Perfusion Computed Tomography in
Acute Ischaemic Stroke
Nguyễn Trường Giang Thai Nguyen Central General Hospital, Vietnam Central for Advanced Imaging, The University of Queensland, Australia
Hanoi, nov 2015
Outline
u Brief introduction u Stroke Imaging u Perfusion CT techniques u Use of perfusion CT in acute stroke u Future direction of perfusion CT u Conclusion
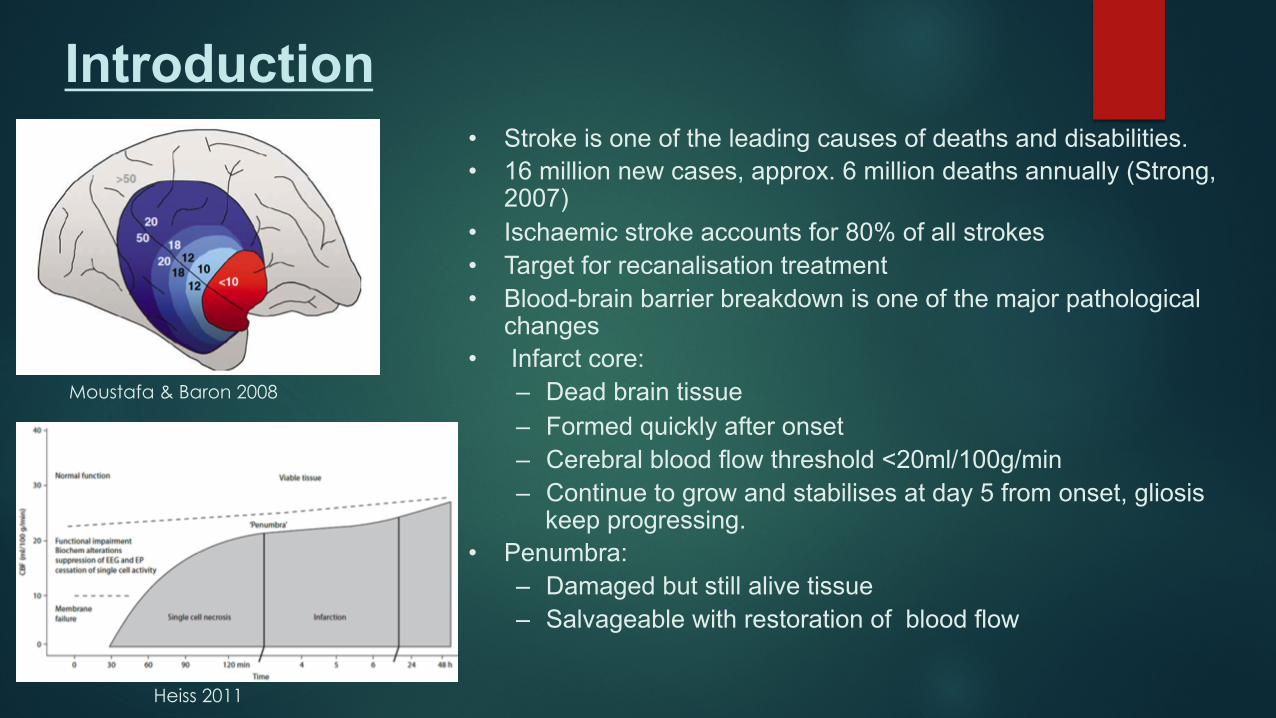
Introduction • Stroke is one of the leading causes of deaths and disabilities. • 16 million new cases, approx. 6 million deaths annually (Strong,
2007) • Ischaemic stroke accounts for 80% of all strokes • Target for recanalisation treatment • Blood-brain barrier breakdown is one of the major pathological
changes • Infarct core:
– Dead brain tissue – Formed quickly after onset – Cerebral blood flow threshold <20ml/100g/min – Continue to grow and stabilises at day 5 from onset, gliosis
keep progressing. • Penumbra:
– Damaged but still alive tissue – Salvageable with restoration of blood flow
Moustafa & Baron 2008
Heiss 2011
Four critical questions must be answered at patient admission (Shetty & Lev 2005):
a. Is this a haemorrhagic stroke? b. Is there thrombotic occlusion of a cerebral artery that can be treated
by thrombolysis or thrombectomy? c. Is an infarct core present in the ischaemic region? d. Is there potentially salvageable penumbral tissue?
Introduction
Stroke Imaging
u Target for Stroke Imaging: u Gives early diagnosis
u Differentiates subtypes of stroke
u Gives accurate amount of affected brain tissue and amount of dead brain
u Unenhanced CT, CT Angiography & Perfusion CT u Magnetic Resonance Imaging, MRA & MRP u DSA & Endovascular intervention
Stroke Imaging
4+ Ps in Stroke u Parenchyma: Indicate the early signs of acute ischaemic stroke, exclude haemorrhage
u Pipes: Gives information of vessels u Extracranial circulation (carotid and vertebral arteries of the neck)
u Intracranial circulation for evidence of intravascular thrombus
u Perfusion Assess cerebral blood volume, cerebral blood flow, and mean transit time
u Penumbra Assess tissue at risk of dying if ischemia continues without recanalization of intravascular thrombus Imaging.
