-
7/31/2019 Marsh - Global Challenge
1/67
David Marsh
Emeritus Professor of Clinical Orthopaedics, University College
London
Royal National Orthopaedic Hospital, Stanmore
International Ambassador for the Bone and Joint DecadePresident
of the Fragility Fracture Network
The Global Challengeof Fragility Fractures
ECOOG 2012
of the Bone and Joint Decade
-
7/31/2019 Marsh - Global Challenge
2/67
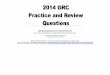
Adapted from Cooper C et al,Osteoporosis Int, 1992; 2:285-9
Total number ofhip fractures:1990 = 1.66 million2050 = 6.26
million
1990 2050
600
3250
1990 2050
6
68
400
1990 2050
1990 2050
100
6293
78
742
Projected Osteoporotic
Hip Fractures Worldwide
-
7/31/2019 Marsh - Global Challenge
3/67
The number of hip fracturesdepends on two things
Age-specific incidence Secular change
Age structure of the population
Demographic change
-
7/31/2019 Marsh - Global Challenge
4/67
General increase in age-adjusted incidence in
the last century
Mixed picture since then
Some plateau, some fall, some continue to rise
-
7/31/2019 Marsh - Global Challenge
5/67
Rochester MN
-
7/31/2019 Marsh - Global Challenge
6/67
Japan
-
7/31/2019 Marsh - Global Challenge
7/67
-
7/31/2019 Marsh - Global Challenge
8/67
Assuming 0.43%annual secular fall
-
7/31/2019 Marsh - Global Challenge
9/67
Summary of the challenge
Despite falling age-adjusted incidence, ageing
will lead to massive increase over next 25 years
In Europe:
Double the number of cases
Treble the cost
In Asia and Latin America 6-fold increase
Unless we do something about it
-
7/31/2019 Marsh - Global Challenge
10/67
TheFragility Fracture Network
of the Bone and Joint Decade
Mission: To promote globally the optimal
multidisciplinary management of the patient with
a fragility fracture, including secondary prevention
-
7/31/2019 Marsh - Global Challenge
11/67
Aims
to disseminate globally the best multidisciplinary
practice in preventing and managing fragility
fractures to promote research aimed at better treatments for
osteoporosis, sarcopenia and fracture
to drivepolicy change that will raise fragility
fractures higher up the healthcare agenda in all
countries
-
7/31/2019 Marsh - Global Challenge
12/67
Membership
Open to professionals in any field relevant to
fragility fractures, eg:
Orthopaedic surgeons
Geriatricians
Osteoporosis doctors
Nurses and allied health professionals Industry
-
7/31/2019 Marsh - Global Challenge
13/67
Outline
The nature of fragility fractures
The opportunity for secondary prevention
Integrated care of the acute episode
Changing policy, changing behaviour
-
7/31/2019 Marsh - Global Challenge
14/67
The nature of fragility fractures
A chronic disease
Modifiable risk factors
The potential for prevention
Challenges of treatment
The need for multidisciplinary care
-
7/31/2019 Marsh - Global Challenge
15/67
50 60 70 80 90 Age
No fractures increasing morbiditydue to ageing alone
Age Adapted from Kanis JA, Johnell O; 1999
The fragility fracture career
- a chronic diseaseMorbidityDependence
-
7/31/2019 Marsh - Global Challenge
16/67
The fragility fracture career
- a chronic diseaseMorbidityDependence
50 60 70 80 90
Colles' fracture
Vertebral fracture
Hip fracture
Age
No fractures increasing morbiditydue to ageing alone
Added morbidity fromfractures
Age Adapted from Kanis JA, Johnell O; 1999
-
7/31/2019 Marsh - Global Challenge
17/67
Why Hip Fractures are the key
Hip fractures 87% of
total cost of all fragility
fractures
(2.0 billion in UK)
1.2 million bed days per
year in UK
Often considerably
increased dependency
-
7/31/2019 Marsh - Global Challenge
18/67
Comparison with other priorities
Issues: Strokes Heart Fragility
& TIAs attacks fractures
-----------------------------------------------------------------------------------------
