
Stem Cell Tandem Transplants Jun 17 1
National Medical Policy Subject: Tandem Stem Cell Transplants in the Adult Patient
Policy Number: NMP331
Effective Date*: March 2007
Update: June 2017
This National Medical Policy is subject to the terms in the
IMPORTANT NOTICE
at the end of this document
For Medicaid Plans: Please refer to the appropriate State’s Medicaid manual(s),
publication(s), citation(s), and documented guidance for coverage criteria and
benefit guidelines prior to applying Health Net Medical Policies
The Centers for Medicare & Medicaid Services (CMS)
For Medicare Advantage members please refer to the following for coverage guidelines first:
Use Source Reference/Website Link
X National Coverage Determination
(NCD) Stem Cell Transplantation:
http://www.cms.gov/medicare-coverage-
database/search/advanced-search.aspx
National Coverage Manual Citation
Local Coverage Determination (LCD)*
Article (Local)*
Other
None Use Health Net Policy
Instructions
Medicare NCDs and National Coverage Manuals apply to ALL Medicare members in ALL
regions.
Medicare LCDs and Articles apply to members in specific regions. To access your specific
region, select the link provided under “Reference/Website” and follow the search
instructions. Enter the topic and your specific state to find the coverage determinations
for your region. *Note: Health Net must follow local coverage determinations (LCDs) of Medicare
Administration Contractors (MACs) located outside their service area when those MACs have
exclusive coverage of an item or service. (CMS Manual Chapter 4 Section 90.2) If more than one source is checked, you need to access all sources as, on occasion, an
LCD or article contains additional coverage information than contained in the NCD or
National Coverage Manual.

Stem Cell Tandem Transplants Jun 17 2
If there is no NCD, National Coverage Manual or region specific LCD/Article, follow the
Health Net Hierarchy of Medical Resources for guidance.
Current Policy Statement Planned tandem transplantations (also known as sequential or double transplants)
consisting of an initial regimen of high dose chemotherapy (HDC) with autologous
stem cell support followed by another course of HDC with autologous transplant or
an allogeneic transplant using a suitably matched HLA donor of a close family
relative (e.g., preferably sibling) usually within a period of 2 to 6 months of each
other is considered medically necessary for any of the following malignancies in
patients with low to moderate surgical risk and no significant comorbid medical
conditions*:
1. Patients with primary testicular cancer who are in the first or second relapse or
whose tumors are refractory to a cisplatin-based chemotherapeutic regimen
2. For patients with multiple myeloma when all of the following are met:
Patient has Durie-Salmon stage I (one bone lesion), Stage II or III
myeloma (see table on Stages of Multiple Myeloma in Scientific Rationale
section); and
Patient has newly diagnosed or chemoresponsive multiple myeloma.
3. As an option for patients with multiple myeloma who do not achieve at least a very
good partial response (VGPR*) after the first autologous SCT. This should preferably
be done within a clinical trial.
*Note: VGPR refers to serum and urine M-protein detectable by immunofixation but
not on electrophoresis, or 90% or greater reduction in serum M-protein plus urine M-
protein level <100 mg per 24 hours. [i.e., Monoclonal (M)-proteins are found in both
the serum and/or urine of patients with a wide variety of clinical conditions. Serum
protein electrophoresis (SPEP) detects the presence and level of various proteins in
the blood, including M protein. Serum protein electrophoresis is used to identify
patients with multiple myeloma and other serum protein disorders. Urine Protein
Electrophoresis (uPEP) can provide quantification of the M protein. In monoclonal
gammopathies, a proteinuria pattern may show a discrete band produced by
monoclonal free light chains, or Bence-Jones Proteinuria (BJP)].
Note: Health Net, Inc. considers planned tandem transplantation not medically
necessary, in patients with indolent myeloma, smoldering myeloma, and monoclonal
gammopathy of uncertain significance [MGUS] because there is insufficient scientific
evidence in the medical literature as to its safety and effectiveness.
* General Criteria for Patient Selection – patient must have all of the
following:
Be medically compliant and free of an active substance or alcohol abuse problem; and
Be free of any active comorbid disease which would significantly reduce
short- term life expectancy

Stem Cell Tandem Transplants Jun 17 3
Specifically, Health Net, Inc. consider all of the following indications for tandem stem
cell transplant investigational, because although trials are ongoing, there is
insufficient scientific evidence in the medical literature to validate their safety and
effectiveness.
An initial course of high dose chemotherapy with autologous stem cell
transplantation (AuSCT) followed by non-marrow ablative chemotherapy
with AuSCT (“mini-transplant”) to treat multiple myeloma
Treatment of patients with amyloidosis
Treatment of patients with any stage, grade, or sub-type of Non-Hodgkin’s
Lymphoma (NHL)
Treatment of solid tumors of childhood
Health Net, Inc. considers all of the following indications for tandem stem cell transplant not
medically necessary:
Performance of the second course of chemotherapy and stem-cell support
at an interval of > 6 months after the first course
Planned tandem autologous stem cell transplantation as a treatment of all
other non-testicular germ cell tumors
A second or repeat allogeneic (ablative or non-myeloablative) transplant
due to persistent, progressive or relapsed disease
Treatment of PNETs including medulloblastoma and ependymoma
Treatment of Waldenstrom’s Macroglobulinemia
Codes Related To This Policy The codes listed in this policy are for reference purposes only. Listing of a code in this policy
does not imply that the service described by this code is a covered or non-covered health
service. Coverage is determined by the benefit documents and medical necessity criteria.
This list of codes may not be all inclusive.
On October 1, 2015, the ICD-9 code sets used to report medical diagnoses and
inpatient procedures have been replaced by ICD-10 code sets.
ICD-9 Codes 203.00-203.01 Multiple myelomas
164.2-164.9 Malignant neoplasm of mediastinum
186.0-186.9 Malignant neoplasm of testis
ICD-10 Codes C38-C38.8 Malignant neoplasm of heart, mediastinum and pleura
C62-C62.92 Malignant neoplasm of testis
C90-C90.32 Multiple myeloma and malignant plasma cell neoplasms
CPT Codes 38204 Management of recipient hematopoietic progenitor cell donor
search and cell acquisition

Stem Cell Tandem Transplants Jun 17 4
38205 Blood-derived hematopoietic progenitor cell harvesting for
transplantation, per collection; allogeneic
38206 Blood-derived hematopoietic progenitor cell harvesting for
transplantation, per collection; autologous
38207-38215 Transplant preparation of hematopoietic progenitor cells
38230 Bone marrow harvesting for transplantation, allogeneic
38232 Bone marrow harvesting for transplantation, autologous
38240 Hematopoietic progenitor cell (HPC); allogeneic transplantation
per donor
38241 Hematopoietic progenitor cell (HPC); autologous transplantation
HCPCS Codes S2142 Cord blood-derived stem cell transplantation, allogeneic
S2150 Bone marrow or blood-derived peripheral stem cells (peripheral or
umbilical), allogeneic or autologous, harvesting, transplantation,
and related complications; including pheresis and cell
preparation/storage, marrow ablative therapy, drugs, supplies,
hospitalization with outpatient follow-up, medical/surgical,
diagnostic, emergency, and rehabilitative services, and the
number of days of pre- and post-transplant care in the global
definition
Scientific Rationale – Update May 2016 The NCCN Guidelines (Version 3.2016) on Multiple Myeloma notes that “Potential
transplant candidates must undergo a stem cell harvest, collecting enough stem cells
for two transplants in anticipation of a tandem transplant or a second transplant,
within 6 months, as subsequent therapy. Alternatively, all patients may consider
continuation of primary therapy until the best response is reached. The optimal
duration of primary therapy after achieving maximal response is unknown; hence
maintenance therapy or observation can be considered beyond maximal response”.
The NCCN Guidelines (Version 2.2016) on Testicular Cancer notes: “Patients who do
not experience a durable complete response to first-line therapy or those who
experience a recurrence can be divided into those with a favorable or unfavorable
prognosis based on prognostic factors. These factors can be used in deciding whether
a patient is a candidate for conventional dose therapy or high-dose therapy with
stem cell support as a second line option”. Scientific Rationale – Update May 2015 Byrne et al (2015) reported on a prospective phase II clinical trial of multiple
myeloma (MM) patients who were randomized to receive a second (tandem)
autologous stem cell transplantation (ASCT) based on whether they achieved a
partial response or worse (≤PR) following initial ASCT (ASCT1). Patients who
achieved a very good partial response or better (≥VGPR) had salvage ASCT at
relapse. Seventy-five patients received conditioning therapy and ASCT1. A total of 44
patients (59%) achieved ≥VGPR, whereas 31 patients entered ≤PR and were offered
tandem ASCT. In all, 20 patients agreed to tandem ASCT. Demographic and clinical
characteristics were similar between the two cohorts except for median lactate
dehydrogenase (LDH) (P= 0.0141) and percentage of marrow plasma cells before
ASCT1 (P = 0.0047), both lower in the ≥VGPR group. Intent to treat analysis showed
that patients who achieved ≥VGPR to ASCT1 had a trend toward improved
progression-free survival (PFS) (37 vs. 26 months, P = 0.078) and superior overall