u Permeability: Evaluate changes in blood-brain barrier permeability following ischaemic insult
Rowley (2001) AJNR 22(4):599-601
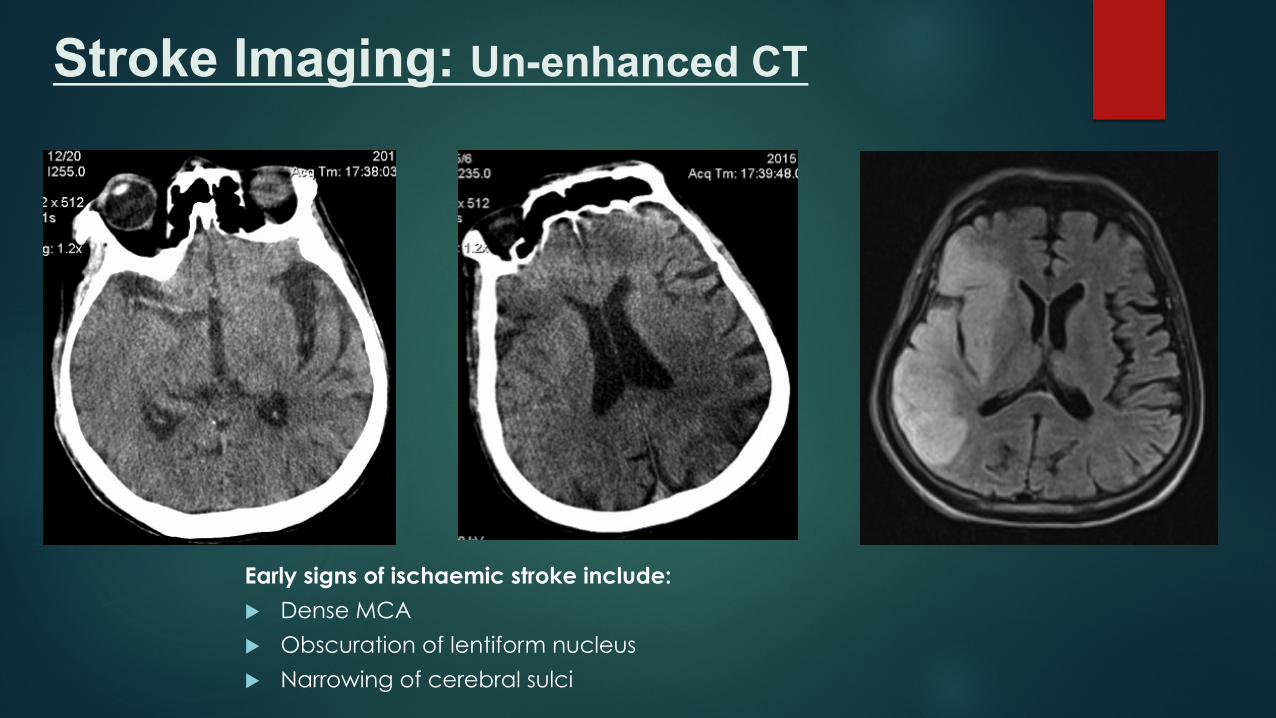
Stroke Imaging: Un-enhanced CT
Early signs of ischaemic stroke include:
u Dense MCA
u Obscuration of lentiform nucleus
u Narrowing of cerebral sulci
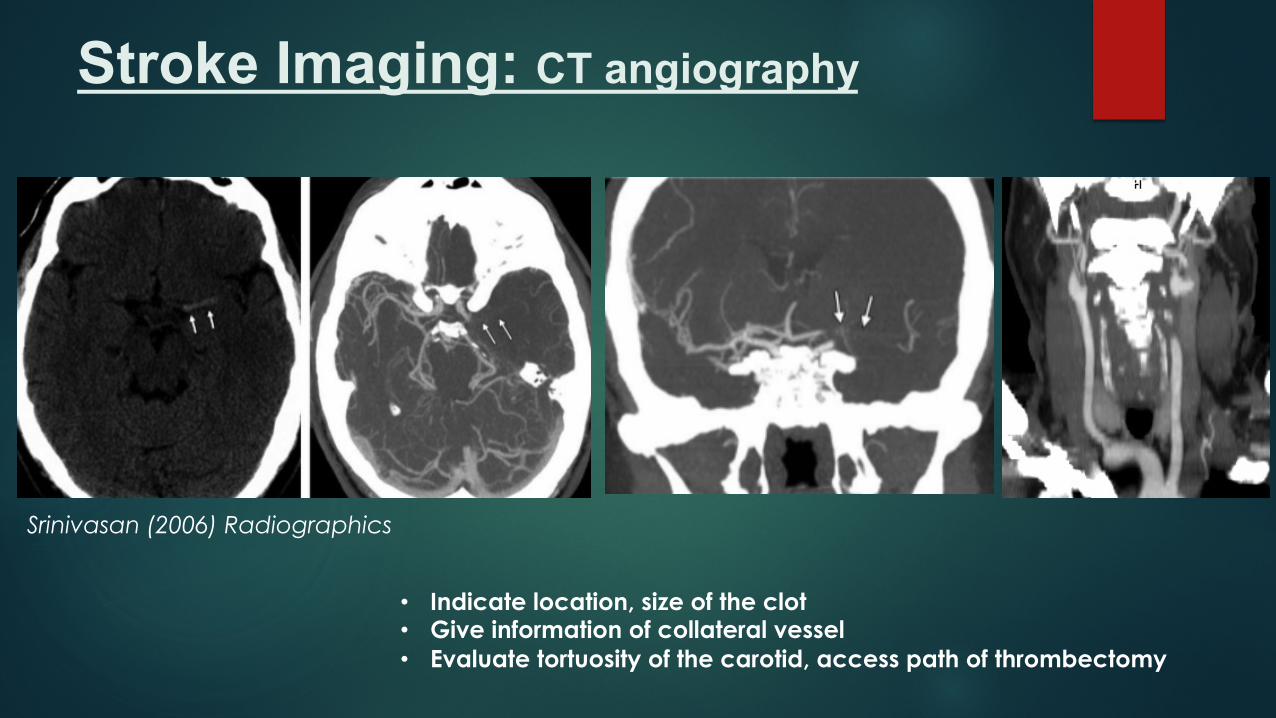
Stroke Imaging: CT angiography
• Indicate location, size of the clot • Give information of collateral vessel • Evaluate tortuosity of the carotid, access path of thrombectomy
Srinivasan (2006) Radiographics
