lable at ScienceDirect
Geriatric Nursing xx (2014) 1e6
Contents lists avai
Geriatric Nursing
journal homepage: www.gnjournal .com
Feature Article
Motivational interviewing for older adults in primary care:A systematic review
Janet Purath, PhD *, Annmarie Keck, BSN, Cynthia E. Fitzgerald, PhDWashington State University, College of Nursing, P.O. Box 1495, Spokane, WA 99210, USA
a r t i c l e i n f o
Article history:Received 5 December 2013Received in revised form25 January 2014Accepted 3 February 2014Available online xxx
Keywords:Motivational interviewingPrimary careOlder adultsHealth behavior change
Funding: No additional funding from any source wathis systematic review.* Corresponding author. Tel.: þ1 509 9518808; fax:
E-mail address: [email protected] (J. Purath).
0197-4572/$ e see front matter � 2014 Mosby, Inc. Ahttp://dx.doi.org/10.1016/j.gerinurse.2014.02.002
a b s t r a c t
Chronic disease is now the leading cause of death and disability in United States. Many chronic illnessesexperienced by older adults can be prevented or managed through behavior change, making patientcounseling an essential component of disease prevention and management. Motivational Interviewing(MI), a type of conversational method, has been effective in eliciting health behavior changes in people ina variety of settings and may also be a useful tool to help older adults change. This review of the literatureanalyzes current research and describes potential biases of MI interventions that have been conducted inprimary care settings with older adults. MI shows promise as a technique to elicit health behavior changeamong older adults. However, further study with this population is needed to evaluate efficacy of MIinterventions in primary care settings.
� 2014 Mosby, Inc. All rights reserved.
Background
Advances in public health, such as improved sanitation, antibi-otics, and vaccinations have contributed to a dramatic reduction indeath and disability from infectious disease. As a result, people inthe developed world are living longer. Longer life spans increasethe likelihood of acquiring chronic illness, the leading cause ofdeath and disability in the US.1 While 80% of Americans have atleast one chronic health condition, aging does not inevitably lead topoor health.2 Many chronic illnesses experienced by older adultscan be prevented or managed through behavior change, makingpatient counseling an essential component of disease preventionand management for health care providers.
In 1983, William Miller pioneered the use of MotivationalInterviewing (MI), a communication method that employs client-centered counseling to elicit and strengthen motivation forbehavior change.3 Originally described as a communication approachfor use in helping problem drinkers, in 2008, Rollnick, Miller, andButler described an expansion of its use in addressing awide array ofhealth behavior changes needed to combat and manage chronicdisease.4 To date, more than 200 randomized control trials and1000 publications have described its use in a variety of clinicalsettings.5,6
s provided to the authors of
þ1 509 3247341.
ll rights reserved.
MI posits that persons considering behavior change experienceambivalence related to the pros and cons of change. MI seeks tohelp people resolve ambivalence by engaging them in a workingrelationship and focusing communication on change. The methodseeks to evoke the client’s own motivation for change, developcommitment to change, and formulate concrete plans for behaviorchange. MI is particularly useful for older adults because olderadults bring with them symptoms, emotions, motives, and beliefsthat are important to change.7 Further, older adults value collabo-rative communication with health care providers8 and may sustainbehavior change more effectively following interventions thatemphasize collaboration.9 A central premise of MI is to encouragethe use of “Change Talk” in which the patient explores reasons forchange. Key communication skills used in MI include: 1) askingopen-ended questions rather than instructing the patient on whatthey should do, 2) affirming, 3) reflecting, 4) summarizing, and 5)providing individualized information and advice with the patient’spermission.10 The MI practitioner focuses on the person’s presentinterests and difficulties and tries to resolve the ambivalence byeliciting and selectively reinforcing “change talk” that will ulti-mately support behavior change.10 Health care team members mayfind MI to be useful when discussing lifestyle changes, settingbehavioral goals, discussing medication use and adherence, anddeveloping plans of care in collaborationwith patients. For MI to beeffective, some degree of formal training in the spirit of MI andpractice with techniques are essential for proficiency in themethod. For some conditions, MI may be more effective whenpaired with other interventions (e.g., pairing MI with participation
J. Purath et al. / Geriatric Nursing xx (2014) 1e62
in a recovery program for substance abuse or using MI to improveparticipation in diabetes education).4 In addition, because MI re-quires a significant amount of insight and communication ability, itmay not be an appropriate strategy for older adults with cognitiveimpairments.