Incidence/year 110,000 275,000 310,000
Current trend Falling Falling Rising
NHS bed days* 1.85m 1.15m 1.2m(hips)
Annual costs 2.8bn 1.7bn 2bn
UK figures from the Department of Health
-
7/31/2019 Marsh - Global Challenge
19/67
Risk of fragility fracture
Bone Density
Bone Turnover
Bone Architecture
Skeletal Geometry
Mineralisation
Postural Instability
Slow Responses
Frailty
Environment
Lack of Padding
BoneStrength
Falls
Risk
Osteoporosistreatment
Strength andbalance training
-
7/31/2019 Marsh - Global Challenge
20/67
Sarcopenia
Traditionally defined as the loss of muscle mass with age
Extended to include loss of strength or performance
-
7/31/2019 Marsh - Global Challenge
21/67
-
7/31/2019 Marsh - Global Challenge
22/67
FRAILTY
SARCOPENIA
-
7/31/2019 Marsh - Global Challenge
23/67
FRAGILITY
SARCOPENIA
OSTEOPOROSIS
-
7/31/2019 Marsh - Global Challenge
24/67
Sarcopenia, frailty, rehabilitation
Falls really are as important as osteoporosis Rehabilitation
after fracture is inadequate
Drug companies are more excited about anti-
sarcopenic drugs than anti-osteoporotic Except bone
anabolics
Muscle-building effects of exercise work in
the elderly
-
7/31/2019 Marsh - Global Challenge
25/67
Earlier fractures signal the hip fractureMorbidity
Dependence
50 60 70 80 90
Colles' fracture
Vertebral fracture
Hip fracture
Age
No fractures increasing morbiditydue to ageing alone
Added morbidity fromfractures
Age Adapted from Kanis JA, Johnell O; 1999
-
7/31/2019 Marsh - Global Challenge
26/67
Secondary prevention
Secondary prevention is more cost-effectivethan primary
prevention
-
7/31/2019 Marsh - Global Challenge
27/67
Prevalence of prior fractures among patientspresenting with hip
fracture
45.3 44.6 45.4
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
80.0
90.0
100.0
Lyles et al Edwards et al Mclellan et al
Percentage
Lyles KW et al. The Horizon Recurrent Clinical Fracture after
Recent Hip Fracture Trial (RFT) Study Cohort Description. ASBMR
2006
Edwards, B. J. et al (2007) Prior Fractures Are Common in
Patients With Subsequent Hip Fractures. Clinical Orthopaedics &
RelatedResearch, 461, 226-230
McLellan Alastair R. et al.(2004) Effectiveness of Strategies
for the Secondary Prevention of Osteoporotic Fractures in Scotland
(CEPS99/03). NHS Quality Improvement Scotland.
n=2124 n=632 n=701
-
7/31/2019 Marsh - Global Challenge
28/67
Post-menopausalwomen 11.1 million
0.2 million
Post-menopausal
women with newfracture each year
3.4 million
Post-menopausalwomen with
osteoporosis
1.8 million
Post-menopausalwomen with prior
fracture history
50% of hip
fractures from
16% of the
population
50% of hip
fractures from
84% of the
population
16% of women over 50 have had at
least one low trauma fracture
UK figures
-
7/31/2019 Marsh - Global Challenge
29/67
National Clinical Audit of Falls and Bone Health (2007) Clinical
Effectiveness and Evaluation Unit, RCP, London
0
10
20
30
40
50
60
Osteoporosisassessment
DXA referral (65-74 years)
Supplementationwith calcium + D3
Treatment withosteoporosismedication
Percentage
hip (n = 3184)
non-hip (n = 5642)
Target 100% 100% 100% ~70%
Interventions after low trauma fracture
-
7/31/2019 Marsh - Global Challenge
30/67
Secondary prevention
Secondary prevention is more effectivethan primary
prevention
A systems approach is needed, wherecapture of patients is
automatic
-
7/31/2019 Marsh - Global Challenge
31/67
Capturing patients reliably
Employment of a dedicated coordinator in the
fracture service is the most effective system
-
7/31/2019 Marsh - Global Challenge
32/67
NEW FRACTURE
EDUCATION
PROGRAMME
EXERCISE
CLASSES
FALLS RISK
ASSESSMENT
INPATIENT
ORTHO/TRAUMA WARD
OUTPATIENT
FRACTURE CLINIC
PRESCRIPTION ISSUED BY GP
Rx FOR FRACTURE
2Y PREVENTION
McLellan et al OI 2003, 14:1028-1034.