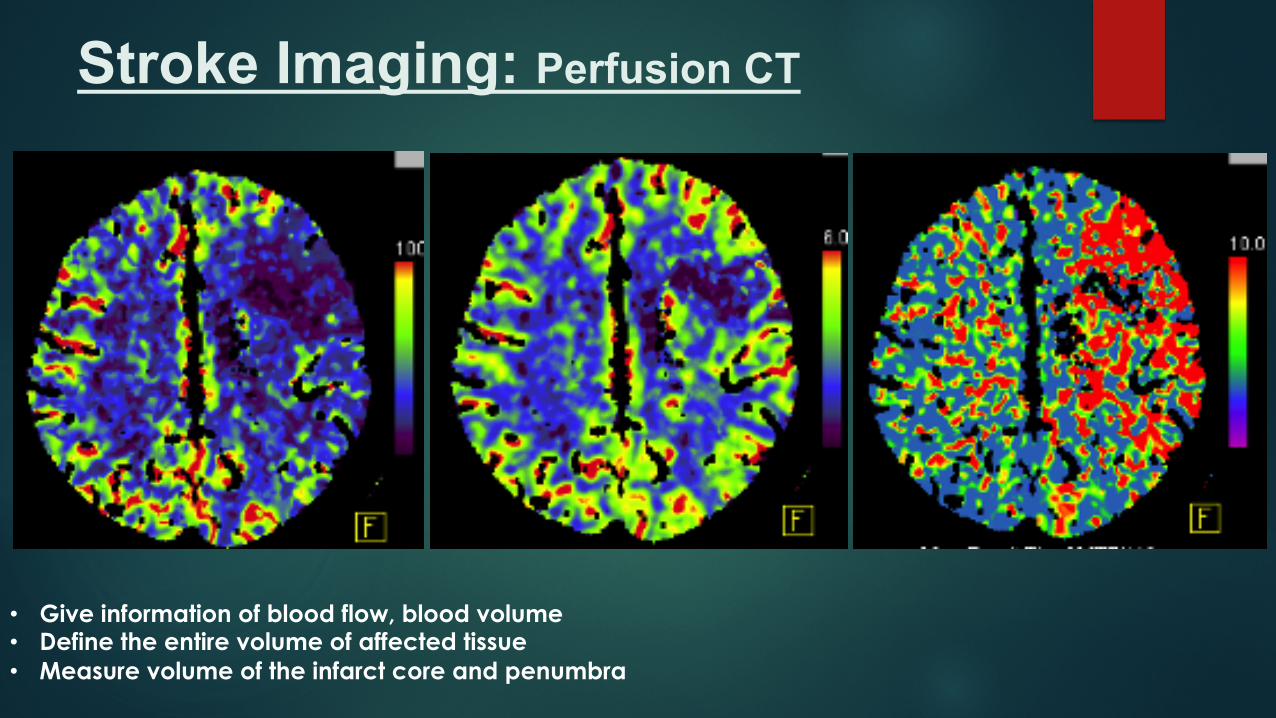
Stroke Imaging: Perfusion CT
• Give information of blood flow, blood volume • Define the entire volume of affected tissue • Measure volume of the infarct core and penumbra
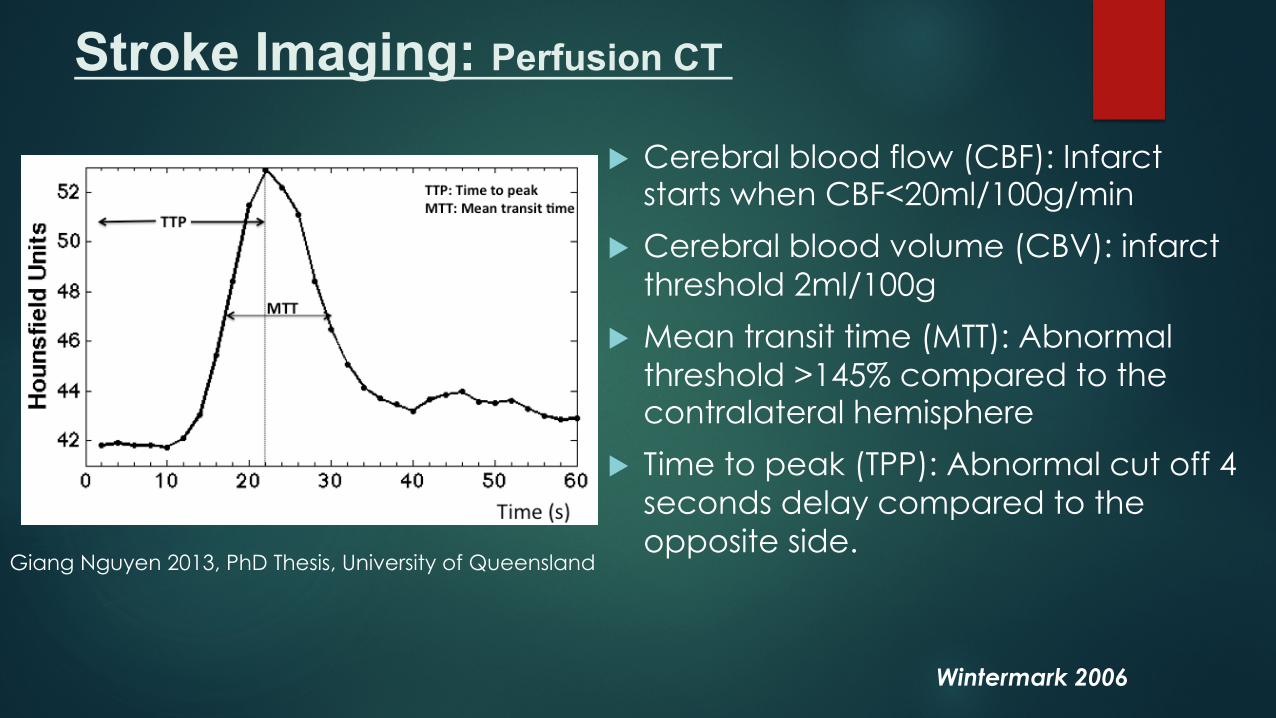
u Cerebral blood flow (CBF): Infarct starts when CBF<20ml/100g/min
u Cerebral blood volume (CBV): infarct threshold 2ml/100g
u Mean transit time (MTT): Abnormal threshold >145% compared to the contralateral hemisphere
u Time to peak (TPP): Abnormal cut off 4 seconds delay compared to the opposite side.
