Neonatal Abstinence SyndromeMultiple Associated Risks
Henrietta S. Bada, MD, MPHProfessor, Department of Pediatrics
University of Kentucky
Director, Division of Maternal and Child HealthDepartment for Public Health
Cabinet for Health and Family Services

Faculty Disclosure
• Received honorarium as member of the advisory board meeting for US WorldMeds

Educational Need/Practice Gap
Gap = Lack of integration and coordination of care for infants with neonatal abstinence syndrome
Need = The risks associated with NAS at all levels in a socio ecological framework

Objectives
Upon completion of this educational activity, you will be able to:
1. Cite the epidemiology of neonatal abstinence syndrome to be able to understand the extent or magnitude of the problem
2. To list the various risks associated with neonatal abstinence syndrome which can affect outcomes

Expected Outcome
• Increased awareness of risks associated with NAS will guide any prevention or intervention.


Historical Background
• ~ 4000 BC Sumerians migrated from Persia and settled between the Tigris and Euphrates Rivers. Discovered a plant that will eventually bring more pleasure and more suffering than any plant in history – the “plant of joy” or opium.
• Opium: grows in different types of climates and soil, and resistant to insects and fungi.
• Gum from opium seedpod contains morphine, codeine, alpha narcotic and papaverine, and thebaine

Historical Background
• Early 16th century. Paracelsus created the concoction (laudanum, from Latin laudare – to be praised), opium mixed with brandy; physicians used laudanum for coughs, diarrhea, dysentery, and gout
• 1800s – Louisa May Alcott and George Washington used liquid opium; Mary Todd Lincoln was addicted to it.
• Isolation of morphine and expansion to medical use• Marketed by Merck & Co., Inc for pain relief and alcohol treatment• Morphine as intravenous drug.• Two opium wars between Britain and China. China lost both times
resulting in China ceded Hongkong to the British.

Historical Background
• 1875: 1st reported case of a newborn with signs of opioid withdrawal at birth; diagnosis: congenital morphism. No treatment; infant died.
• 1898: Heinrich Dreser developed heroin (diacethylmorphine); High drug potency, less dose needed, and less risk for addiction
• 1947- Methadone approved for use in US• 1966 - Buprenorphine discovered and FDA approved in 1985• 1975--Finnegan published the “Neonatal Abstinence Syndrome Score”
(January)• –Lipsitz published “The Neonatal Drug Withdrawal Scoring System”
(June)

Historical Background• 1986: Portenoy published based on 38 patients that “ opioid
maintenance therapy can be safe, salutary, and more humane alternative for patients with intractable non-malignant pain and no history of drug abuse.” Believed that compassion for patients with terminal cancer be extended to all patients
• Birth of pain as “fifth vital sign.”• Drugs like oxycodone had finally solved the problem of pain
relief “without addiction”• 1997--First reported case of buprenorphine withdrawal in
newborns.• 2002--First reported case of oxycontin withdrawal in newborns.

Big concern…
128 in the US die each day from an opioid-related overdose.”
Centers for Disease Control and Prevention,USA, 2018

• Opioid epidemic/crisis• Deaths from overdose• Increase in NAS cases• Increase in hospital
costs• ??? Consequences post
discharge
12

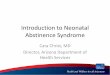
NAS Hospitalizations of Kentucky Resident Newborns, 2001 - 2016
46 6998 123 133 179 209 251
327 379522
632756
1060
13541257
1116
907
0200400600800
1000120014001600
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
2018
Num
ber
Year of admission
NAS is defined by any mention of the ICD-9-CM codes 779.5 and V3x, or of the ICD-10-CM codes P96.1 and Z38. The U.S. transition to ICD-10-CM occurred on October 1, 2015. The transition to ICD-10-CM should be considered as a possible contributor to any changes in trend observed between 2014 and 2016.Years on the time axis represent the admission date (not the discharge date). *2015 data from NAS State reportingProduced by Kentucky Injury Prevention Research Center, August, 2016Data source: Kentucky Inpatient Hospitalization Claims Files, Years 2001-2015; Cabinet for Health and Family Services, Office of Health PolicyData for 2010-2015 are provisional and subject to change.
*
* Data from NAS Surveillance Registry