Stem Cell Tandem Transplants Jun 17 5
survival (OS) (not reached vs. 50 months, P = 0.0073). Patients with ≤PR who
declined tandem transplantation had shortened PFS (20 vs. 28 months, P = 0.05)
but similar OS (53 vs. 57.5 months, P = 0.29) compared to those who received it.
Thus, a favorable clinical response to ASCT1 identifies a low-risk group with superior
long-term prognosis despite similar PFS.
Iacobelli et al (2015) reported that previous studies have shown that obtaining
complete hematologic remission (CR) in multiple myeloma is an important predictor
of PFS and OS. This applies both to autologous and allogeneic transplantation.
However, the importance of CR obtained before vs after second transplant or
following allogeneic vs autologous transplantation is not clear. The author
investigated the role of CR analyzing data from the EBMT-NMAM2000 interventional
prospective study comparing tandem autologous/reduced intensity conditioning
allogeneic transplantation (auto/RICallo) to autologous transplantation-single or
double (auto/auto). Allocation to treatment was performed according to availability
of a matched sibling donor. Cox regression and multi-state models were applied. The
long-term probability of survival in CR was superior in auto/RICallo, both comparing
groups according to treatment allocated at start (28.8 vs 11.4% at 60 months,
P=0.0004) and according to actual administration of second transplant (25.6 vs
9.6% at 60 months, P=0.008). CR achieved before the second transplant was
predictive for PFS (hazard ratio (HR)=0.44, P= 0.003) and OS (HR 0.51, P=0.047)
irrespective of the type of second transplant. CR achieved after auto/RICallo was
more beneficial for PFS (HR=0.53, P=0.027) than CR after auto/auto (HR=0.81,
P=0.390), indicating a better durability of CR obtained after an allotransplant
procedure.
Scientific Rationale – Update May 2014 High-dose therapy with stem cell support is a critical component in the treatment
plan for eligible patients with newly diagnosed multiple myeloma (MM.) The types of
stem cell transplant (SCT) may be single autologous SCT, a tandem SCT (a planned
second course of high-dose therapy and SCT within 6 months of the first), or an
allogeneic SCT. An allogeneic SCT can either be performed after prior myeloablative
therapy or after nonmyeloablative therapy. A tandem transplant differs from a repeat
transplantation which is requested or performed more than 6 months after the first
transplant, and is used as salvage therapy after failure of initial transplantation or
relapsed disease. Nonmyeloablative therapy, also referred to as “mini transplant,”
is a technique to decrease toxicity of the allotransplant while preserving the
alloimmune graft-versus-myeloma effect. An allogeneic SCT may also follow an
autologous SCT.
Autologous SCT results in high response rates and remains the standard of care after
primary therapy for eligible patients with multiple myeloma. The NCCN Multiple
Myeloma panel recommends collecting enough stem cells for two eligible transplants
in ALL eligible patients. Per the Multiple myeloma panel, a tandem transplant with or
without maintenance therapy can be considered for all patients who are candidates
for SCT and is an option for patients who do not achieve at least a very good
partial response (VGPR) after the first autologous SCT. The benefit from the second
transplant in patients who are in complete response (CR), or VGPR and also in those
who achieve less than VGPR after the first SCT should preferably be answered in a
clinical trial. The other option for this group of patients includes maintenance
therapy or observation. NCCN notes that a randomized prospective NIH and
intergroup-supported trial is currently ongoing.

Stem Cell Tandem Transplants Jun 17 6
Imrie et al (2009) published guidelines on stem cell transplantation
recommendations in adults. Per the guidelines:
Autologous stem cell transplantation is the recommended treatment option for
eligible younger patients (under age 65-70 years) with newly diagnosed MM.
Tandem (double) autologous stem cell transplantation is an option for patients
who obtain less than a complete response to the first autologous transplant.
Repeat autologous transplantation is an option for patients with MM who relapse
after a long remission (> 2 years) to a single autologous transplant.
Allogeneic transplantation is an option for selected patients with MM including
those with high-risk cytogenetics and those whose disease is unresponsive to
primary therapy.
The guidelines states further that the evidence on the role of stem cell
transplantation in the management of multiple myeloma is rapidly emerging.
Kozelj et al (2013) reported that tandem autologous hematopoietic stem cell
transplantation (ta-HSCT) is a standard treatment for multiple myeloma (MM).
Patients receive a high-dose cyclophosphamide (CY), followed by two myeloablative
cycles of melphalan (MEL). There are scarce data about long term cardiotoxicity.
The authors studied 12 patients (62.25 ± 8.55 years) six years after the completion
of MM treatment with ta-HCST. Late cardiotoxic effects were evaluated clinically and
echocardiographically. None of the patients developed clinical signs of heart failure,
all were in sinus rhythm and NT-pro BNP concentration was elevated (778 ± 902.76
pg/mL). The left ventricular (LV) size remained normal. The LV ejection fraction did
not decrease (73.75 ± 5.67%, 69.27 ± 6.13%, p = NS). The LV diastolic function
parameters (E, A, ratio E/A and A/a) did not change significantly. In tissue Doppler
parameters we observed a nonsignificant decrease in Em (10.26 ± 2.63 cm/s, 7.57
± 1.43 cm/s) and Sm velocities (8.7 ± 0.87 cm/s, 7.14 ± 1.17 cm/s, p = NS). The
E/Em values were in an abnormal range (8.66 ± 1.05, 10.55 ± 2.03). The authors
concluded the treatment of MM with ta-HSCT, during which patients receive a high
dose CY followed by two myeloablative cycles of MEL, causes mild, chronic, partially
reversible and clinically silent cardiotoxic side-effects. However, ta-HSCT in patients
with MM is a safe regarding cardiotoxic side effects, but, because of increasing life
expectancy needs long term attention.
Gahrton et al (2013) reported long-term follow-up of prospective studies comparing
allogeneic transplantation to autologous transplantation in multiple myeloma is few and
controversial. They reported an update at a median follow-up of 96 months of the European
Group for Blood and Marrow Transplantation Non-Myeloablative Allogeneic stem cell
transplantation in Multiple Myeloma (NMAM)2000 study that prospectively compares tandem
autologous/reduced intensity conditioning allogeneic transplantation (auto/RICallo) to
autologous transplantation alone (auto). There are 357 myeloma patients up to age 69
years enrolled. Patients with an HLA-identical sibling were allocated to auto/RICallo (n =
108) and those without to auto alone (n = 249). At 96 months progression-free survival
(PFS) and overall survival (OS) were 22% and 49% vs 12% (P = .027) and 36% (P = .030)
with auto/RICallo and auto respectively. The corresponding relapse/progression rate (RL)
was 60% vs 82% (P = .0002). Non-relapse mortality at 36 months was 13% vs 3% (P =
.0004). In patients with the del(13) abnormality corresponding PFS and OS were 21% and
47% vs 5% (P = .026), and 31% (P = .154). Long-term outcome in patients with multiple
myeloma was better with auto/RICallo as compared with auto only and the auto/RICallo
approach seemed to overcome the poor prognostic impact of del(13) observed after

Stem Cell Tandem Transplants Jun 17 7
autologous transplantation. Follow up longer than 5 years is necessary for correct
interpretation of the value of auto/RICallo in multiple myeloma.
Kharfan-Dabaja et al (2013) reported that despite advances in understanding of
clinical, genetic, and molecular aspects of multiple myeloma (MM) and availability of
more effective therapies, MM remains incurable. The autologous-allogeneic (auto-
allo) hematopoietic cell transplantation (HCT) strategy is based on combining
cytoreduction from high-dose (chemo- or chemoradio)-therapy with adoptive
immunotherapy. However, conflicting results have been reported when an auto-allo
HCT approach is compared to tandem autologous (auto-auto) HCT. The authors
performed a systematic search that identified 152 publications, of which five studies
(enrolling 1538 patients) met inclusion criteria. All studies eligible for inclusion
utilized biologic randomization. Assessing response rates by achievement of at least
a very good partial response did not differ among the treatment arms [risk ratio (RR)
(95% CI)=0.97 (0.87-1.09), p=0.66]; but complete remission was higher in the
auto-allo HCT arm [RR=1.65 (1.25-2.19), p=0.0005]. Event-free survival did not
differ between auto-allo HCT group versus auto-auto HCT group using per-protocol
analysis [hazard ratio (HR)=0.78 (0.58-1.05)), p=0.11] or using intention-to-treat
analysis [HR=0.83 (0.60-1.15), p=0.26]. Overall survival (OS) did not differ among
these treatment arms whether analyzed on per-protocol [HR=0.88 (0.33-2.35),
p=0.79], or by intention-to-treat [HR=0.80 (0.48-1.32), p=0.39] analysis. Non-
relapse mortality (NRM) was significantly worse with auto-allo HCT [RR
(95%CI)=3.55 (2.17-5.80), p<0.00001]. The reviewers concluded despite higher
complete remission rates, there is no improvement in OS with auto-allo HCT; but this
approach results in higher NRM in patients with newly diagnosed MM. At present,
totality of evidence suggests that an auto-allo HCT approach for patients with newly
diagnosed myeloma should not be offered outside the setting of a clinical trial.
Armeson et al (2013) utilized meta-analysis to compare tandem autologous (TA)
hematopoietic SCT (auto-HSCT) or single auto-HSCT followed by reduced intensity
conditioning (RIC), allogeneic (AR) hematopoietic SCT in the upfront management of
patients with multiple myeloma (MM). A comprehensive search strategy of published and
unpublished reports utilized the following entry criteria: newly diagnosed patients, first
autologous transplantation in both arms, use of an RIC regimen and assignment to TA or AR
based exclusively on the availability of an HLA matched donor. Six trials were identified
yielding 1192 subjects in TA and 630 in AR. Patients in AR had higher likelihoods of TRM
(relative risk (RR)=3.3, 95% confidence interval (CI)=2.2-4.8) and CR (RR=1.4, 95%
CI=1.1-1.8). OS was not different in the first 36 months (hazard ratio (HR)=1.15, 95%
CI=0.91-1.45) or after (HR=0.74, 95% CI=0.53-1.04) 36 months from assignment. Similar
findings were seen for PFS. When compared with TA in the upfront management of MM, AR
is associated with higher TRM and CR without improvement in PFS or OS.
At this time, there is a clinical trial, a multicenter, prospective phase II-study investigating
safety and efficacy of the combination of auto-allo tandem stem cell transplantation in
patients with multiple myeloma and age of >55 years, followed by maintenance therapy
with low-dose Thalidomide and Donor Lymphocyte Infusions currently recruiting participants
(NCT00777998). Numerous other trials were identified on the Clinical trial.gov website
investigating tandem SCT for a variety of indications (e.g., high-risk neuroblastoma,
relapsed or refractory lymphoma, high risk solid tumors, refractory acute leukemia)
Scientific Rationale – Update May 2013 The NCCN Multiple Myeloma Panel (2013) recommends:

