618 FETAL CARDIOVASCULAR RESPONSE TO HYPOXEMIA IS DEPENDENT UPON GES-TATIONAL AGE IN RHESUS MONKEYS JORGE TOLOSA1, JUHA RASANEN2,ELIOT SPINDEL3, JOHN FANTON4, LEONARDO PEREIRA1, PATRICIA ROBERTSON1,MICHAEL GRAVETT5, 1Oregon Health & Science University (OHSU), MaternalFetal Medicine, Portland, Oregon, 2University of Oulu, Obstetrics and Gyne-cology, Oulu, Finland, 3OHSU, Oregon National Primate Research Center(ONPRC), Division of Neuroscience, Beaverton, Oregon, 4OHSU, ONPRC,Surgery Svs, Beaverton, Oregon, 5OHSU, ONPRC, Maternal Fetal Medicine,Portland, Oregon
OBJECTIVE: To test the hypothesis that cardiovascular responses tohypoxemia change with advancing gestation and demonstrate the value of aunique animal model using non-human primates.
STUDY DESIGN: Rhesus macaques with timed gestations underwent Dop-pler ultrasonographic examination at 91 (n=2) gestational days (term is 165days), at 104 (n=1) days and at 140 (n=1) days of gestation while sedatedwith continuous rate infusion ketamine (400-500 mcg/kg/min). Fetal cardio-vascular hemodynamics were evaluated (Voluson 730 Expert, GE Healthcare,USA) prior to and during fetal hypoxemia which was induced by decreasingmaternal inhaled oxygen content; (gas mixture was approximately 70%oxygen and 30% helium) to achieve a pulse oximetry of 80% saturation.
RESULTS: Umbilical artery, right pulmonary artery (RPA), middle cerebralartery pulsatility index (PI) values all decreased with advancing gestation. Theductus venosus and inferior vena cava PI values did not show a similar trend.During hypoxemia, fetal cardiovascular hemodynamic parameters remainedunchanged at 91 and 104 gestational days. However, at 140 days fetalhypoxemia led to a 3-fold increase in RPA PI values when compared withbaseline.
CONCLUSION: Rhesus macaque fetuses demonstrated changes in cardio-vascular hemodynamics similar to human fetuses with advancing gestationalage. At 140 days of gestation, fetal pulmonary artery vascular impedanceincreased in response to hypoxemia.
(Supported by NIH grants AI42490 and HD/HL37131).
619 THROMBOPHILIC PATIENTS DEMONSTRATE PROGRESSIVE INCREASES IN VAS-COACTIVITY COMPARED TO NORMAL PREGNANCY GABRIELE URBAN1, ROMOLO DIIORIO2, EMANUELA MARINONI3, DE-HUI KU4, YALE ARKEL5, MICHAEL PAIDAS1,1Yale University, Obstetrics & Gynecology, New Haven, Connecticut, 2Uni-versity La Sapienza, Rome, Italy, 3University of Rome La Sapienza, Gynecol-ogy, perinatology and Child health, Rome, Italy, 4New York University,Obstetric and Gyencology, New York City, New York, 5Maine Medical Cen-ter Research Institute, Portland, Maine
OBJECTIVE: Pregnancy is characterized by progressive coagulation activa-tion. Adrenomedullin (AM) is a specific G-protein signaling peptide vasodi-lator whose maternal plasma levels increase in pregnancy. While pregnantpatients with thrombophilic conditions have elevated coagulation activation,AM levels has never been measured in this group. We speculate thrombophiliais associated with exaggerated vasoactivity and coagulation activation com-pared to normal pregnancy.
STUDY DESIGN: In this nested case control study, we compared matermalplasma levels of SFP and AM from 42 singleton uncomplicated and 23thrombophilic singleton gestations, matched from gravidity, parity, gestationalage (GA) at draw. Patients were sampled in three trimesters prospectively inpregnancy and plasma was stored at �80(C until assay. AM and SFP levelswere measured by radioimmunoassay and immunoassay, resp. Data wereanalyzed by Spearman correlaton and Fisher Exact test.