Giang Nguyen 2013, PhD Thesis, University of Queensland
Stroke Imaging: Perfusion CT
Wintermark 2006
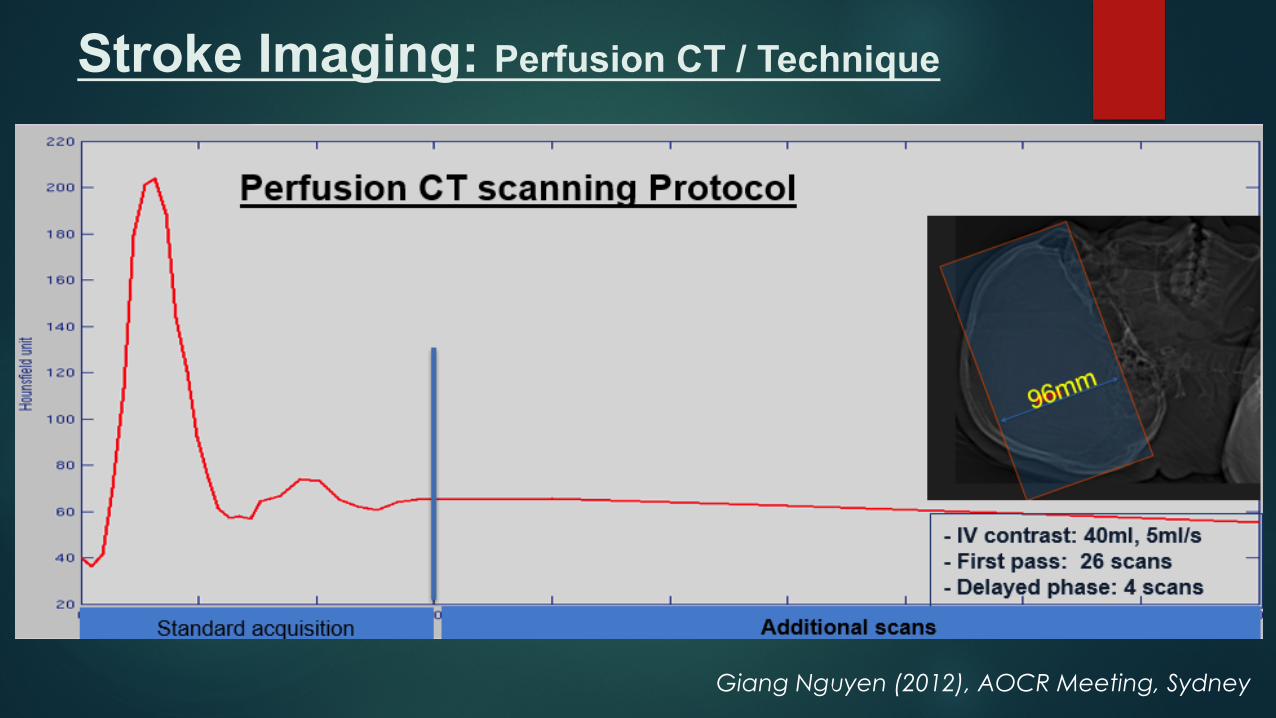
Stroke Imaging: Perfusion CT / Technique
Giang Nguyen (2012), AOCR Meeting, Sydney
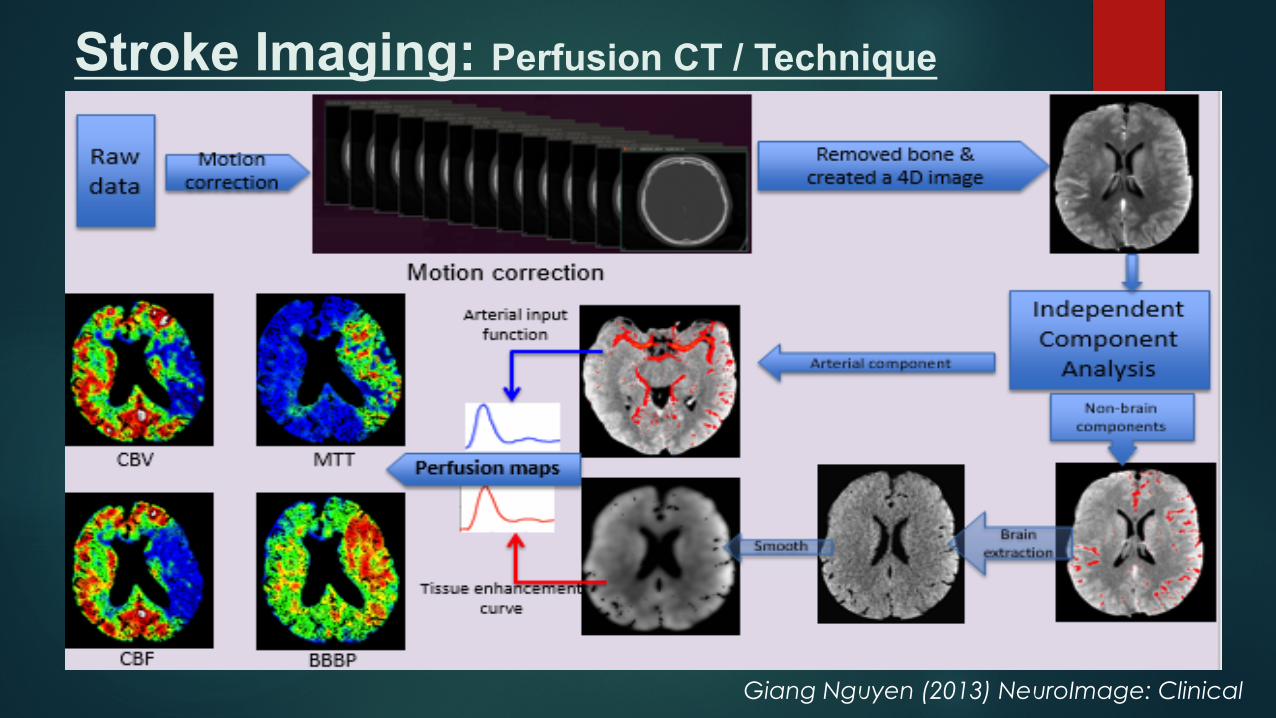
Stroke Imaging: Perfusion CT / Technique
Giang Nguyen (2013) NeuroImage: Clinical
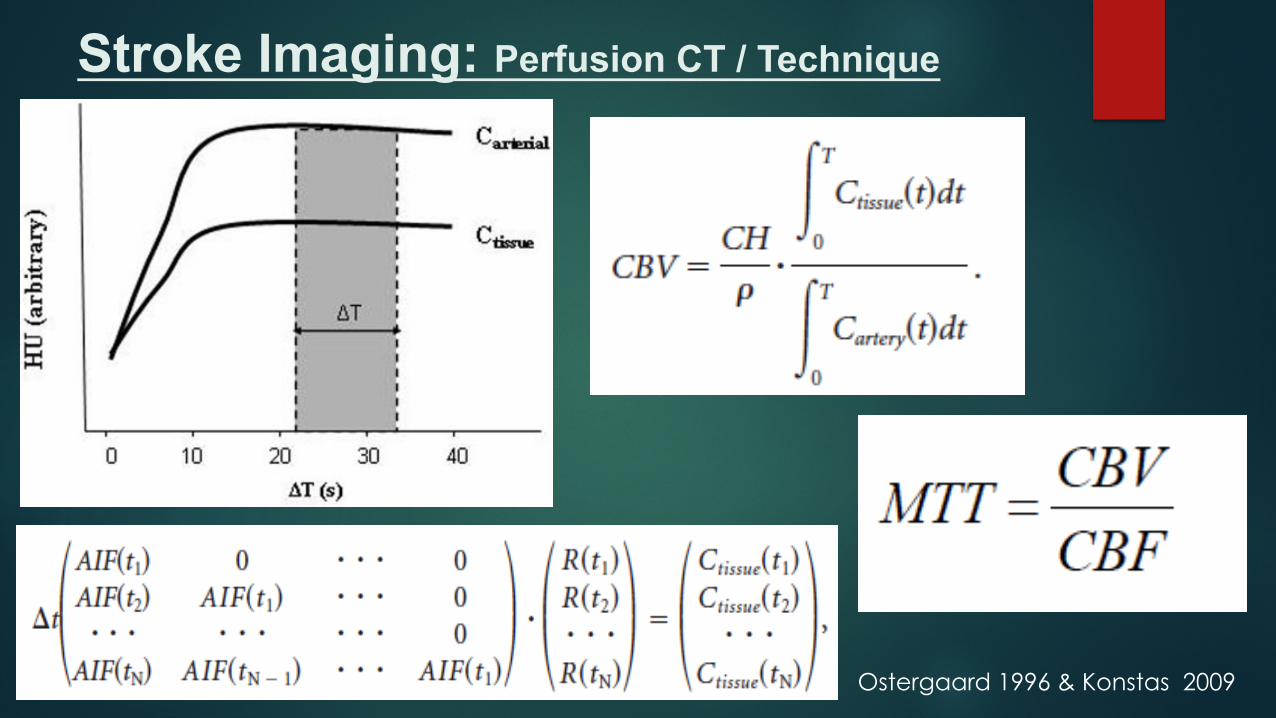
Stroke Imaging: Perfusion CT / Technique
Ostergaard 1996 & Konstas 2009
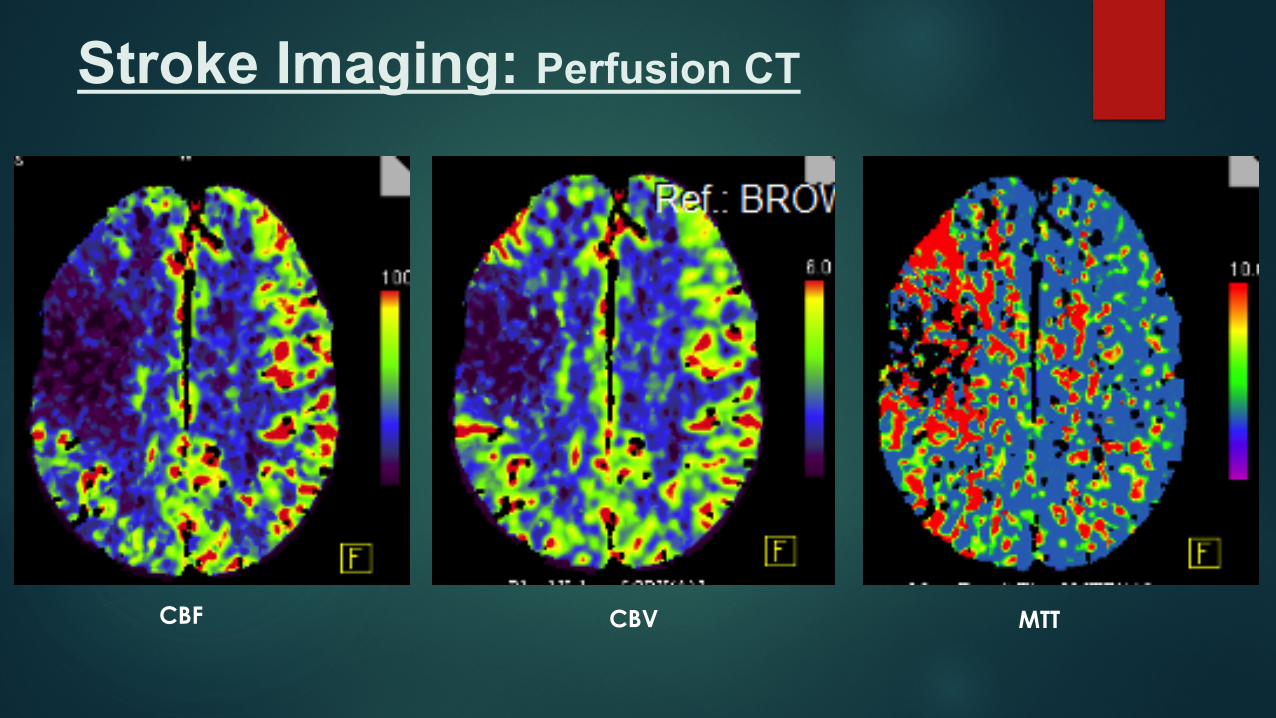
Stroke Imaging: Perfusion CT
CBF CBV MTT
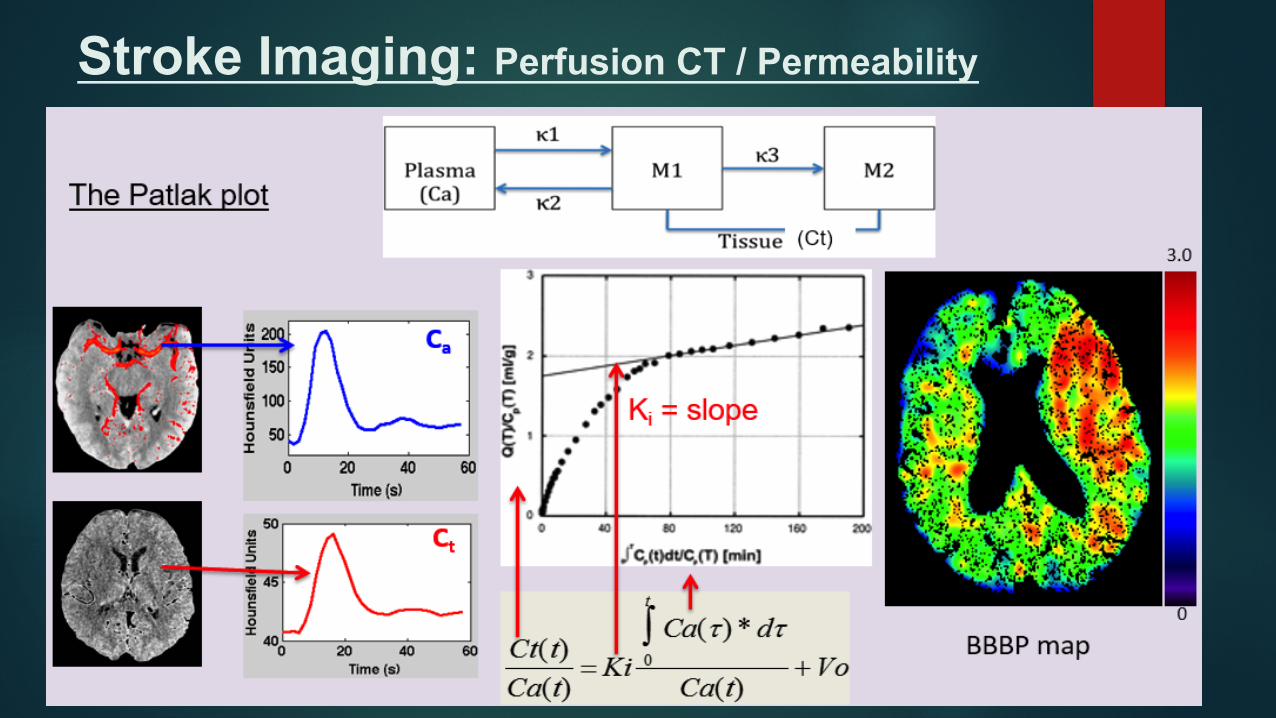
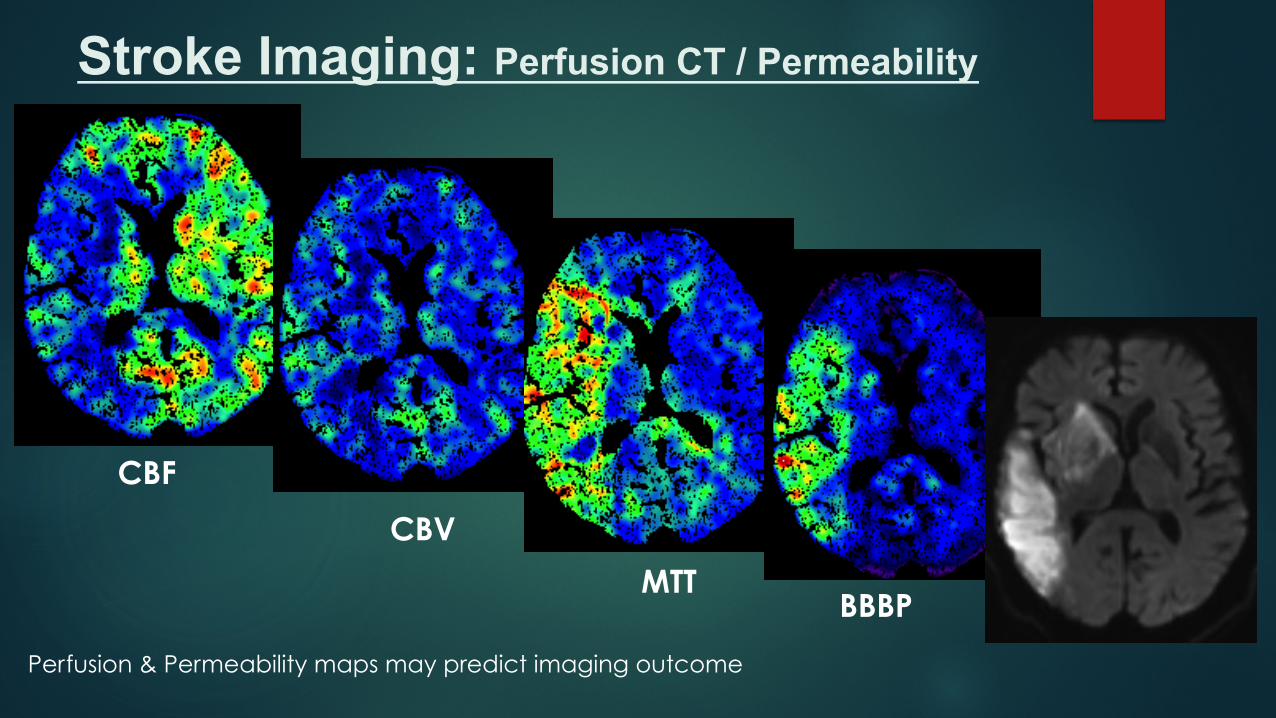
Stroke Imaging: Perfusion CT / Permeability
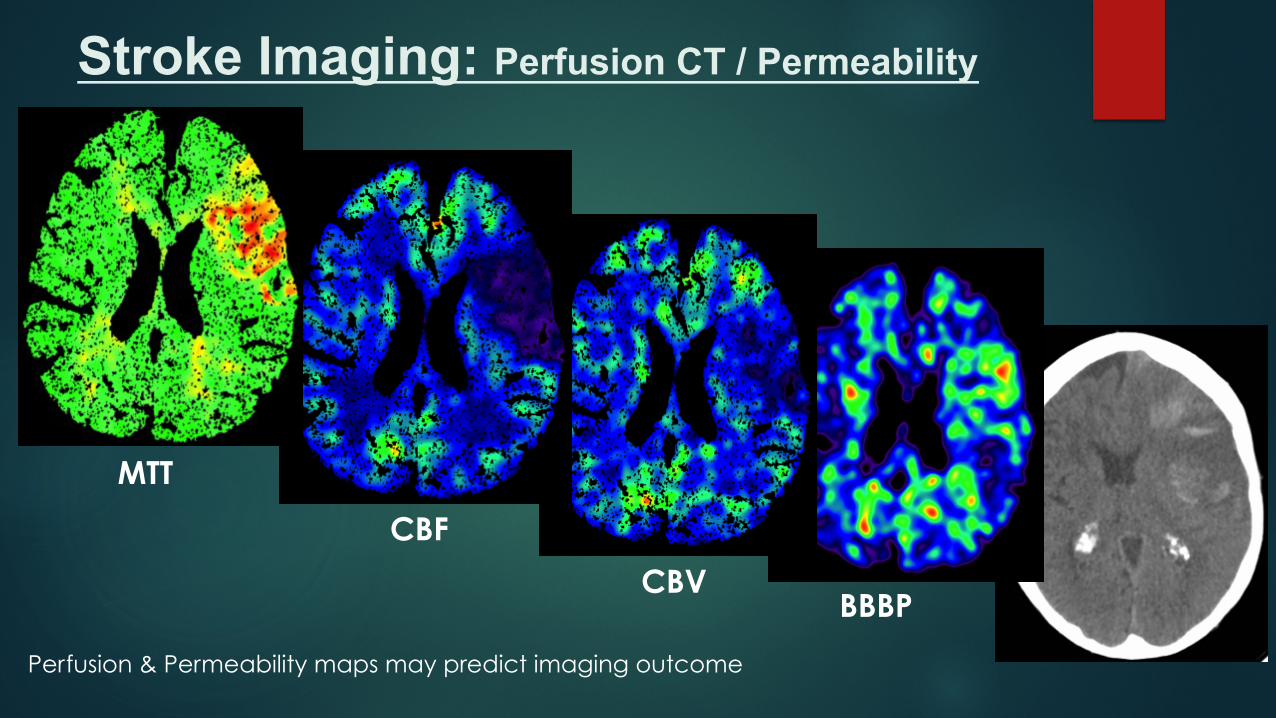
