Neuroprotection for Scoliosis Surgery
Mary Ellen McCann, MD, MPH
Associate Professor of Anaesthesia Harvard Medical School
Children’s Hospital Boston [email protected]

Disclosure
• I have no financial relationships to disclose • I will not be discussing off label or
investigational use in this talk
Overview
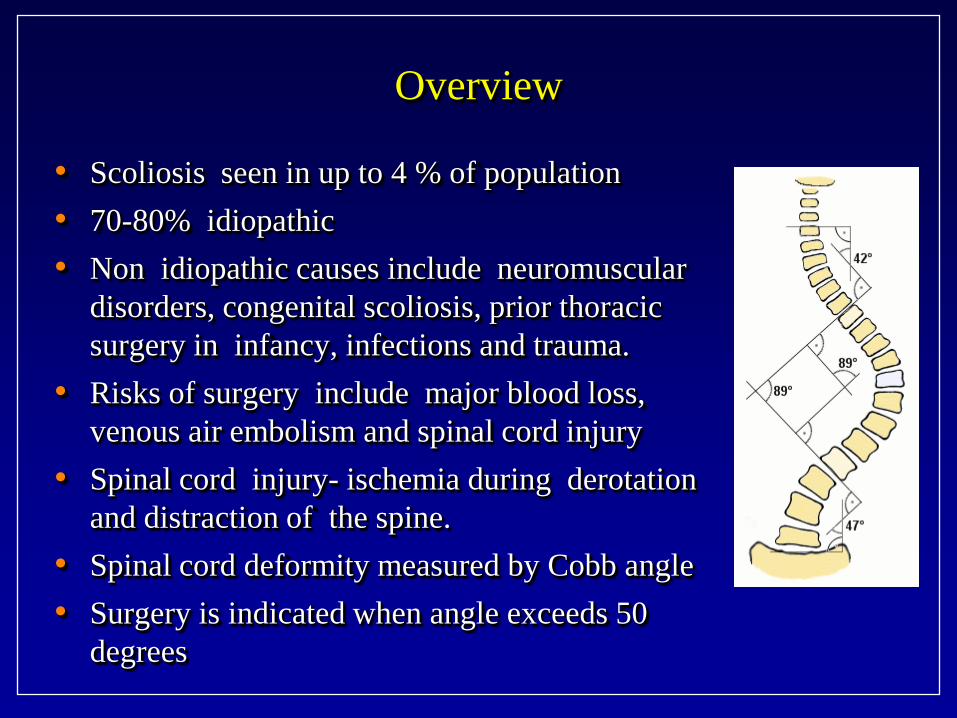
• Scoliosis seen in up to 4 % of population • 70-80% idiopathic • Non idiopathic causes include neuromuscular
disorders, congenital scoliosis, prior thoracic surgery in infancy, infections and trauma.
• Risks of surgery include major blood loss, venous air embolism and spinal cord injury
• Spinal cord injury- ischemia during derotation and distraction of the spine.
• Spinal cord deformity measured by Cobb angle • Surgery is indicated when angle exceeds 50
degrees
IOM definition
• Intraoperative Monitoring (IOM) • Can be unimodal or multimodal
- The use of modalities (test(s)) to help detect surgical or peri-surgically induced insults to neural structures, in order to prevent permanent neurologic deficits
The Evidence for Intraoperative Neurophysiological Monitoring in Spine
Surgery: Does It Make a Difference? Fehlings, Spine 2010
• 1990-2009 • 32 articles • HLE –MIOM sensitive and specific for detecting intraoperative
neurologic injury • HLE-MEPs are better than SSEPs • LLE that IOM reduces the rate of new or worsened periperative
neuro deficits • VLLE that intraop responses to NM alert reduces rate of periop
neuro deterioration.
