in patients using antihypertensive
agents that reduce sympathetic outflow or peripheral vasodilatory actions,
such ascentrally acting a-2-adrenergic agonists, post-ganglionic adrenergic inhibitors, a-1-adrenergic antagonists, and diuretics. Management of orthostatic hypotension
includes avoiding sudden postural changes, such as return to sitting position from
the supine operating position. The patient should also be instructed to stay seated
for a short period until such time that adequate cerebral perfusion has occured.
5. OTHER DENTAL CONCERNS
Aspirin is now commonly taken by patients with hypertension to decreaseassociated coronary or cerebral vascular thrombotic disease, and aspirin may cause
bleeding problems. Many patients with hypertension develop systolic heart
murmurs, in which case prophylaxis for endocarditis
Algorithm for Management of Hypertensive Dental Patient
5/12/2018 Management of Hypertension in Clinical Dentistry - slidepdf.com
http://slidepdf.com/reader/full/management-of-hypertension-in-clinical-dentistry 7/16
* SELECTIVE DENTAL PROCEDURE may include, but not limited to;
y dental prophylaxisy restorative procedures
y nonsurgical periodontal therapy
y nonsurgical endodontic procedures
# EMERGENT NONSTRESSFUL DENTAL PROCEDURE may include, but notlimited to dental procedures that may help alleviate pain, infection or masticatory
dysfunction. e.g.,
simple incision and drainage of intraoral fluctuant dental abscess.The medical benefits should outweigh the risk of complications secondary to the
hypertensive state, in stage III and IV hypertensive patients.
Modified from:
1. Joint National Committee on Detection, Evaluation, and Treatment of High Blood
Pressure. The fifth report of the Joint National Committee on Detection, Evaluation,
and Treatment of High Blood Pressure. Arch Intern Med 153:154-83, 1993

5/12/2018 Management of Hypertension in Clinical Dentistry - slidepdf.com
http://slidepdf.com/reader/full/management-of-hypertension-in-clinical-dentistry 8/16
2. Muzyka B.C., and M. Glick. The hypertensive dental patient, JADA 128: 1109-1120, 1997
ORAL MEDICATIONS USED FOR MANAGEMENT OF HYPERTENSION
(common brand names available in the U.S. is shown in bracket)
Diuretics Beta-Adrenergic Blockers
Central Acting Inhibitors
Peripheral-Acting Adrenergic Inhibitors
Non selective Alpha and Beta Adrenergic Blockers
Vasodilators
Angiotensin-Converting Enzyme (ACE) Inhibitors
DIUR ETICS
TOP
A. Thiazides and related sulfonamides
Mode of action:
y increase the excretion of Na+, Cl-, and water by interfering with they transport of sodium ions across the renal tubular epithelium
y reduce blood pressure by decreasing cardiac output
Representative agent:
y hydrochlorothiazide
Side effects:
y xerostomia
y increased thirsty orthostatic hypotensiony polyuria
y dizziness
y fatigue, weakness
5/12/2018 Management of Hypertension in Clinical Dentistry - slidepdf.com
http://slidepdf.com/reader/full/management-of-hypertension-in-clinical-dentistry 9/16
B. Loop diuretics (also called High-efficiency diuretics)
Mode of action:
y inhibit Na+ and Cl- reabsorption in the descending limbs of the loop of
Henley enhance excretion of K+, Mg++, and Ca++.
y reduce blood pressure by decreasing fluid volume and thereby reducing
cardiac output
Representative agents:
y furosemide
y ethacrynic acid
y bumetanide
Side effects:
y xerostomiay increased thirsty lichenoid drug reaction
y neutropenia
y leukopeniay anemia
y orthostatic hypotension
y renal failure
C. Potassium-sparing agents
Mode of action:
y competitive antagonism of the endogenous mineralocorticoid aldestronechange
y pressure levels and reduce blood pressure by reducing total fluid volume
Representative agents:
y amiloridey spironolactone (Aldactone)
y triamterene
5/12/2018 Management of Hypertension in Clinical Dentistry - slidepdf.com
http://slidepdf.com/reader/full/management-of-hypertension-in-clinical-dentistry 10/16
Side effects:
y xerostomiay increase thirst
y gingival bleeding (spironolactone)
y lichenoid drug reaction
D. Carbonic anhydrase inhibitors
Mode of action:
y inhibition of the enzyme carbonic anhydrase in the proximal and distalsegments of the renal tubule so as to allow diuresis
y reduce blood pressure by decreasing fluid volume and thereby reducingcardiac output
Representative agents:
y acetazolamidey dichlorphenamide
y methazolamide
Side effects:
y xerostomia
y burning mouth, tongue, lips
y parasthesiay metallic taste
y thirst
BETA-ADR ENER GIC BLOCKERS
TOP
Mode of action:
y blocks b-1 and b-2 receptors in

5/12/2018 Management of Hypertension in Clinical Dentistry - slidepdf.com
http://slidepdf.com/reader/full/management-of-hypertension-in-clinical-dentistry 11/16
y cardiac effect: by blocking beta-1 receptors, reduces rate of SA node firing
rate, slows the conduction through AV node, and reduces contractile
strength and automaticity
y in the vascular system, reduce blood pressure by reducing cardiac output
and increasing peripheral resistance
Representative agents:
y Acebutololy atenolol
y metoprolol
y nadolol
y penbutolol
y pindololy propranolol
y timolol
Side effects
y orthostatic hypotensiony xerostomia
y sore throat
y nasal stuffiness
y asthmay drowsiness
y depression
y fluid retention
CENTRAL-ACTING ADNERNER GIC INHIBITORS
TOP
Mode of action:
y direct effect on alpha 2-adrenoceptor (sympathetic vasomotor center inCNS), which reduces impulses in sympathetic nervous system
y reduces blood pressure by decreasing peripheral resistance and by
decreasing plasma renin levels
Representative agents:

