Management of Persistent Pulmonary Hypertension of the Newborn (PPHN)yp ( )Arlene M Sheehan NNPStanford Children’s HospitalNeonatal ECMO Coordinator
State Level SymposiumEvidence Based Care of the High-Risk Neonate
Shrimad Rajchandra HospitalShrimad Rajchandra HospitalDharampur
Introduction Neonatal respiratory failure occurs in 6-7% of neonates of all
gestational ages in India1gestational ages in India• Respiratory problems are responsible for 20% of neonatal mortality in
India2
P i t t l h t i (PPHN) li t th f Persistent pulmonary hypertension (PPHN) complicates the course of approximately 10% of infants with respiratory failure.
Newborns with hypoxic respiratory failure and/or PPHN are at riskNewborns with hypoxic respiratory failure and/or PPHN are at risk for death (5-10%), neurologic injury (25%), and other morbidities.
1Kumar A, Bhat BV. Epidemiology of respiratory distress of newborns. Indian J Pediatr 1996;63:93e8.
2Bajas, M, Goya S ,Jain, B. Clinical profile of neonates with respiratory distress. International Journal of Contemporary Pediatrics Bajad M et al. Int J Contemp Pediatr. 2016 Aug;3(3):1009-1013
PPHN: Definition PPHN is caused by failure of the transition from fetal to
newborn circulation, which normally occurs after birth., y
PPHN is characterized by• High pulmonary vascular resistance (PVR) or high blood pressure in the
lungs• Shunting of deoxygenated blood from area of high pressure to area of
lower pressure (pulmonary circulation to systemic circulation) • Right to Left Shunt: blood shunts right to left through fetal channels,
patent ductus arteriosus [PDA] and/or patent foramen ovale [PFO}
PPHN results in:PPHN results in:• Hypoxemia • High right-sided heart pressures• Right heart failure• Right heart failure
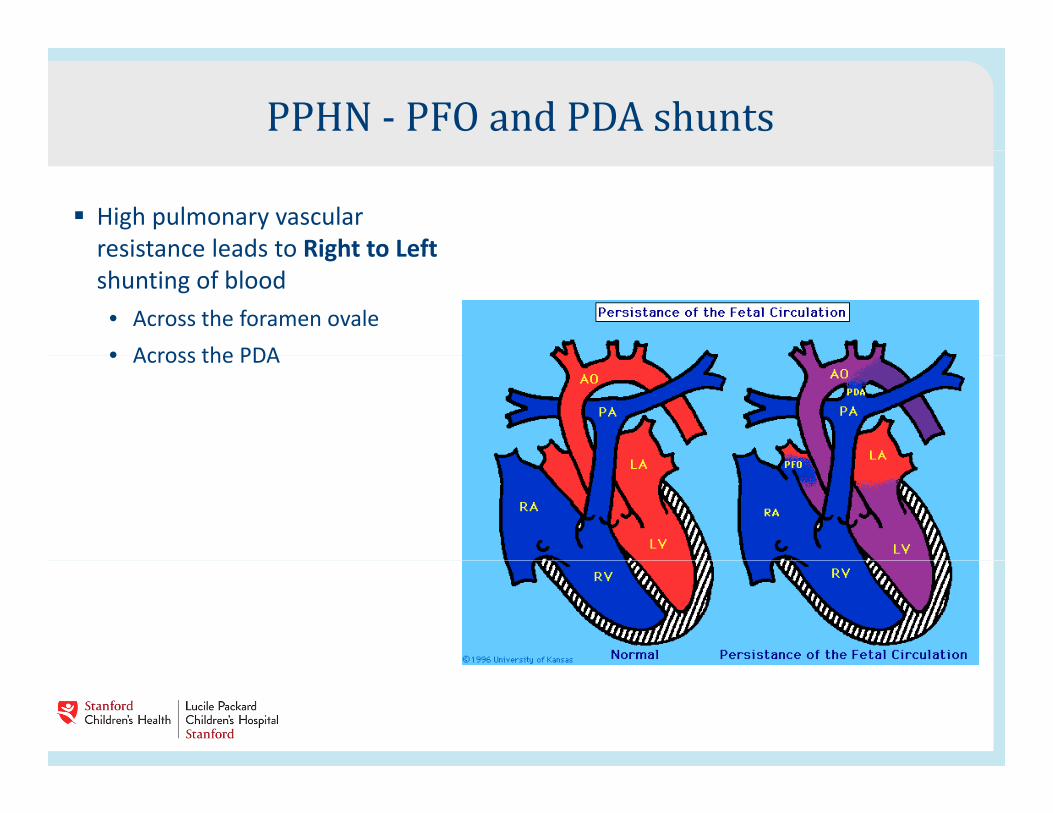
PPHN - PFO and PDA shunts High pulmonary vascular
resistance leads to Right to Leftresistance leads to Right to Left shunting of blood• Across the foramen ovale• Across the PDA• Across the PDA
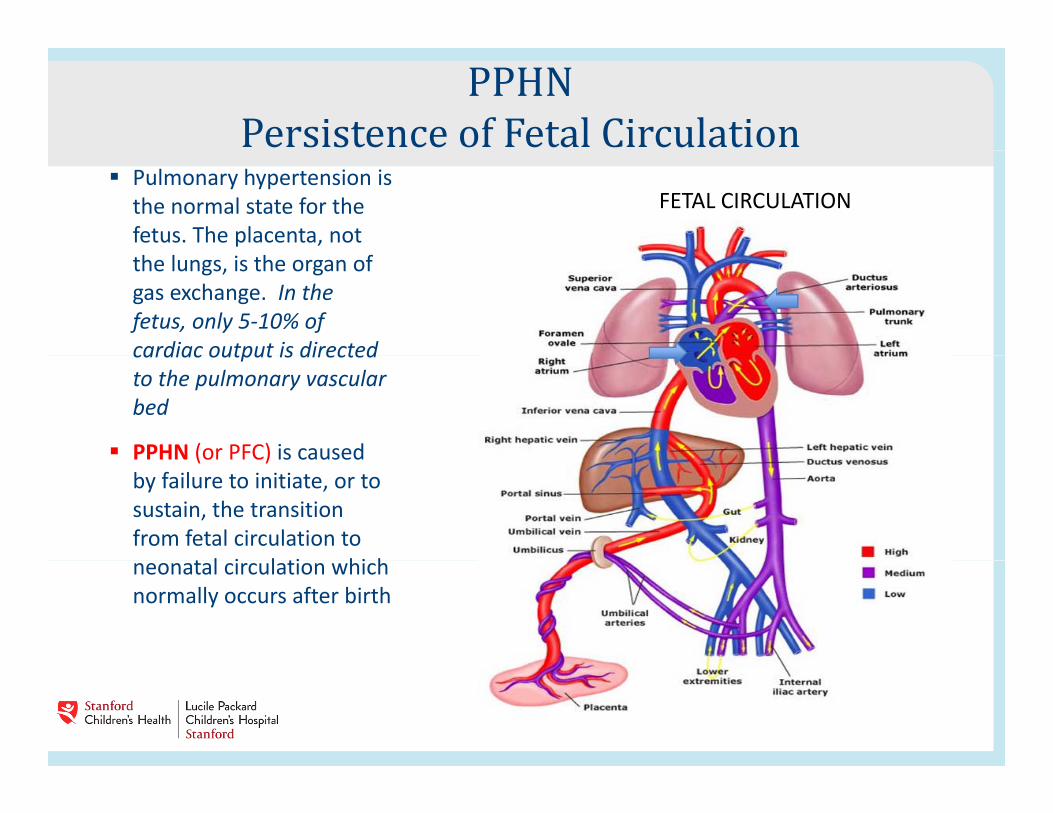
PPHNPersistence of Fetal Circulation Pulmonary hypertension is
the normal state for the fetus. The placenta, not
FETAL CIRCULATION
the lungs, is the organ of gas exchange. In the fetus, only 5-10% of cardiac output is directedcardiac output is directed to the pulmonary vascular bed
PPHN (or PFC) is causedPPHN (or PFC) is caused by failure to initiate, or to sustain, the transition from fetal circulation to
t l i l ti hi hneonatal circulation which normally occurs after birth
Transitional CirculationThe transition from fetal to normal circulation is triggered by mechanical distension of the lung with first breaths, followed by a decrease in carbon dioxide levels and an increase in oxygenation as the lungs become air filled and start to ventilate. yg g
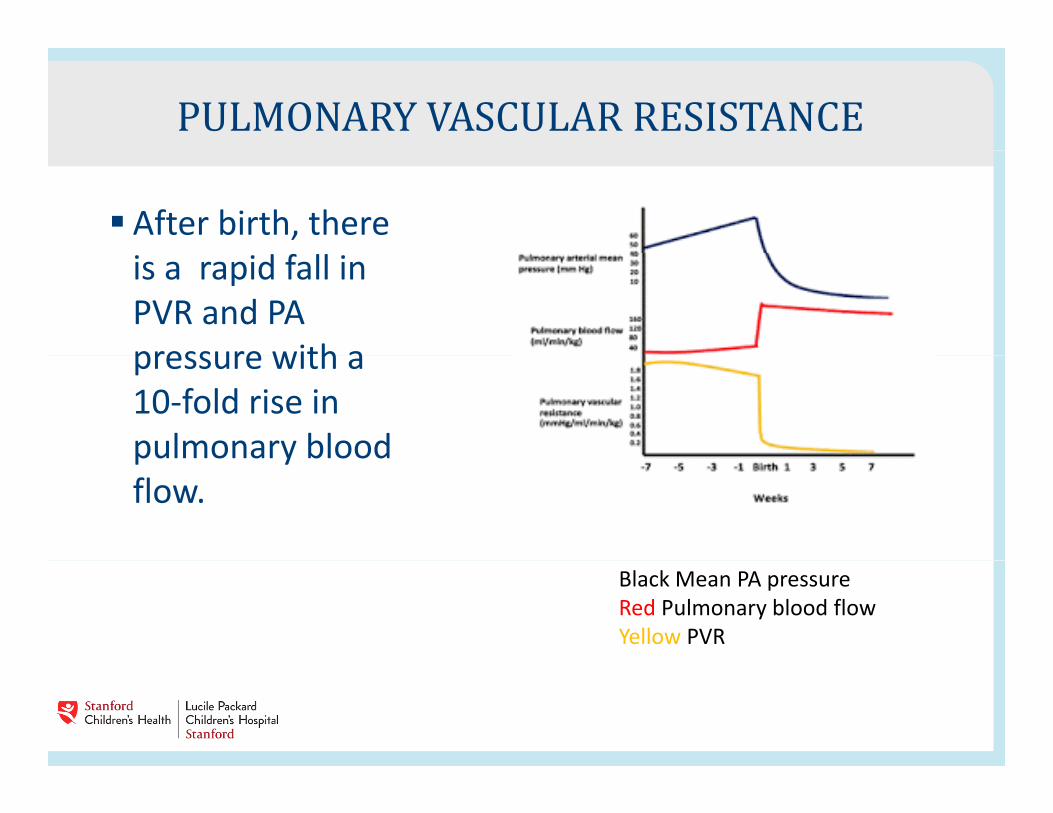
PULMONARY VASCULAR RESISTANCE After birth, there
is a rapid fall in PVR and PA pressure with apressure with a 10-fold rise in pulmonary bloodpulmonary blood flow.