Stem Cell Tandem Transplants Jun 17 8
Collecting enough stem cells for two transplants, in all eligible patients. They state:
“A tandem transplant can be considered for all multiple myeloma patients who are
candidates for stem cell transplant (SCT), and is an option for patients who do not
achieve at least a very good partial response (VGPR) after the first autologous SCT.
The benefit from the second transplant in patients who are in complete response
(CR), or VGPR and also in those who achieve less than VGPR after the first SCT
should preferably be answered in a clinical trial.” The other option for this group of
patients includes maintenance therapy or observation.
The International Myeloma Working Group has response criteria for multiple
myeloma disease progression and relapse. Progressive disease is to be used for
calculation of time to progression and progression-free survival and points for all
patients including those in complete remission. Progressive disease requires one or
more of the following and an increase of > 25% from baseline in:
Serum M-component and/or (the absolute increase must be > 0.5g/Dl)2
Urine M-component and/or (the absolute increase must be > 200mg/24 hours
Only in patients without measurable serum and urine M-protein levels: the
difference between involved and uninvolved free light chain (FLC) levels. The
absolute increase must be over 10 mg/Dl
Bone marrow plasma cell percentage: the absolute % must be > 10%3
Definitive development of new bone lesions or soft tissue plasmacytomas or
definite increase in the size of existing bone lesions or soft tissue
plasmacyutomas
Development of hypercalcemia (corrected serum calcium >11.5 mg/dL or
2.65 mmo/L) that can be attributed solely to the plasma cell proliferative
disorder
Monoclonal or M-proteins are found in both the serum and/or urine of patients with a wide
variety of clinical conditions. The occurrence and clinical symptoms of these conditions vary
widely. Clearly the significance of M-proteins varies widely and the mere presence of an M-
protein must be evaluated in the clinical context for each patient.
Serum protein electrophoresis (SPEP) detects the presence and level of various proteins in
the blood, including M protein. Serum protein electrophoresis is used to identify patients
with multiple myeloma and other serum protein disorders. Electrophoresis separates
proteins based on their physical properties, and the subsets of these proteins are used in
interpreting the results. A homogeneous spike-like peak in a focal region of the gamma-
globulin zone indicates a monoclonal gammopathy. Monoclonal gammopathies are
associated with a clonal process that is malignant or potentially malignant, including
multiple myeloma, Waldenström’s macroglobulinemia, solitary plasmacytoma, smoldering
multiple myeloma, monoclonal gammopathy of undetermined significance, plasma cell
leukemia, heavy chain disease, and amyloidosis. The quantity of M protein, the results of
bone marrow biopsy, and other characteristics can help differentiate multiple myeloma from
the other causes of monoclonal gammopathy.
For the urine, it is important to follow the monoclonal free light chains and not the intact M-
protein immunoglobulin that may be found in the urine. The prognosis and threat to the
kidney is mainly due to the amount of monoclonal free light chain and not due to the intact
M-protein. Urine Protein Electrophoresis (uPEP) can provide quantification of the M protein.
In monoclonal gammopathies, a proteinuria pattern may show a discrete band produced by
monoclonal free light chains, or Bence-Jones Proteinuria (BJP).

Stem Cell Tandem Transplants Jun 17 9
The 2013 NCCN guidelines on Multiple Myeloma include and note this clinical trial by Fenk et
al. (2011), a retrospective case –matched control analysis, that was done comparing
patients who underwent a 2nd autologous SCT to those treated with conventional
chemotherapy for relapsed multiple myeloma. Similar to previously published smaller
studies, this analysis demonstrated that a 2nd autologous SCT is associated with superior
relapse-associated mortality compared with conventional chemotherapy (68% versus 78%)
along with improved overall survival (OS) (32% versus 22%) at 4 years. In this analysis,
factors associated with improved OS and progression free survival (PFS) included younger
age (<55 years), beta-2 microglobulin <2.5 mg/L at diagnosis, a remission duration of >9
months and a greater than partial remission (PR) to their 1st autologous SCT. This analysis
indicates that a 2nd autologous SCT, for relapsed or progressive MM patients, may be an
option for carefully selected patients. Some of these patients can achieve durable complete
or partial remission. Tandem SCT refers to a planned second course of high dose therapy
and SCT within 6 months of the first.
Scientific Rationale – Update March 2013 There is no conclusive evidence that high-dose therapy with or without
hematopoietic stem cell infusion at any point during treatment is beneficial for
patients with poor-risk localized and metastatic Ewing sarcoma family of tumors
(EFT). Seventy per cent of patients with EFT are under the age of 20 years old. Most
patients with advanced or recurrent disease need new approaches to improve
outcomes, and participation in clinical trials should be encouraged. Long-term follow-
up is needed following therapy because disease relapse, treatment-related
complications, and second malignancies all occur beyond five years after treatment
is initiated.
High dose chemotherapy and autologous hematopoietic cell transplantation can
achieve sustained remissions in some patients with recurrent or refractory Hodgkin
lymphoma. However, in the absence of randomized trials, a number of important
issues remain unresolved concerning this approach including patient selection,
choice of procedure, cytoreductive therapy, and the use of adjunctive radiotherapy.
In view of the five percent early mortality and the appreciable risk of late
myelodysplastic syndrome and/or acute myeloid leukemia associated with high dose
chemotherapy and transplantation, this approach should be considered as a
treatment of choice only in patients with a poor prognosis.
When multiple myeloma is suspected, the diagnosis must be carefully verified. For
example, patients who have 10 percent or more clonal plasma cells in the marrow
but no evidence of end organ damage that can be attributed to the plasma cell
disorder (smoldering multiple myeloma) do not require therapy because there is no
proof of clear benefit with currently available therapies, and some of these patients
remain stable without treatment over extended periods of time. (Per Rajkumar
(2013, UpToDate). AL amyloidosis can occur alone or in association with multiple
myeloma or, much less often, Waldenström’s macroglobulinemia or non-Hodgkin
lymphoma.
Per Kieran (2013, UpToDate) the initial treatment for patients with ependymoma
arising in the brain consists of maximal safe resection, which is usually followed by
adjuvant radiotherapy. Chemotherapy does not appear to play an important role in
the management of these tumors in adults and older children, but may in young
children or in patients with bulk residual disease. Until better molecular prognostic
markers are available, current therapeutic approaches continue to focus on the
degree of resection as the major determinant of treatment. Incompletely resected
ependymomas of either grade (II or III) require a short course of chemotherapy
Stem Cell Tandem Transplants Jun 17 10
followed by second-look surgery if there is residual signal, followed by conformal
radiation therapy. Ependymomas of either grade that achieve a complete resection
up-front should go directly to conformal radiation therapy. An exception to these
approaches should only occur in the context of approved prospective clinical trials.
Scientific Rationale – Update March 2012 Krishnan et al (2011) aimed to assess effectiveness of allogeneic HSCT with non-
myeloablative conditioning after autologous HSCT compared with tandem autologous
HSCT. In this phase 3 biological assignment trial, investigators enrolled patients
with multiple myeloma attending 37 transplant centers in the USA. Patients (<70
years old) with adequate organ function who had completed at least three cycles of
systemic antimyeloma therapy within the past 10 months were eligible for inclusion.
Investigators assigned patients to receive an autologous HSCT followed by an
allogeneic HSCT (auto-allo group) or tandem autologous HSCTs (auto-auto group)
on the basis of the availability of an HLA-matched sibling donor. Patients in the auto-
auto group subsequently underwent a random allocation (1:1) to maintenance
therapy (thalidomide plus dexamethasone) or observation. To avoid enrolment bias,
investigators classified patients as standard risk or high risk on the basis of
cytogenetics and β2-microglobulin concentrations. They used the Kaplan-Meier
method to estimate differences in 3-year progression-free survival (PFS; primary
endpoint) between patients with standard-risk disease in the auto-allo group and the
best results from the auto-auto group (maintenance, observation, or pooled). This
study is registered with ClinicalTrials.gov, number NCT00075829. Between Dec 17,
2003, and March 30, 2007, they enrolled 710 patients, of whom 625 had standard-
risk disease and received an autologous HSCT. 156 (83%) of 189 patients with
standard-risk disease in the auto-allo group and 366 (84%) of 436 in the auto-auto
group received a second transplant. 219 patients in the auto-auto group were
randomly assigned to observation and 217 to receive maintenance treatment, of
whom 168 (77%) completed this treatment. PFS and overall survival did not differ
between maintenance and observation groups and pooled data were used. Kaplan-
Meier estimates of 3-year PFS were 43% (95% CI 36-51) in the auto-allo group and
46% (42-51) in the auto-auto group (p=0·671); overall survival also did not differ at
3 years (77% [95% CI 72-84] vs 80% [77-84]; p=0·191). Within 3 years, 87 (46%)
of 189 patients in the auto-allo group had grade 3-5 adverse events as did 185
(42%) of 436 patients in the auto-auto group. The adverse events that differed most
between groups were hyperbilirubinaemia (21 [11%] patients in the auto-allo group
vs 14 [3%] in the auto-auto group) and peripheral neuropathy (11 [6%] in the auto-
allo group vs 52 [12%] in the auto-auto group). Investigators concluded non-
myeloablative allogeneic HSCT after autologous HSCT is not more effective than
tandem autologous HSCT for patients with standard-risk multiple myeloma. Further
enhancement of the graft versus myeloma effect and reduction in transplant-related
mortality are needed to improve the allogeneic HSCT approach.
Bashir et al (2011) investigated 149 patients with multiple myeloma (MM) who
received allogeneic hematopoietic stem cell transplantation (allo-HCT) with
myeloablative (MAC; n = 38) or reduced-intensity conditioning (RIC; n = 110)
regimens at a single center. Of the total, 120 (81%) patients had relapsed or had
refractory disease. Median age of MM patients was 50 (28-70) years with a followup
time of 28.5 (3-164) months. The 100-day and 5-year treatment related mortality
(TRM) rates were 17% and 47%, respectively. TRM was significantly lower with RIC
regimens (13%) vs. 29% for MAC at 100 days (P = 0.012). The cumulative
incidence of Grade II-IV acute graft-versus-host disease (GVHD) was 35% and
chronic GVHD was 46%. PFS and OS at 5 years were 15% and 21%, respectively. In