IOM
• Spinal sensory evoked potentials (SSEP) • Transcranial Motor evoked potentials (TcMEP) • Neurogenic Motor Evoked Potentials • Electromyography • Pedicle screw stimulation • Stagnara wake-up test
Spinal Sensory Evoked Potential
• Stimulation site: - peripheral nerve (post tib) - Constant current stimulation 25-50mA - 300-500 trials averaged
• Recording from scalp (sensory cortex) • Meaningful Change
- Measure: conduction latency>10% and amplitude<50%
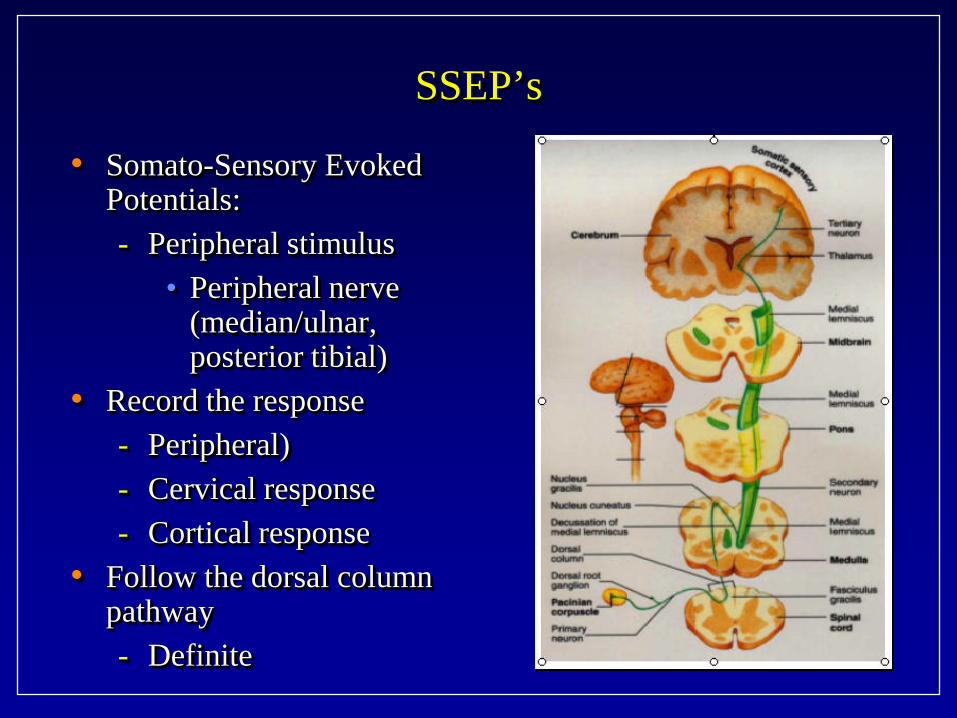
SSEP’s
• Somato-Sensory Evoked Potentials: - Peripheral stimulus
• Peripheral nerve (median/ulnar, posterior tibial)
• Record the response - Peripheral) - Cervical response - Cortical response
• Follow the dorsal column pathway - Definite
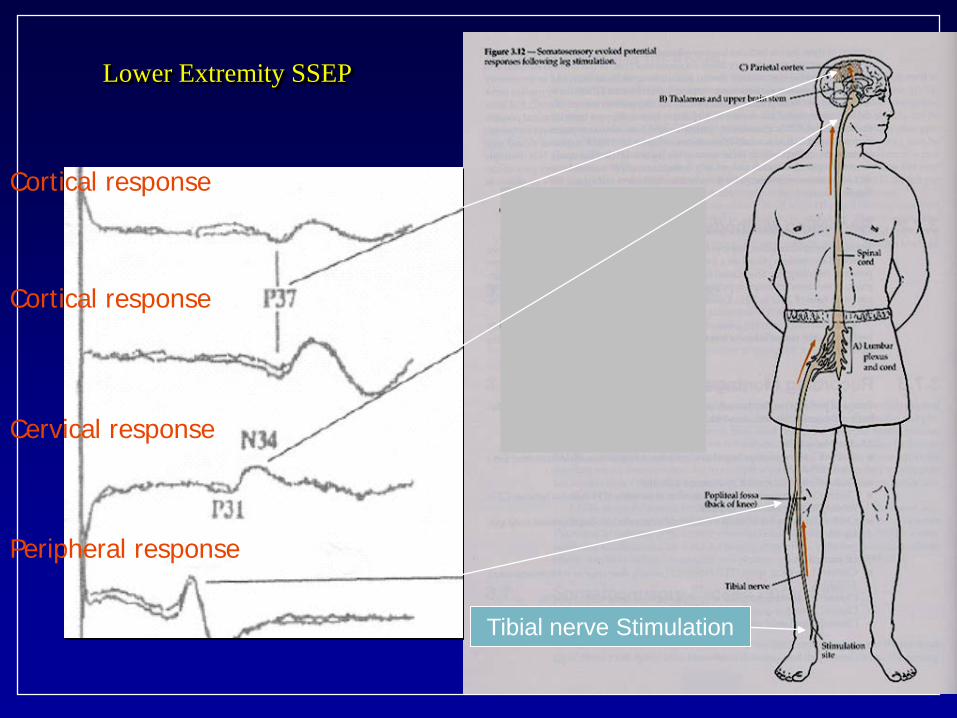
Lower Extremity SSEP
Tibial nerve Stimulation
Cortical response
Cervical response
Peripheral response
Cortical response
SSEP
• Limitations, Disadvantages: - Motor pathways more sensitive than sensory to
ischemia - Affected by inhalational anesthetic agents,
intravenous agents, hypotension and hypothermia - Changes must be averaged over 5 minutes
• Advantages: - Can use NMBs - Successful in infants of >3 mo
Transcranial Stimulation for Motor Evoked Potentials – TCMEP’s
• Stimulation: - Cortical structures across intact cranium
• Response: - Evoked potentials recorded in peripheral
structure • True motor pathway • Direct information about cortical function

Transcranial Stimulation
• Transcranial Electrical Stimulation (TcMEP) • Transcranial Magnetic Stimulation (TcMS)

TCMEPs
• TransCranial Electrical Motor Evoked Potentials