Several reviews have evaluated randomized controlled trials(RCTs) that explored the use of MI in primary care settings. Van-Buskirk and Wetherell11 identified 9 studies in which MI was moreeffective than other behavior change strategies in achieving a va-riety of outcomes in primary care patients. None of the studiesreviewed by these authors included older adults, despite increasingevidence describing the importance of offering preventive healthand risk reduction interventions to this rapidly increasing popula-tion.12,13 Cummings and colleagues14 reviewed 15 studies that re-ported on the use of MI interventions with older adults. However,only four of the reviewed studies had samples where the mean ageof participants was 60 years or greater.
Objective
As understanding grows about the relationships betweenbehavior change and health status improvement for older adults, itis important to determine if MI can be successful in helping thispopulation achieve and sustain behavior change that will lead toimproved health outcomes. The purpose of this paper is to sys-tematically review research studies inwhichMI interventions wereused to elicit health-related behavior change among older adults inprimary care settings.
Review methods
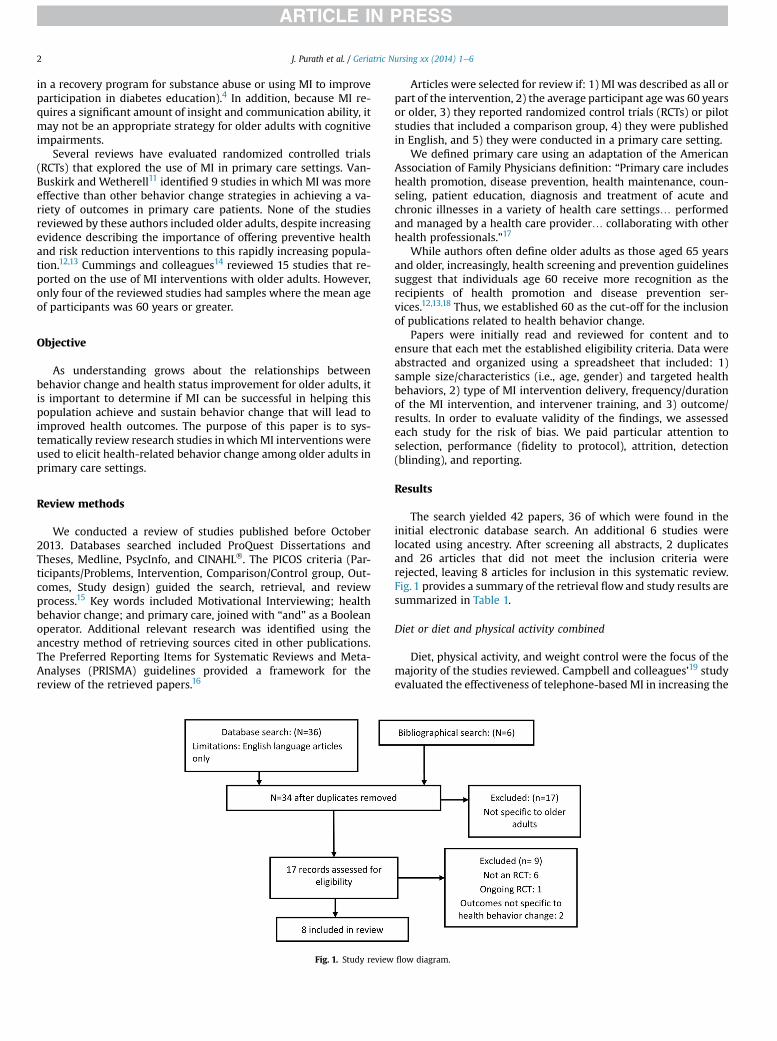
We conducted a review of studies published before October2013. Databases searched included ProQuest Dissertations andTheses, Medline, PsycInfo, and CINAHL�. The PICOS criteria (Par-ticipants/Problems, Intervention, Comparison/Control group, Out-comes, Study design) guided the search, retrieval, and reviewprocess.15 Key words included Motivational Interviewing; healthbehavior change; and primary care, joined with “and” as a Booleanoperator. Additional relevant research was identified using theancestry method of retrieving sources cited in other publications.The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines provided a framework for thereview of the retrieved papers.16
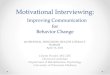
Fig. 1. Study review
Articles were selected for review if: 1) MI was described as all orpart of the intervention, 2) the average participant agewas 60 yearsor older, 3) they reported randomized control trials (RCTs) or pilotstudies that included a comparison group, 4) they were publishedin English, and 5) they were conducted in a primary care setting.
We defined primary care using an adaptation of the AmericanAssociation of Family Physicians definition: “Primary care includeshealth promotion, disease prevention, health maintenance, coun-seling, patient education, diagnosis and treatment of acute andchronic illnesses in a variety of health care settings. performedand managed by a health care provider. collaborating with otherhealth professionals.”17
While authors often define older adults as those aged 65 yearsand older, increasingly, health screening and prevention guidelinessuggest that individuals age 60 receive more recognition as therecipients of health promotion and disease prevention ser-vices.12,13,18 Thus, we established 60 as the cut-off for the inclusionof publications related to health behavior change.