-
7/31/2019 Marsh - Global Challenge
33/67
Secondary prevention
Secondary prevention is more effectivethan primary
prevention
A systems approach is needed, wherecapture of patients is
automatic
When it is done vigorously,it is cost-saving
-
7/31/2019 Marsh - Global Challenge
34/67
Cost-saving
Per 1000 fragility fracture patients, 18 fractures (11
hip) prevented net saving 21,000
-
7/31/2019 Marsh - Global Challenge
35/67
38% reduction in expected hip fracture incidence
-
7/31/2019 Marsh - Global Challenge
36/67
Secondary prevention
If universally applied, coordinator-based systems in
fracture units could
Prevent ~25% of the burden of disease from hip fractures
Save money
-
7/31/2019 Marsh - Global Challenge
37/67
Treatment of the acute episode
A multidisciplinary approach is needed
Senior input from physicians
Good surgery
Coordinated rehabilitation and discharge
Treating fragility fractures well ischeaper than treating them
badly
-
7/31/2019 Marsh - Global Challenge
38/67
days from injury to death
300200
1000
140
120
100
80
60
40
20
0
Royal VictoriaHospital, Belfast
1999-2003
1003 deaths byone year in 5553
patients
Mortality after hip fracture
-
7/31/2019 Marsh - Global Challenge
39/67
Complexity of elderly patients
Mean age hip fracture = 80 yrs
Comorbidities
(median ASA 3) Cardiac murmurs
Renal - Dialysis
COPD - home O2
Diabetes
Delirium / dementia
Pseudo-obstruction
Alcohol abuse
Impaired metabolic response to
injury
Hyponatraemia Management problems
Consent
Theatre scheduling
Discharge planning
Polypharmacy Warfarin
Plavix
Neurotropics
-
7/31/2019 Marsh - Global Challenge
40/67
Acute medical management
Difficult judgement balance between medicaloptimisation and
prompt surgery
Inexperienced surgical trainees not the bestpeople to look after
such people and preparethem for surgery
Ideal solution is close supervision by seniorphysicians having
expertise with elderly patients
pre- and peri-operatively, not just for rehabilitation
-
7/31/2019 Marsh - Global Challenge
41/67
Senior medical backup
Can come from different specialists,
depending on health care system Anaesthesia
Internal medicine
Geriatrics
Orthogeriatricsa key role in UK, Spain andseveral other
countries
-
7/31/2019 Marsh - Global Challenge
42/67
-
7/31/2019 Marsh - Global Challenge
43/67
Compared four types of model
Integrated care on an orthopaedic ward gave the best Mortality
rate
Length of stay
Time to surgery
-
7/31/2019 Marsh - Global Challenge
44/67
J Am Geriatric Soc 2008
Geriatric Fracture Center in Rochester, USA
Comparison with other fracture services in locality
In-hospital mortality 1.5% vs 3.2%
Readmission 9.7% vs 19.4%
Length of stay 4.6 vs 5.2 days
-
7/31/2019 Marsh - Global Challenge
45/67
Orthogeriatric co-management of the
acute episode
Gives the patient a better quality of carewith better
outcomes
Saves money by enabling
more efficient use of resources
fewer readmissions
-
7/31/2019 Marsh - Global Challenge
46/67
Four big messages
Multidisciplinary approach to themanagement of fragility
fracturepatients
Reliable secondary preventionosteoporosisfalls
Chronic disease model
Quality assurance
the NHFD
-
7/31/2019 Marsh - Global Challenge
47/67
BOA-BGS Blue Book
six standards for hip fracture care
1. All patients with hip fracture should be admitted to an
acuteorthopaedic ward within 4 hours of presentation
2. All patients with hip fracture who are medically fit should
havesurgery within 48 hours of admission, during normal working