• Stimulate motor cortex • Record in muscle (hand,
foot) • Follow the lateral
corticospinal pathway
TcMEP’s • TcMEP’s-activation of motor neurons of the
corticospinal tract via application of strong electrical impulse across scalp into the cranium
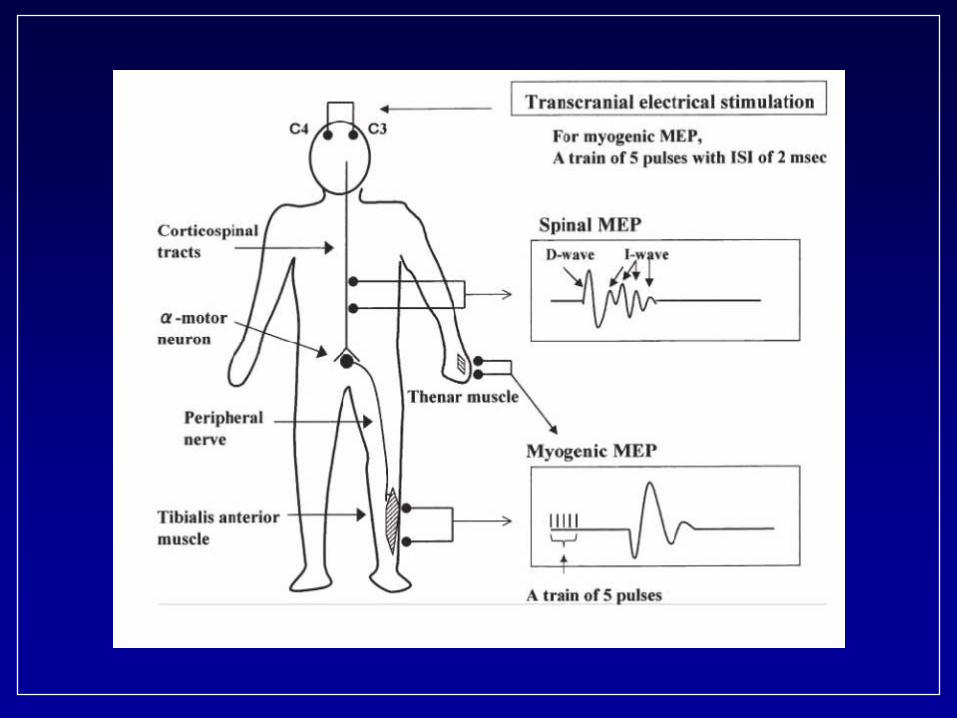
• 2 waves generated which can be recorded by epidural or direct spinal cord probe: - D wave (direct): unaffected by anesthesia
• depolarization of axon directly correlates to post-op motor function
- I wave (indirect): affected by anesthetic agents • unstable waveform, difficult to reliably reproduce
TcMEP’s
• Monitors motor spinal cord motor pathway integrity during surgery - Single stimulus technique - Multiple stimulus technique
• 3-5 pulses at 500 hz

TcMEP
• Multiple stimulus technique: - Short train of repetitive electrical stimuli to cortex - EMG needles in extremities
• compound muscle action potential is produced • Can be combined with D-wave recording to have
combined D-wave + EMG • Latter is sensitive to pathology in spinal cord with
little affect from anesthesia
TcMEP’s
• In young children: - Sutures still open - Electrodes away form open sutures - Motor pathways not mature until age 18 months
• Response may be incomplete, unobtainable <6 years
TcMEP’s
• Limitations: - Poor cortical tissue:
• Severe CP • Severe hydrocephalus
- Suppressed cortex • Severe seizure disorder on lots of seizure meds
- Poor peripheral nerves: • Peripheral neuropathy
- No motors • Severe myopathy

TcMEP’s
• Some safety concerns - Bite blocks to avoid tongue lacerations, jaw injury - Seizures can rarely be triggered (5 in 15,000 cases.