Papers were initially read and reviewed for content and toensure that each met the established eligibility criteria. Data wereabstracted and organized using a spreadsheet that included: 1)sample size/characteristics (i.e., age, gender) and targeted healthbehaviors, 2) type of MI intervention delivery, frequency/durationof the MI intervention, and intervener training, and 3) outcome/results. In order to evaluate validity of the findings, we assessedeach study for the risk of bias. We paid particular attention toselection, performance (fidelity to protocol), attrition, detection(blinding), and reporting.
Results
The search yielded 42 papers, 36 of which were found in theinitial electronic database search. An additional 6 studies werelocated using ancestry. After screening all abstracts, 2 duplicatesand 26 articles that did not meet the inclusion criteria wererejected, leaving 8 articles for inclusion in this systematic review.Fig. 1 provides a summary of the retrieval flow and study results aresummarized in Table 1.
Diet or diet and physical activity combined
Diet, physical activity, and weight control were the focus of themajority of the studies reviewed. Campbell and colleagues’19 studyevaluated the effectiveness of telephone-based MI in increasing the
flow diagram.
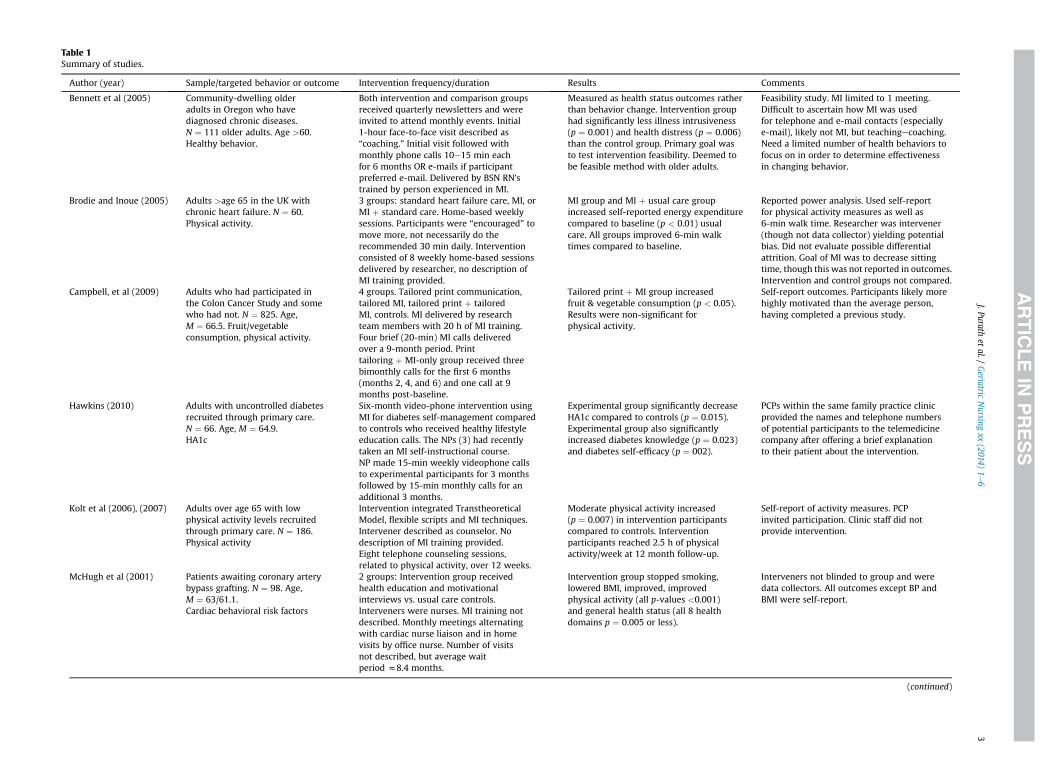
Table 1Summary of studies.
Author (year) Sample/targeted behavior or outcome Intervention frequency/duration Results Comments
Bennett et al (2005) Community-dwelling olderadults in Oregon who havediagnosed chronic diseases.N ¼ 111 older adults. Age >60.Healthy behavior.
Both intervention and comparison groupsreceived quarterly newsletters and wereinvited to attend monthly events. Initial1-hour face-to-face visit described as“coaching.” Initial visit followed withmonthly phone calls 10e15 min eachfor 6 months OR e-mails if participantpreferred e-mail. Delivered by BSN RN’strained by person experienced in MI.
