Opportunity's of Personalised
Medicine for Health Insurance
Madelon Johannesma, Msc, PhD
Health Insurance company CZ
26-6-2017
2
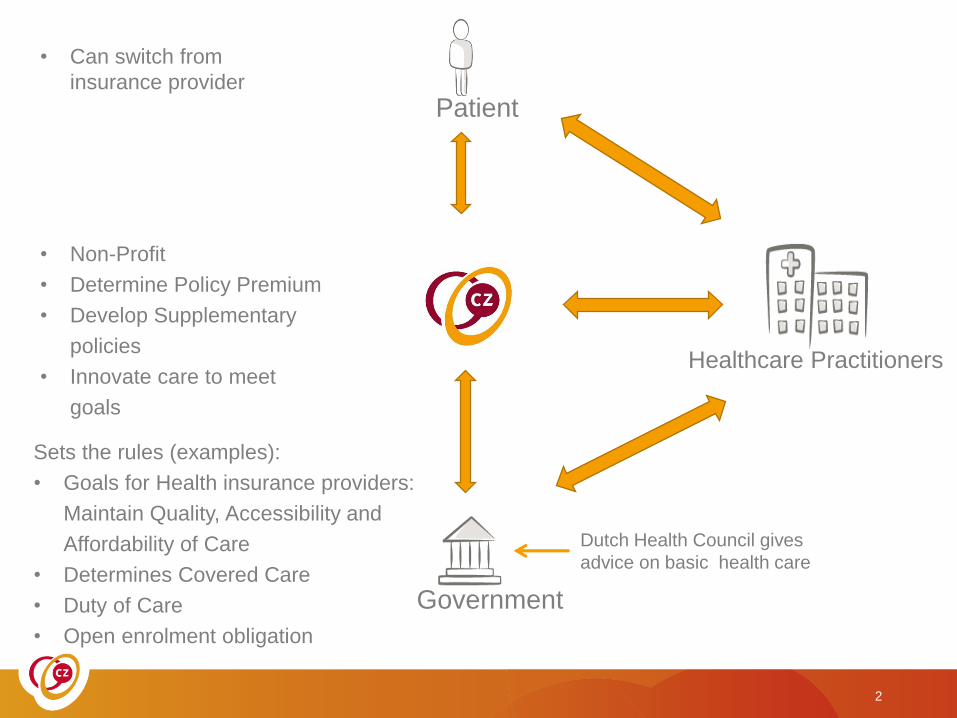
Healthcare Practitioners
Government
Sets the rules (examples):
• Goals for Health insurance providers:
Maintain Quality, Accessibility and
Affordability of Care
• Determines Covered Care
• Duty of Care
• Open enrolment obligation
• Non-Profit
• Determine Policy Premium
• Develop Supplementary
policies
• Innovate care to meet
goals
• Can switch from
insurance provider
Patient
Dutch Health Council gives
advice on basic health care

3
There are a lot of providers in The Netherlands….