Stem Cell Tandem Transplants Jun 17 11
multivariate analysis, allo-HCT for primary remission consolidation was associated
with longer PFS (HR 0.35; 95% CI, 0.18-0.67) and OS (HR 0.29; 95% CI 0.15-
0.55), while absence of high-risk cytogenetics was associated with longer PFS only
(HR 0.59; 95% CI 0.37-0.95). We observe that TRM has decreased with the use of
RIC regimens, and long-term disease control can be expected in a subset of MM
patients undergoing allo-HCT. The investigators recommended further studies should
be conducted in carefully designed clinical trials in this patient population.
Khalafallah et al (2011) investigated the health-related quality of life (HR-QoL) in
patients with multiple myeloma (MM) undergoing tandem autologous stem cell
transplantation (TASCT). Eighteen patients with advanced MM who underwent dose-
modified TASCT were enrolled in this study between March 2006 and March 2008.
Patients <60 year old (10) received conditioning with melphalan 140 mg/m(2) and
patients who were ≥60 years (8) received 100 mg/m(2). The median age was 57.5
years (range 35-69). The investigators conducted the European Organization of
Research and Treatment of Cancer (EORTC) QLQ-C30 and the QLQ-MY24
questionnaires via interviews at presentation, after each ASCT and thereafter every
3 months for 24 months. Mean global health measure improved from 3.44 before
transplant to 4.50 (1=very poor, 7=excellent) at the second and subsequent follow-
up visits (P<0.001) and the mean global quality of life score improved from 3.61 to
4.71 (P<0.001). Pain symptoms were reduced (P=0.001), and physical functioning
improved (P<0.001) throughout the period of post-transplant follow-up. The
investigators concluded the study showed that dose-reduced TASCT is well tolerated
with low toxicity albeit the transient reduction in QoL during both transplants. Post-
transplant follow-up showed significant improvement in overall HR-QoL that reflects
positively on the overall disease-outcome. They noted a sole focus on patient-
survival does not adequately provide indication regarding the tolerability and
effectiveness of a proposed treatment on the patient's perceived quality of life and
the primary concern should be toward patient-welfare as well as survival.
Scientific Rational Update – December 2010 (2011) The National Cancer Comprehensive Network (NCCN) Myeloma Panel recommends
collecting enough stem cells for two transplants in all eligible patients. According to the
NCCN Multiple Myeloma Panel, a tandem transplant can be considered for all patients who
are candidates for stem cell transplant (SCT) and is an option for patients who do not
achieve at least a very good partial response (VGPR) after the first autologous SCT. The
benefit from the second transplant in patients who are in complete remission or VGPR and
also those who achieve less than VGPR after the first SCT, should be answered in a clinical
trial. A randomized perspective NIH and intergroup supported trial is currently ongoing. The
other option for this group of patients includes maintenance therapy or observation.
Planned tandem stem cell transplants (SCT) refer to a planned second course of high dose
therapy and SCT within 6 months of the first. Planned tandem stem cell transplants have
been studied in several randomized control trials. The IFM94 trial reported by Attal et al.
randomized newly diagnosed myeloma patients to single or tandem autologous transplants.
A total of 78% of patients assigned to the tandem transplant group received the 2nd
transplant at a median time of 2.5 months after the first. A variety of options for salvage
therapy were provided. For example, relapsing patients in either group received no
therapy, additional conventional therapy or another stem cell transplant. The probability of
surviving event free was 10% in the single transplant group, compared to 20% in the
double transplant group. The authors of the IFM94 trial have suggested that the
improvement in projected survival associated with tandem transplant is related not to
improved response rates but to longer durations of response.

Stem Cell Tandem Transplants Jun 17 12
Four other trials have compared single versus tandem transplant, but none have shown a
significant improvement in overall survival. However, since the median follow-up is 45-53
months, the lack of significant improvement is not surprising. The Cavo Trial found that
patients not in complete remission or near complete remission after the first transplant
benefited the most from a second transplant. This confirms the observations of the IFM94
trial using non-TBI based high dose regimens.
A review of long-term outcomes of several trials of autologous transplantation by Barlogie et
al. (2010) found that tandem transplantations were superior to both single transplants and
standard therapies. Also, post relapse survival was longer when event-free survival was
sustained for at least 3.5 years after tandem transplantation.
The 2010 NCCN guidelines for the treatment of testicular cancer state that if a patient with
favorable prognostic factors (defined as testicular primary site, prior complete response to
first line therapy, low levels of serum markers and low volume disease), experiences an
incomplete response to conventional-dose salvage chemotherapy therapy or relapses after
salvage chemotherapy, high-dose chemotherapy with autologous stem cell support is the
preferred option. Patients with unfavorable prognostic factors for conventional-dose salvage
therapy (e.g. an incomplete response to first line therapy) and patients requiring third-line
salvage therapy are considered for treatment with high-dose chemotherapy plus autologous
stem cell support (category 2B). The 2010 guidelines do not address the use of tandem or
sequential hematopoietic stem cell transplantation (HSCT) in the treatment of testicular
tumors.
Testicular cancer is a unique malignancy in its curability. Long-term followup of patients
treated with chemotherapy suggests that the long-term relapse-free survival for complete
responders is in the range of 80% to 90%. Nonetheless, once a complete remission is
obtained, patients remain at risk for two types of adverse late consequences: relapse,
including contralateral primary testicular neoplasms, and toxicity from therapy.
After obtaining complete remission, 8% to 15% of germ cell tumor (GCT) patients will
relapse, usually within the first 2 years after treatment. The timing of a relapse does not
seem to be dependent on histology, extent of disease, or induction regimen used. Late
recurrences, defined as relapses occurring more than 24 months after diagnosis, have been
reported in 1.5% to 4% of patients achieving a complete response. The majority of late
relapses occur longer than 5 years from diagnosis. Nearly 50% of relapses were
retroperitoneal and 35% intrathoracic (including the mediastinum). Proposed mechanisms
for late relapses include the development of second primary lesions, growth of an occult
contralateral testicle tumor that is not affected by chemotherapy because of the blood-
testicular barrier, the “reactivation” of quiescent carcinoma, or malignant degeneration of
mature teratoma. The latter argument is the most favored, in that teratomatous elements
are observed in either the orchiectomy or relapse specimens in most patients. Teratomatous
elements were present in the orchiectomy specimens of 66% of 21 nonseminomatous germ
cell transplant (NSGCT) patients with a late relapse reported in three series. Nonetheless,
this theory does not account for the 33% of late-relapse NSGCT patients who did not have
teratoma described in their orchiectomy specimen (perhaps a microscopic focus was
missed), or the seven pure seminoma patients in these series who experienced a late
relapse.
A late relapse should be treated aggressively as a de novo malignancy. Outcomes in this
setting are a reflection of the underlying histology at the time of relapse. Patients with
teratoma who are treated surgically have excellent long-term outcomes, whereas the