Legatt 2004) • Exclusion criteria:
- Metal plates in skull - Cochlear implants,cardiac pacemakers,dorsal column
stimulators or other implanted device that might be impaired by high intensity electrical stimulation
• Young patients with immature brains-less myelination can have suboptimal TcES
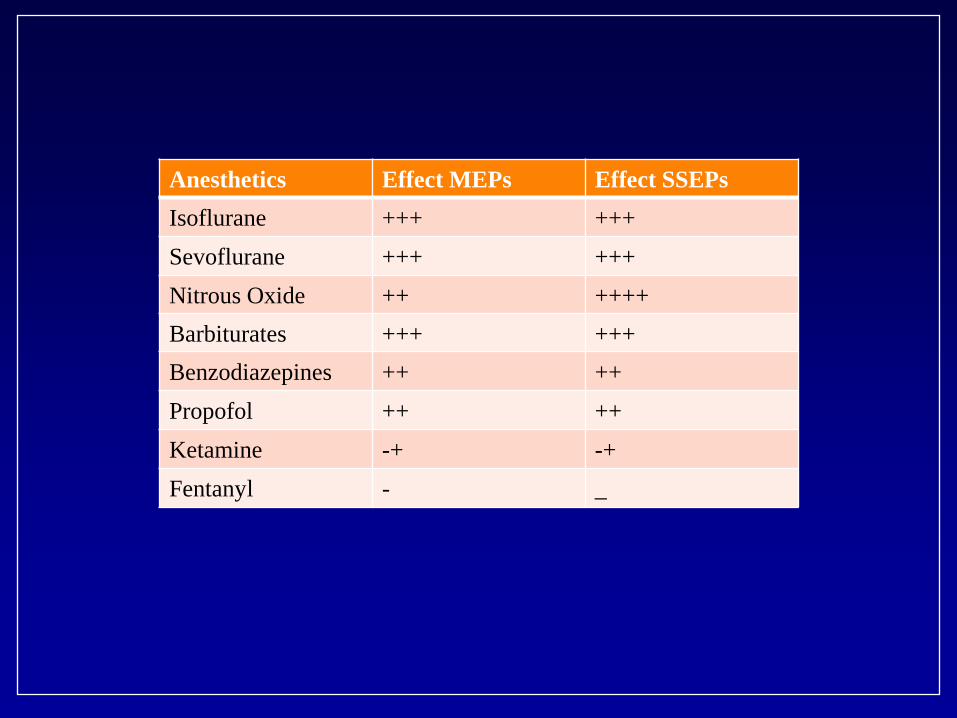
Anesthetics Effect MEPs Effect SSEPs Isoflurane +++ +++ Sevoflurane +++ +++ Nitrous Oxide ++ ++++ Barbiturates +++ +++ Benzodiazepines ++ ++ Propofol ++ ++ Ketamine -+ -+ Fentanyl - _
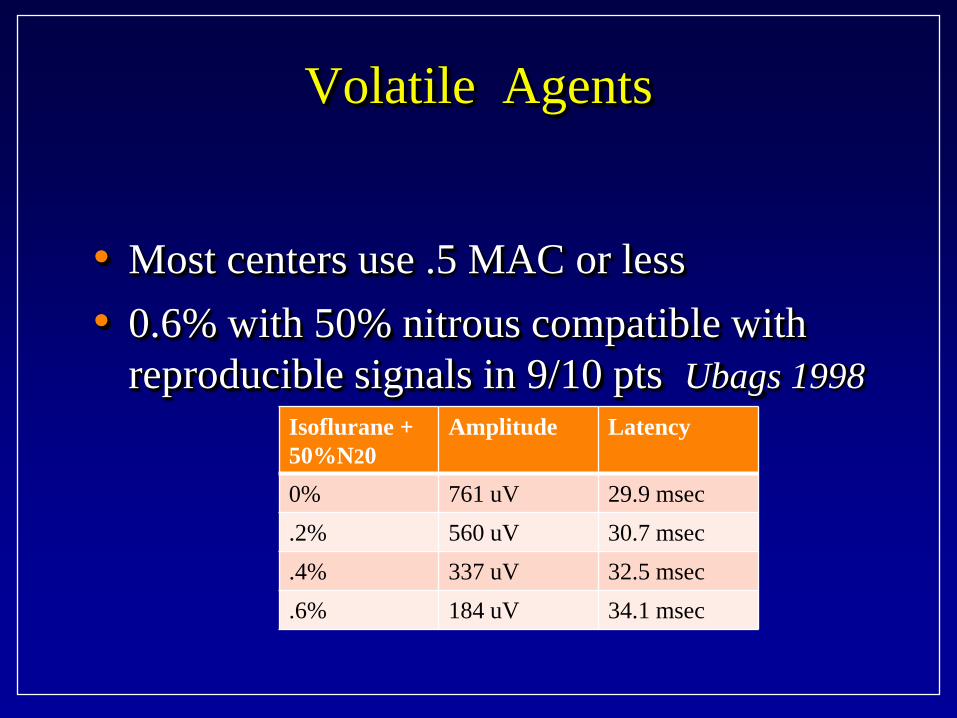
Volatile Agents
• Most centers use .5 MAC or less • 0.6% with 50% nitrous compatible with
reproducible signals in 9/10 pts Ubags 1998
Isoflurane + 50%N20
Amplitude Latency
0% 761 uV 29.9 msec .2% 560 uV 30.7 msec .4% 337 uV 32.5 msec .6% 184 uV 34.1 msec

Nitrous Oxide
• 60% N2O compatible with multipulse stimulation Van Dongen 1999
• Hi dose propofol not compatible Sakamoto 2001
• Suppression augmented by hypothermia in rabbits Kakimoto 2002
Propofol
• Superior MEPs compared to isoflurane + N20 • Keep dose <200 ug/kg/min
Dexmedetomidine
• Similar to propofol Mahmoud 2010
• May allow lower doses of propofol and diminish risk of PRIS
Ketamine
• No effect on MEPs until high doses • 1 mg/kg no effect on human volunteers Kalkman
1994
• 41% patients will have dysphoria at 1-2 mg/kg/hr
• 14% at 1 mg/kg/hr when paired with low dose propofol Kawaguchi 2000

Midazolam
• Similar effects to other types of TIVA
Evoked Potential Fade
• Gradual MEP amplitude fading and threshold increase normal with either TIVA or inhalational agents
• Estimated that increase 11 V/hr intact pts, 23 V/hr myelopathic pts Lyon 2005
Optimal Physiologic Parameters
• Blood Pressure MAP>65-70 mm Hg • Normal temperature • Normovolemia • Hematocrit>21% • Normal Cardiac Output
Effect of Hemorrhage and Hypotension on Transcranial Motor-evoked Potentials in Swine
