04/13/23 1
NICHE Building Blocks II: Clinical Protocols
John Jorgensen, RN, MPADirector, Informatics, Auxiliary ServicesFort Sanders Regional Medical CenterKnoxville, Tennessee
Deirdre Carolan Doerflinger, CRNP, Ph.D.Geriatrics Clinical Nurse SpecialistInova Fairfax HospitalFalls Church, Virginia

04/13/23 2
Introduction
The purpose of this presentation is to provide information not only on what makes a good protocol but more over how to utilize protocols to drive improvements in the care of older adults.

04/13/23 3
Objectives
Discuss factors that influence the selection, implementation and dissemination of evidenced based clinical best practice protocols
Describe implementation strategies for successful implementation of a protocol
List at least three methods of “hardwiring” protocols

04/13/23 4
Objectives (continued)
Identify the importance of interdisciplinary collaboration for protocol implementation
Delineate strategies for addressing the challenges of measuring performance

04/13/23 5
A Protocol by Any Other Name
Protocol – “Precise guidelines with a structures and logical approach to a closely specified clinical problem” (D. Jenkins, 1991)
Procedure – “Set of action steps describing how to complete a clinical function”
Algorithms- Set of steps that approximates the decision process of and expert clinician
Clinical Practice Guidelines – “Systematically developed statements to assist the practitioner and patient decisions about appropriate health care for specific clinical circumstances (S. Wolf, 1990)
Critical Paths – Multidisciplinary approach that guides the nurse in what to do and when

04/13/23 6
NICHE Protocols Research based clinical practice protocols for
specific geriatric syndromes Help the nurse prevent, recognize and treat clinical
conditions seen frequently in elders Common Geriatric syndromes and/or other Clinical
Issues for hospitalized older adults are:
Pressure Ulcers
Advance Directives
Adverse Drug Events
Falls
Physical Restraint Use
Pain Nutrition-Weight Loss
Delirium
Sleep Disturbance
Dementia Discharge Planning
Functional Decline
Incontinence Depression
Capezuti, E., Zwicker, D., Mezey, M., Fulmer, T., Gray-Miceli, D., and Kluger, M. (Eds.). (2008). Evidence-based geriatric nursing protocols for best practice (3rd edition). New York: Springer Publishing Company

04/13/23 7
Influential Factors For Protocol Adoption The high level view of the process
includes: Recognition Selection of appropriate
evidenced based practice (EBP) protocols
Adoption/Implementation Hardwiring the protocol

04/13/23 8
Step One: Recognition
Takes many forms As simple as clinical area identifying
areas of practice concerns/patient outcomes Must be data driven
As robust as using an assessment tool such as the Geriatric Institutional Assessment Profile (GIAP) to identify areas for needed improvement

04/13/23 9
Step Two: Selection of the EBP Protocol Many well researched protocols
are available Why are they not used even when
there is clear evidence of their effectiveness? Social influence theory Transtheoretical model Diffusion of innovation theory

04/13/23 10
Social Influence Theory
Social influence theory posits that behavior of one person influences others as to how they respond, feel and think about change. (Zinbardo, Leippe, 1991)
– decisions and actions are strongly guided by prevailing practice, social norms, economic pressures and the habits, customs and values held by peers (Mittman, 1992)

04/13/23 11
Transtheoretical Model Transtheoretical model – identifies 5
stages involving movement from knowledge and attitudinal change to action phrases where emotional and positive reinforcement need to occur and finally to practitioners adapting to the behavior enters a maintenance phase where the behavior is self sustaining as long a social support and reward systems are in place (Rogers, 1995).

04/13/23 12
Diffusion of Innovation Theory
Diffusion of innovation theory posits that change occurs when a small group of innovators believe strongly that adoption of a protocol will improve patient care. This “change idea” then passes from the innovators to the “early adopters” and the idea takes off. (Rogers, 1995)

04/13/23 13
Step Two: Selection of the EBP Protocol Involve end users from outset, enlist
ownership Involve key players
“Nay sayers” Champions
Be flexible - may need to incorporate EBP into own protocol
Lobby, lobby, lobby! Present opportunities individualized to
specific audience

04/13/23 14
Step 3: Implementation Successful implementation
dependent upon recognition of factors which inhibit and encourage protocol adoption. Qualities
ProtocolHealthcare professionalPractice setting
Incentives for adoption Regulatory requirements

