The Importance of Maternal Mortality Measurement
1-2 November 2010
Colombo, Sri Lanka
Christopher J.L. Murray
Institute Director
Maternal Mortality Workshop

Outline• Scope and purpose of the workshop
• Background
• Concepts and definitions
• Metrics
• Obstacles to the measurement of maternal mortality
2

Specific Objectives
I. To discuss maternal mortality trends across Asia and to consider the strengths and weaknesses of current scientific approaches to estimating maternal mortality
II. To learn about accessible data sources that can be utilized to produce estimates of maternal deaths at the global and country levels.
III. To compare methods and results from WHO and IHME
IV. To discuss the implications of more than one figure of MMR (estimates) for the same country
V. To define next steps for improving maternal deaths estimates
3

Outline• Scope and purpose of the workshop
• Background
• Concepts and definitions
• Metrics
• Obstacles to the measurement of MM
4

Global maternal mortality measurement
• Widespread perception that progress on maternal mortality is lagging behind other key MDG health indicators
• Complicated by belief that maternal mortality is very difficult to measure
• Need to assess progress given international commitment to Millennium Development Goal 5
o MDG 5 target: reduce the maternal mortality ratio by three-quarters from 1990 to 2015
5

Broader Context
• Safe Motherhood Initiative in 1987
o Response to a lack of focus on maternal health through primary health care programs
• 1994 International Conference on Population and Development
• Millennium Declaration
• Obama administration’s Global Health Initiative prompting renewed policy attention
• Civil society groups such as the White Ribbon Alliance raising the profile of the issue
6

Recent Monitoring Efforts
• Beginning in 1996, WHO sponsored development of country estimates for 1990, 1995, 2000, 2005
• Assessments have been controversial with countries
• Recent assessment (Hill et al, 2007) reported 576,300 maternal deaths in 1990 and 535,900 in 2007
• 0.48% annual rate of decline in the global maternal mortality ratio
7

Opportunities for a Robust Reassessment of Maternal Mortality
• Global Burden of Disease (GBD) study has undertaken correction of vital registration data
• Methodological advances in correcting sibling history data for known biases (survivor bias, recall bias, zero-sibs bias)
• Growing body of population-based verbal autopsy studies
• New estimates of all-cause reproductive-aged female mortality (Rajaratnam, 2010, The Lancet)
• Methodological developments in other fields provide improved estimation tools
8

Outline• Scope and purpose of the workshop
• Background
• Concepts and definitions
• Metrics
• Obstacles to the measurement of MM
9

Maternal deaths evolution
• Since ICD 1st until ICD 8th revision (1900-1978): deaths where the cause-of-death was identified as complications of pregnancy, childbirth, and the puerperium
• In 1979, ICD 9th revision incorporated explicit definition around the timing of the death
o Kept the same concept but with a limitation of time, “…until 42 days after end of pregnancy”. Indirect obstetric causes were included (647 and 648)
• In 1994 (ICD 10th revision) the definition remained related with complications and time, but included two new concepts:
o Pregnancy-related death
o Late maternal death (O96 and O97)
10

Maternal deaths
11
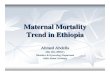
Maternal mortality ratio, USA, 1915-2003 ICD Revision
Year of use
ICD Codes
Observations
1st 1900-09 151-159 Deaths where the cause-of-death codes were identified as complications of pregnancy, childbirth, and the puerperium
2nd 1910-20 134-141 3rd 1921-29 143-150 4th 1930-38 140-150 5th 1939-48 140-150
6th 1949-57 640-689 Change in DC format, UCD, rules for coding
7th 1958-67 640-689 8th 1968-78 630-678 9th 1979-92 630-676 Until 42 days of the end
of pregnancy More Indirect Obstetric causes
10th 1993-2014? O00-O99 Late maternal death Pregnancy related death Box in DC
11th 2014

Definitions
• Maternal death: “death of a woman while pregnant or within 42 days of termination of pregnancy…from any cause related to the pregnancy or its management, but not from accidental or incidental causes” (ICD-10)
• For inter-temporal and international comparisons, ICD and MDG manual recommend A+B+C excluding D+E+F
Direct Indirect HIV Incidental
Early maternal (<42 days) A B C D
Late maternal (> 42 days & < 1 year) E F
12

Maternal Deaths O00-O99
• The ICD 10th revision definition allows identification of maternal deaths, based on their causes, as either direct or indirect.
o Direct obstetric deaths are those resulting from obstetric complications of the pregnant state (pregnancy, delivery, and postpartum), from interventions, omissions, incorrect treatment, or from a chain of events resulting from any of the above, for example, haemorrhage, pre-eclampsia/eclampsia or those due to complications of anaesthesia or caesarean section
o Indirect obstetric deaths are those resulting from previous existing disease, or diseases that developed during pregnancy, and which were not due to direct obstetric causes but aggravated by physiological effects of pregnancy, for example, deaths due to aggravation of an existing cardiac or renal disease
13