Black Mean PA pressureRed Pulmonary blood flowYellow PVR
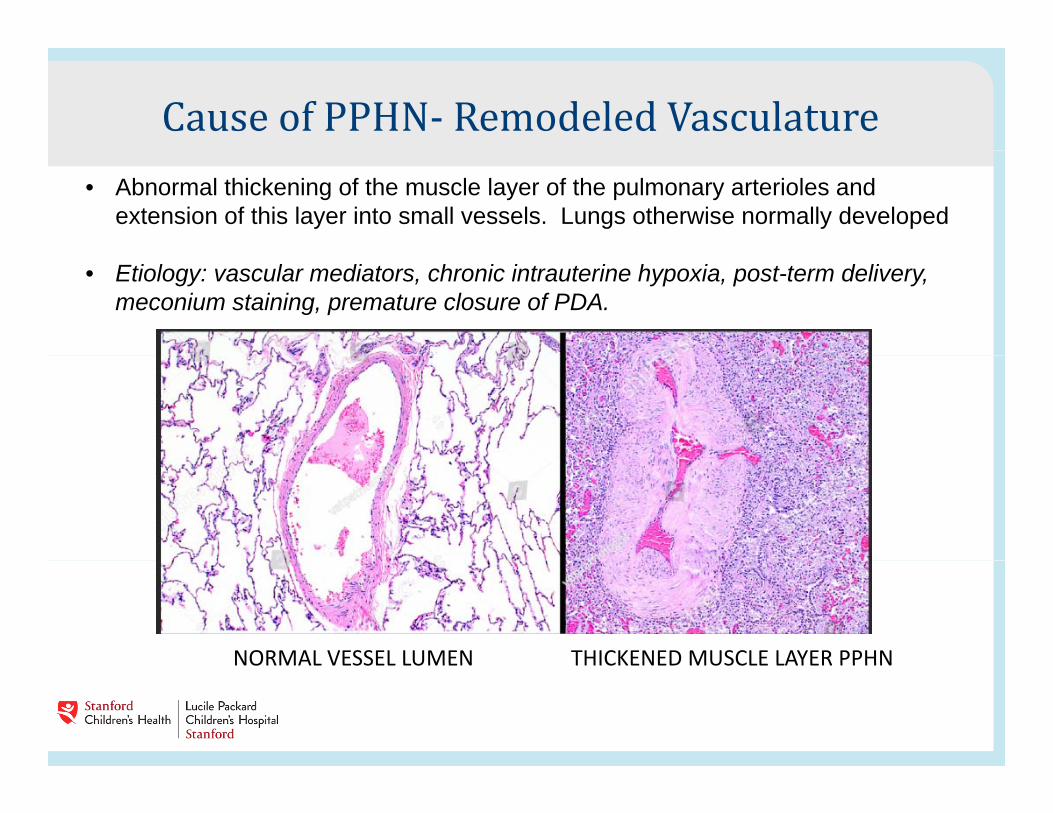
Cause of PPHN- Remodeled Vasculature• Abnormal thickening of the muscle layer of the pulmonary arterioles and
extension of this layer into small vessels. Lungs otherwise normally developed
• Etiology: vascular mediators, chronic intrauterine hypoxia, post-term delivery, meconium staining, premature closure of PDA.
NORMAL VESSEL LUMEN THICKENED MUSCLE LAYER PPHNNORMAL VESSEL LUMEN THICKENED MUSCLE LAYER PPHN
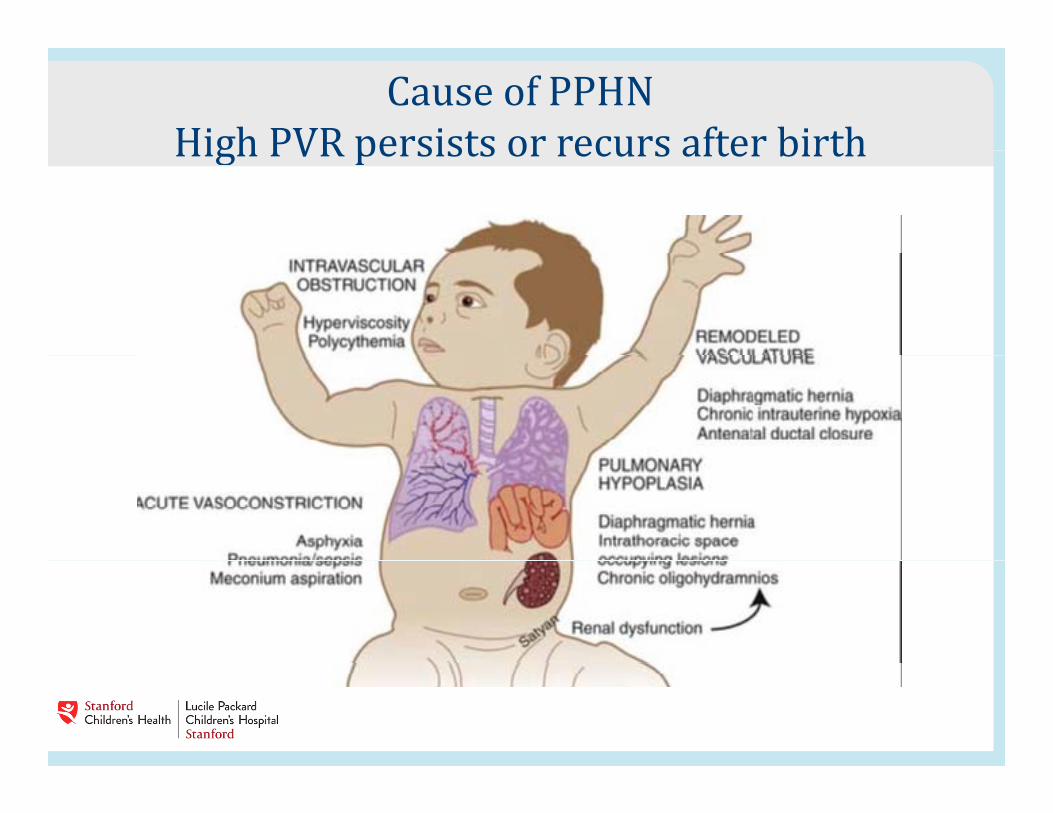
Cause of PPHNHigh PVR persists or recurs after birthHigh PVR persists or recurs after birth
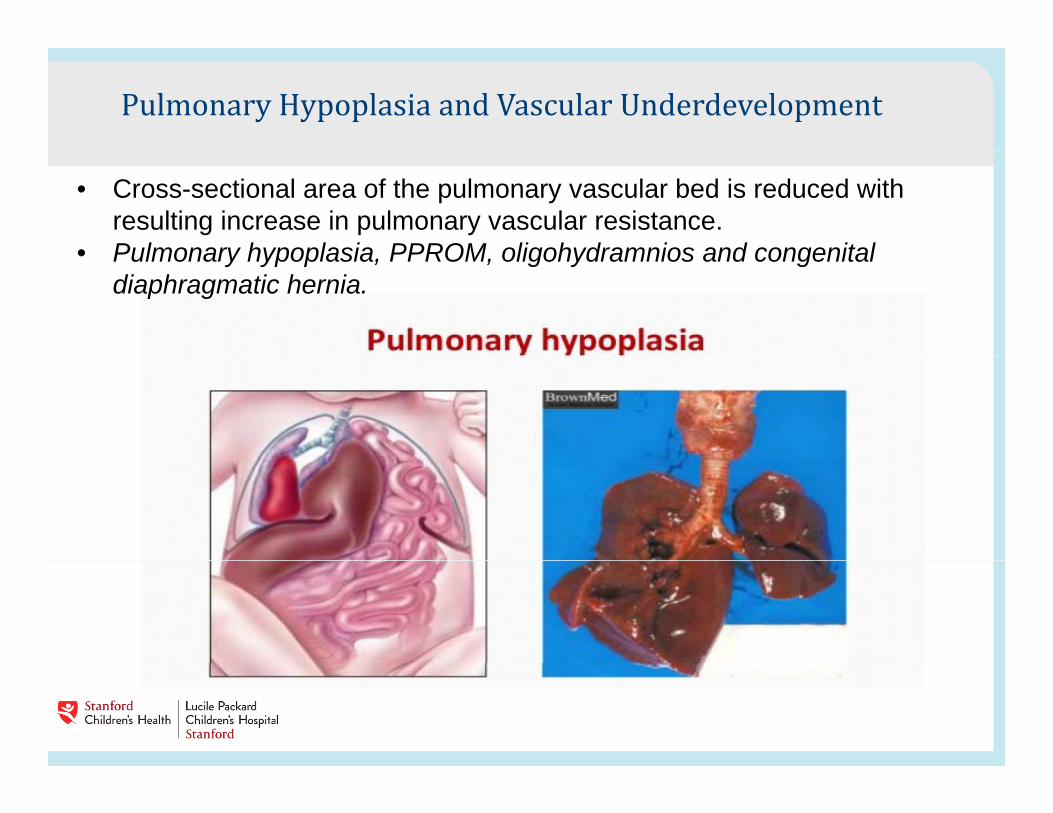
Pulmonary Hypoplasia and Vascular Underdevelopment• Cross-sectional area of the pulmonary vascular bed is reduced with