Stroke Imaging: Perfusion CT / Permeability
MTT
CBF
CBV BBBP
Perfusion & Permeability maps may predict imaging outcome
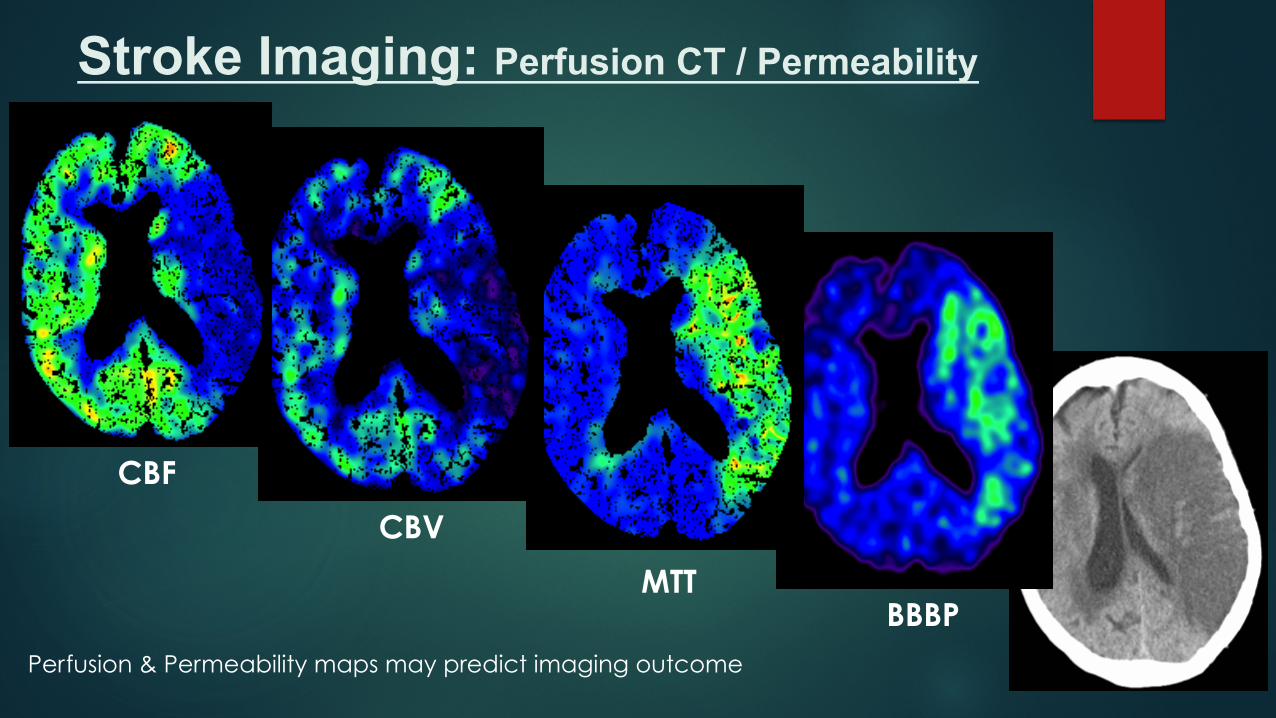
Stroke Imaging: Perfusion CT / Permeability
CBF
CBV
MTT BBBP
Perfusion & Permeability maps may predict imaging outcome
Stroke Imaging: Perfusion CT / Permeability
CBF
CBV
MTT BBBP
Perfusion & Permeability maps may predict imaging outcome
u Perfusion CT can be used in patient selection in some stroke centres • Help to measure brain perfusion & blood-brain barrier permeability
• High sensitive in detection ischaemic stroke in anterior circulation (Bivard 2013)
• May help predict complications (haemorrhage, massive oedema) (Nguyen 2013)
• Help considering recanalisation treatment