Measured as health status outcomes ratherthan behavior change. Intervention grouphad significantly less illness intrusiveness(p ¼ 0.001) and health distress (p ¼ 0.006)than the control group. Primary goal wasto test intervention feasibility. Deemed tobe feasible method with older adults.
Feasibility study. MI limited to 1 meeting.Difficult to ascertain how MI was usedfor telephone and e-mail contacts (especiallye-mail), likely not MI, but teachingecoaching.Need a limited number of health behaviors tofocus on in order to determine effectivenessin changing behavior.
Brodie and Inoue (2005) Adults >age 65 in the UK withchronic heart failure. N ¼ 60.Physical activity.
3 groups: standard heart failure care, MI, orMI þ standard care. Home-based weeklysessions. Participants were “encouraged” tomove more, not necessarily do therecommended 30 min daily. Interventionconsisted of 8 weekly home-based sessionsdelivered by researcher, no description ofMI training provided.
MI group and MI þ usual care groupincreased self-reported energy expenditurecompared to baseline (p < 0.01) usualcare. All groups improved 6-min walktimes compared to baseline.
Reported power analysis. Used self-reportfor physical activity measures as well as6-min walk time. Researcher was intervener(though not data collector) yielding potentialbias. Did not evaluate possible differentialattrition. Goal of MI was to decrease sittingtime, though this was not reported in outcomes.Intervention and control groups not compared.
Campbell, et al (2009) Adults who had participated inthe Colon Cancer Study and somewho had not. N ¼ 825. Age,M ¼ 66.5. Fruit/vegetableconsumption, physical activity.
4 groups. Tailored print communication,tailored MI, tailored print þ tailoredMI, controls. MI delivered by researchteam members with 20 h of MI training.Four brief (20-min) MI calls deliveredover a 9-month period. Printtailoring þ MI-only group received threebimonthly calls for the first 6 months(months 2, 4, and 6) and one call at 9months post-baseline.
Tailored print þ MI group increasedfruit & vegetable consumption (p < 0.05).Results were non-significant forphysical activity.
Self-report outcomes. Participants likely morehighly motivated than the average person,having completed a previous study.
Hawkins (2010) Adults with uncontrolled diabetesrecruited through primary care.N ¼ 66. Age, M ¼ 64.9.HA1c
Six-month video-phone intervention usingMI for diabetes self-management comparedto controls who received healthy lifestyleeducation calls. The NPs (3) had recentlytaken an MI self-instructional course.NP made 15-min weekly videophone callsto experimental participants for 3 monthsfollowed by 15-min monthly calls for anadditional 3 months.
Experimental group significantly decreaseHA1c compared to controls (p ¼ 0.015).Experimental group also significantlyincreased diabetes knowledge (p ¼ 0.023)and diabetes self-efficacy (p ¼ 002).
PCPs within the same family practice clinicprovided the names and telephone numbersof potential participants to the telemedicinecompany after offering a brief explanationto their patient about the intervention.
Kolt et al (2006), (2007) Adults over age 65 with lowphysical activity levels recruitedthrough primary care. N ¼ 186.Physical activity
Intervention integrated TranstheoreticalModel, flexible scripts and MI techniques.Intervener described as counselor. Nodescription of MI training provided.Eight telephone counseling sessions,related to physical activity, over 12 weeks.
Moderate physical activity increased(p ¼ 0.007) in intervention participantscompared to controls. Interventionparticipants reached 2.5 h of physicalactivity/week at 12 month follow-up.
Self-report of activity measures. PCPinvited participation. Clinic staff did notprovide intervention.
McHugh et al (2001) Patients awaiting coronary arterybypass grafting. N ¼ 98. Age,M ¼ 63/61.1.Cardiac behavioral risk factors
2 groups: Intervention group receivedhealth education and motivationalinterviews vs. usual care controls.Interveners were nurses. MI training notdescribed. Monthly meetings alternatingwith cardiac nurse liaison and in homevisits by office nurse. Number of visitsnot described, but average waitperiod z8.4 months.
Intervention group stopped smoking,lowered BMI, improved, improvedphysical activity (all p-values <0.001)and general health status (all 8 healthdomains p ¼ 0.005 or less).
Interveners not blinded to group and weredata collectors. All outcomes except BP andBMI were self-report.
(continued)
J.Purathet
al./Geriatric
Nursing
xx(2014)
1e6
3

Table
1(con
tinu
ed)
Author
(yea
r)Sa
mple/targe
tedbe
hav
ioror
outcom
eInterven
tion
freq
uen
cy/duration
Results
Com
men
ts
Simset
al(199
8)Prim
arycare
patients
>ag
e65
.N
¼20
.Age
,M¼
72.2.