resulting increase in pulmonary vascular resistance. • Pulmonary hypoplasia PPROM oligohydramnios and congenital• Pulmonary hypoplasia, PPROM, oligohydramnios and congenital
diaphragmatic hernia.
Vascular Underdevelopment : Alveolar Capillary DysplasiaDysplasia
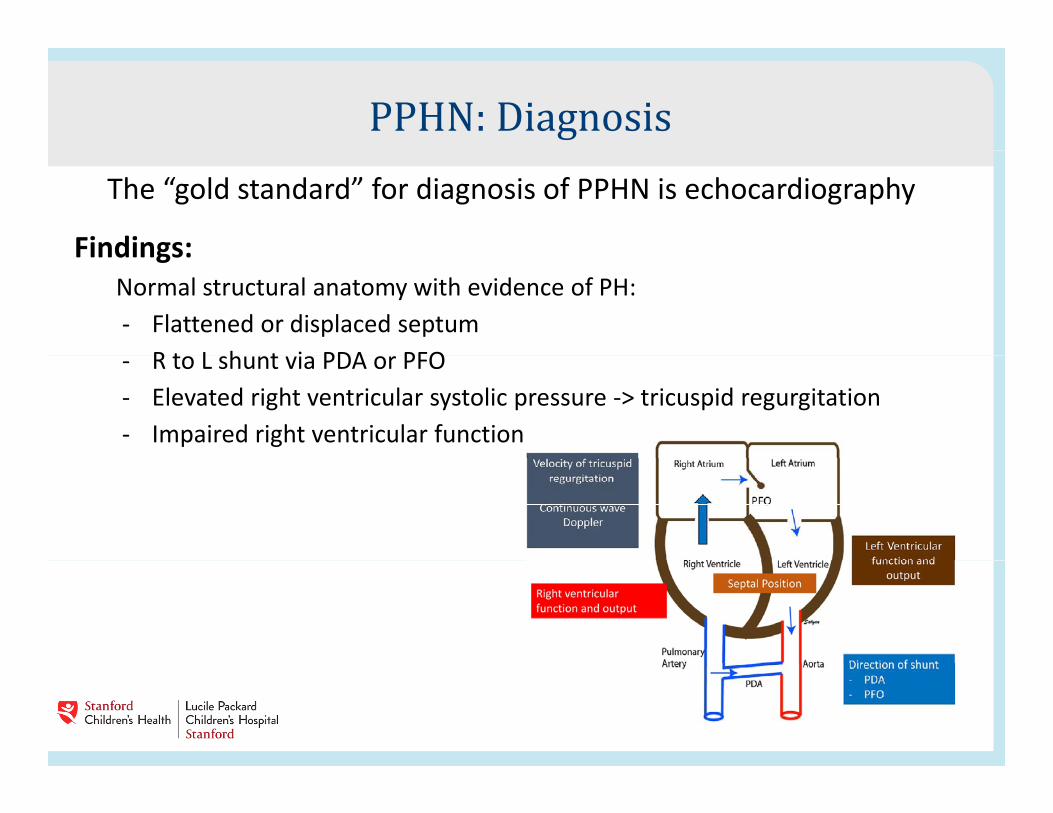
PPHN: DiagnosisThe “gold standard” for diagnosis of PPHN is echocardiography
Findings:Findings:Normal structural anatomy with evidence of PH:- Flattened or displaced septum
R t L h t i PDA PFO- R to L shunt via PDA or PFO- Elevated right ventricular systolic pressure -> tricuspid regurgitation- Impaired right ventricular function
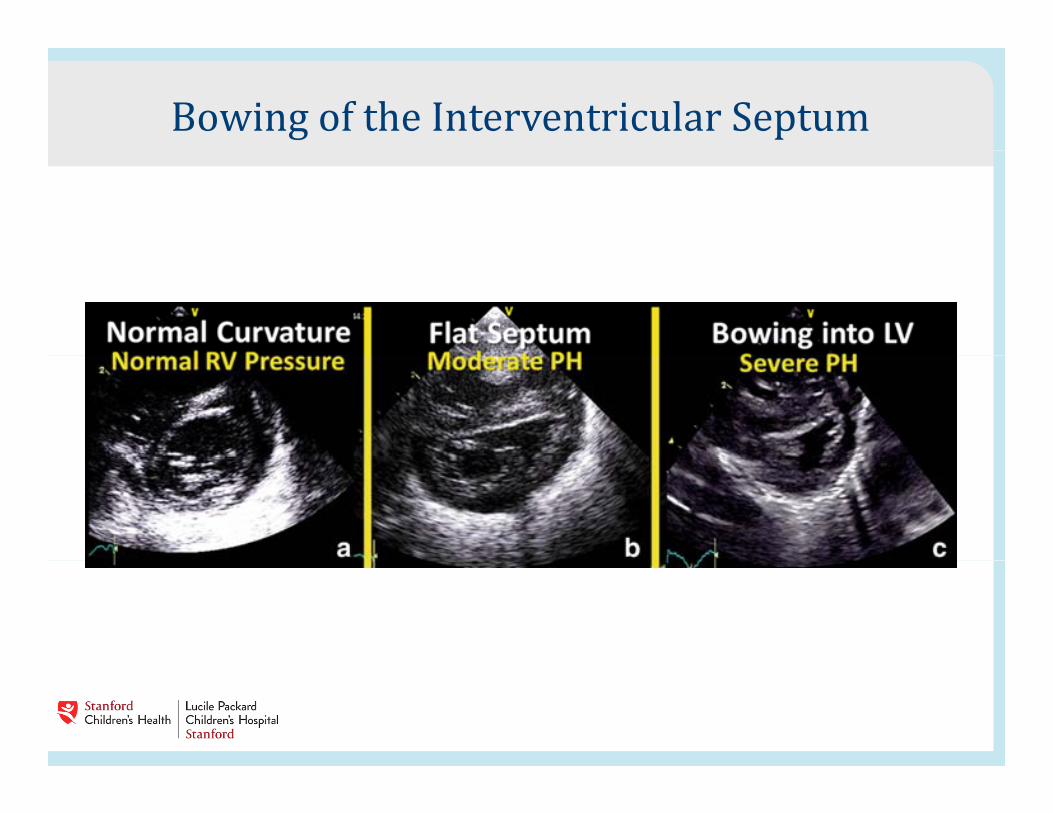
Bowing of the Interventricular Septum
PPHN Diagnosis Cyanotic, hypoxic newborn. Late Preterm, Term or Post Term
• History • Evidence of Intrauterine asphyxia?• Is the infant post-dates?