CZ-group is third largest Dutch health insurer
4
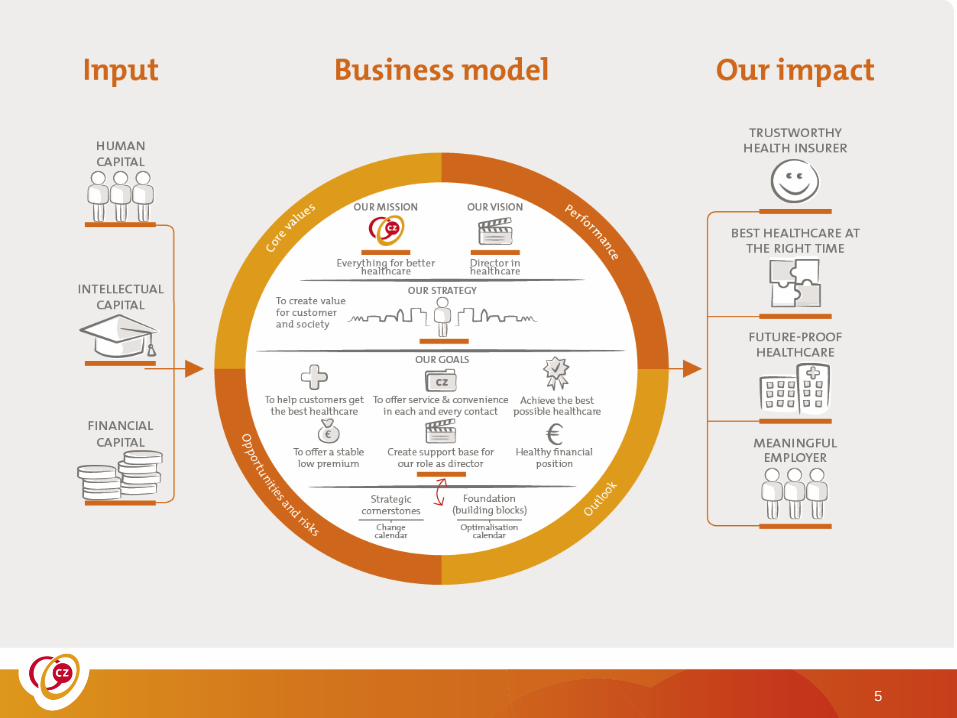
5
CZ defines ‘the best possible care’ as care which
creates the most patient value
6
Founding father of
the concept of ‘value’
is Michael E. Porter
Value is defined as
Quality
------------
Cost
Health Care Costs are rising exponentially
7
…and as a consequence the premium
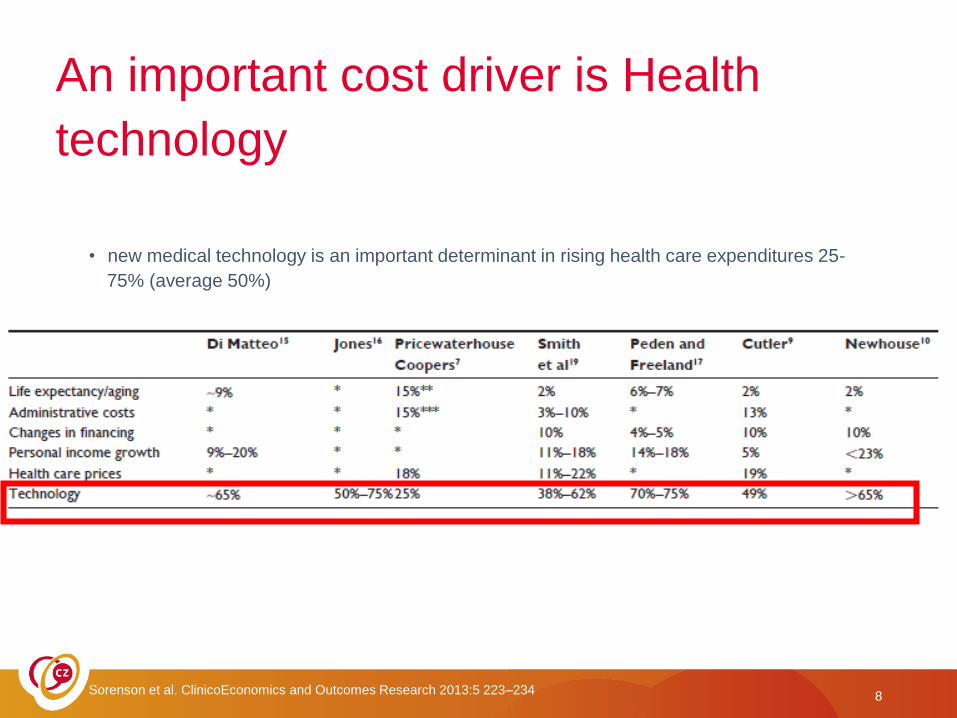
An important cost driver is Health
technology
Sorenson et al. ClinicoEconomics and Outcomes Research 2013:5 223–234
• new medical technology is an important determinant in rising health care expenditures 25-
75% (average 50%)
8
A new treatment/technology is considered to be