NAS Trend (2001-2018)
0.0
5.0
10.0
15.0
20.0
25.0
30.0
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017 2018
NAS Rate 2 per. Mov. Avg. (NAS Rate)
Cases/1000
14
Kentucky Data
Almost 23 fold increase in rate from 0.9/1000 in 2001 to 20.4/1000 in 2016 and decreasing to 16.5/1000
https://chfs.ky.gov/agencies/dph/dmch/Documents/NASReport.pdf

Neonatal Abstinence SyndromeCalendar Year 2018
• Total unduplicated cases: 907 (infants transferred will have two reports)
• 64% with polysubstance exposure (excluding tobacco and alcohol)
Data Source: Kentucky Reportable Disease Surveillance System*Note: Unduplicated includes symptomatic, KY resident infants only

16
Characteristics of NAS Cases (2017)
NAS cases n ( %) No NAS n (%)
Maternal age <20 y 105 (9.4) 3853 (7.8)
20-24 y 207 (18.5) 13320 (26.8)
25 -29 y 410 (36.7) 15513 (31.2)
Race: White 982 (88.3) 41206 (83.8)
Black 38 (3.4) 4709 (9.5)
Less than HS 430 (38.9) 6892 (14.0)
Rural 449 (43.4) 11333 (22.8)
Medicaid/self-pay 1021 (92.7) 26211 (53.2)
Late preterm 119 (11.5) 3928 (7.9)
NICU 318 (31.1) 4452 (9.0)
Smoking 797 (73.3) 8477 (17.1)
Hepatitis C 353 (34.5) 824 (1.7)
KY NAS Surveillance Registry

Most Common Substances Used
Exposures (maternal history/tests or baby’s tests1. Buprenorphine – 61.7%2. Opiates Other – 41.2%3. Heroin – 19.6%4. Methadone – 9.5%5. Cannabinoid – 27.6%6. Benzodiazepine – 13.8%7. Cocaine – 8.4%8. Gabapentin – 5.7%
Data Source: Kentucky Reportable Disease Surveillance System*Note: Unduplicated includes symptomatic, KY resident infants only

• Opioids: opium, morphine, meperidine (Demerol), methadone, heroin, oxycodone (Oxycontin), hydrocodone (Lortab, Vicodin),hydromorphone (Dilaudid), codeine, pentazocine, fentanyl, propoxyphene (Darvon), Tramadol, Buprenorphine (Subutex)
• Alcohol, barbiturates, caffeine• Selective serotonin reuptake
inhibitors (Celexa, Prozac, Paxil, Zoloft, Effexor)
• Others: tricyclic antidepressants (Anafranil), desipramine (Pertrofan, Norpram)
• Chordiazepoxide (Librium), Diazepam (Valium), Diphenhydramine (Benadryl), ethchorvynol (Placidyl), glutethimide (Doriden), hydroxyzine (Atarax), meprobamate (Miltown, Equanil)
Drugs which produce “neonatal abstinence/withdrawal”—NAS or NOWS?

Kratom
• Leaves from the tropical tree Kratom in Southeast Asia which causes stimulant and sedative effects in different doses. More commonly abused in the Asia Pacific region than the United States.

Kratom
• A derivative of Mitragyna speciosa (coffee plant family)• 2 main alkaloids (opioid agonists)
• Mitragynine pseudoindoxyl (small affinity for receptors)• 7-hydroxymitragynine - increased potency as opioid agonist; higher
potency than morphine• Will not appear in urine toxicology• Use for pain, anxiety, depression, to stop or reduce withdrawal symptoms,
use as opioid substitute• Neonatal Abstinence Syndrome

Signs of Neonatal Narcotic Withdrawal
• Central Nervous System Signs• High-pitched cry• Decreased sleeping time• Hyperactivity• Hyper-reflexia• Tremors• Hypertonia• Myoclonic jerks• Convulsions• Irritability
• Gastrointestinal disturbances• Excessive sucking• Poor feeding• Regurgitation• Projectile vomiting• Loose to watery stools
• Metabolic/vaso-motor disturbances• Sweating• Fever• Yawning• Mottling

Signs of Neonatal Narcotic Withdrawal
• Respiratory disturbances• Nasal stuffiness• Sneezing• Nasal flaring• Tachypnea• Retractions
• Other manifestations• Abrasions or excoriations
(knees, elbows, chin)• Fever