Stem Cell Tandem Transplants Jun 17 13
complete-response rates to chemotherapy alone for those who relapse with viable GCT are
approximately 50%, and the median survival in this setting is approximately 24 months
according to one recent series. Approximately 70% of seminoma patients can be rendered
free of disease with chemotherapy, radiation, or both. Whereas 80% of patients with NSGCT
can currently be cured with platinum-based therapy, 20% will ultimately die of their disease
because of either failure to achieve a complete response with induction therapy or relapse
after becoming disease-free with primary therapy. Before the initiation of salvage therapy,
the diagnosis of relapsed or primarily refractory GCT must be clearly established.
Scientific Rationale Initial Despite treatment with high-dose chemotherapy followed by stem cell transplant,
many patients with advanced malignancies eventually relapse, indicating the
presence of residual neoplastic cells. Tandem high-dose or non-myeloablative
chemotherapy with autologous and/or allogeneic stem cell support is the planned
administration of more than one cycle of high-dose chemotherapy, alone or with
total body irradiation, each of which is followed by re-infusion of stem cells. In the
former the patient is given his own stem cells in an autologous transplantation, and
in the later the patient is given stem cells donated from a matched sibling as an
allogeneic stem cell rescue after a recuperation period of about two to 6 months. The
hypothesis is that eradication of residual tumor cells can be achieved using multiple
cycles of myeloablative or non-myeloablative chemotherapy with stem cell support.
Sibling allogeneic transplants have several potential advantages relative to
autologous transplants, including no chance that the transplant will reinfuse
malignant cells and the possibility that donor cells may mediate immunologic
antitumor effects. The tandem transplant achieves remission rates similar to those
with a high-dose allogeneic transplant but with much lower morbidity and mortality.
Testicular Cancer
Testicular cancer forms in tissues of the testis that make sperm and male hormones
and usually occurs in young- or middle-aged men. Two main types of testicular
cancer are seminomas (cancers that grow slowly and are more sensitive to radiation
therapy) and nonseminomatous germ cell tumors (NSGCTs) (different cell types that
grow more quickly than seminomas). Although the exact cause of testicular cancer is
unknown, several factors seem to increase risk. These include a past medical history
of undescended testicle(s), abnormal testicular development, Klinefelter's syndrome
(a sex chromosome disorder that may be characterized by low levels of male
hormones, sterility, development of breasts, and small testes), or previous testicular
cancer. Between 6,000 and 8,000 men are diagnosed with testicular cancers each
year. Although testicular cancer accounts for 1% of all cancers in men, it is the most
common form of cancer in young men 15 to 40 years old. It may also occur in young
boys, but only about 3% of all testicular cancer is found in this group. Seminomas
account for about 30-40% of all testicular tumors. These are usually is found in men
in their 30s and 40s. The condition is usually localized to the testes, although in
about 25% of cases it has spread to lymph nodes. Non-seminomas account for 60%
of all testicular tumors.
Testicular cancer is a highly treatable, often curable, cancer that usually develops in
young and middle-aged men. For patients with seminoma (all stages combined), the
cure rate exceeds 90%. For patients with low-stage disease, the cure rate
approaches 100%. Tumors that have a mixture of seminoma and nonseminoma
components should be managed as nonseminomas. Nonseminomas include
embryonal carcinomas, teratomas, yolk sac carcinomas and choriocarcinomas, and
Stem Cell Tandem Transplants Jun 17 14
various combinations of these cell types. Risk of metastases is lowest for teratoma
and highest for choriocarcinoma, with the other cell types being intermediate.
Tumors that appear to have a seminoma histology but that have elevated serum
levels of alpha fetoprotein (AFP) should be treated as nonseminomas. Elevation of
the beta subunit of human chorionic gonadotropin (hCG) alone is found in
approximately 10% of the patients with pure seminoma.
A number of prognostic classification schema are in use for metastatic nonsemino-
matous testicular cancer and for primary extragonadal nonseminomatous germ cell
cancers treated with chemotherapy. Most incorporate some or all of the following
factors, which may independently predict worse prognosis:
Presence of liver, bone, or brain metastases.
Very high serum markers.
Primary mediastinal nonseminoma.
Large number of lung metastases.
Even patients with widespread metastases at presentation, including those
with brain metastases, may still be curable and should be treated with this
intent.
Radical inguinal orchiectomy with initial high ligation of the spermatic cord is the
procedure of choice in treating a malignant testicular mass. Evaluation of the
retroperitoneal lymph nodes usually by CT scanning is an important aspect of
treatment planning in adults with testicular cancer. An important aspect of the
diagnosis and follow-up of testicular cancer is the use of serum markers. Serum
markers include AFP, hCG (measurement of the beta subunit reduces luteinizing
hormone cross-reactivity), and lactate dehydrogenase. The serum markers may
detect a tumor that is too small to be detected on physical examination or x-rays.
Serum markers plus chest x-rays are important parts of the monthly checkups for
patients after definitive therapy of testicular cancer as well as periodic abdominal
computed tomographic (CT) scans for 2 to 3 years. The absence of markers does not
mean the absence of tumor. Patients typically receive follow-up monthly for the first
year and every other month for the second year after diagnosis and treatment.
While the majority of tumor recurrences appear within 2 years, late relapse has been
reported, and lifelong marker, radiologic, and physical examination is recommended.
Since the majority of testis cancer patients who receive chemotherapy are curable, it
is important to be aware of possible long-term effects of platinum-based treatment
such as cisplatin, bleomycin, and etoposide, some of which may be very serious
(e.g., infertility, secondary leukemias, bilateral hearing deficits, etc.). Bleomycin is
known for its pulmonary toxic effects may, but it is rarely fatal at the total
cumulative doses used and are reversible after the completion of chemotherapy.
In contrast to the excellent outcomes for men with good risk advanced testicular
tumors, up to 50% of men who have features of intermediate or poor risk disease
will require salvage therapy for relapsed disease following first-line chemotherapy.
Once relapse after cisplatin-containing therapy is diagnosed, the optimal treatment
for men depends upon the initial treatment and response to prior therapy, the
location and timing of the relapse, the stage of the tumor, the extent of the disease
and tumor histology. Most patients can still be cured. A single autologous stem cell
transplantation to treat testicular tumors in patients that do not achieve a complete
remission or in patients in second complete remission or in second relapse has
become standard of care. Planned tandem high-dose chemotherapy regimens with
Stem Cell Tandem Transplants Jun 17 15
autologous stem cell transplant followed by allogeneic stem cell donation of a
matched family member has also been accepted treatment despite the level of
evidence supporting its use rises to include multiple case series.
Ayash et al (2001) reported their results of double dose-intensive chemotherapy
with autologous stem cell support for relapsed and refractory testicular cancer and
reviewed the literature. They concluded that patients with relapsed/ refractory
testicular cancer benefit most from ABMT if they have platinum-sensitive disease in
first relapse. Patients, who do poorly despite ABMT have a mediastinal primary site,
true cisplatin-refractory disease, disease progression prior to ABMT, and/or markedly
elevated betaHCG at ABMT.
Multiple Myeloma Multiple myeloma is a hematological malignancy composed of an expanding clone of
plasma cells within the bone marrow. Multiple myeloma is a classic example of a
monoclonal proliferation of tumor cells: in 90% of cases the disease is characterized
by the plasma cell production of a monoclonal immunoglobulin, often referred to as a
M-component, which can be quantified in the serum or urine. The expansion of the
malignant clone of cells in the bone marrow with associated destruction of bone, and
the production of the M-component lead to the classic signs/symptoms of MM: lytic
bone lesions with painful fractures, hypercalcemia, anemia, amyloidosis, renal failure
as well as infections associated with immunodeficiency. Approximately 50% of
patients are older than 65 years of age at diagnosis.
Multiple myeloma is highly treatable but rarely curable. The disease is staged by
estimating the myeloma tumor cell mass on the basis of the amount of monoclonal
(or myeloma) protein (M protein) in the serum and/or urine, along with various
clinical parameters, such as the hemoglobin and serum calcium concentrations, the
number of lytic bone lesions, and the presence or absence of renal failure. The stage
of the disease at presentation is a strong determinant of survival, but it has little
influence on the choice of therapy since almost all patients, except for rare patients
with solitary bone tumors or extramedullary plasmacytomas, have generalized
disease. Treatment selection is influenced by the age and general health of the
patient, prior therapy, and the presence of complications of the disease.
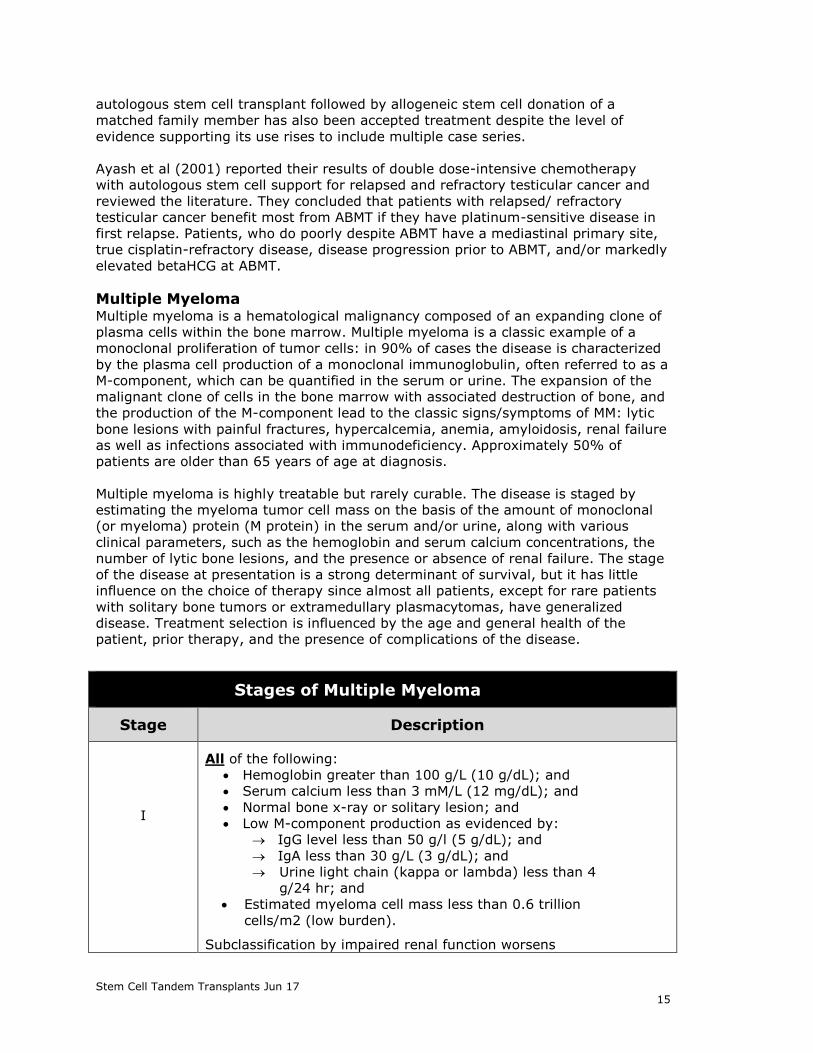
Stages of Multiple Myeloma
Stage Description
I
All of the following:
Hemoglobin greater than 100 g/L (10 g/dL); and
Serum calcium less than 3 mM/L (12 mg/dL); and
Normal bone x-ray or solitary lesion; and
Low M-component production as evidenced by:
IgG level less than 50 g/l (5 g/dL); and
IgA less than 30 g/L (3 g/dL); and
Urine light chain (kappa or lambda) less than 4
g/24 hr; and
Estimated myeloma cell mass less than 0.6 trillion
cells/m2 (low burden).
Subclassification by impaired renal function worsens

Stem Cell Tandem Transplants Jun 17 16
prognosis regardless of stage:
Creatinine less than 2.0 mg/dL.
Creatinine greater than or equal to 2.0 mg/dL.
II
Fitting neither Stage I nor Stage III (Overall data not
as minimally abnormal as shown for Stage I and no
single value abnormal as defined for Stage III); and
Estimated myeloma cell mass 0.6 to 1.2 trillion cells/m2
(intermediate burden).
III
One or more of the following:
Hemoglobin less than 85 g/L (8.5 g/dL)
Serum calcium greater than 3 mM/L (12 mg/dL)
Advanced lytic bone lesions
High M-component production as shown by:
IgG greater than 70 g/L (7 g/dL)
IgA greater than 50 g/L (5 g/dL)
Urine light chain (kappa or lambda) greater than
12 g/24 hours
Estimated myeloma cell mass greater than 1.2 trillion
cells/m2 (high burden).
Systemic antineoplastic therapy is the initial approach to treatment for patients with
signs and symptoms of progressive disease. For the past two decades, the
combination of melphalan and prednisone has been the standard therapy for MM. For
patients who have proven to be resistant to this therapy, a combination of
vincristine, adriamycin with dexamethasone (VAD) has been implemented. The
literature indicates that multi-drug combinations have failed to substantially improve
the results originally obtained with standard melphalan and prednisone.
Approximately 40 to 50% respond initially (using 50% tumor reduction criteria),
although the incidence of true complete remission is rare, probably lower then 10%.
The median survival does not exceed 3 years. About 5% of patients, mainly those
presenting with low tumor mass and responding to initial therapy, survive 10 and 15
years, but eventually succumb to their disease.
High dose chemotherapy (HDC) followed by stem cell transplant (preferably
autologous) has been shown to be a treatment of choice for select patients with MM.
This is done in an attempt to obtain greater and more extended response rates by
permitting the use of chemotherapeutic agents at doses that exceed the myelo-
toxicity threshold; consequently, a greater tumor cell kill might be anticipated. Total
body irradiation (TBI) is an additional variable. A variety of regimens have been
developed for MM, which primarily involve the use of different alkylating agents.
Patients with the disease who are responsive to standard doses of chemotherapy,
and are either asymptomatic or have a good performance status and who do not
have any serious co-morbidities are considered optimal candidates for HDC.
It has been suggested that better results might be obtained with tandem (double or
sequential) autologous hematopoietic cell transplants. One such regimen consists of
melphalan for the first transplant and either the same dose or melphalan plus total
body irradiation for the second transplant, depending upon the response status prior
to the second transplant, which was usually performed within six months. In a
recent review on the treatment strategies for MM, Gisslinger and Kees (2003) stated,