accepted as compared to standard treatment if:
Trade off
• Better survival rates
• and/or a better QoL
• Acceptable costs
Determined by the Dutch Health Counsil for basic health care
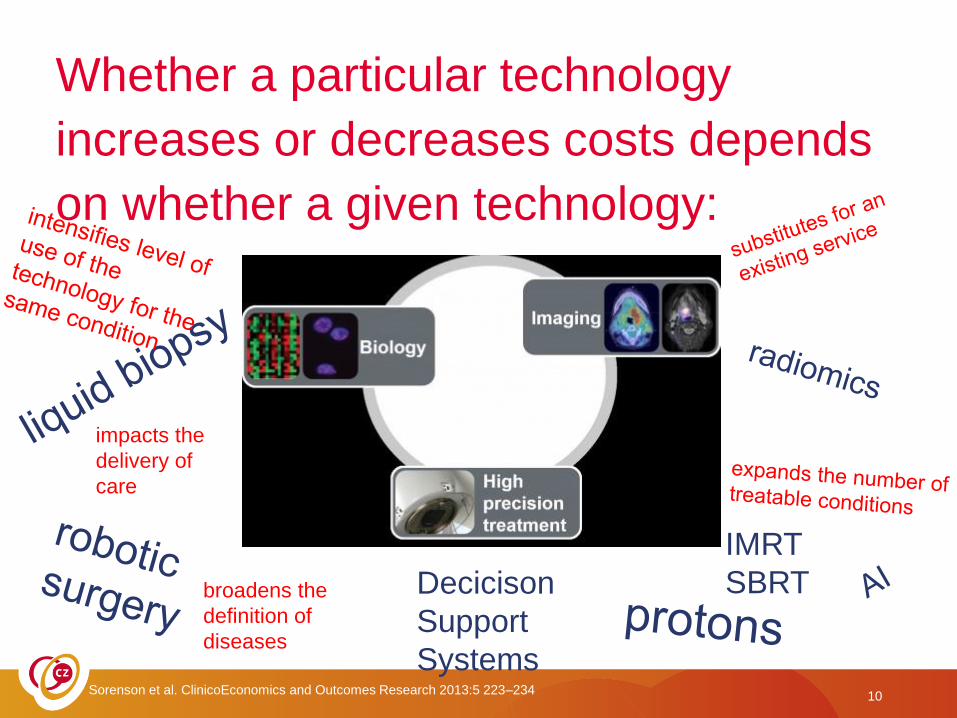
Whether a particular technology
increases or decreases costs depends
on whether a given technology:
Decicison
Support
Systems10
impacts the
delivery of
care
broadens the
definition of
diseases
IMRT
SBRT
Sorenson et al. ClinicoEconomics and Outcomes Research 2013:5 223–234
Economic evaluation
• ‘The comparative analysis of alternative courses of
action in terms of both their costs and their effects’.
• (Drummond et al., 1996)