04/13/23 15
Step 3: Implementation
Tips Place protocols in easily accessible
location Use pocket cards with bullet points
or checklists Computer prompts Use of trigger cards such as
SPICES mnemonics (Fulmer, 1991)

04/13/23 16
Step 3: Implementation Considerations
Determine opinion leaders (nurse managers or credible staff person) – gain their support
Clinician factors such as age, training, knowledge base in protocol domain
Irrational forces – fear, anxiety and resistance to change all tied to beliefs about self-efficacy
Are the protocols too rigid

04/13/23 17
Step 3: Implementation
Publicize in every possible forum: you never know where you will find
a new champion! No surprises, no matter how
insignificant Know your measurement
mechanism going in

04/13/23 18
Step 4: Hardwiring
Continual review of outcomes Education
New staff Annual review
Competency Training Monitoring use of the protocol

04/13/23 19
Strategies for Successful Protocol Implementation – Administrative Support 8 of the top 10 barriers to using research
findings in practice are related to the work environment and the organizational process Lack of authority Little support from other staff and
physicians Management refusal Insufficient time
These barriers are directly influenced by management

04/13/23 20
Strategies for Successful Protocol Implementation – Committee/Council Prevailing organizational culture (customs,
attitudes, beliefs) must support protocol adoption and implementation
Teams are at the very root of this culture Utilize teams as the base units for change
Staff survey as to key geriatric syndromes
Manager conducts interviews to collect commentary to determine priorities
Annual goal setting Unit staff and manager work
collaboratively to establish goals, set action plans and assigned specific tasks to complete
Unit progress monitored – staff become experts

04/13/23 21
Strategies for Successful Protocol Implementation – Social Influence Strategies
The most crucial factor for successful protocol implementation is the use of multifaceted strategies (Kaluzney et al., 1995; Oxman et al., 1995; Solberg et al., 2000.

04/13/23 22
Strategies for Successful Protocol Implementation – Social Influence Strategies Catalogues of strategies to meet
specific to the situation seem most appropriate Must fit desired behavioral
change Practitioner type Technologies in use

04/13/23 23
Strategies for Successful Protocol Implementation – Social Influence Strategies
Social influence strategies useful in healthcare setting Use of opinion leaders (excellent
staff clinicians, APRNs, nursing school faculty members, outside experts)
Performance improvement Study groups Patient care rounds Participatory guideline development

04/13/23 24
Strategies for Successful Protocol Implementation - Consultants Wherever possible involve internal
consultations and involve them on patient care teams Pharmacy for poly pharmacy Therapies for skin care, mobility,
discharge planning SLPs for swallowing protocols Risk management for elopement
Involve outside consultants to assess, kick off your program and to evaluate progress GIAP services provide valuable
information on institutional attitudes, education and practice

04/13/23 25
Strategies for Successful Protocol Implementation – Models of Care Fit strategies to the model of care being
used. Geriatric Resource Nurse (GRN) Model
Experts on each unit guide protocol development
Acute Care for Elderly (ACE) Protocol development for distinct unit
Social influence strategies remain in play regardless of care model

04/13/23 26
Hardwiring Protocols – Sustaining Behaviors Promote compliance with creative
rewards and incentives Friendly competition between units Use of awards for unit with best
project – See NICE AWARD Reports at leadership on nursing unit
performance Falls rates Skin care stats Documentation screening on
admission, assessments and interventions for pain and patient discharge planning.
Regular study groups, sensitivity training, monthly rounds, Games that increase knowledge

04/13/23 27
Hardwiring Protocols – Sustaining Behaviors Use of special training for opinion
leaders who become the role models when training of all staff is initiated
Case presentations Huddles where there is a short meeting
to identify patient issues and communicate to all team members
Consider educating consumers through public relations Knowledge of best practice empowers
consumers to make choices that are more informed
A way to evaluate appropriateness of care

04/13/23 28
Hardwiring Protocols – Sustaining Behaviors
New employee education should include information on the protocol & its justification for use
Extends to floats & temporary employees Cover the critical protocols of fall
prevention, restraint use and management of difficult behaviors
Incorporate this training into annual competency training for all staff to reinforce and sustain the behavior change
Titler and colleagues suggest “reinfusion” of evidenced-based practice by developing a plan of systematically reintroducing the protocol and monitoring its use.