u However, current stroke guidelines have not included perfusion CT
§ Lacuna, posterior circulation lesions and reperfusion information need to be validated (Bivard 2013)
§ CBV based infarct volume may not replace DWI – MRI (Copen 2015)
§ Perfusion parameters are varied between software packages (Kudo 2013)
§ Benefit of Perfusion CT for selecting patients has not ben proven (Power 2015)
§ Further randomised studies are necessary (Power 2015)
Stroke Imaging: Perfusion CT / Permeability
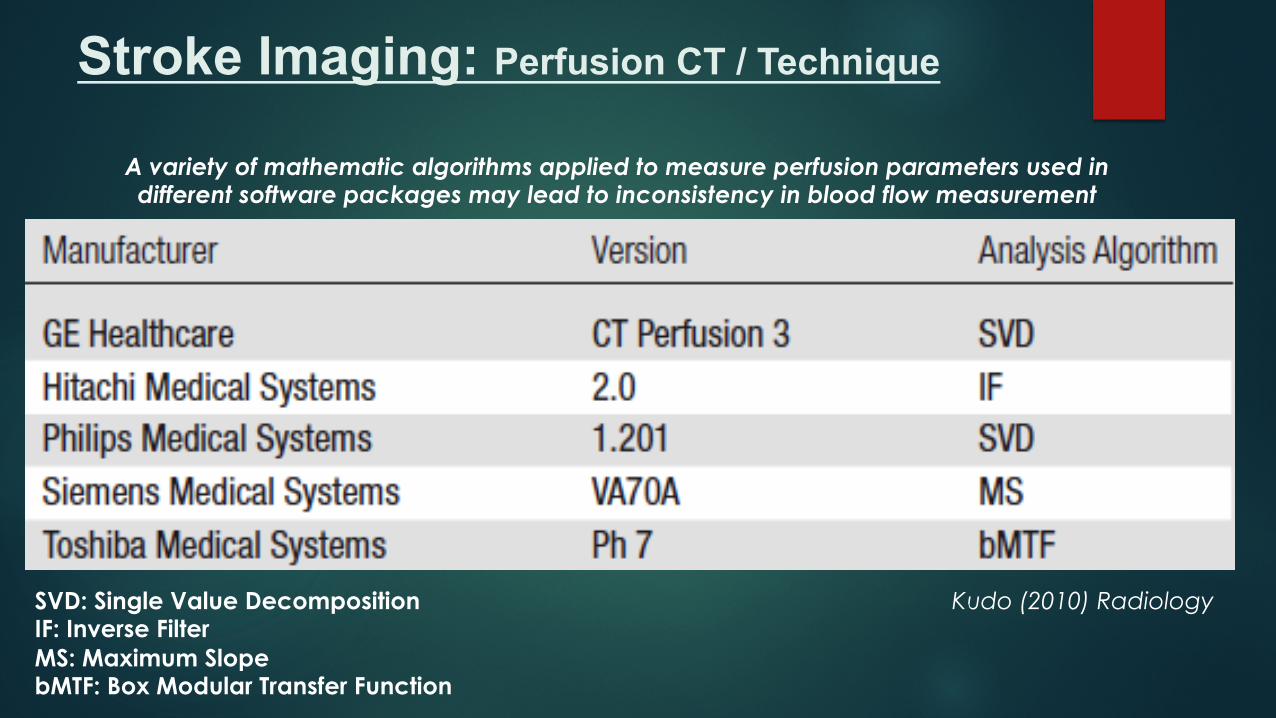
Stroke Imaging: Perfusion CT / Technique
SVD: Single Value Decomposition IF: Inverse Filter MS: Maximum Slope bMTF: Box Modular Transfer Function
Kudo (2010) Radiology