Stem Cell Tandem Transplants Jun 17 17
“the use of tandem transplantation, developed to further escalate the conditioning
dose, has achieved additional improvement in survival”.
In a randomized study, Attal et al (2003) evaluated treatment of MM with HDC
followed by either one or two successive ASCT. A total of 399 previously untreated
patients under the age of 60 years were randomly assigned to receive a single, or
double transplant. A complete or a very good partial response was achieved by 42%
of patients in the single-transplant group and 50% of patients in the double-
transplant group (p = 0.10). The probability of surviving event-free for 7 years after
the diagnosis was 10% in the single-transplant group and 20% in the double-
transplant group (p = 0.03). The estimated overall 7-year survival rate was 21% in
the single-transplant group and 42% in the double-transplant group (p = 0.01).
Among patients who did not have a very good partial response within 3 months after
one transplantation, the probability of surviving 7 years was 11% in the single-
transplant group and 43% in the double-transplant group (p < 0.001). The authors
concluded that as compared with a single ASCT after HDC, double transplantation
improves overall survival among patients with MM, especially those who do not have
a very good partial response after undergoing one transplantation.
Stadtmauer et al (2003) conducted a randomized trial of 399 previously untreated
patients < 60 years of age from France found significantly improved seven-year
event-free survival (20 versus 10%) and overall survival (42 versus 21%) in
recipients of double versus single autologous transplant. Factors predicting for longer
survival in this study included low levels of beta-2-microglobulin and lactate
dehydrogenase at diagnosis, and younger age. The beneficial effect of the second
transplant on overall survival differed according to the response to the first
transplant. Patients who achieved a complete response (CR) or very good partial
response (VGPR) with the first transplant did not benefit significantly from the
second transplant. On the other hand, patients who did not have at least a VGPR to
the first transplant had a significant benefit from the second; seven year rates of
overall survival for this group were 11 versus 43% for those in the single or double
transplantation groups, respectively. The authors stated, as did the accompanying
editorial, that one reason the patients in the double transplant group might have
done better was that they received a higher overall dose of melphalan. There was
the suggestion that had the patients received 200 mg of melphalan for the first
transplant (without total body irradiation [TBI]), instead of the 140 mg/m2 dose with
TBI, they might not have needed the second transplant, putting these results into
some question. Results of other randomized trials are pending. However, as stated
earlier and based on the results discussed above, it is reasonable to consider a
second (tandem) HCT in patients failing to achieve CR or VGPR with the first
transplant.
An alternative to tandem transplant is to perform an initial autologous transplant
with one-half of the collected stem cells, and to perform a second autologous
transplant with the remaining cells after relapse. One early study suggests that this
strategy produces results equivalent to those reported with tandem transplantation.
However, results of a European registry retrospective analysis suggested that best
results were obtained when the second transplant was performed before relapse and
within 6 to 12 months of the first transplant. Since patients achieving CR or VGPR
with the first HCT do not appear to benefit from a tandem HCT approach, the second
transplant in this population can be reserved for relapsed disease.

Stem Cell Tandem Transplants Jun 17 18
Few patients are considered eligible for a second autologous stem cell transplant to
treat myeloma that has relapsed after a complete or partial remission that followed
an initial autotransplant. Thus, it is unlikely that prospective trials will ever be
conducted to rigorously compare outcomes of this strategy with alternatives.
Nevertheless, retrospective studies report durable complete or partial responses and
extended survival for patients treated this way, particularly when a long disease- or
progression-free interval followed the first transplant. Several peer reviewed
published case series report complete response rates after allogeneic transplant in
patients with myeloma range from 22% to 67%. A number of observations suggest
that graft-vs-myeloma effects occur following allogeneic transplantation, including
the identification of myeloma-specific cytotoxic T cells in transplant recipients and
clinical responses to donor lymphocyte infusions.
A study published by Maloney (2003) included 54 patients with previously treated
myeloma (52% refractory or relapsed disease) given an initial autologous stem cell
transplant conditioned with 200 mg/m2 melphalan. Of these, 52 received a
subsequent mini-allogeneic stem cell transplant. Investigators reported 78% overall
survival (OS) at a median 552 days after allografting. Treatment achieved a
complete remission (CR) in 57% and an overall response rate of 83%. Acute graft-
versus host-disease (GVHD) developed in 38% of patients, and chronic GVHD
requiring therapy in 46%. Twelve patients died: 1 from viral infection after the initial
autotransplant, 2 from myeloma progression (3 and 23 months post-mini-
allotransplant), 7 from GVHD, and 1 each from lung cancer and encephalopathy.
Multiple myeloma also includes indolent myeloma, smoldering myeloma and MGUS.
With conventional-dose chemotherapy, patients with MM have a median survival of
about 3 years, while the disease course of indolent and smoldering myeloma and
MGUS is more uncertain. Therefore, the distinction between these entities is
important because HDC is clearly indicated only in cases of symptomatic MM.
Review History March 2007 Medical Advisory Council initial approval
December 2010 Update. Added Medicare table with link to NCD. No revisions.
March 2012 Update - no revisions. Code updates.
March 2013 Update – no revisions. Code updates.
May 2013 Added that tandem transplant can be considered as an option for multiple
myeloma patients who do not achieve at least a very good partial
response (VGPR) after the first autologous SCT. (NCCN Multiple Myeloma
2013)
May 2014 Update – Clarified policy statement noting that tandem SCT can be done
with autologous stem cells as recommended by NCCN guidelines.
May 2015 Update – no revisions
May 2016 Update – no revisions. Codes updated.
June 2017 Update- no revisions
This policy is based on the following evidence-based guidelines: 1. Imrie K; Esmail R; Meyer RM. The role of high-dose chemotherapy and stem-cell
transplantation in patients with multiple myeloma: a practice guideline of the
Cancer Care Ontario Practice Guidelines Initiative. Ann Intern Med. 2002;
136(8):619-629.
2. American Society for Blood and Bone Marrow Transplantation. Policy
Statements, Guidelines and Reviews.

Stem Cell Tandem Transplants Jun 17 19
3. Myeloma Management Guidelines. A Consensus Report From The Scientific
Advisors Of The International Myeloma Foundation. Available at:
http://www.myeloma.org/pdfs/MyelomaManagementGuidelines.pdf
4. Anderson KC, Alsina M, Bensinger W, et al; National Comprehensive Cancer
Network (NCCN). Multiple myeloma. Clinical practice guidelines in oncology. J
Natl Compr Canc Netw. 2009; 7 (9): 908-942.
5. National Cancer Comprehensive Network (NCCN) Clinical Practical Guidelines in
Oncology. Testicular Cancer. V.2.2010. Update Version 1.2012. Update 1.2014.
Update 1.2015. Updated Version 2.2016.
6. National Cancer Comprehensive Network (NCCN) Clinical Practical Guidelines in
Oncology. Multiple Myeloma, Version 1.2011. Update Version 1.2013. Update
version 2.2014. Update Version 4.2015. Update Version 3.2016. 7. Imrie K, Rumble RB, Crump M, Advisory Panel on Bone Marrow and Stem Cell
Transplantation, Hematology Disease Site Group. Stem cell transplantation in
adults: recommendations. Toronto (ON): Cancer Care Ontario Program in
Evidence-based Care; 2009 Jan 30. 78 p. Available at:
https://www.cancercare.on.ca/common/pages/UserFile.aspx?serverId=6&path=
/File%20Database/CCO%20Files/PEBC/pebc_stemcell.pdf
References – Update May 2016 1. Palumbo A, Cavallo F, F, et al. Autologous Transplantation and Maintenance Therapy in
Multiple Myeloma. NEJM. 2014;371:895-905.
References – Update May 2015 1. Byrne M, Salmasinia D, Leather H, et al. Tandem Autologous Stem Cell Transplantation
for Multiple Myeloma Patients Based on Response to Their First Transplant-A
Prospective Phase II Study. Clin Med Insights Oncol. 2014 Sep 3;8:101-5
2. Iacobelli S, de Wreede LC, Schönland S, et al. Impact of CR before and after allogeneic
and autologous transplantation in multiple myeloma: results from the EBMT NMAM2000
prospective trial. Bone Marrow Transplant. 2015 Apr;50(4):505-10.
3. Tamura H. Single vs double stem cell transplantation for the treatment of multiple
myeloma. Nihon Rinsho. 2015 Jan;73(1):85-9.
References – Update May 2014 1. Agarwala AK, Perkins SM, Abonour R, et al. Salvage chemotherapy with high-dose
carboplatin and etoposide with peripheral blood stem cell transplant in patients with
relapsed pure seminoma. Am J Clin Oncol. 2011 Jun;34(3):286-8.
2. Armeson KE, Hill EG, Costa LJ. Tandem autologous vs autologous plus reduced
intensity allogeneic transplantation in the upfront management of multiple myeloma:
meta-analysis of trials with biological assignment. Bone Marrow Transplant. 2013
Apr;48(4):562-7.
3. Brito M, Sanchez P, Velho S, et al. High dose chemotherapy with autologous stem-cell
support in germ cell tumors: The Instituto Português de Oncologia de Lisboa Francisco
Gentil Series. Acta Med Port. 2011 Jul-Aug;24(4):533-44.
4. Connolly RM, McCaffrey JA. High-dose chemotherapy plus stem cell transplantation in
advanced germ cell cancer: a review. Eur Urol. 2009 Jul;56(1):57-64.
5. Einhorn LH, Williams SD, Chamness A, et al. High-dose chemotherapy and stem-cell
rescue for metastatic germ-cell tumors. N Engl J Med. 2007 Jul 26;357(4):340-8.
6. Gahrton G, Iacobelli S, Björkstrand B, et al. Autologous/reduced-intensity allogeneic
stem cell transplantation vs autologous transplantation in multiple myeloma: long-term
results of the EBMT-NMAM2000 study. Blood. 2013 Jun 20;121(25):5055-63.