Treatment of NAS
• Non-pharmacologic management• Reduced noise• Dim light• Swaddling• Rocking• Massage; OT, PT, ST, Music
• Optimal nutritional support• Breast feeding• Formula (high nutrient density)• Appropriate head position; slow flow nipple, etc
• Pharmacological treatment: morphine, clonidine, methadone, buprenorphine (currently in clinical trial); single or with adjunct therapy, phenobarbital
23

Infants With NAS: Associated Conditions and Common Measures of Outcomes
• Preterm birth• Intrauterine growth restriction• Congenital malformations• Medical complications• Pharmacotherapy: (no/yes, duration of therapy)• NICU care• Length of stay

What are we missing? Where are the gaps?
25

The Infants with NAS• DCBS reporting• Maternal characteristics (drug dependence,
treatment or none, comorbidities- medical and mental health)
• Discharge teaching (safe sleep, shaken baby, routine well-baby care, coping with a difficult child)
• Discharge disposition (mother, kinship care, foster care, adoption, institution)
• Follow-up care (medical home)and developmental monitoring
• Plan of safe care
Discharge Planning

Leading Causes of Infant Mortality
USA• Congenital malformations• Diseases related to
prematurity• Conditions affected by
maternal / pregnancy complications
• Sudden Unexpected Infant Deaths (SUID)
Kentucky• Diseases related to
prematurity• Sudden Unexpected Infant
Deaths (SUID)• Congenital malformations• Conditions affected by
maternal / pregnancy complications
27

154.6/100,000
AAP & Back to sleep campaign
87.5/100,000
92.6/100,000
SOURCE: CDC/NCHS, National Vital Statistics System, Compressed Mortality File

Rate of NAS cases by Area Development District 2018

56.3
66.771.3
76.2
65.3
46.5
54.850
59.5
47.4
32.426.2
31.9 31
52.6
45.1
57.1 55.3
67.973.7
78.9
89.394.7 95.2 93.7
0
10
20
30
40
50
60
70
80
90
100
2012 2013 2014 2015 2016
PERC
ENT
surface not designed for infant sleep sharing sleep surface sleep position (prone/side)
soft bedding and hazards at least one risk factor present
αNote: SUID Category includes only deaths to infants (<1 year of age) where the cause of death was coded as SIDS (R95), Accidental Suffocation in Bed (W75), Undetermined (R99), Other specified threats to breathing (W83), or Unspecified threat to breathing (W84). ∞Note: Categories under the Sleep-Related Risk Factors are not mutually exclusive**Note: 4 cases in 2015 were missing risk factor data and thus were excluded from the denominator data (N=84).Data Source: Kentucky Vital Statistics, Death Certificate File 2012-2016; Coroner’s Reports; Child Fatality Review Team Reports; and Kentucky Medical Examiner’s Reports, 2012-2016.
Percent of SUIDαCases with Sleep Related Risk Factors∞, Kentucky Residents, 2012-2016*

Child Fatalities/Near Fatalities(KY 2011-2015)
4753
39
0
20
40
60
80
100
Physical abuse Neglect Impairedcaregiver
Percent
6773
52
0
20
40
60
80
100
Substance abuse Domestic violence Mental illness
Percent
• Categories of maltreatment
• Risk factors in fatalities/near fatalities
https://justice.ky.gov/Documents/CFNFERP/2016%20Annual%20Report%20Final.pdf

Key Findings External ReviewChild Near Fatalities /Fatalities
• Substance abuse: most common risk factor• Most common risk factors contributing to fatality or near fatality
• Substance abuse by a caregiver• Mental health issues• Substance abuse in the home• Prior criminal history• Family violence• Prior history with child protective services
32
https://justice.ky.gov/Documents/CFNFERP/2016%20Annual%20Report%20Final.pdf

Complexity in Outcomes: Cumulative Risks Will Influence Outcomes

Adverse Childhood Experiences
• Seven categories of ACEs• Psychological• Physical• Sexual abuse• Violence against mother• Living with household members (substance
abusers)• Mentally ill or suicidal• Or ever imprisoned
• Cumulative ACEs (0-7) and association with risk factors for leading causes of death
Felitti V et al. Am J Prev. Med 1998; 14:245

Among Kentuckians With 5 or more ACES
• Almost five times as likely to have depression• Over four times as likely to have poor mental health• Almost four times as likely to be a current smoker• Almost two and a half times as likely to have asthma
2015 Kentucky Behavioral Risk Factor Survey (KyBRFS)

Connecting the ACEs and social, emotional, and cognitive impairment is the Disrupted Neurodevelopment.
Felitti V et al. Am J Prev. Med 1998; 14:245 https://childabuse.standford.edu