courtesy Bram Ramaekers, MUMC+ (all slides about economic evaluatie)
Value for moneyQALY
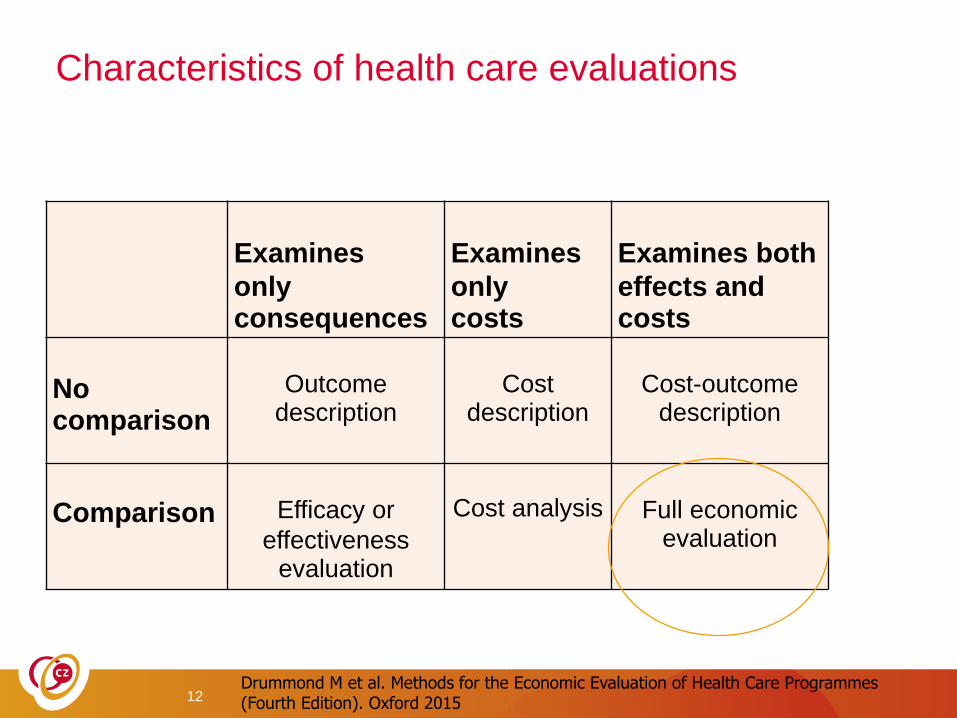
Characteristics of health care evaluations
Examines
only consequences
Examines
only costs
Examines both
effects and costs
No comparison
Outcome description
Cost description
Cost-outcome description
Comparison Efficacy or
effectiveness evaluation
Cost analysis Full economic evaluation
12Drummond M et al. Methods for the Economic Evaluation of Health Care Programmes(Fourth Edition). Oxford 2015
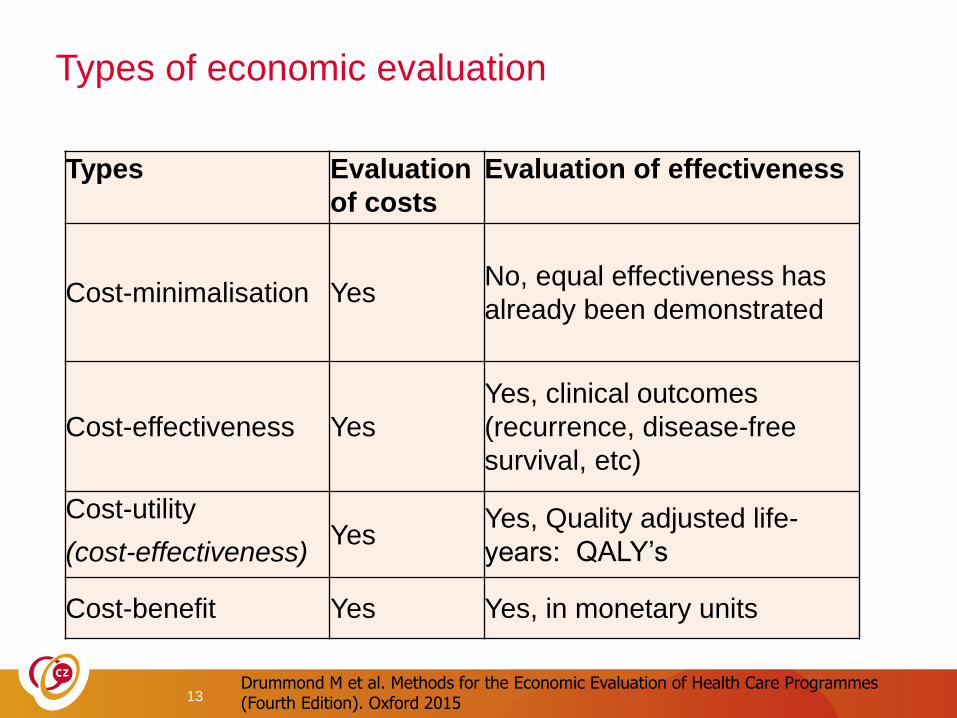
Types of economic evaluation
Types Evaluation
of costs
Evaluation of effectiveness
Cost-minimalisation YesNo, equal effectiveness has