Stem Cell Tandem Transplants Jun 17 20
7. Gohji K, Hara I, Yamada Y, et al. Clinical results of super high-dose chemotherapy with
peripheral blood stem cell transplantation for patients with advanced germ cell tumor.
Hinyokika Kiyo. 1999 Nov;45(11):799-804.
8. Hara I, Yamada Y, Kumano M, et al. High dose chemotherapy including paclitaxel (T-
ICE) combined with peripheral blood stem cell transplantation for male germ cell tumor.
Preliminary report. Int J Urol. 2005 Dec;12(12):1074-8.
9. Kharfan-Dabaja MA, Hamadani M, Reljic T, et al. Comparative efficacy of tandem
autologous versus autologous followed by allogeneic hematopoietic cell transplantation
in patients with newly diagnosed multiple myeloma: a systematic review and meta-
analysis of randomized controlled trials. J Hematol Oncol. 2013 Jan 4;6:2.
10. Koychev D, Oechsle K, Bokemeyer C, Honecker F. Treatment of patients with relapsed
and/or cisplatin-refractory metastatic germ cell tumours: an update. Int J Androl. 2011
Aug;34(4 Pt 2):e266-73.
11. Kozelj M, Zver S, Zadnik V. Long term follow-up report of cardiac toxicity in patients
with multiple myeloma treated with tandem autologous hematopoietic stem cell
transplantation. Radiol Oncol. 2013 May 21;47(2):161-5.
12. Ladicka M, Ballova V, Drgona L, et al. Tandem autologous stem cell transplantation in
multiple myeloma after high-dose chemotherapy with two separate collections: single
institution experience. Neoplasma. 2012;59(5):551-8.
13. Lazarus HM, Stiff PJ, Carreras J, et al. Utility of single versus tandem autotransplants
for advanced testes/germ cell cancer: a center for international blood and marrow
transplant research (CIBMTR) analysis. Biol Blood Marrow Transplant. 2007
Jul;13(7):778-89.
14. Marjanović S, Cerović S, Brajusković G. Use of high-dosage chemotherapy with
autologous hematopoietic stem cell transplantation as a first-line therapy for the
patients with poor-prognosis testicular tumors. Vojnosanit Pregl. 2005 Mar;62(3):213-
8.
15. Michallet M, Sobh M, El-Cheikh J, et al. Evolving strategies with immunomodulating
drugs and tandem autologous/allogeneic hematopoietic stem cell transplantation in first
line high risk multiple myeloma patients. Exp Hematol. 2013 Dec;41(12):1008-15.
16. Miki T, Mizutani Y, Akaza H, et al. Long-term results of first-line sequential high-dose
carboplatin, etoposide and ifosfamide chemotherapy with peripheral blood stem cell
support for patients with advanced testicular germ cell tumor. Int J Urol. 2007
Jan;14(1):54-9.
17. Miyazaki J, Miyanaga N, Kawai K, et al. High-dose chemotherapy with peripheral blood
stem cell transplantation for advanced testicular cancer. Int J Urol. 2000 Jul;7(7):258-
62.
18. Naumann-Winter F, Greb A, Borchmann P, et al. First-line tandem high-dose
chemotherapy and autologous stem cell transplantation versus single high-dose
chemotherapy and autologous stem cell transplantation in multiple myeloma, a
systematic review of controlled studies. Cochrane Database Syst Rev. 2012 Oct
17;10:CD004626
19. Rosiñol L, Kumar S, Moreau P, Cavo M. Initial treatment of transplant-eligible patients
in multiple myeloma. Expert Rev Hematol. 2014 Feb;7(1):43-53.
References – Update May 2013 1. Bergantim R, Trigo F, Guimarães JE. Impact of tandem autologous stem cell
transplantation and response to transplant in the outcome of multiple myeloma. B Exp
Hematol Oncol. 2012; 1: 35. 2012 November 26. doi: 10.1186/2162-3619-1-
35PMCID: PMC3547750.
2. Delgado JC. Diagnosis of Monoclonal Gammopathies. ARUP Laboratories. Available at:
http://www.arup.utah.edu/media/gammopathies/2011%20Jan%20-
%20Monoclonal%20Gammopathies.pdf

Stem Cell Tandem Transplants Jun 17 21
3. Lakshminarayanan R, Li Y, Janatpour K, et al. Detection by Immunofixation of M
Proteins in Hypogammaglobulinemic Patients With Normal Serum Protein
Electrophoresis Results. Immunopathology/ M Proteins Hypogammaglobulinemic
Patients. American Society for Clinical Pathology. 2007;127:746-751.
4. O’Connell TX, Horita TJ, Kasravi B. Understanding and Interpreting Serum Protein
Electrophoresis. m Fam Physician. 2005 Jan 1;71(1):105-112.
References – Update March 2013 1. Bjorkstrand B, Iacobelli S, Hegenbart U, et al. Tandem autologous/reduced-intensity
conditioning allogeneic stem-cell transplantation versus autologous transplantation in
myeloma: Long-term follow-up. J Clin Oncol. 2011;29 (22):3016-3022.
2. Canellos GP, Mauch PM. Hematopoietic cell transplantation in classical Hodgkin
lymphoma. UpToDate. April 19, 2012.
3. Harmon DC, Gebhardt MC. Treatment of the Ewing sarcoma family of tumors.
UpToDate. December 11, 2012.
4. Kieran MW. Ependymoma. UpToDate February 12, 2013.
5. Rajkumar SV. Clinical presentation, laboratory manifestations, and diagnosis of
immunoglobulin light chain (AL) amyloidosis (primary amyloidosis). UpToDate.
November 27, 2012.
6. Rajkumar SV. Treatment and prognosis of Waldenström macroglobulinemia. UpToDate.
February 22, 2013.
7. Sureda A, Canals C, Arranz R, et al. Allogeneic stem cell transplantation after reduced
intensity conditioning in patients with relapsed or refractory Hodgkin's lymphoma.
Results of the HDR-ALLO study - a prospective clinical trial by the Grupo Español de
Linfomas/Trasplante de Médula Osea (GEL/TAMO) and the Lymphoma Working Party of
the European Group for Blood and Marrow Transplantation. Haematologica. 2012
Feb;97(2):310-7. Epub 2011 Oct 11.
References – Update March 2012 1. Bashir Q, Khan H, Orlowski RZ, et al. Predictors of prolonged survival after allogeneic
hematopoietic stem cell transplantation for multiple myeloma. Am J Hematol. 2011 Dec
17. doi: 10.1002/ajh.22273.
2. Khalafallah A, McDonnell K, Dawar HU, et al. Quality of life assessment in multiple
myeloma patients undergoing dose-reduced tandem autologous stem cell
transplantation. Mediterr J Hematol Infect Dis. 2011;3(1):e2011057
3. Krishnan A, Pasquini MC, Logan B, et al. Autologous haemopoietic stem-cell
transplantation followed by allogeneic or autologous haemopoietic stem-cell
transplantation in patients with multiple myeloma (BMT CTN 0102): a phase 3 biological
assignment trial. Lancet Oncol. 2011 Dec;12(13):1195-203
4. Matsui W, Borrello I, Mitsiades C. Autologous stem cell transplantation and multiple
myeloma cancer stem cells. Biol Blood Marrow Transplant. 2012 Jan;18(1 Suppl):S27-
32.
5. Rigacci L, Puccini B, Dodero A, et al. Allogeneic hematopoietic stem cell transplantation
in patients with diffuse large B cell lymphoma relapsed after autologous stem cell
transplantation: A GITMO study. Ann Hematol. 2012 Jan 14
References Update - December 2010 1. CMS. Centers for Medicare & Medicaid. NCD for Stem Cell Transplantation (110.8.1).
Implementation Date 11/10/2010.

Stem Cell Tandem Transplants Jun 17 22
2. Barlogie B, Attal M, Crowley J, et al. Long term follow up on auto-transplantation trials
for multiple myeloma; update of protocols. Journal of Clinical Oncology; 2010 28: 1209-
1214.
3. Kumar A, Kharfan-Dabaja MA, Glasmacher A, et al. Tandem versus single autologous
hematopoietic cell transplantation for the treatment of multiple myeloma: A systematic
review and meta-analysis. J Natl Cancer Inst. 2009;101 (2):100-106.
4. Agarwal R, Dvorak CC, Stockerl-Goldstein KE, et al. High-dose chemotherapy followed
by stem cell rescue for high-risk germ cell tumors: the Stanford experience. Bone
Marrow Transplant. 2009 Apr;43(7):547-52.
5. Ryan CJ, Small EJ, Torti FM. Abeloff: Abeloff's Clinical Oncology, 4th ed. Chapter 90
Testicular Cancer. 2008.
6. Lazarus HM, Stiff PJ, Carreras J, et al. Utility of single versus tandem autotransplants
for advanced testes/germ cell cancer: a center for international blood and marrow
transplant research (CIBMTR) analysis. Biol Blood Marrow Transplant. 2007 Jul;13
(7):778-89.
7. Lorch A, Kollmannsberger C, Hartmann JT, et al. Single versus sequential high-dose
chemotherapy in patients with relapsed or refractory germ cell tumors: a prospective
randomized multicenter trial of the German Testicular Cancer Study Group. J Clin Oncol.
2007 Jul 1;25 (19):2778-84.
References Initial 1. Elice, F, Raimondi, R, Tosetto, A, et al. Prolonged overall survival with second
on-demand autologous transplant in multiple myeloma. Am J Hematol 2006;
81:426.
2. Kopp HG, Kuczyk M, Classen J, et al. Advances in the treatment of testicular
cancer. Drugs. 2006;66(5):641-59.
3. Barlogie, B, Tricot, G, Anaissie, E, et al. Thalidomide and hematopoietic-cell
transplantation for multiple myeloma. N Engl J Med 2006; 354:1021.
4. Barlogie, B, Tricot, G, Rasmussen, E, et al. Total therapy 2 without thalidomide
in comparison with total therapy 1: role of intensified induction and
posttransplantation consolidation therapies. Blood 2006; 107:2633.
5. Margolin KA, Doroshow JH, Frankel P, et al. Paclitaxel-based high dose
chemotherapy with autologous stem cell rescue for germ cell cancer. Biol Blood
Marrow Transplant. 2005 Nov;11(11):903-11.
6. Morris, C, Iacobelli, S, Brand, R, et al. Benefit and timing of second
transplantations in multiple myeloma: clinical findings and methodological
limitations in a European group for blood and marrow transplantation registry
study. J Clin Oncol 2004; 22:1674.
7. Lahuerta, JJ, Grande, C, Martinez-Lopez, J, De La, Serna J. Tandem transplants
with different high-dose regimens improve the complete remission rates in
multiple myeloma. Results of a Grupo Espanol de Sindromes
Linfoproliferativos/Trasplante Autologo de Medula Osea phase II trial. Br J
Haematol 2003; 120:296.
8. Fassas, AB, Barlogie, B, Ward, S, et al. Survival after relapse following tandem
autotransplants in multiple myeloma patients: The University of Arkansas total
therapy I experience. Br J Haematol 2003; 123:484.
9. Barlogie, B, Tricot, GJ, van Rhee, F, et al. Long-term outcome results of the first
tandem autotransplant trial for multiple myeloma. Br J Haematol 2006;
135:158.
10. Jacobson, J, Barlogie, B, Shaughnessy, J, Drach, J. MDS-type abnormalities
within myeloma signature karyotype (MM-MDS): only 13% 1-year survival
despite tandem transplants. Br J Haematol 2003; 122:430.