Epigenetic: Transmission of Mothering Behavior
Mothering is transmitted epigenetically from mother to daughter through levels of the ERα gene promoter

Promoting Child Development and
Maternal-Child Attachment
38

Child Development After NAS Amidst Crisis in the Home and Environment

Rate of Maternal* Deaths; Kentucky 2013-2018**
40
27.119.5 23.3
33.340.2
57.5
36.2
17.7
43.1 46.332.9
74.280.8
45.7
73.1
109.8
84.8
140.9
0
25
50
75
100
125
150
175
200
0
25
50
75
100
125
150
175
200
2013 2014 2015 2016 2017 2018
Rate
per
100
,000
live
birt
hs
Overdose P-Related All deaths
US – 18/100,000 (Pregnancy-related)
*Maternal death is defined as any female between the ages of 15-55 that was pregnant within one year prior to death or pregnant at death and died from any cause.**2016-2018 data is preliminary and numbers may changeData Source: KY Vital Statistics files, linked live birth and death certificate files years 2013-2018
US – 23.8/100,000

State Data (NAS Cases and Post Discharge Health)
KY NAS Data linked with Medicaid claims compared against HEDIS measures https://www.ncqa.org/hedis/measures/child-and-adolescent-well-care-visits/

Outcomes of Exposed Versus Controls
105110.13 107.5
53.9
42.849.2
88.2
107.599.9
49.5
35.542.4
0
20
40
60
80
100
120
MDI PDI Stanford-Binet McCarthyMotor
Expressive Receptive
Controls Opiate Exposed***
**
*
**
Hunt et al. Early Human Dev 2008 ; 84:29-35
*** p<0.001; **p<0.01; *P<0.05

Developmental Outcomes of Infants Treated for NAS
92.3 92.8 94.490.582.9 86.3
0
20
40
60
80
100
120
Motor Cognitive Language
One Year Two Years
**
Mirsky et al. PAS 2017

Cognitive Outcomes Through 13 years
44 Bauer et al. Maternal Lifestyle Study

Behavior Outcomes (Total Problems Through 15 years)
45
Bauer et al. Maternal Lifestyle Study


Risks and Protective FactorsRisk Protective Factors
Individual Male Resilience
Small head Temperament
Low verbal or full IQ
Overweight (medical problems)
Family Depression, psychological functioning
Secure attachment
Domestic violence Home
Illegal and legal drug Use Caretaker involvement
Caretaker supervision
Family support/resources
Community Violence Neighborhood
Gangs, Crimes Friends, extracurricular activities
Bada H. 2012 Pediatrics 130 (6) e1479-88

Risk and Protective FactorsDetermine outcomes considering the balance between cumulative risk and protective index
• High risk index – low protective index• High risk index – high protective index• Low risk index – low protective index• Low risk index – high protective index
Bada H. 2012 Pediatrics 130 (6) e1479-88

Total Behavior Problems: Balance of Risk and Protective Factors
Bada H. 2012 Pediatrics 130 (6) e1479-88

Drug Use & Other Risks
Protective Factors

Resilience
• Resilience is the ability to overcome serious hardship• The foundation of resilience is the combination of
• Supportive relationships• Adaptive skill building• Positive experiences that re-inforce self-efficacy, perceived control, and
belonging
• Resilience requires relationships• The capabilities that underlie resilience can be strengthened at any
age
Harvard Center for the Developing Child. Key Concepts

Approach Directed to Enhance Outcomes of Neonatal Abstinence Syndrome (NAS)
• Mother and infant dyad• Multifaceted• Coordinated• Collaborative• Integrated

Integration of Services
Dyad
CHFS
Community
PCP
Hospital
Prenatal Care TreatmentPregnancy
Limited or NoPrenatal Care
Continue maternal MAT or refer for treatment/mental healthManage NASDischarge planningEducation: Safe sleep &Prevent abusive head trauma
Well Child, Immunization, Growth, ER Visits, Rehospitalization
Referral and monitor LDH/Community services
DPH: HANDS, WIC, Family PlanningCMHC, Peer Support, DCBS
Tangible services:HousingTransportation, legal, other community resources

“The level of civilization attained by any society will be determined by the attention it has paid to the welfare of its children”… the Children’s Bill of Rights
… Billy F. Andrews, 1964.
Recommended