already been demonstrated
Cost-effectiveness Yes
Yes, clinical outcomes
(recurrence, disease-free
survival, etc)
Cost-utilityYes
Yes, Quality adjusted life-
years: QALY’s(cost-effectiveness)
Cost-benefit Yes Yes, in monetary units
13Drummond M et al. Methods for the Economic Evaluation of Health Care Programmes(Fourth Edition). Oxford 2015
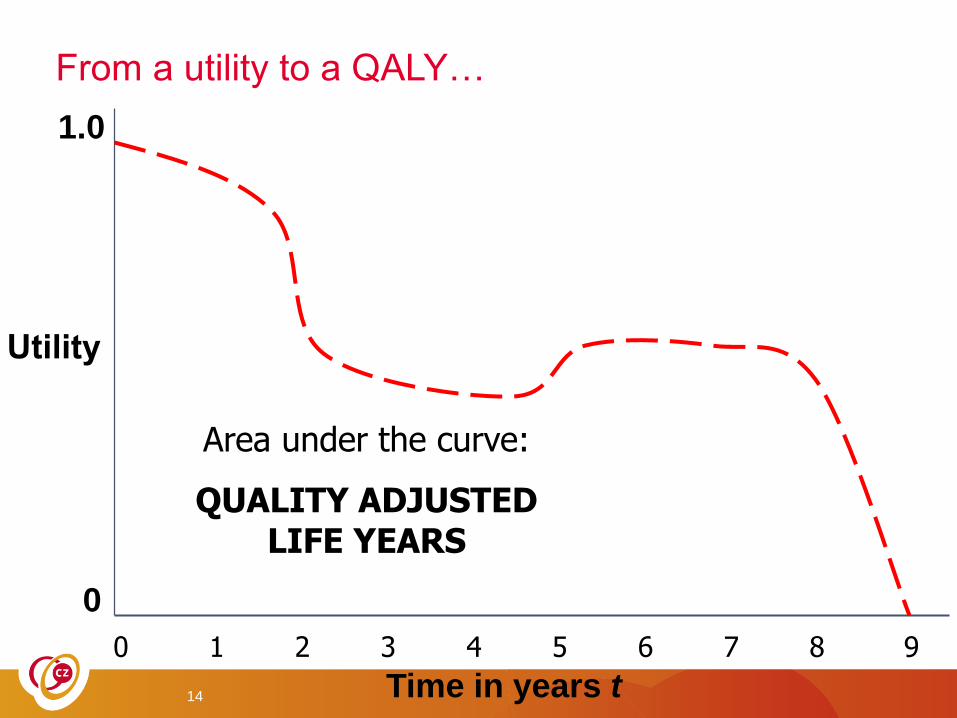
From a utility to a QALY…
14 Time in years t
0
1.0
Area under the curve:
QUALITY ADJUSTED LIFE YEARS
0 1 2 3 4 5 6 7 8 9
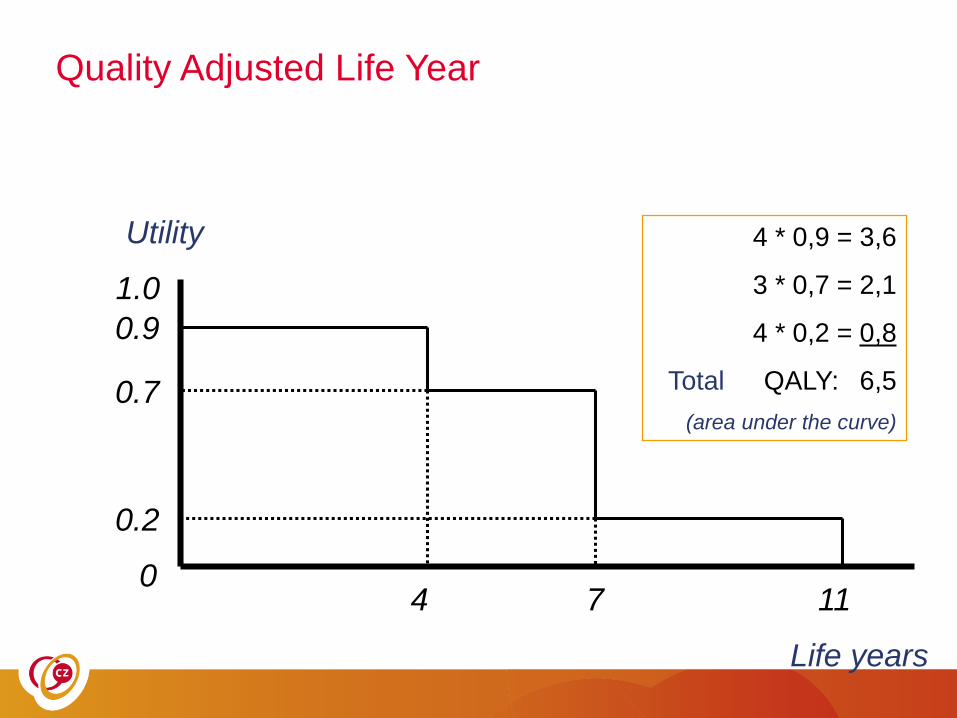
Quality Adjusted Life Year
Life years
0
1.0
Utility
4 7
0.9
0.7
0.2
11
4 * 0,9 = 3,6
3 * 0,7 = 2,1