Stem Cell Tandem Transplants Jun 17 23
11. Attal, M, Harousseau JL, Facon T, et al. Single versus double autologous stem-
cell transplantation for multiple myeloma. NEJM. 2003;349:2495-2502.
12. de Giorgi U, Papiani G, Severini G, et al. High-dose chemotherapy in adult
patients with germ cell tumors. Cancer Control. 2003;10(1):48-56.
13. Tricot, G, Spencer, T, Sawyer, J, et al. Predicting long-term (5 years) event-free
survival in multiple myeloma patients following planned tandem autotransplants.
Br J Haematol 2002; 116:211.
14. Einhorn LH. Curing metastatic testicular cancer. Proc Natl Acad Sci U S A. 2002
Apr 2;99(7):4592-5.
15. Anagnostopoulos A, Giralt S. Critical review on non-myeloablative stem cell
transplantation (NST). Crit Rev Oncol Hematol. 2002;44(2):175-190.
16. Barbui AM, Galli M, Dotti G, et al. Negative selection of peripheral blood stem
cells to support a tandem autologous transplantation programme in multiple
myeloma. Br J Haematol. 2002; 116(1):202-210.
17. Child JA, Morgan GJ, Gilson D, et al. High-dose chemotherapy with
hematopoietic stem-cell rescue for multiple myeloma. NEJM. 2003;
348(19):1875-1883.
18. Kröger N, Schwerdtfeger R, Kiehl M, et al. Autologous stem cell transplantation
followed by a dose-reduced allograft induces high complete remission rate in
multiple myeloma. Blood. 2002; 100(3):755-760.
19. Dalton WS, Bergsagel PL, Kuehl WM, et al. Multiple myeloma. Hematology (Am
Soc Hematol Educ Program). 2001;157-177.
20. Ayash LJ, Clarke M, Silver SM, et al. Double dose-intensive chemotherapy with
autologous stem cell support for relapsed and refractory testicular cancer: the
University of Michigan experience and literature review. Bone Marrow
Transplant. 2001 May;27(9):939-47.
21. Oliver RT. Testicular cancer. Curr Opin Oncol. 2001 May;13(3):191-8.
22. Sirohi, B, Powles, R, Singhal, S, et al. High-dose melphalan and second
autografts for myeloma relapsing after one autograft: Results equivalent to
tandem autotransplantation. Blood 2001; 98:402a.
23. Attal M, Harousseau JL. Randomized trial experience of the Intergroupe
Franchophone du Myelome Semin Hematol. 2001;38:226-30.
24. Badros A, Barlogie B, Morris C, et al. High response rate in refractory and poor-
risk multiple myeloma after allotransplantation using a nonmyeloablative
conditioning regimen and donor leukocyte infusions. Blood. 2001;97(9):2574-
2579.
25. Bhatia S, Abonour R, Porcu P, et al. High-dose chemotherapy as initial salvage
chemotherapy in patients with relapsed testicular cancer. JCO.
2000;18(19):3346-3351.
26. Sobecks RM, Vogelzang NJ. High dose chemotherapy with autologous stem-cell
support for germ cell tumors. A critical review. Semin Oncol. 1999;26:106-18.
27. Barlogie, B, Jagannath, S, Desikan, KR, et al. Total therapy with tandem
transplants for newly diagnosed multiple myeloma. Blood 1999; 93:55.
28. Murty VV, Chaganti RS. A genetic perspective of male germ cell tumors. Semin
Oncol. 1998 Apr;25(2):133-44.
29. Fermand JP, Ravaud P, Chevret S, et al. High-dose therapy and autologous
peripheral blood stem cell transplantation in multiple myeloma: up-front or
rescue treatment? Results of a multicenter sequential randomized clinical trial.
Blood. 1998; 92(9):3131-3136.
30. Schmoll KJ, Beyer J. Prognostic factors in metastatic germ cell tumors. Seminars
in Oncology. 1998;25(2):174-186.

Stem Cell Tandem Transplants Jun 17 24
31. Broun ER, Nichols CR, Gize G, et al. Tandem high dose chemotherapy with
autologous bone marrow transplantation for initial relapse of testicular germ cell
cancer. Cancer. 1997 Apr 15;79(8):1605-10.
32. Barlogie B, Jagannath S, Vesole DH, et al. Superiority of tandem autologous
transplantation over standard therapy for previously untreated multiple
myeloma. Blood. 1997; 89(3):789-793.
33. Bataille R, Harousseau JL. Multiple myeloma. NEJM. 1997;336(23):1657-1664.
34. Attal M, Harousseau JL, Stoppa AM, et al. A prospective, randomized trial of
autologous bone marrow transplantation and chemotherapy in multiple
myeloma. NEJM. 1996;335(2):91-97.
Important Notice
General Purpose. Health Net's National Medical Policies (the "Policies") are developed to assist Health Net in administering plan benefits and determining whether a particular procedure, drug, service or supply is medically necessary. The Policies are based upon a review of the available clinical information including clinical outcome studies in the peer-reviewed published medical literature, regulatory status of the drug or device, evidence-based guidelines of governmental bodies, and evidence-based guidelines and positions of select national health professional
organizations. Coverage determinations are made on a case-by-case basis and are subject to all of the terms, conditions, limitations, and exclusions of the member's contract, including medical necessity requirements. Health Net may use the Policies to determine whether under the facts and circumstances of a particular case, the proposed procedure, drug, service or supply is medically necessary. The conclusion that a procedure, drug, service or supply is medically necessary does not constitute coverage. The member's contract defines which procedure, drug, service or supply is covered, excluded, limited, or subject to dollar caps. The policy provides for clearly written, reasonable and current criteria that have been approved by Health Net’s National Medical Advisory Council (MAC). The clinical criteria and medical policies provide guidelines for determining the medical necessity criteria for specific procedures, equipment, and services. In order to be eligible, all services must be medically necessary and otherwise defined in the member's benefits contract as described this "Important Notice" disclaimer. In all cases, final benefit determinations are based on the applicable contract language. To the extent there are any conflicts between medical policy guidelines and applicable contract language, the contract language prevails. Medical policy is not intended to override the policy that defines the member’s benefits, nor is it intended to dictate to providers how to practice medicine. Policy Effective Date and Defined Terms. The date of posting is not the effective date of the Policy. The Policy is effective as of the date determined by Health Net. All policies are subject to applicable legal and regulatory mandates and requirements for prior notification. If there is a discrepancy between the policy effective date and legal mandates and regulatory requirements, the requirements of law and regulation shall govern. * In some states, prior notice or posting on the website is required before a policy is deemed effective. For information regarding the effective dates of Policies, contact your provider representative. The Policies do not include definitions. All terms are defined by Health Net. For information regarding the definitions of terms used in the Policies, contact your provider representative. Policy Amendment without Notice. Health Net reserves the right to amend the Policies without notice to providers or Members. In some states, prior notice or website posting is required before an amendment is deemed effective. No Medical Advice. The Policies do not constitute medical advice. Health Net does not provide or recommend treatment to members. Members should consult with their treating physician in connection with diagnosis and treatment decisions. No Authorization or Guarantee of Coverage. The Policies do not constitute authorization or guarantee of coverage of particular procedure, drug, service or supply. Members and providers should refer to the Member contract to determine if exclusions, limitations, and dollar caps apply to a particular procedure, drug, service or supply. Policy Limitation: Member’s Contract Controls Coverage Determinations. Statutory Notice to Members: The materials provided to you are guidelines used by this plan to authorize, modify, or deny care for persons with similar illnesses or conditions. Specific care and treatment may vary depending on individual need and the benefits covered under your contract. The determination of coverage for a particular procedure, drug, service or supply is not based upon the Policies, but rather is subject to the facts of the individual clinical case, terms and conditions of the member’s contract, and requirements of applicable laws and regulations.

Stem Cell Tandem Transplants Jun 17 25
The contract language contains specific terms and conditions, including pre-existing conditions, limitations, exclusions, benefit maximums, eligibility, and other relevant terms and conditions of coverage. In the event the Member’s contract (also known as the benefit contract, coverage document, or evidence of coverage) conflicts with the Policies, the Member’s contract shall govern. The Policies do not replace or amend the Member’s contract. Policy Limitation: Legal and Regulatory Mandates and Requirements The determinations of coverage for a particular procedure, drug, service or supply is subject to applicable legal and regulatory mandates and requirements. If there is a discrepancy between the Policies and legal mandates and regulatory requirements, the requirements of law and regulation shall govern. Reconstructive Surgery CA Health and Safety Code 1367.63 requires health care service plans to cover reconstructive surgery. “Reconstructive surgery” means surgery performed to correct or repair abnormal structures of the body caused by congenital defects, developmental abnormalities, trauma, infection, tumors, or disease to do either of the following:
(1) To improve function or
(2) To create a normal appearance, to the extent possible.
Reconstructive surgery does not mean “cosmetic surgery," which is surgery performed to alter or reshape normal structures of the body in order to improve appearance.
Requests for reconstructive surgery may be denied, if the proposed procedure offers only a minimal improvement in the appearance of the enrollee, in accordance with the standard of care as practiced by physicians specializing in reconstructive surgery.
Reconstructive Surgery after Mastectomy
California Health and Safety Code 1367.6 requires treatment for breast cancer to cover prosthetic devices or reconstructive surgery to restore and achieve symmetry for the patient incident to a mastectomy. Coverage for prosthetic devices and reconstructive surgery shall be subject to the co-payment, or deductible and coinsurance conditions, that are applicable to the mastectomy and all other terms and conditions applicable to other benefits. "Mastectomy" means the removal of all or part of the breast for medically necessary reasons, as determined by a licensed physician and surgeon. Policy Limitations: Medicare and Medicaid Policies specifically developed to assist Health Net in administering Medicare or Medicaid plan benefits and determining coverage for a particular procedure, drug, service or supply for Medicare or Medicaid members shall not be construed to apply to any other Health Net plans and members. The Policies shall not be interpreted to limit the benefits afforded Medicare and Medicaid members by law and regulation.
Recommended

