• 12 swine-prop/ket/fent-hemorrhaged to TcMEPs 40% baseline
• Treatment with colloid or phenylephrine did not improve TcMEPs
• Treatment with epinephrine did improve TcMEPs • Decrease in TcMEPs associated with decrease in CO
and DO2 but not MAP
Neurogenic Motor Evoked Potentials – NMEP’s
• Stimulation site: - Spinal cord
• Percutaneous needle or open spinous process • Epidural electrode
• Parameters: - Stimulation current less than 300mA - Average of 100 trials
• Recording site: - Neurogenic MEP
• Popliteal fossa/post tib nerve for mixed motor sensory response
- Myogenic MEP - use the muscle of choice for electromyography
NMEP
• Disadvantages: - affected by inhalational anesthetic agents,
intravenous agents, hypotension, hypothermia (but less than SSEP’s)
- NMEP-probably not a true indicator of motor pathway function
- Myogenic MEP - cannot paralyze patient pharmacologically
Electromyography
• Continuous free-running electro-myographic monitoring
• Stimulus-triggered electromyography
Continuous Free-Running Electromyography
• Paired intramuscular needle or wire electrodes - Monitor muscles innervated by nerves or
nerve roots considered to be at risk during surgery
- High frequency EMG activity • Neurotonic discharges
• Trauma to roots or peripheral nerve • Previously irritated root
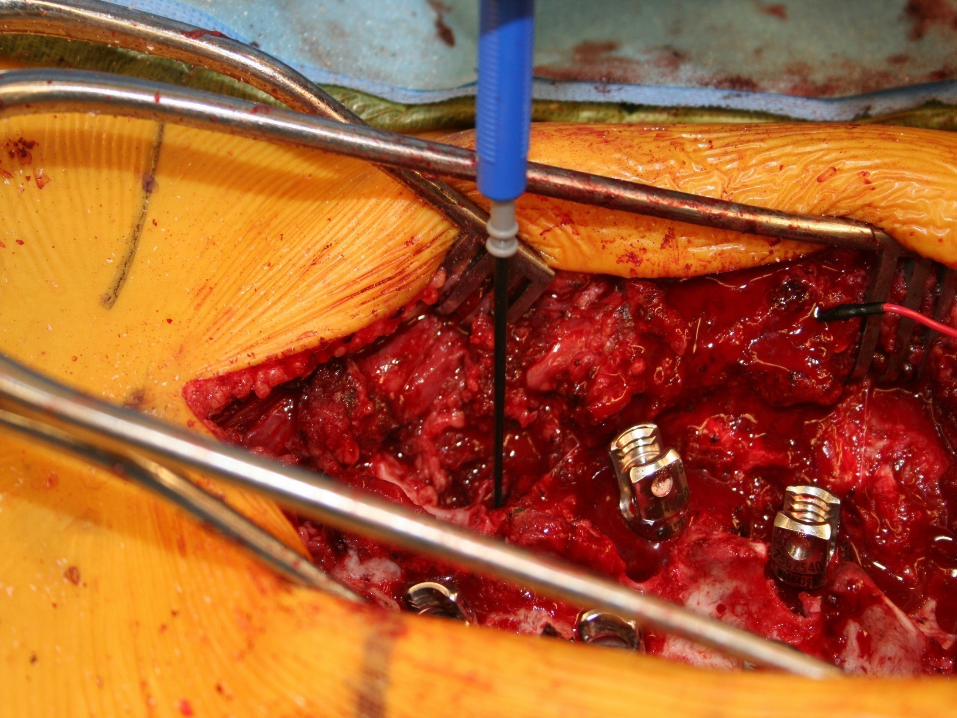
Stimulus-Triggered Electromyography
• Electrical stimulation of motor nerves: - Compound muscle action potentials (CMAPs) in
innervated muscles • Intraoperative stimulus-triggered EMG:
- Integrity of instrumented pedicles • Cortical bone has high impedence to passage of
current • Perforation of pedicle:
• Lowers the impedence • Activates the local nerve root at a lower
stimulus intensity
Testing Pedicular Instrumentation
• Each hole or screw can be tested individually • A misplaced hole can be redirected and retested • Stimulus thresholds of less than 4-6-8 mA are