RESULTS: Thrombophilic patients demonstrate progressive increases inBOTH AM and SFP levels in pregnancy, while patients with normalpregnancy display only significantly elevated AM levels in the third trimester.There is a significant correlation (rs=0.738; p!.05) between the AM concen-tration in the third trimester and SFP in normal pregnancy. There were nodifferences in GA at draw, GA at del, gravidity or parity.
CONCLUSION: Pregnant patients with thrombophilia have early onsetincreases in vasoactivity compared to patients with normal pregnancy. Wespeculate that in normal pregnancy, the increases in coagulation activation andvasoactivity occur in preparation for delivery, while in thrombophilic patientschronic elevation in vasoactivity may be contributing to pregnancy complica-tions.
Maternal SFP and AM throuthout pregnancy
Ist trimester 2nd trimester 3rd trimester
Thrombophilic SFP mg/ml 11.0 G 3.5 16.4 G 3.6 24.8 G 2.9Normal SFP mg/ml 9.2 G 3.1 9.7 G 2.5 8.8 G 2.0Thrombophilic AM �g/ml 31.2 G 3.9 42.5 G 2.3 52.9 G 41Normal AM �g/ml 34.1 G 4.6 33.4 G 2.2 57.1 G 5.0
S176 SMFM Abstracts
620 NEUROBIOLOGICALLY-BASED EARNING BENEFITS OF BEING BREASTFED: LONG-TERM ECONOMIC ANALYSIS JAMES MCGREGOR1, MANUK BARSEGHYAN2, 1Univer-sity of Southern California, OB/GYN, Los Angeles, California, 2CaliforniaState University Northridge, Economics, Northridge, California
OBJECTIVE: 1. Estimate differences in life-long labor market earningspotential accruing from neurocognitive benefits derived from breastfeeding. 2.Estimate variances of lifetime earnings associated with gender, birth weight,and SES.
STUDY DESIGN: We analyzed findings of ‘‘best evidence’’ (prospectivecontrolled trials, well-controlled epidemiologic expiriments) on possible im-provements in neurocognitive and special sense functioning resulting frombeing breastfed R6 months. We performed econometric calculations on theeffects of childhood neurologic performance measures (Salkever DS, EnvironRes 70:1-6 1995) on estimated lifetime earnings during a typical (47 years)employment career. Each point difference in IQ performance correlated with3.225% net increase among females, and 1.931% among males annually. Wecalculated results using this formula.
DEZE!
�DW
WC
DP
P
�
Formula
RESULTS: Multiple models were estimated: Assuming a discounted meannationally representative lifetime earnings of $723,300 for each 2-year-old in2000 dollars (3.8 million cohort) and a 4 point intelligence increase, theestimated positive earnings range from $110 to $319 billion. However, ifestimated annually with an average income of $41,000 and compounded overthe period of persons workforce participation, the amounts are significantlylarger ranging form 566 to 945 billions of 2005 U.S. dollars. Increased earningsassociated with breastfeeding accrued most significantly to female, low birthweight and low SES children.
CONCLUSION: We estimated variances in average lifetime earnings puta-tively affected by improved neurocognitive performance associated withbreastfeeding. Increases in earnings are substantial and increase most infemale, LBW and low SES infants. These monetary benefits are likely to below estimates, as they exclude the short-term economic savings or long-termhealth and social benefits of breastfeeding.
621 MATERNAL RACE AND THE GESTATIONAL AGE-SPECIFIC RISK FOR STILLBIRTHSEAN BLACKWELL1, JERRIE REFUERZO1, ROBERT J. SOKOL1, SONIA HASSAN1,YORAM SOROKIN2, 1Wayne State University, Obstetrics & Gynecology, Detroit,Michigan, 2Wayne State University, Ob/Gyn/Maternal Fetal Med, Detroit,Michigan
OBJECTIVE: The purpose of this study was to determine whether there areracial differences in the gestational age (GA)-specific stillbirth risk in an urban,lower socioeconomic population.