A variety of mathematic algorithms applied to measure perfusion parameters used in different software packages may lead to inconsistency in blood flow measurement
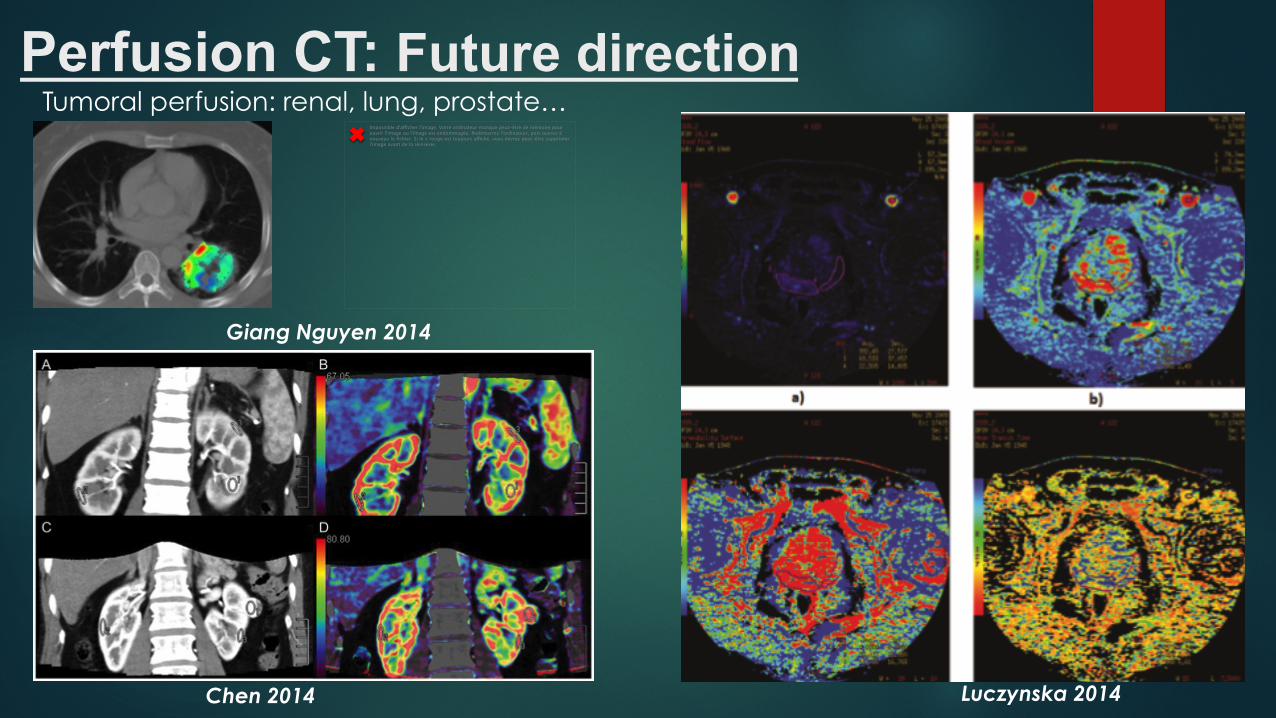
Perfusion CT: Future direction Tumoral perfusion: renal, lung, prostate…
Impossible d'afficher l'image. Votre ordinateur manque peut-être de mémoire pour ouvrir l'image ou l'image est endommagée. Redémarrez l'ordinateur, puis ouvrez à nouveau le fichier. Si le x rouge est toujours affiché, vous devrez peut-être supprimer l'image avant de la réinsérer.
Luczynska 2014 Chen 2014
Giang Nguyen 2014
Conclusion o Perfusion CT give the last 3 Ps in 4P+ in Stroke imaging: Perfusion, Penumbra
& Permeability
o Along with CT, CTA, Perfusion CT may help in patient selection for recanalisation treatment
o Perfusion CT may help to predict stroke complications and radiological outcome
o Perfusion CT may be more accessible than MRI in many stroke centres
o Software to create perfusion map needs to be consistent
o More randomised studies needed for prove benefit of perfusion CT
o Perfusion CT may be used in other body parts: lung, prostate…

Thank you!
Acknowledgement:
• Centre for Advanced Imaging, University of Queensland, Australia: David Reutens
• Royal Brisbane & Women’s Hospital, Australia:
• Alan Coulthard
• Andrew Wong
• Robert Henderson
• Dept of Radiology, Newcastle Hospital, NSW, Australia: Mark Parsons
• Thái Nguyên Central General Hospital, Vietnam
Recommended

