Physical
activity
2grou
ps.Interven
tion
received
hom
e-ba
sed,
unsu
pervised,inform
ationwithmotivational
telephon
ecalls
basedon
Tran
stheo
retical
Mod
el.Interven
erswerenurses.T
raining
not
described
.Te
lephon
ecallat
2an
d6wee
ks.
Nosign
ificantincrea
sein
activity
inthetrea
tmen
tgrou
p.
Underpow
ered
.Con
trol
grou
pinterven
tion
not
described
.Used“m
otivational
interviews”
tech
niquean
dtrainingnot
described
.Unclea
rhow
interven
tion
andco
mparison
grou
pprotoco
lwereim
plemen
tedin
order
toco
ntrol
forco
ntaminationof
interven
tion
.Pilotstudy.
Nofollo
w-upinterven
tion
iden
tified
intheliterature.
Smithet
al(199
7)Obe
sewom
enwithNID
DM.N
¼22
(16co
mpletedstudy).A
ge,M
¼62
.4.
Diet,physical
activity,g
luco
seco
ntrol.
2grou
ps.Usu
alcare
included
caloriean
dfat
gram
reco
mmen
dations,increa
sephysical
activity
andhom
egluco
semon
itoring.
Activityan
dcalories
wereself-m
onitored
.Interven
tion
grou
preceived
usu
alcare
þ3
individualized
MIsessionsco
nducted
by2psych
olog
ists
experiencedin
MI.
Bothgrou
pslost
weigh
tco
mpared
toba
selin
e,(p
<0.00
01).Interven
tion
participan
tshad
better
gluco
seco
ntrol
compared
tousu
alcare
(p¼
0.02
).
Well-described
MIinterven
tion
.Fidelitynot
addressed
withrega
rdto
MIdelivery.
Pilot
study,
underpow
ered
.27%
dropou
trate
with
nodescription
ofch
aracteristicsof
dropou
ts.
J. Purath et al. / Geriatric Nursing xx (2014) 1e64
consumption of fruits and vegetables and physical activity. Studyprocedures were well described. Details were provided about stafftraining, monitoring, evaluation of the fidelity of the MI technique,and interview coding methods that were used in the study. Theoutcomes of food intake and physical activity were self-reported bystudy participants. Measurement of a biomarker, plasma caroten-oids, was used to validate dietary self-report. Intervention partici-pants increased fruit and vegetable consumption but not physicalactivity.
Two smaller studies evaluated MI interventions with personswith diabetes. The earlier of these, a study of women with obesityand Type II diabetes, measured outcomes related to a behavioralintervention and included completion of food diaries, recordedblood glucose levels, physical activity, objectively measured gly-cemic control, and weight loss.20 Two psychologists trained in MIprovided the intervention. No discussion of MI intervener trainingorMI intervention fidelity was presented. MI techniques were well-described and congruent with MI principals. Only 16 womencompleted the last data collection, representing a 27% drop out rate.At the completion of the study, intervention participants had betterglucose control than the comparison group.
Hawkins21 evaluated a 6-month MI intervention using briefvideophone calls compared to the videophone calls that includedhealthy-lifestyle education. Outcomes were glycemic control anddiabetes self-management skills. Participants were older adultswith HA1C levels greater than 7.0 mg/dl (N ¼ 66). Two nursepractitioners trained with an MI self-instructional course deliveredthe intervention. Transcripts of three intervention calls were codedfor content, although neither the coding method nor coding resultswere described. A lag for some participants between baselinemeasures and start of the study (reported as 0e48 days) may haveallowed maturation to affect study results. Compared to controls,intervention participants decreased HA1C levels and increaseddiabetes knowledge and diabetes self-efficacy.21
Physical activity
Three trials focused on physical activity alone as the healthbehavior outcome measure. In a randomized control trial involving186 older adults, Kolt and colleagues tested the effectiveness oftelephone counseling using MI techniques with inactive olderadults.22,23 Primary care physicians from three practices screenedall older adults in their practices andmailed letters inviting them toparticipate. In addition, some patients were recruited by studypersonnel in clinic waiting rooms. Telephone calls to interventionparticipants followed specific but flexible scripts that were basedon the individual’s stage of change of physical activity. Interviewertraining in MI was not described, nor were the MI techniques. Alldata were self-report. At 3 months, the intervention groupincreased all areas of physical activity when compared to controls.At 12 months, total moderate leisure activity time was the onlysignificant finding, indicating a dampening of effect over time.Intervention participants increased physical activity compared tocontrols.