• Chronic intrauterine hypoxia causing pulm vasoconstriction• Was there meconium?Was there meconium?
• Airway obstruction and surfactant inactivation• Inflammatory mediators- cytokines, thromboxane, angiotensin
• Were there risk factors for sepsis? k d d l l h• Cytokine induced pulmonary vascular changes
• Maternal smoking or NSAID exposure?• In utero closure of ductus
• Gestational or Insulin Dependent Diabetes? Obesity?p y• Higher incidence of resp distress and PPHN.
• Polycythemia and Hyperviscosity• Increase PVR
PPHN Diagnosis• Physical Exam of Cyanotic infant
• LGA or SGA?LGA or SGA?• Is there a scaphoid abdomen?
• CDHh f l ?• Is the infant limp, apneic?
• Sepsis• Does the infant have increased WOB?
• Yes- Pulmonary etiology. TTN, Pneumonia, Sepsis, CDH• No- Consider Congenital Heart Disease
• Does the infant’s color improve with oxygen administration?• Does the infant’s color improve with oxygen administration?• Not Cyanotic CHD
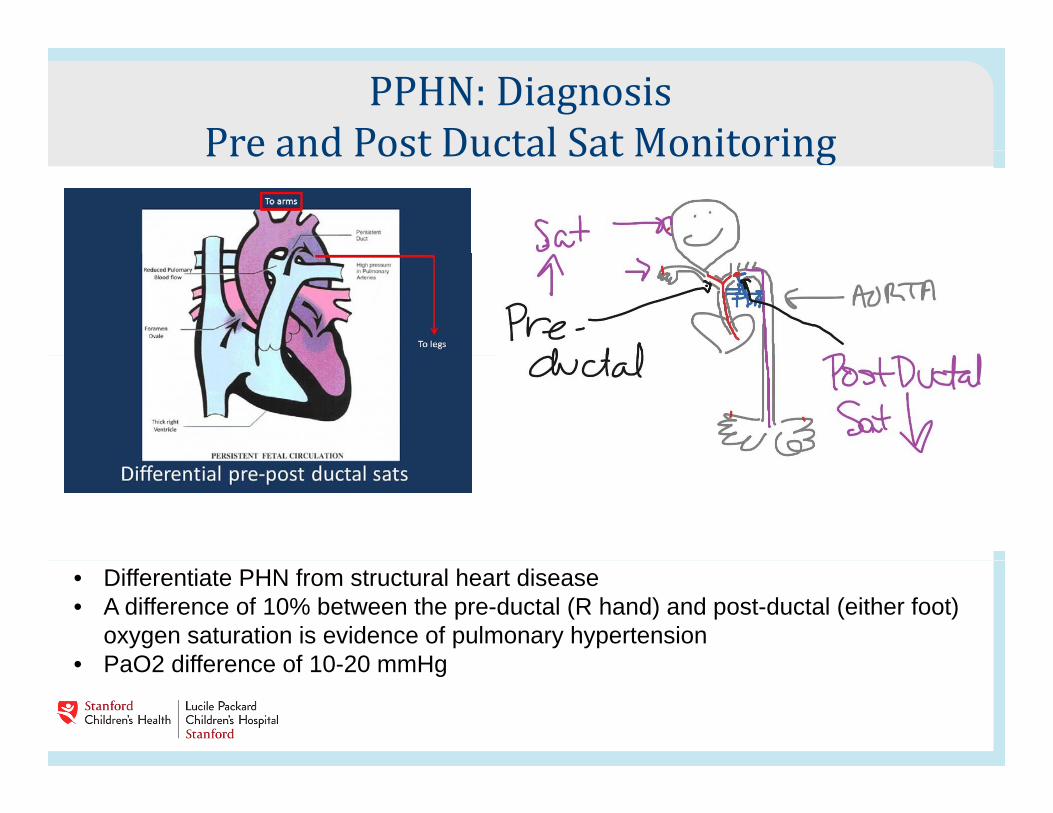
PPHN: DiagnosisPre and Post Ductal Sat MonitoringPre and Post Ductal Sat Monitoring
• Differentiate PHN from structural heart disease• A difference of 10% between the pre-ductal (R hand) and post-ductal (either foot)
oxygen saturation is evidence of pulmonary hypertension• PaO2 difference of 10 20 mmHg• PaO2 difference of 10-20 mmHg
PPHN: DiagnosisHyperoxia and Hyperventilation TestsHyperoxia and Hyperventilation Tests Differentiate between pulmonary and cardiac causes of
cyanosisy
Deliver 100% FiO2 (invasive or non-invasive method of administration) to decrease PVR
Hyperventilate and drive down pCO2 (relax pulm vessels)
Check SpO2 and/or Arterial Blood Gas 10 minutes postCheck SpO2 and/or Arterial Blood Gas 10 minutes post administration.
Positive response to test indicates PPHN, NOT CHD
HEART ECHO is preferred diagnostic tool due to known adverse effects of hyperoxia and hyperventilation
PPHN - Clinical findings Respiratory distress within the first 24 hours of life
Hypoxia tachypnea retractions and grunting with cyanosisHypoxia, tachypnea, retractions and grunting with cyanosis
Cardiac exam with harsh systolic murmur at LLSB (tricuspid regurgitation)regurgitation)
Labile Hypoxemia• Frequent desat episodes and wide swings in SpO2 and arterial PO2Frequent desat episodes and wide swings in SpO2 and arterial PO2
without changes in vent settings or FiO2 administration. • Caused by pulmonary vascular constriction and relaxation and
intermittent right-> left shuntintermittent right > left shunt
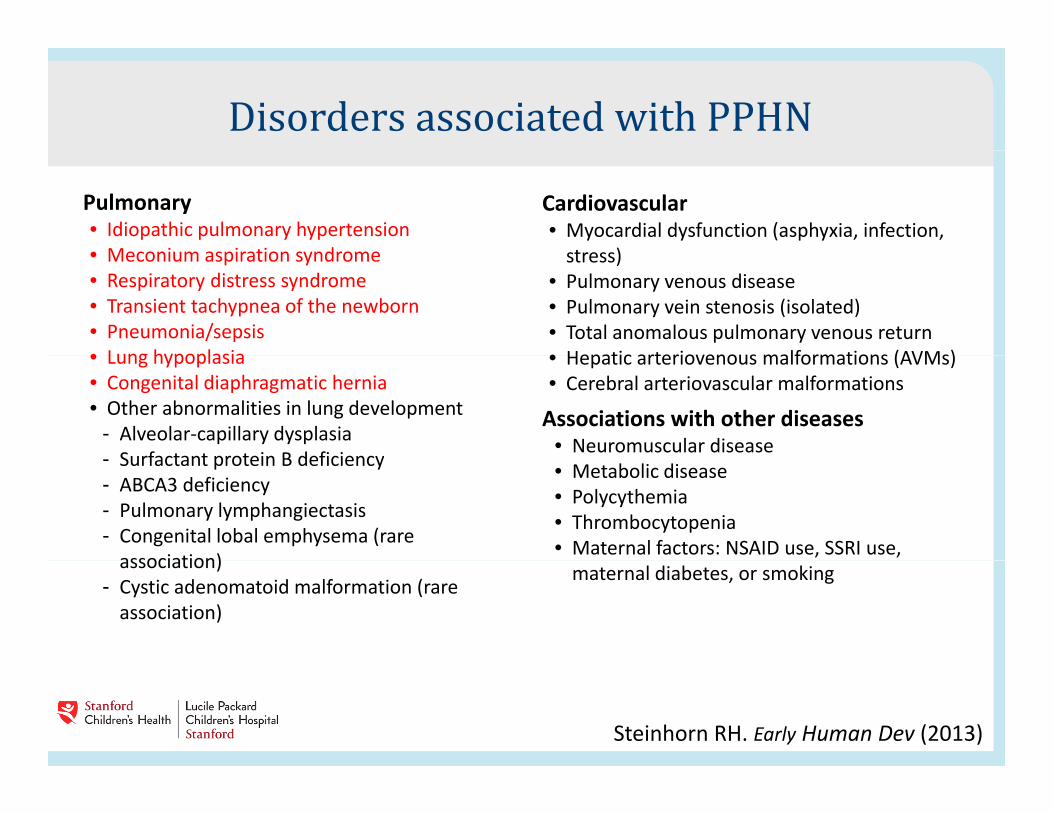
Disorders associated with PPHNPulmonary• Idiopathic pulmonary hypertension• Meconium aspiration syndrome
Cardiovascular• Myocardial dysfunction (asphyxia, infection,