04/13/23 29
Hardwiring Protocols – Sustaining Behaviors
Agreed upon documentation can be embedded into the electronic medical record Prompts & screen lay out are critical to success Education of staff on use of screens critical Constant monitoring via clinical electronic query
provide leadership with information on performance
A variety of EBP tools can be incorporated Alerts can be sent to various disciplines: for
abuse, frail elder consults, pharmacy consults for med reconciliation, functional assessment screening can trigger therapy involvement and fall event data tracked more efficiently to reduce incidence.

04/13/23 30
Interprofessional Collaboration The goal of protocol implementation is to
ensure the actual use of the protocol. Involvement of disciplines requires a
common language and documentation that transcends petty fiefdoms within the traditional bureaucratic structure of health care organizations
Intra professional teams can be formed to work jointly on issues common to all
Clear examples include skin care, fall prevention, pain management, restraint reduction and preventing the hazards of immobility

04/13/23 31
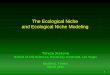
Approach Deployment Results
(1) Reacting To Problems (2) Early Systematic Approach
(3) Aligned Approach (4) Integrated Approach
Steps Toward a Mature Process Approach

04/13/23 32
Measuring Performance (Quality is in the eye of the beholder) Different interests for multiple
users a key challenge Stakeholders
Internal• Administration• Clinical staff• Quality department
External• Regulatory agencies• Consumers – Health grades, CORE
Measure information

04/13/23 33
Measuring Performance (Quality is in the eye of the beholder) (cont’d) Must use acceptable measurement tools
where care measures are identified and standardized with a common measurement language grounded in shared perspectives on quality across groups and disciplines.
Once systems are in place data must be collected: Logistical issues of collecting,
recording, reporting and managing data
Data must be analyzed in statistically appropriate ways
Health care environments are different and change frequently – finding common denominators is a major hurdle

04/13/23 34
Measurement Tools Assessment phase findings - Data
allergies Collecting data without:
Knowing why Seeing results Developing findings and conclusions
Cataloging monitoring activities to Determine if they are truly needed What / where they get reported Are there actionables Who is the owner so that collection
can readily be accessed –important o these days of continuous readiness.

04/13/23 35
Characteristics of Good Measurement Tools
Characteristics of good performance measures Usefulness
What do we need to know? How do we intend to use the performance
measure and can it be used this way? Targets improvement now, in the past and for
the future Precisely defined – clear operational definitions Validity – does the measure measure what it is
intended to measure? Sensitivity – ability to capture the “true” cases of
the event being measured (false positives) Specificity – The likelihood of a negative test
when the condition is actually present – indicates low specificity.

04/13/23 36
Characteristics of Good Measurement Tools
Characteristics of good performance measures (cont’d) Reliability – Results that are reproducible and
consistent indicate high reliability. Interpretable – the degree to which it conveys
a result that can be linked to the quality of clinical care.
Risk-adjusted – Some patients are sicker than others some have co morbidities, some older and more frail. – create level playing field
Easy to collect – Easily retrievable data with little burden – goal quick and good rather than quick and dirty!
In control – must reflect the practice being observed and must be within the control of the practitioner

04/13/23 37
Data Collection Methods Standard chart review Clinical Query in which the
documentation database can be queried for specific elements
Direct observation Interviews
Staff Patients Physicians
Tracers – essentially and interview and record review all in one

04/13/23 38
Analysis / Interpretation /Reporting Results -Begins with taking data
and organizing it into categories Could be hierarchical Based on a structural taxonomy
Findings – Taking results to the next level that speak to the outcomes of the results
Conclusions – An overview of findings for use in future projects or as predictors for future activities.

04/13/23 39
Healthcare Change / Differences / Considerations
Healthcare is dynamic and change occurs frequently
There is movement of care from one setting to another
Frequent introduction of new technology Even within supposed integrated health
care delivery systems there is often a lack of standardized processes between facilities
Also exists a new public awareness where there is a desire to see outcome data prior to undergoing procedures or being admitted to a particular facility

04/13/23 40
Summary Elder focused practice protocols have the
potential to improve patient care by fostering clinical decision making based on best practice geriatric nursing standards
Administrative commitment and a comprehensive organizational strategy are pivotal.
Pay close attention to how and what protocols are developed
Recognize/publish small successes in winning additional support
Remember imagination, courage and love are positive drivers for change.
Recommended