Sims and colleagues24 reported on a pilot study (N ¼ 20) thattested the feasibility of a physical activity intervention using MItechniques. Participants were recruited from two primary carepractices. The intervention was described as a motivational tele-phone interview by a nurse that encouraged the development of anindividualized exercise plan. Study length appeared to be eightweeks. The intervention group received telephone calls at 2 and 6weeks. Content of the telephone calls was described as based on theStages of Change rather than MI. This small sample did not yieldsignificant change in physical activity.

J. Purath et al. / Geriatric Nursing xx (2014) 1e6 5
Brodie and Inoue25 compared the effectiveness of a physicalactivityMI intervention to usual care in a group of older adults withchronic heart failure. Participants were recruited from a generalmedical ward in one of two UK hospitals. Sixty of 92 enrolleescompleted the 5-month study, a 35% drop out rate. The studyevaluated groups that received usual care, usual care with MI, andMI alone. Specifics of the MI intervention were not described, butthe timing of the interventions and an overview of the strategiesused were discussed. MI training and evaluation of MI treatmentdelivery were not addressed. Comparison of intervention to usualcare groups was not reported. One study goal was to decreasesitting time, although this was not reported in outcomes. Partici-pants in the MI-alone group and the MI plus usual care bothincreased self-reported physical activity when compared tobaseline.
Health risk and healthy behavior
Bennett and colleagues26 evaluated the feasibility of an inter-vention that coupled the Transtheoretical Model andMI techniquesin an intervention of older adults with one ormore chronic diseases(N ¼ 111). The study evaluated intervention feasibility as well aschanges in health status in persons who received nurse coachingcompared to controls. Older community members were recruitedby direct mail and from a pool of persons excluded from a previousstudy. Details about client enrollment and follow-up were wellreported. Fifteen per cent of the 66 individuals who received theintervention and 26% of those in the control group did not completethe study. Significantly less illness intrusiveness and health distresswere noted in intervention participants compared to controls.
McHugh and Lawler27 conducted a nurse-led effectivenessstudy using MI to measure changes in coronary heart disease riskfactors and general health status in persons awaiting cardiac arterybypass surgery. An office nurse and a cardiac nurse specialist nursedelivered health education to all participants (N ¼ 98). In addition,the experimental group participated in motivational interviews(N ¼ 49) on alternating months. Neither training nor interventionfidelity was described. The study reported several objectivelymeasured outcomes; however, some important measures, such assmoking status and physical activity, were self-reported. Inter-vention participants stopped smoking, lost weight, improvedphysical activity, and improved health status compared to controls.
Quality assessment results
MI has gained a great deal of popularity as an interventionmethod. Its use represents a convergence of science and practice.28
Critical factors such as the dynamic nature of change and a focus oncommunication and empathy make MI interventions difficult tomanualize and control. We might consider MI to be a “fluid”intervention. The AHRQ describes these as interventions for whichthe protocol explicitly allows for modification based on patientneeds, and notes that such fluidity does not mean the interventionsare implemented incorrectly.29 However, when researchersdescribe an intervention that uses motivational coaching, motiva-tional techniques, or MI principals without a clear description ofmethods and training it is difficult to determine whether theintervention was true to MI principals. That being said, thereremain weaknesses in the reviewed research.
Selection bias and confoundingRisk for selection bias is a potential concern when primary care
settings are used as sites for intervention studies. Two of thereviewed studies,21,24 reported using a recruitment strategy inwhich providers approached potential participants on their
caseload who they believed might be interested in participation.Approaching all eligible participants in a neutral manner wouldavoid the possibility that providers were influenced by precon-ceived notions about who in their population would be desirableparticipants. In addition, recruitment is often difficult and requiresmultiple strategies. Campbell and colleagues’19 strategy of recruit-ing participants from a previous study may have led to bias as aresult of exposure to information in the previous study, thoughstratification by group likely helped abate this issue.
Performance biasLack of fidelity to protocol, inadequate blinding, and systematic
differences in care all lead to potential performance bias. Most ofthe studies in this review reported a lack of blinding, a problem thatis difficult to address in behavioral interventions. However, whenthe primary researcher serves as the intervener, bias poses a seriousthreat. Studies that use clinic nurses to provide the intervention totheir own patients further adds concerns of performance bias.29
Attrition biasMost of studies in this review addressed attrition. Brodie and
Inoue25 reported the largest attrition rate but did not report dif-ferences between drop outs and those retained, nor did theydescribe an analysis of intention-to-treat. Studies reviewed heredid not consistently report drop-out rates. Even when drop-outrates were described, it was not clear that the significance ofattritionwas assessed, which would have strengthened the reports.