stress)• Meconium aspiration syndrome• Respiratory distress syndrome• Transient tachypnea of the newborn• Pneumonia/sepsis• Lung hypoplasia
stress)• Pulmonary venous disease• Pulmonary vein stenosis (isolated)• Total anomalous pulmonary venous return• Hepatic arteriovenous malformations (AVMs)• Lung hypoplasia
• Congenital diaphragmatic hernia• Other abnormalities in lung development
- Alveolar-capillary dysplasiaSurfactant protein B deficiency
• Hepatic arteriovenous malformations (AVMs)• Cerebral arteriovascular malformations
Associations with other diseases• Neuromuscular disease- Surfactant protein B deficiency
- ABCA3 deficiency- Pulmonary lymphangiectasis- Congenital lobal emphysema (rare
association)
• Metabolic disease• Polycythemia• Thrombocytopenia• Maternal factors: NSAID use, SSRI use,
association)- Cystic adenomatoid malformation (rare
association)
maternal diabetes, or smoking
Steinhorn RH. Early Human Dev (2013)
Initial studies needed Pulse oximetry screening (pre and post-ductal)
Arterial blood gas
Chest radiograph• Parenchymal disease such as MAS, RDS• Idiopathic PPHN: “black lung”
Echocardiogram
CBC and blood/ET culture
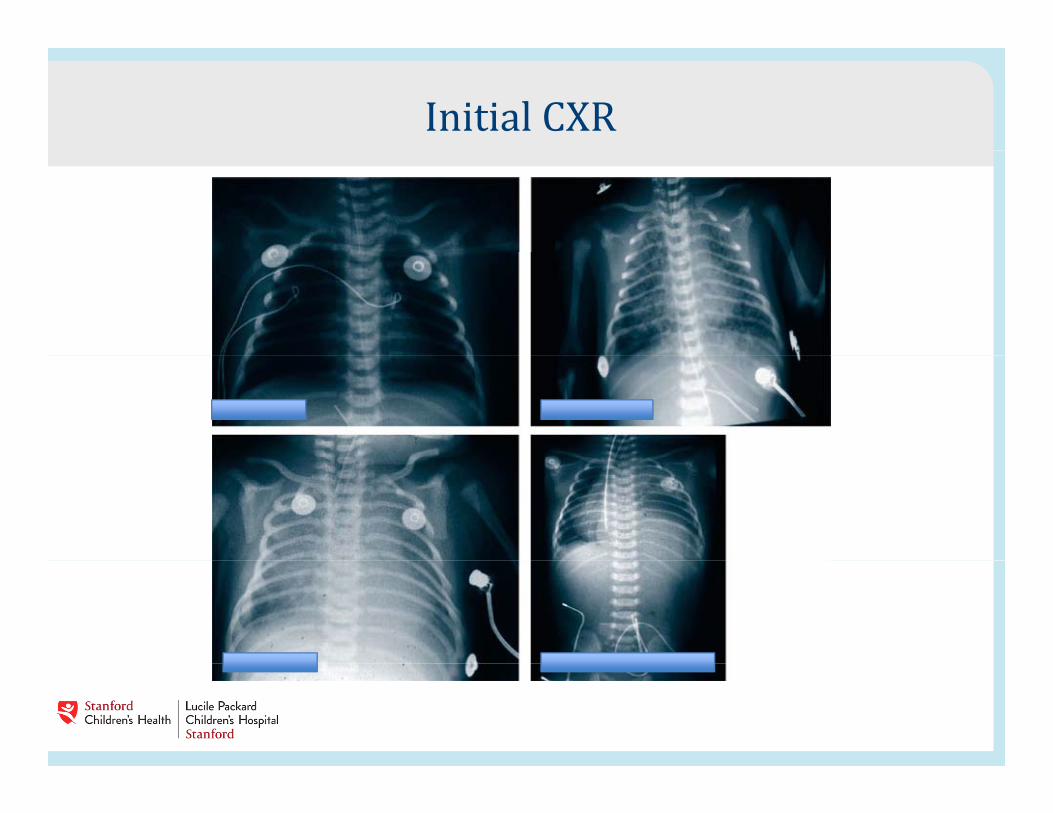
Initial CXR
Early management strategies Close monitoring of oxygenation, ventilation and pH (Consider
placing UAC for blood gases)p g g )• Hypoxia, hypercarbia and acidosis all cause and increase in
PVR
Maintenance of normal temperature and electrolytes• Cold stress causes increase in PVR• Hypocalcemia and hypomagnesemia can cause decrease in cardiacHypocalcemia and hypomagnesemia can cause decrease in cardiac
output and worsen R -> L shunt
Empiric antibiotics with blood culture are indicated (sepsis is f i d i h PPHN)often associated with PPHN)
Maintain adequate oxygen-carrying capacity
PPHN management strategies Intubation and mechanical ventilation for infants with
continued instability of oxygenationcontinued instability of oxygenationAchieve normal lung volumesAvoid adverse effects of high or low lung volumes on PVR
Gradual weaning of FiO2 is critical due to pulmonary vascular reactivity
Arterial blood gas and SpO2 targets If there is clinical or echo evidence of PPHN target
blood gases are:blood gases are:
pH >7.35
PaCO2 35-45
PaO2 > 60
SpO2 target: 90 97% SpO2 target: 90-97%
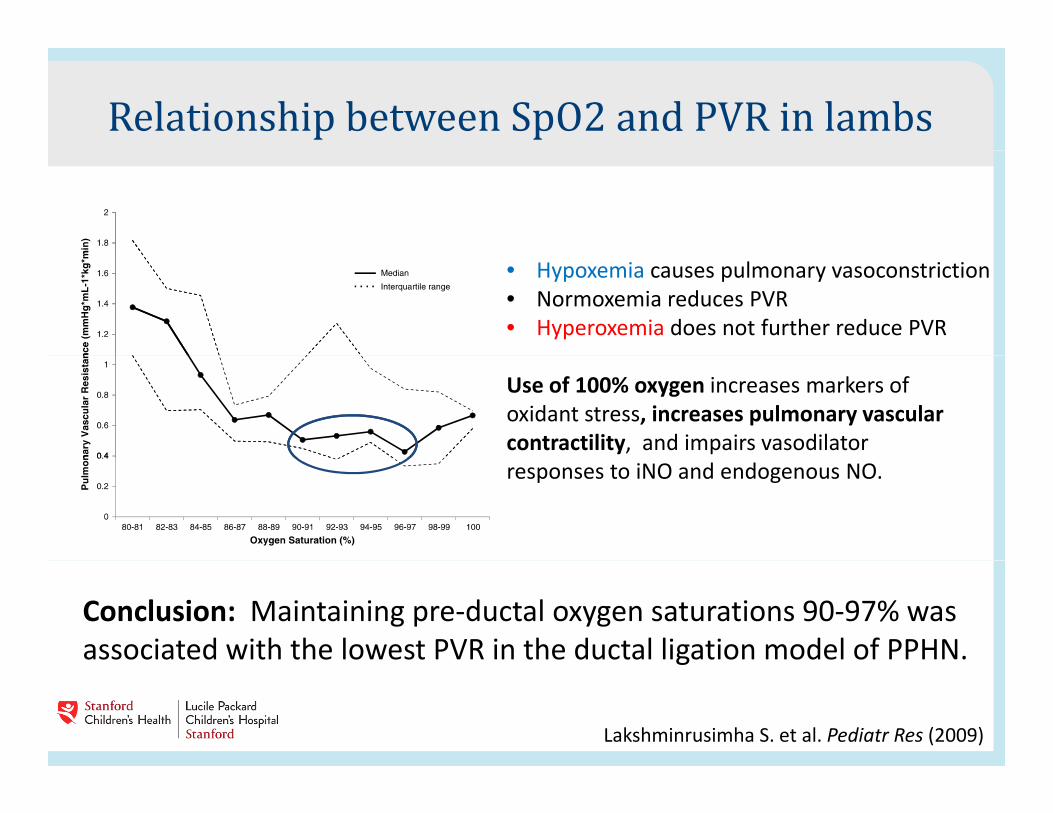
Relationship between SpO2 and PVR in lambs• Hypoxemia causes pulmonary vasoconstriction• Normoxemia reduces PVR• Hyperoxemia does not further reduce PVR
Use of 100% oxygen increases markers ofoxidant stress, increases pulmonary vascularcontractility, and impairs vasodilator responses to iNO and endogenous NO.
Conclusion: Maintaining pre-ductal oxygen saturations 90-97% was associated with the lowest PVR in the ductal ligation model of PPHN.