Maternal Deaths O00-O99
• Direct obstetric deaths (ICD 10th O00-O95)o O00-O08 Pregnancy with abortive outcome
o O10-O16 Edema, proteinuria and hypertensive disorders in pregnancy, childbirth and the puerperium
o O20-O29 Other maternal disorders predominantly related to pregnancy
o O30-O48 Maternal care related to the fetus and amniotic cavity and possible delivery problems
o O60-O75 Complications of labour and delivery
o O85-O92 Complications predominantly related to the puerperium
o O95 Obstetric death of unspecified cause
• Indirect obstetric deaths (ICD 10th O98-O99)o O98 Maternal infectious and parasitic diseases classifiable elsewhere but
complicating pregnancy, childbirth and the puerperium
o 099 Other maternal diseases classifiable elsewhere but complicating pregnancy, childbirth and the puerperium
14

Other maternal deaths
• Late maternal deaths
o The death of a woman from direct or indirect obstetric causes, more than 42 days but less than one year after termination of pregnancy
─ O96 Death from any obstetric cause occurring more than 42 days but less than one year after delivery and
─ O97 Death from sequelae of direct obstetric causes
• Pregnancy-related maternal death
o The death of a woman while pregnant or within 42 days of termination of pregnancy, irrespective of the cause of death
15

Incidental deaths
Due to conditions occurring during pregnancy, even though the pregnancy was unlikely to have contributed significantly to the death, i.e. accidents, murder, self-inflected, poisoning, etc.
•Various definitions across countries make it difficult
•Sometimes indirect causes fall under this category
•Some countries include suicides related with depression post-partum as maternal deaths (i.e. Brazil) and others do not
16

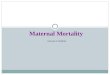
Distribution of maternal deaths by group of causes by GBD region
17
%Direct Obst. Deaths 82.6 Indirect Obst. Deaths 15.2Late Maternal Deaths 2.2
ICD 10th Direct (O00-O95); Indirect (O98-O99); Late (O96-O97)

Distribution of maternal deaths by group of causes, 1995-2008
18
ICD 10th Direct (O00-O95); Indirect (O98-O99); Late (O96-O97)

Measuring Maternal Deaths using different sources
• Countries with Vital Registrationo Obstetric (direct and indirect) + late maternal
• Countries with Verbal Autopsieso Obstetric (direct and indirect) + late maternal
o Incidental and deaths related with pregnancy (?)
• Countries with Surveys, Census (sibling method)o Deaths related with pregnancy
19
1. In strict sense, there are problems of comparability among countries and across time
2. WHO (ICD Collab. Centers) are proposing more changes:• Depression post delivery, Suicide• HIV-AIDS as indirect• Consequences of medical care and eliminate Obstructed labor• Etc.

Outline• Scope and purpose of the workshop
• Background
• Concepts and definitions
• Metrics
• Obstacles to the measurement of MM
20

Metrics
Direct measures based in VR or VA
• Maternal mortality ratio
• Maternal mortality rate (age std) or specific by age
• Proportion of maternal deaths
• Lifetime risk of maternal death
Indirect measures based in Surveys and Censuses
• Proportion of maternal deaths
21

Maternal Mortality Ratio (MMR)• Number of maternal deaths during a given time period per
100 000 live births during the same time-period.
22
Maternal Mortality Rate
• Number of maternal deaths during a given time period per 100 000 women during the same time-period, also can be age-specific
Proportion of maternal deaths (PMDF)
• Number of maternal deaths during a given time period divided by all deaths of women at reproductive age

Outline• Scope and purpose of the workshop
• Background
• Concepts and definitions
• Metrics
• Obstacles to the measurement of MM
23

In spite of standard definitions
• First, it is challenging to identify maternal deaths precisely, particularly in settings where routine recording of deaths is not complete within civil registration systems, and the death of a woman of reproductive age might not be recorded.
• Second, even if such a death were recorded, the woman’s pregnancy status may not have been known and the death would therefore not have been reported as a maternal death even if the woman were pregnant.
• Third, in most developing-country settings where medical certification of cause of death does not exist, accurate attribution of a female death as a maternal death is difficult.
24

Potential reasons for misclassification
• Inadequate understanding of ICD rules (either ICD-9 or ICD-10).
• Death certificates completed without mention of pregnancy status.
• Desire to avoid litigation.
• Desire to suppress information (especially as related to abortion deaths).
25

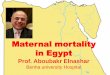
Awareness
26
Changes:ICD9 to ICD 10 in 1999States with question 36
1996-98 16 1999-00 172000-02 182003 21
Recommended