hours
3. All patients with hip fracture should be assessed and cared
for with aview to minimising their risk of developing a pressure
ulcer4. All patients presenting with a fragility fracture should be
managed on an
orthopaedic ward with routine access to orthogeriatric medical
supportfrom the time of admission
5. All patients presenting with fragility fracture should be
assessed to
determine their need for bone-protective therapy to prevent
futureosteoporotic fractures6. All patients presenting with a
fragility fracture following a fall
should be offered multidisciplinary assessment and
interventionto prevent future falls
-
7/31/2019 Marsh - Global Challenge
48/67
UK National Hip Fracture Database
(NHFD) Project- jointly led by BOA and BGS
Measures compliance with Blue Book standards
A web-based national database, now including
every fracture unit in England, Wales and N. Ireland
Feed back to units their performance compared to national
A professional steering group to manage analysis of,
and access to the data
Extensile for research
Adopted by government as a national clinical audit
-
7/31/2019 Marsh - Global Challenge
49/67
Smart commissioning
Alliance between multidisciplinary providersand healthcare
commissioners can tacklefragility fractures and drive change
Prioritisation
Incentivisation
-
7/31/2019 Marsh - Global Challenge
50/67
Objective 1: Improve outcomes andimprove efficiency of care
after hip
fractures by following the 6 Blue
Book standards
Hipfracturepatients
Objective 2: Respond to the first
fracture, prevent the second throughFracture Liaison Services
inacute and primary care
Non-hip fragilityfracture patients
Objective 3: Early intervention to restore
independence through falls carepathway linking acute and
urgentcare services to secondary fallsprevention
Individuals at highrisk of 1st fragility
fracture or otherinjurious falls
Objective 4: Prevent frailty, preservebone health, reduce
accidents
through preserving physicalactivity, healthy lifestyles
andreducing environmental hazards
Older people
UK DoH package for older people
Top priority
-
7/31/2019 Marsh - Global Challenge
51/67
Best Practice Tariff (BPT)
From April 2010
Reimbursement to Hospitals for each case of hip
fracture will vary according to the quality of care
Two criteria will be used
Time to theatre less than 36 hours
Involvement of orthogeriatrics in the acute phase Compliance for
each case will be determined from
the record in the National Hip Fracture Database
-
7/31/2019 Marsh - Global Challenge
52/67
Now the hospital CEO gives a damn
Nationalaverage
cost
before April
2010
~500 BPTsupplement
PAYMENTPER CASE
-
7/31/2019 Marsh - Global Challenge
53/67
UK National Hip Fracture Database
Annual Report 2010-2011
Eligible
hospitals
Hospitals
achievingBPT
Number of
pts submitted
Number of pts
achieving BPT
Qtr 1 162 92 (57%) 9455 2303 (24%)
Qtr 2 165 105 (64%) 11839 3328 (28%)
Qtr 3 163 111 (68%) 13136 4502 (34%)
Qtr 4 167 118 (71%) 12680 4671 (37%)
-
7/31/2019 Marsh - Global Challenge
54/67
Incentivisation
Next year the BPT differential will double to 900
But the base tariff will be reduced
More carrot but also more stick
Extra drive to introduce modern multidisciplinary
services will benefit our patients
-
7/31/2019 Marsh - Global Challenge
55/67
Adapted from Cooper C et al,
Osteoporosis Int, 1992; 2:285-9
Total number ofhip fractures:1990 = 1.66 million2050 = 6.26
million