Lakshminrusimha S. et al. Pediatr Res (2009)
g
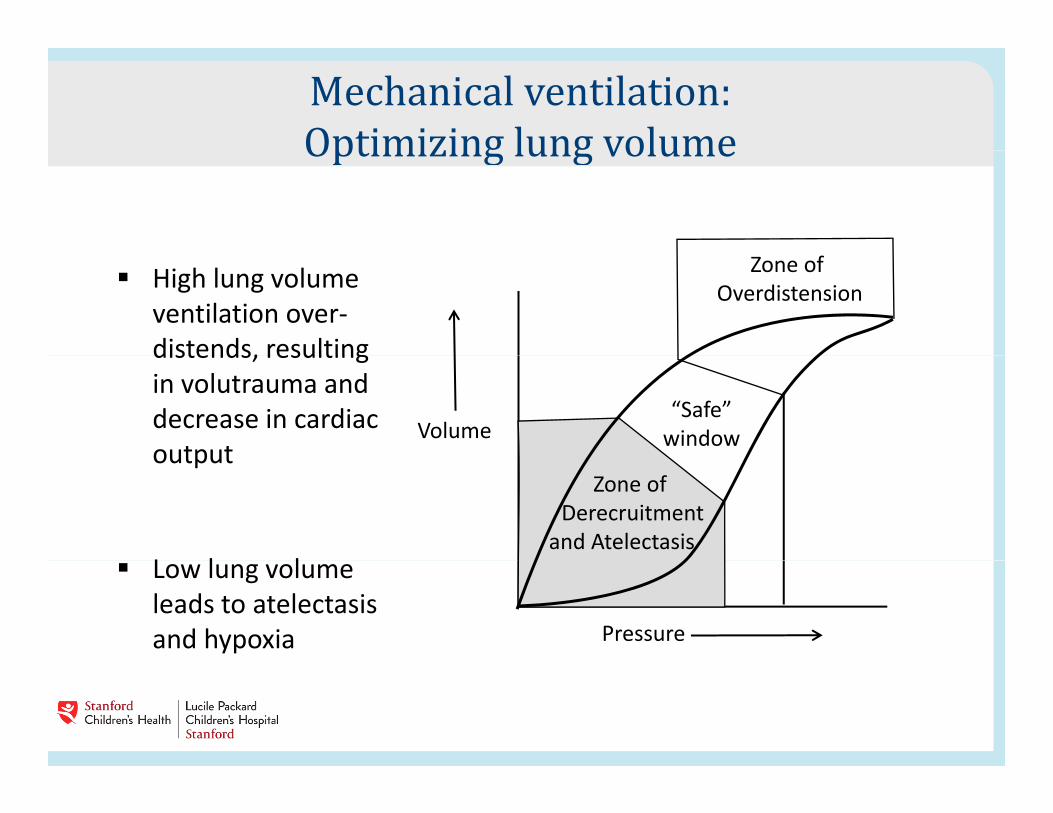
Mechanical ventilation:Optimizing lung volumeOptimizing lung volume High lung volume
ventilation over-distends, resulting
Zone of Overdistension
distends, resulting in volutrauma and decrease in cardiac output
“Safe”windowVolume
output
L l l
Zone ofDerecruitment
and Atelectasis Low lung volume
leads to atelectasis and hypoxia Pressure
PPHN management - Hemodynamics Optimize blood pressure to enhance cardiac output and
oxygen delivery (R to L shunt increases as cardiac output andoxygen delivery (R to L shunt increases as cardiac output and BP fall)
• Consider UVC for intravascular volume monitoring (CVP)
• Keep mean blood pressure at least 45-55 with systolic 60-70
• Vasopressor support is often needed with PPHN Dopamine is• Vasopressor support is often needed with PPHN. Dopamine is first line started at 5 mcg/kg/min and titrated up to 20 mcg/kg/min. Also epinephrine and hydrocortisone
Additional PPHN strategies Minimize handling and noise
Assure adequate sedation and analgesia. Use neuromuscular paralysis only if oxygenation is sub-optimal after other therapeutic strategies have been usedtherapeutic strategies have been used
Calculate Oxygenation Index (OI) for all infants with FiO2>60%
OI = MAP x FiO2 x 100 ÷ PaO2
Calculating the OIOI = MAP x FiO2 x 100 ÷ PaO2
MAP on Vent- for example, 15
FiO2 – 75% = 0.75
PaO2- for example, 45 on ABG
OI = 15 x 0 75 x 100 ÷ 45 = 25OI = 15 x 0.75 x 100 ÷ 45 = 25
When OI > 20 consider maximal medical therapies
Maximal medical therapy alternatives Surfactant therapy
High frequency oscillatory ventilation (HFOV)
Inhaled nitric oxide (iNO)
Extracorporeal membrane oxygenation (ECMO)
Others – Sildenafil Bosentan Others – Sildenafil, Bosentan
Surfactant use in term neonates with respiratory failurewith respiratory failure Hypoxic respiratory failure often is associated with secondary surfactant deficiency due to either the primary disease orsurfactant deficiency due to either the primary disease or ventilator or hyperoxia associated injury.
Give carefully; consider a “test dose” as some infants will becomeGive carefully; consider a test dose as some infants will become more unstable during administration
Lotze A, et al. J Pediatr (1998)

iNO for hypoxic respiratory failure: NINOS and CINRGI trial resultsNINOS and CINRGI trial resultsp = .014
p = .001
Need forECMOECMO
Conclusion: Inhaled nitric oxide significantly reduces the need for ECMO in term and near term infants with hypoxic respiratory failure
NINOS. Pediatrics (1997)Clark R et al. NEJM (2000)
term and near-term infants with hypoxic respiratory failure.