Detection biasIn studies reporting significant results, internal validity was
threatened by reliance on participant self-report of outcomes. BothSmith’s et al20 and Hawkins’s21 studies used objective measures asoutcomes. Using objective outcomes strengthens our confidencethat these findings have less risk for detection bias when comparedto those studies that used only self-report. A larger problem thatmay bias study outcomes relates to performance bias and lack ofintervention fidelity.29 In this review, MI training was extremelyvariable. Only one study provided evidence of counselor compe-tence in delivering MI.19 In addition, Campbell’s study reported thatindependent reviewers coded a subset of intervention interviewsfor MI content,19 the most accepted fidelity check for use of MI inintervention studies.28
Reporting biasMost studies reported outcomes that related directly to study
hypotheses and protocols. The study by Brodie and Inoue, however,reported onwalk time rather than sitting time, which they proposedto explore.25 Several studies described using MI or a motivationalintervention, but seemed to focus on motivation as a constructrather than as a specific technique with identifiable elements.
Conclusions
Related to review findings
This review of eight studies that evaluated the use of MI witholder adults indicates that MI may be effective when incorporatedinto health promotion and disease prevention interventions.Further, the use of MI may have potential as an application acrossdiverse professionals and health care settings. These findingsshould be viewed cautiously, because few studies reported MI in-terventions in sufficient detail to allow the reader to determineintervention quality. MI is heavily influenced by clinician andcontextual aspects of delivery. These are factors that can be learnedand understood but that cannot be standardized in a treatment

J. Purath et al. / Geriatric Nursing xx (2014) 1e66
manual.10 Since the basic principle of MI is person-centered care inwhich the client’s needs are the priority, many RCTs that use aprotocol for the delivery of MI interventions seem to use a meth-odology that is contrary to a client-centered approach. In addition,Miller and Rollnick note that provider empathy predicts variation inoutcomes even when the same treatment is delivered.10 This sug-gests that even protocol-driven interventions may be differentwhen delivered by different interveners.
In order to truly evaluate MI efficacy, the specific interventionneeds to be well-described. Making a determination of the effec-tiveness of health behavior interventions using MI would requirelarger sample sizes (similar to those reported in the Campbellstudy),12 adequate provider/intervener training, and careful atten-tion to MI fidelity. Future research reports should provide details ofthe training of MI interveners as well as specifics about the MI in-terventions themselves. Although PCPs in each of the trials mighthave conducted their own MI intervention with participants withchronic health conditions, none of the trials exclusively used theparticipants’ own PCP to conduct the MI intervention. This is likelydue to the need to optimize experimental control and to supportthe intervention efficacy. It would be useful to determine if MI in-terventions are effective, or more effective, when used by patients’own providers. This is particularly important in older adults, 92% ofwhom see their providers at least yearly.30
References
1. Centers for Disease Control and Prevention. Chronic Disease Prevention andHealth Promotion. http://www.cdc.gov/chronicdisease/overview/index.htm;Accessed 07.11.13.
2. Centers for Disease Control and Prevention. Healthy Aging: Helping People to LiveLong and Productive Lives and Enjoy a Good Quality of Life, http://www.cdc.gov/chronicdisease/resources/publications/AAG/aging.htm; 2011. Accessed 07.11.13.
3. Miller WR. Motivational interviewing with problem drinkers. Behav Psychother.1983;11:147e172. http://dx.doi.org/10.1017/S0141347300006583.
4. Rollnick S, Miller WR, Butler CC. Motivational Interviewing in Health Care:Helping Patients Change Behavior. New York: Guilford Press; 2008.
5. Miller WR, Rollnick S. What’s New Since MI-2?. Stockholm, Sweden: Interna-tional Conference on Motivational Interviewing; 2012 [June].
6. Motivational Interviewing. http://www.motivationalinterview.org//; n.d.Accessed 07.10.13.
7. Rejeski WJ, Brawley LR. Functional health: innovations in research on physicalactivity with older adults. Med Sci Sports Exerc. 2006;38(1):93e99.
8. Kemp EC, Floyd MR, McCord-Duncan E, Lang F. Patients prefer the methodof ‘tell back-collaborative inquiry to assess understanding of medical infor-mation’. J Am Board Fam Med. 2008;21:24e30. http://dx.doi.org/10.3122/jabfm.2008.01.070093.
9. Saczynski JS, Margrett JA, Willis SL. Older adults’ strategic behavior: effects ofindividual versus collaborative cognitive training. Educ Gerontol. 2004;30(7):587e610. http://dx.doi.org/10.1080/03601270490466985.