1990 2050
6
00
3250
1990 2050
668
400
1990 2050
1990 2050
100
6293
78
742
Projected Hip Fractures Worldwide
-
7/31/2019 Marsh - Global Challenge
56/67
Launch meeting
Berlin, 8-9 Sep 2011
Discipline No
Orthopaedic surgeons 54Geriatricians 20
Osteoporosis doctors 6
Nurses 3
Scientists 6
Industry partners 12
Total 101
-
7/31/2019 Marsh - Global Challenge
57/67
Countries represented
Australia 3 Japan 4Austria 1 Lebanon 1
Belgium 1 Netherlands 3
Brazil 2 New Zealand 1
Canada 1 Norway 3China 2 Philippines 1
Denmark 1 Slovenia 1
Finland 1 Spain 6
France 2 Sweden 3Germany 16 Switzerland 5
Hong Kong 3 Thailand 1
Ireland 1 Turkey 1
Italy 23 UK 9
USA 6
-
7/31/2019 Marsh - Global Challenge
58/67
Global Regions
Europe 75
N America 7
S America 2Middle East 2
Asia-Pacific 15
Middle East Forum of the Bone and Joint Decade
Ghassan Maalouf FFN Board memberVice-chair of the Scientific
Committee
Coordinator for the Middle East North Africa region
-
7/31/2019 Marsh - Global Challenge
59/67
Aims
to disseminate globally the best multidisciplinary
practice in preventing and managing fragility
fractures to promote research aimed at better treatments
for osteoporosis, sarcopenia and fracture
to drivepolicy change that will raise fragilityfractures higher
up the healthcare agenda in all
countries
-
7/31/2019 Marsh - Global Challenge
60/67
Global dissemination
of best practice
Obviously, conditions differ between countries
But there is much in common and all countriescan learn from each
other
There is no time to rediscover the wheel a
hundred times This is the philosophy of the Bone and Joint
Decade
-
7/31/2019 Marsh - Global Challenge
61/67
Two main issues
Multidisciplinary care of the
acute fracture episode Particularly hip fractures
Secondary prevention - reduce risk of
another fracture in a patient who has
already had one, by addressing
Osteoporosis
Falls risk
-
7/31/2019 Marsh - Global Challenge
62/67
First Global
Congress
6-8 Sep 2012
Berlin Please come and
share your
experience
-
7/31/2019 Marsh - Global Challenge
63/67
The first FFN Global Congress
Berlin 6-8 Sep 2012
International speakers giving state of the art
on all relevant aspects
Workshops on practical ways forward
Submitted abstracts on research and audit of
different service models
-
7/31/2019 Marsh - Global Challenge
64/67
To register for the Global Congressand submit abstracts online,
please
go to
www.ffn-congress.com
http://www.ffn-congress.com/http://www.ffn-congress.com/http://www.ffn-congress.com/http://www.ffn-congress.com/
-
7/31/2019 Marsh - Global Challenge
65/67
If you want to get involved:
Go to www.ff-network.org
Download newsletter
Link to congress
Join FFN (50)
Contact me at [email protected]
or Ghassan Maalouf at
[email protected]
http://www.ff-network.org/mailto:[email protected]:[email protected]:[email protected]:[email protected]://www.ff-network.org/http://www.ff-network.org/http://www.ff-network.org/
-
7/31/2019 Marsh - Global Challenge
66/67
-
7/31/2019 Marsh - Global Challenge
67/67
Summary
Fragility fractures will present an unmanageable
problem all over the world unless we act now
Secondary prevention and multidisciplinarymanagement are the
keys to success
The international forum for exchanging ideas and
stimulating action is the Fragility FractureNetwork of the Bone
and Joint Decade
[email protected]
mailto:[email protected]:[email protected]://www.ff-network.org/http://www.ff-network.org/http://www.ff-network.org/