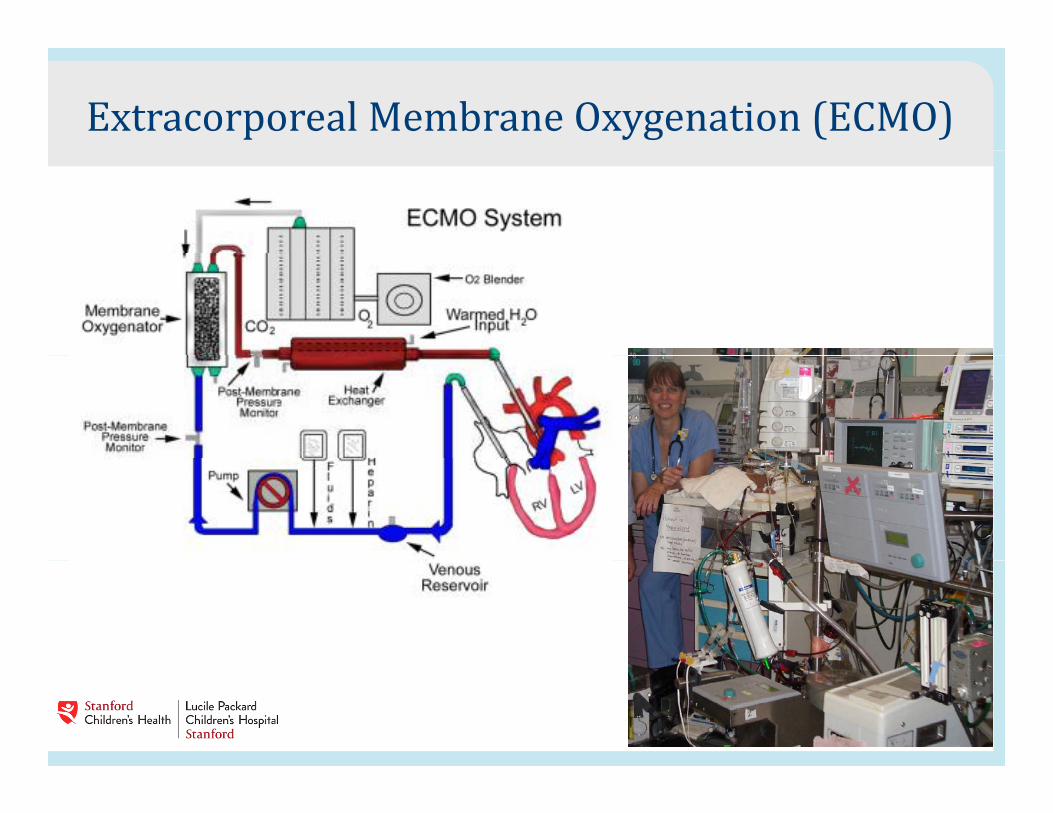
Extracorporeal Membrane Oxygenation (ECMO)
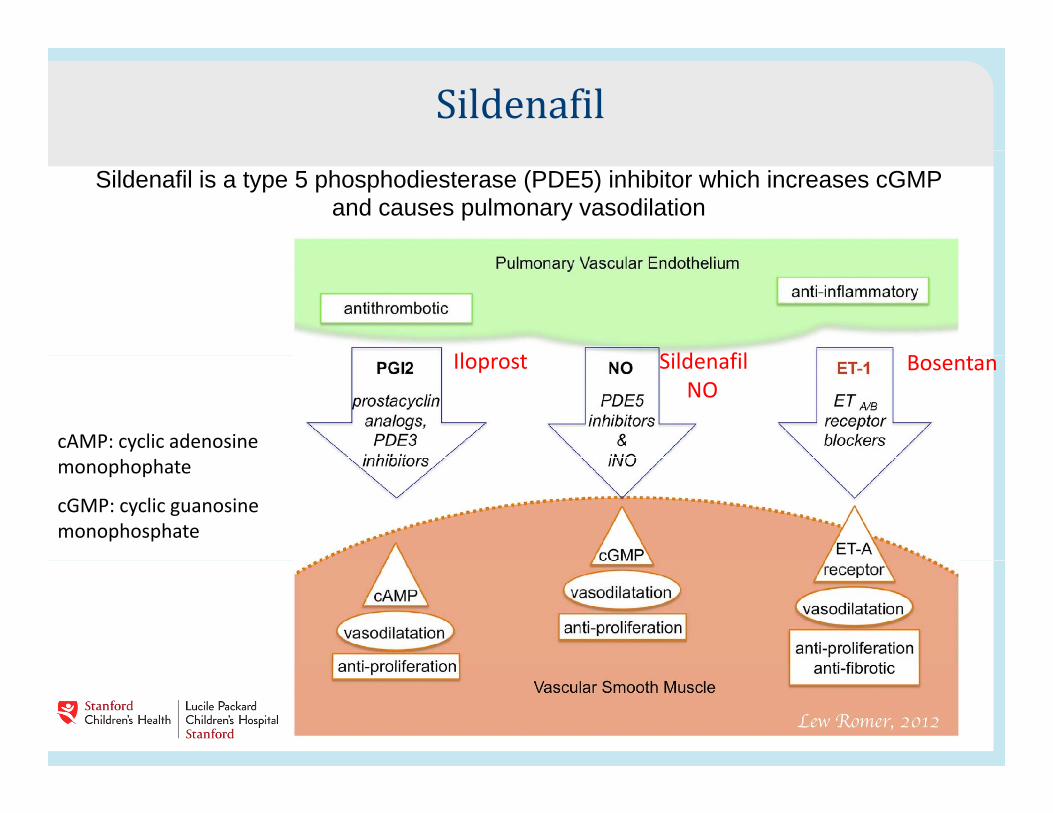
SildenafilSildenafil is a type 5 phosphodiesterase (PDE5) inhibitor which increases cGMP
and causes pulmonary vasodilation
Sild filIl t B
cAMP: cyclic adenosine
SildenafilNO
Iloprost Bosentan
monophophate
cGMP: cyclic guanosinemonophosphate
Cochrane Review1: PO Sildenafil for PPHN 77 patients from 3 efficacy trials in settings without iNO or
HFOVHFOV
Sildenafil given enterally at doses ranging 0.5 to 3 mg/kg/dose every 6 hoursevery 6 hours
Discontinued when OI < 10-20, or a predetermined number of doses had been giveng
Baquero H, et al. Pediatrics (2006)Herrera Torres R, et al. Revista Mexicana de Pediatria (2006)Vargas-Origel A, et al. Am J Perinatol (2010)g g , ( )Kelly LE, Shah PS, Ohlsson A. The Cochrane Collaboration (2017)
1Cochrane is an international and independent non-profit organization established in 1993 aimed at providing up-to-date, accurate information about the effects of healthcare available worldwide. Cochrane produces and disseminates systematic reviews of healthcare interventions and diagnostic tests, and promotes the search for evidence in the form of clinical trials and other interventional studies.
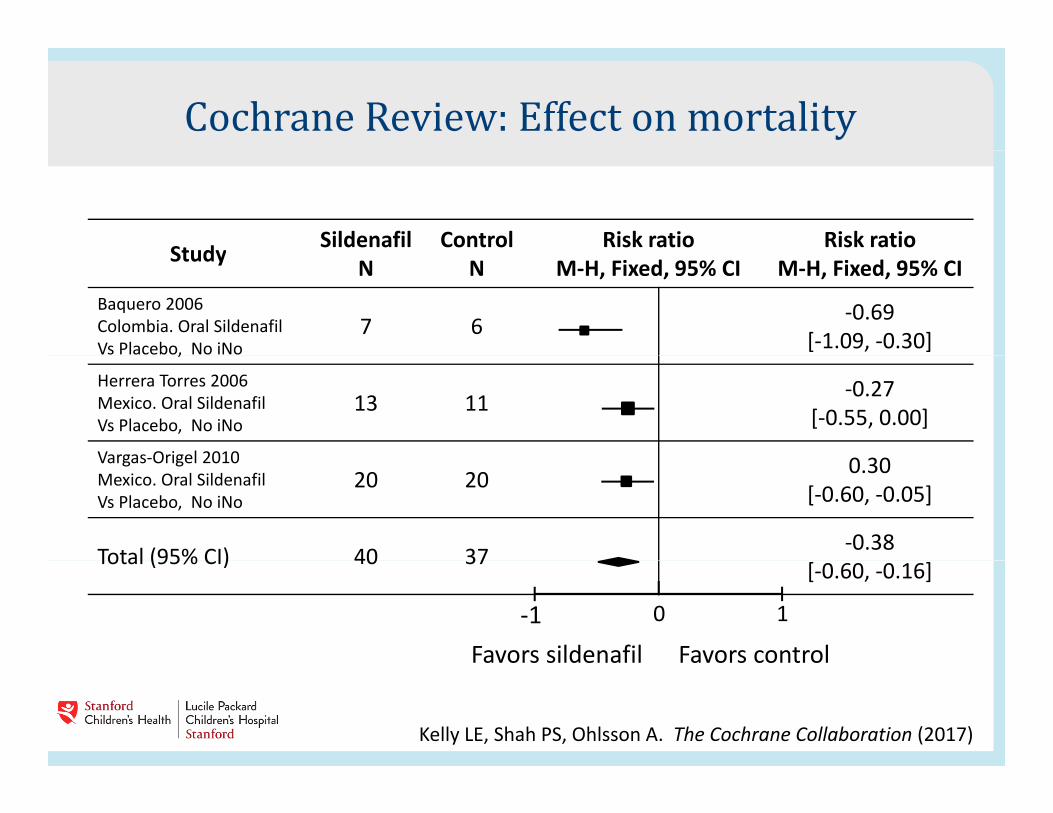
Cochrane Review: Effect on mortalityStudy Sildenafil Control Risk ratio Risk ratioStudy N N M-H, Fixed, 95% CI M-H, Fixed, 95% CI
Baquero 2006Colombia. Oral SildenafilVs Placebo, No iNo
7 6 -0.69[-1.09, -0.30],
Herrera Torres 2006Mexico. Oral SildenafilVs Placebo, No iNo
13 11 -0.27[-0.55, 0.00]
Vargas-Origel 2010 0 30Vargas-Origel 2010Mexico. Oral SildenafilVs Placebo, No iNo
20 20 0.30[-0.60, -0.05]
Total (95% CI) 40 37 -0.38Total (95% CI) 40 37 [-0.60, -0.16]
-1 0 1
Favors sildenafil Favors control
Kelly LE, Shah PS, Ohlsson A. The Cochrane Collaboration (2017)
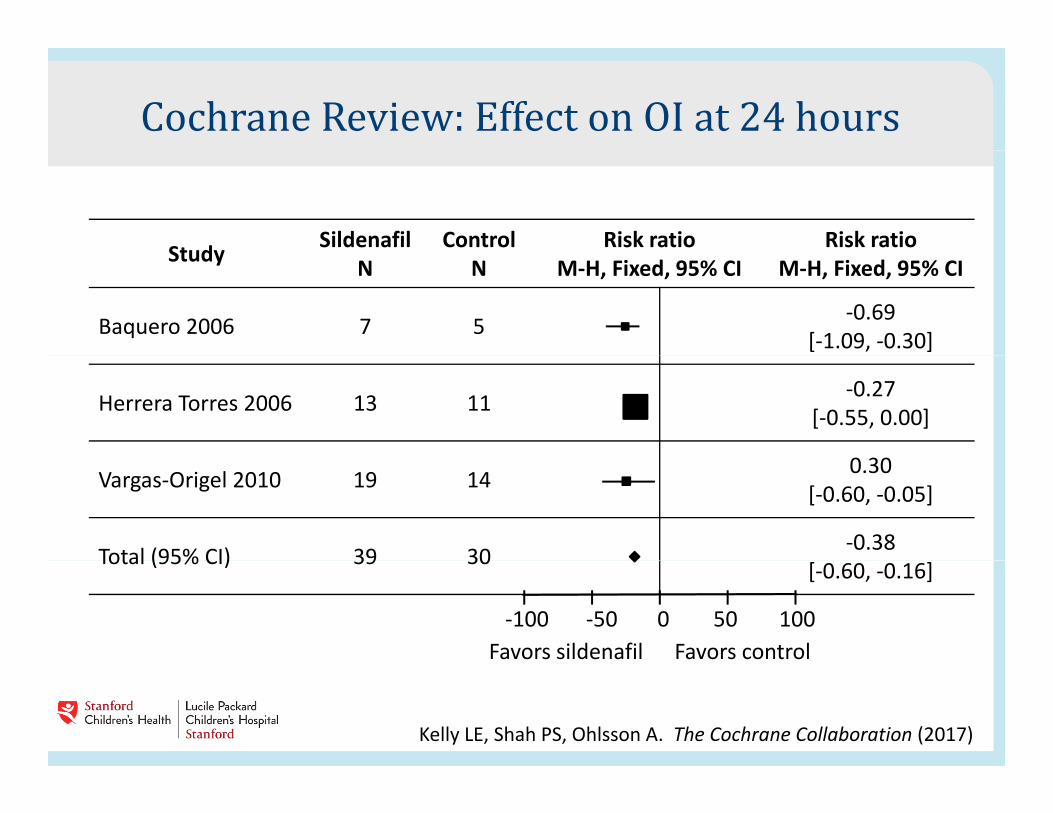
Cochrane Review: Effect on OI at 24 hoursStudy Sildenafil Control Risk ratio Risk ratioStudy N N M-H, Fixed, 95% CI M-H, Fixed, 95% CI
Baquero 2006 7 5 -0.69[-1.09, -0.30]
Herrera Torres 2006 13 11 -0.27[-0.55, 0.00]
0 30Vargas-Origel 2010 19 14 0.30[-0.60, -0.05]
Total (95% CI) 39 30 -0.38Total (95% CI) 39 30 [-0.60, -0.16]
Favors sildenafil Favors control-100 0 10050-50
Kelly LE, Shah PS, Ohlsson A. The Cochrane Collaboration (2017)
Cochrane Review: PO Sildenafil for PPHN Conclusion: When comparing Sildenafil to placebo, significant reduction in mortality in Sildenafil group was seen as well asreduction in mortality in Sildenafil group was seen as well as improvement in oxygenation. No clinically important side effects.