10. Miller WR, Rollnick S. Motivational Interviewing: Helping People Change. NewYork, NY: Guilford Press; 2013.
11. Vanbuskirk KA, Wetherell JL. Motivational interviewing with primary carepopulations: a systematic review and meta-analysis. J Behav Med; 2013. http://dx.doi.org/10.1007/s10865-013-9527-4. [Epub ahead of print].
12. U.S. Preventive Services Task Force. Screening for Osteoporosis: Systematic Re-view to Update the 2002 U.S. Preventive Services Task Force Recommendation,http://www.uspreventiveservicestaskforce.org/uspstf10/osteoporosis/osteoes.pdf; July 2010. Accessed 13.01.14.
13. Guide to Community Preventive Services. Interventions to Reduce DepressionAmong Older Adults: Home-based Depression Care Management, http://www.thecommunityguide.org/mentalhealth/depression-home.html; January 23, 2014.Accessed 24.01.14.
14. Cummings SM, Cooper RL, Cassie KM. Motivational interviewing to affectbehavior change in older adults. Res Soc Work. 2009;19:195e204. http://dx.doi.org/10.1177/1049731508320216.
15. Vaska M. Defining a Researchable Question: The PICOS Approach. CochraneReviewer’s Workshop, January 22-23, 2009. http://bit.ly/liiloHc; Accessed29.10.13.
16. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for sys-tematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med.2009;151:264e269.18.
17. American Academy of Family Practice. Primary Care, http://www.aafp.org/about/policies/all/primary-care.html; 2013. Accessed 01.11.13.
18. Cherry D, Lucas C, Decker SL. Population aging and the use of office-basedphysician services. NCHS Data Brief 2010;(41). Hyattsville, MD: National Cen-ter for Health Statistics.
19. Campbell MK, Carr C, Devellis B, et al. A randomized trial of tailoring andMotivational Interviewing to promote fruit and vegetable consumption forcancer prevention and control. Ann Behav Med. 2009;38:71e85. http://dx.doi.org/10.1007/s12160-009-9140-5.
20. Smith DE, Heckemeyer CM, Kratt PE, Mason DA. Motivational Interviewing toimprove adherence to a behavioral weight-control program for older obesewomen with NIDDM: a pilot study. Diabetes Care. 1997;20:52e54.
21. Hawkins SY. Improving glycemic control in older adults using a videophonemotivational diabetes self-management intervention. Res Theory Nurs Pract.2010;24:217e232. http://dx.doi.org/10.1891/1541-6577.24.4.217.
22. Kolt G, Oliver M, Schofield G, et al. An overview and process evaluation ofTeleWalk: a telephone-based counseling intervention to encourage walking inolder adults. Health Promot Int. 2006;21:201e208. http://dx.doi.org/10.1093/heapro/dal015.
23. Kolt G, Schofield G, Kerse N, et al. Effect of telephone counseling on physicalactivity for low-active older people in primary care: a randomized, controlledtrial. J Am Geriatr Soc. 2007;55:986e992. http://dx.doi.org/10.1111/j.1532-5415.2007.01203.x.
24. Sims J, Smith R, Duffy A, Holton S. Can practice nurses increase physical ac-tivity in the over 65s? Methodological considerations. Br J Gen Pract. 1998;48:1249e1250.
25. Brodie DA, Inoue A. Motivational interviewing to promote physical activity forpeople with chronic heart failure. J Adv Nurs. 2005;50:518e527. http://dx.doi.org/10.1111/j.1365-2648.2005.03422.x.
26. Bennett JA, Perrin NA, Hanson G, et al. Healthy aging demonstration project:nurse coaching for behavior change in older adults. Res Nurs Health. 2005;28:187e197. http://dx.doi.org/10.1002/nur.20077.
27. McHugh JE, Lawlor BA. Exercise and social support are associated withpsychological distress outcomes in a population of community-dwellingolder adults. Health Psychol. 2001;17:833e844. http://dx.doi.org/10.1177/1359105311423861.
28. Miller WR, Rose GS. Toward a theory of Motivational Interviewing. Am Psychol.2009;64:527e537. http://dx.doi.org/10.1037/a0016830.
29. Agency for Healthcare Research and Quality. Methods Guide for ComparativeEffectivenessReviews:Assessing theRiskofBias of Individual Studies inSystematicReviews of Health Care Interventions. http://effectivehealthcare.ahrq.gov/ehc/products/322/998/MethodsGuideforCERs_Viswanathan_IndividualStudies.pdf;n.d. Updated November 18, 2013. Accessed 20.11.13.
30. Centers for Disease Control and Prevention. Summary Health Statistics for U.S.Adults: National Health Interview Survey, 2011:16, http://www.cdc.gov/nchs/data/series/sr_10/sr10_256.pdf; 2012. Accessed 01.11.13.
Recommended