suggestive of cortical bony perforation - Triggered EMG study had 99.6% screw “left in
place” with threshold 8.0mA or greater (Raynor et al SRS 2004) in lumbar spine
• Thoracic triggered EMG’s not as reliable

Pedicle Screw Stimulation
• C3-4 Trapezius • C5-6 Biceps • C6-7 Triceps • C7-8 Ex Dig communis • T1 Abductor pollicis brevis • T7-12 Ext Oblique and Rec Ab

Pedicle Screw Stimulation
• L1-2 Iliacus • L2-4 Vastus Medialis • L4-5 Tibialis anterior • S1-2 Medial Gastrocnemius • S3-4 Anal and Urethral Sphincter
What is a significant change?
• SSEPs - 50% in amplitude - 10% in latency
• TCeMEPs - 80% in amplitude
• EMG - Sustained activity
• Triggered EMG - < 8 mA stim
Stagnara Wake-up Test
• Gold Standard? • Limitations:
- Not continuous ( although can be)
- Patient must follow commands: “squeeze hands, wiggle toes, move feet up and down and in and out”
- Someone at head and feet - Inhalational WU faster than
TIVA
Stagnara Wake-up Test
• Risks: - Extubation: - Movement off table
• Dislodge lines • Dislodge, plough implants
- Air embolism - flood wound with saline sponges
Strategies for changed IOM
• Three basic causes: - Technical
• Equipment • Anesthetic • Positioning?
- Mechanical change to neural structure
- Vascular compromise of neural structure
Strategies for changed IOM
• Maximize perfusion: - BP - Hct - Temp
• What did you last do? (or do before that?) - May be significant lag - Reverse last (or last several manuevers) - If no improvement, consider
• Remove all correction • Retain stabilization if spine unstable
Strategies for changed IOM
• Wake-up test • Significance of resolved IOM change?
- Early warning - Indicator of cord status
Inadvertent benefits of IOM:
• Communication with surgeon, neuromonitoring team
• Brain status • Early pick-up of upper extremity issues
Recommended

