5/12/2018 Management of Hypertension in Clinical Dentistry - slidepdf.com
http://slidepdf.com/reader/full/management-of-hypertension-in-clinical-dentistry 12/16
y clonidine (Catapres)y methldopa (Aldomet)
y guanabenz
y guanfacine
Side effects:
y xerostomiay taste changes
y salivary pain or swelling
y palpitation
y ECG abnormalities
y insomnia
y anxiety
y drowsiness
PER IPHERAL-ACTING ADR ENER GIC INHIBITORS
TOP
Mode of action:
y inhibits the active uptake of catecholamines into storage vesicles of the
nerve terminaly decrease blood pressure by decreasing sympathetic tone, and by decreasing
peripheral vascular resistance
Representative agents:
y guanadrely guanethidine
y Rauwolfia alkaloids (e.g. reserpine)
Side effects:
y xerostomiay bleeding
y thrombocytopenia purpura
y orthostatic hypotension
y drowsiness, fatigue, weakness
5/12/2018 Management of Hypertension in Clinical Dentistry - slidepdf.com
http://slidepdf.com/reader/full/management-of-hypertension-in-clinical-dentistry 13/16
Mode of action:
y decrease total vascular resistance by vasodilation of arterioles and
capacitance veins, by selective blocking of alpha 1-receptors on vascular
smooth muscle
Representative agents:
y selective alpha 1-adrenergic blockerso prazosin (Minipress)
o terazosin (Hytrin)
Side effects:
y xerostomiay orthostatic hypertension, postural dizziness
y nausea, Gl upset
y drowsiness, fatigue, weakness
y anxiety, depression
NONSELECTIVE ALPHA- AND BETA- ADR ENER GIC BLOCKERS
TOP
Mode of action:
y competitive blocking of both a- and b- adrenergic receptors (greater affinityfor b- receptors) on vascular smooth muscle
y decrease blood pressure by decreasing peripheral vascular resistance
Representative agents:
y labetalol (Normodyne, Trandate)
Side effects:
y xerostomiay taste changes
5/12/2018 Management of Hypertension in Clinical Dentistry - slidepdf.com
http://slidepdf.com/reader/full/management-of-hypertension-in-clinical-dentistry 14/16
y orthostatic hypotension
y nausea, Gl upset
y nervousness
y anxiety, depressiony parasthesia
y bronchospasm
VASODILATORS
TOP
Mode of action:
y direct relaxation (vasodilation) of arteriolar smooth muscle
y decrease blood pressure by decreasing peripheral vascular resistance
Representative agents:
y hydralazine (Apresoline)
y minoxidil (Loniten)
Side effects:
y nasal congestiony lupus-like syndromes
y leukopenia
ANGIOTENSIN-CONVERTING ENZYME (ACE) INHIBITORS
TOP
Mode of action:
y inhibits ACE preventing conversion of angiotension I to angiotensin II, resulting in dilation of arteriole, venous vessels
y decrease blood pressure by removing the vasoconstricting effect of ACE and
thereby decreasing peripheral vascular resistance
5/12/2018 Management of Hypertension in Clinical Dentistry - slidepdf.com
http://slidepdf.com/reader/full/management-of-hypertension-in-clinical-dentistry 15/16
Representative agents:
y captopril (Capoten)
y enalapril (Vasotec)
y lisinopril (Zestril
,
Prinivil)
Side effects:
y xerostomiay loss of taste
y angiodema
y glossitis
y oral ulceration (Stevens-Johnson syndrome - captopril, enapril)y lichenoid drug reaction
y renal insufficiency
Slow Channel Calcium-Entry Blocking Agents
Mode of action:
y direct relaxation (vasodilation) of coronary and peripheral arteriolar smooth
muscles by blocking Ca++ influx
Representative agents:
y verapamil (Calan, Isoptin)
y dilitiazen
y nifedipine (Adalat, Procadia)
y nitrendipine
Side effects:
y gingival hyperplasia
y xerostomiay orthostatic hypotension
y light-headedness, nausea
y edema
y flushing, skin reactions
y congestive heart failure

5/12/2018 Management of Hypertension in Clinical Dentistry - slidepdf.com
http://slidepdf.com/reader/full/management-of-hypertension-in-clinical-dentistry 16/16
Do you wish to take this course for continuing education credit? Yes
Top of Page | PIC Homepage | Member Homepage
R EFER ENCES
1. Joint National Committee on Detection, Evaluation, and Treatment of HighBlood Pressure. The fifth report of the Joint National Committee on
Detection, Evaluation, and Treatment of High Blood Pressure. Arch Intern
Med 153:154-83, 19932. Muzyka B.C., and M. Glick. The hypertensive dental
patient, JA D A 128:1109-1120, 1997
3.
Rose L.,
and D. Kaye. Internal Medicine for Dentistry,
2nd ed. C.V. WesbyCo., St. Louis, 1990.
4. Niedle E.N., and J.A. Yagiela. Pharmacology and Therapeutics for
Dentistry, (3rd Ed.) Mosby, St. Louis. 19895. Gage T.W., and F.A. Pickett. Dental Drug Reference. Mosby, St. Louise.
1996
Recommended