STUDY DESIGN: A computerized perinatal database identified singletonpregnancies delivered from Jan 1, 1991 to Dec 31, 2004 at one tertiary careurban hospital. The GA -specific risk of stillbirth (per 100,000 undeliveredfetuses at risk) was calculated and compared between African-American (AA)and Caucasian (CAU) women. Stillbirth was defined as fetal death at GA O20 wks or birth weight (BW) O 400 grams at delivery. Kaplan and Meirsurvival curves were generated and compared with log rank test. P ! 0.05 wasconsidered significant.
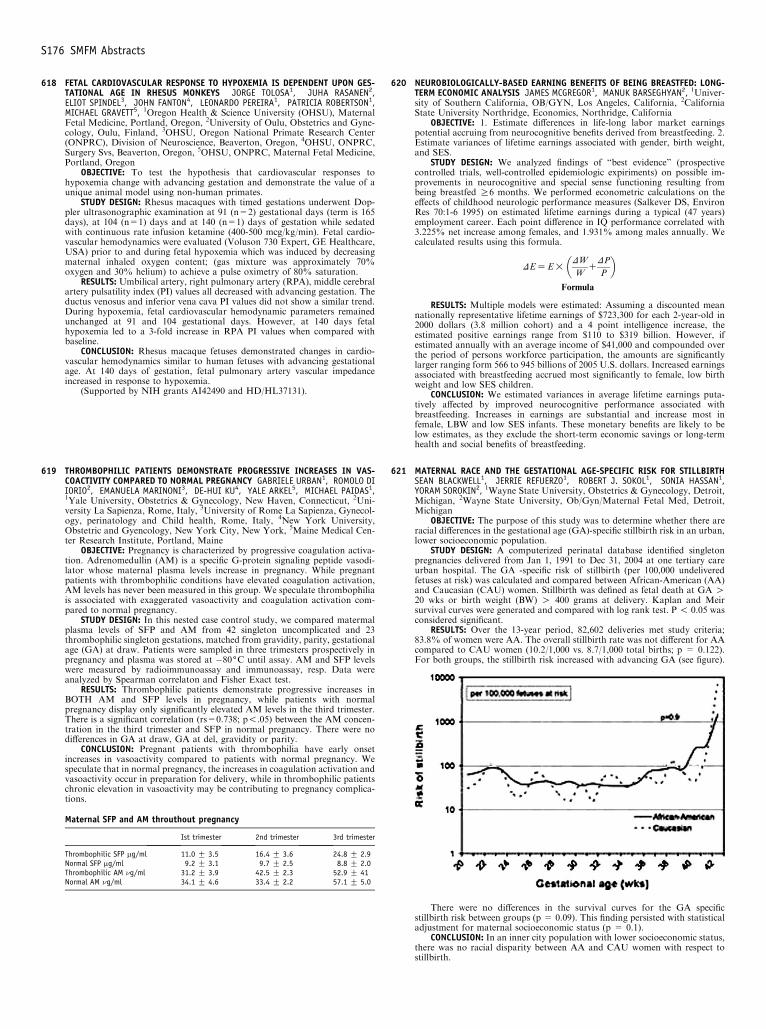
RESULTS: Over the 13-year period, 82,602 deliveries met study criteria;83.8% of women were AA. The overall stillbirth rate was not different for AAcompared to CAU women (10.2/1,000 vs. 8.7/1,000 total births; p = 0.122).For both groups, the stillbirth risk increased with advancing GA (see figure).
There were no differences in the survival curves for the GA specificstillbirth risk between groups (p = 0.09). This finding persisted with statisticaladjustment for maternal socioeconomic status (p = 0.1).
CONCLUSION: In an inner city population with lower socioeconomic status,there was no racial disparity between AA and CAU women with respect tostillbirth.
Recommended

![Postpartum remodeling, Lactation, and Breast Cancer risk ......parous women who never breastfed, women who had breastfed were at reduced risk of breast cancer (odds ratio [OR] = 0.90,](https://img.pdfslide.net/doc/110x75/6001e6a91975f01a69010f9d/postpartum-remodeling-lactation-and-breast-cancer-risk-parous-women-who.jpg)