• The quality of evidence for reducing mortality or improving respiratory parameters was low owing to the small number of included studies and the small number of babies evaluated. Some of the included studies have methodological issues resulting in low to very low quality ofstudies have methodological issues, resulting in low to very low quality of evidence.
• Cochrane grades of evidenceHigh quality: We are very confident that the true effect lies close to that of the estimate of the effectModerate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially differentLow quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effectV l lit W h littl fid i th ff t ti t Th t ff t i lik l t b b t ti ll diff tVery low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect
PO Sildenafil Protocol1,2 Initial dosing: 0.5-1.0 mg/kg PO q 6 hrs
• Preparation: Dissolve a crushed and powdered 50 mg tablet of Sildenafil in Orobase, making a concentration of 2 mg/ml (if refrigerated, this is safe for 1 month after preparation)
R i 20 i 3 h Response time: 20 minutes to 3 hours
May double dose (max 2 mg/kg/dose) if oxygenation does not improve and blood pressure remains stable
Discontinue after 6-8 doses if no significant improvement
1 Mohsen, AHA. Salah, Amr. Risk Factors and Outcomes of Persistent Pulmonary Hypertension of the Newborn in Neonatal Intensive Care Unit of Al-Minya University Hospital in Egypt. Journal of Clinical Neonatology. 2013 apr-Jun; 2(2): 78-82.
2 Yaseen, H. Is Sildenafil an Effective Therapy in the Management of PPHN? Journal of clinical Neonatology. 2012 Oct-Dec. 1(4):171-175
RCT of Bosentan for PPHNSafety and Efficacy TrialSafety and Efficacy Trial Bosentan is an oral dual endothelin-1 receptor
antagonistantagonist • Endothelin-1 is a potent vasoconstrictor• High concentration of endothelin-1 in plasma of neonatesHigh concentration of endothelin 1 in plasma of neonates
with PPHN
Study Methods: (Saudi Arabia) Study Methods: (Saudi Arabia) • 47 neonates ≥34 weeks and <7 days with FiO2>0.50 and PH
by echo (R to L shunt and Pap ≥40). • Bosentan dose 1 mg/kg PO BID
Mohamed WA, et al. J Perinatol (2012)
RCT of Bosentan for PPHNResultsResults All infants who received bosentan showed significant
improvement in oxygenation at 6 h after initiation ofimprovement in oxygenation at 6 h after initiation of treatment.
Duration of mechanical ventilation was significantly decreasedDuration of mechanical ventilation was significantly decreased compared with placebo group.
No adverse events potentially secondary to bosentan p y ytreatment.
None of infants in the bosentan-treated group had neurologic g p gsequelae.
Of 24 bosentan-treated neonates, only 1 infant died., y
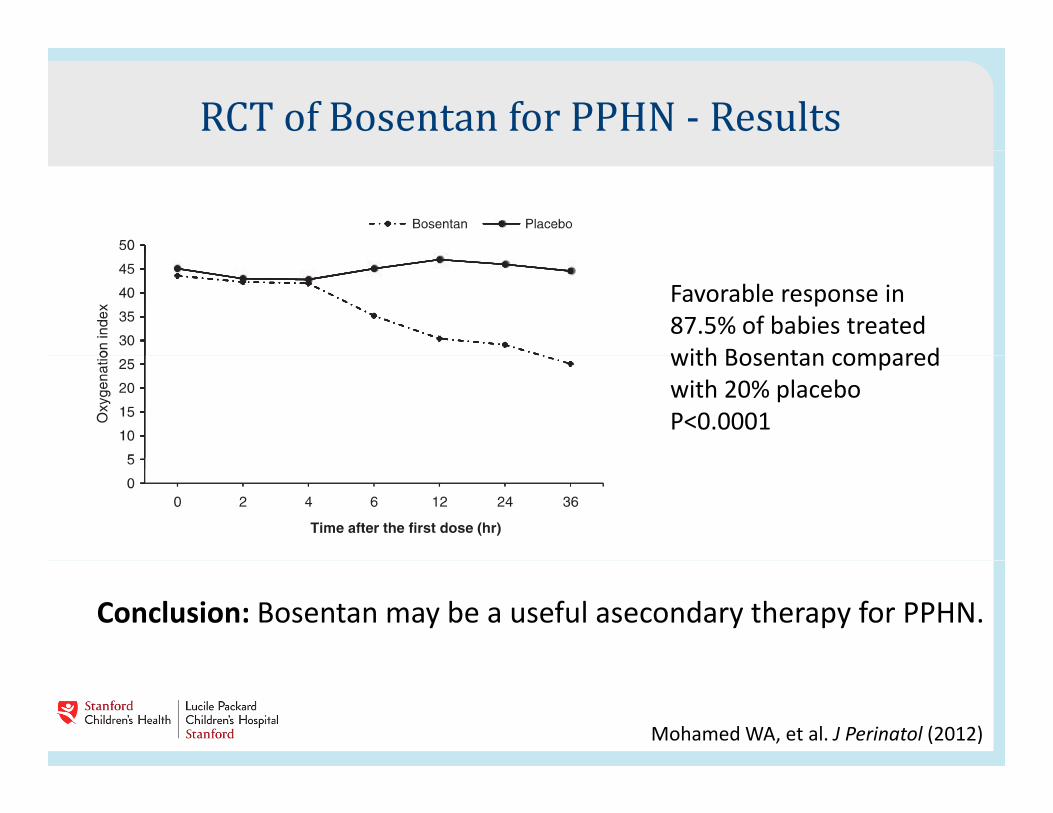
RCT of Bosentan for PPHN - ResultsFavorable response in87.5% of babies treatedwith Bosentan comparedwith Bosentan comparedwith 20% placebo P<0.0001
Conclusion: Bosentan may be a useful asecondary therapy for PPHN.
Mohamed WA, et al. J Perinatol (2012)
Bosentan In contrast, a small trial of 21 infants with PPHN reported no
improvement in oxygenation or other outcomes in the group treated with enteral bosentan compared with those who received placebowith enteral bosentan compared with those who received placebo [57]. This trial was terminated early because of slow recruitment
Conflicting outcomes in 2 reported trials of Bosentan for PPHN. Need bigger trials to determine efficacy
Steinhorn RH et al. Bosentan as Adjunctive Therapy for PPHN of the Newborn: Results of the Randomized Multicenter Pacebo=Controlled Exploratory Trial. J Pediatr 2016; 177:90
Conclusions PPHN should be suspected in the term or near term newborn who presents
with cyanosis and hypoxia not responsive to oxygen administration
The differential diagnosis includes congenital heart disease and sepsis
Gold standard for diagnosis is by cardiac ECHO
In absence of ECHO, diagnosis by pulse oximetry showing a pre/post ductal difference of > 10%
M t di t d t i th i ht t l ft l t t i Management directed at reversing the right to left pulmonary to systemic shunt by vasodilating the pulmonary vasculature (oxygen, sildenafil), supporting BP (volume, dopamine), and preventing pulmonary vasoreactivity (avoidance of hypercarbia and acidosis sedation slowvasoreactivity (avoidance of hypercarbia and acidosis, sedation, slow weaning).
Conclusions Oxygenation Index (OI)is used to assess severity of PPHN and to determine
whether more advanced therapies should be used• Surfactant therapy is beneficial for babies with PPHN due to MAS, RDS
or sepsis but not for idiopathic PPHN. It is best used when the OI is 15-22.
• Inhaled nitric oxide significantly reduces the need for ECMO. • Oral Sildenafil has been reported in small studies to be safe and useful
in the treatment of PPHN in newbornsin the treatment of PPHN in newborns• Insufficient data on efficacy of Bosentan
Recommended