4 * 0,2 = 0,8
Total QALY: 6,5
(area under the curve)
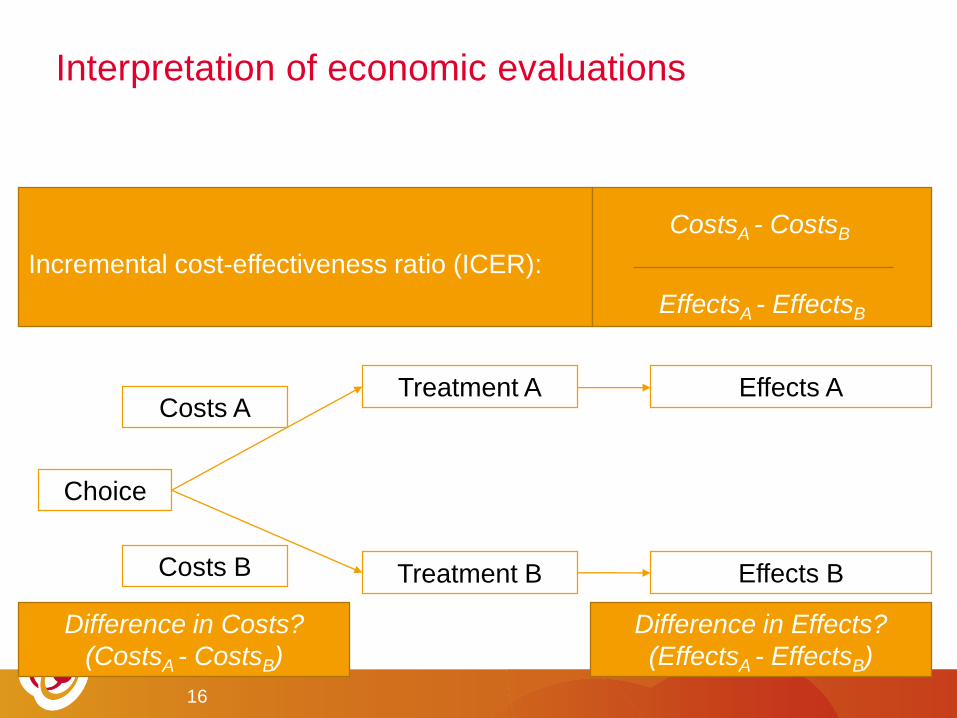
• Multiple alternatives
• Considering both Costs and Effects
Interpretation of economic evaluations
Effects ACosts A
Choice
Treatment A
Costs B Treatment B Effects B
Incremental cost-effectiveness ratio (ICER):
CostsA - CostsB
EffectsA - EffectsB
16
Difference in Costs?
(CostsA - CostsB)
Difference in Effects?
(EffectsA - EffectsB)
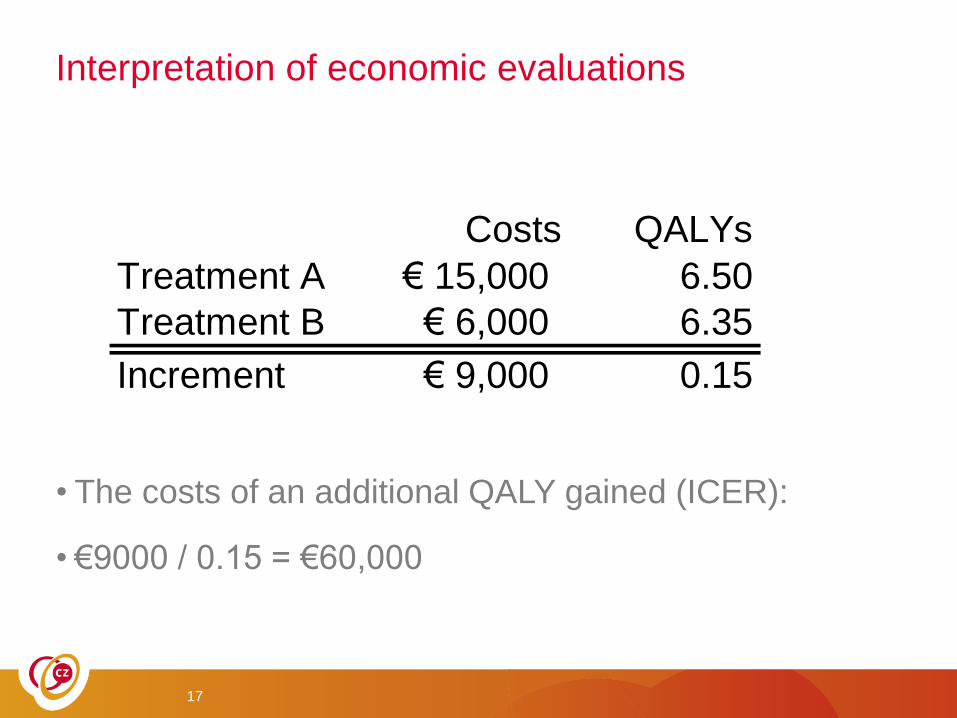
Interpretation of economic evaluations
• The costs of an additional QALY gained (ICER):
• €9000 / 0.15 = €60,000
17
Costs QALYs
Treatment A € 15,000 6.50
Treatment B € 6,000 6.35
Increment € 9,000 0.15
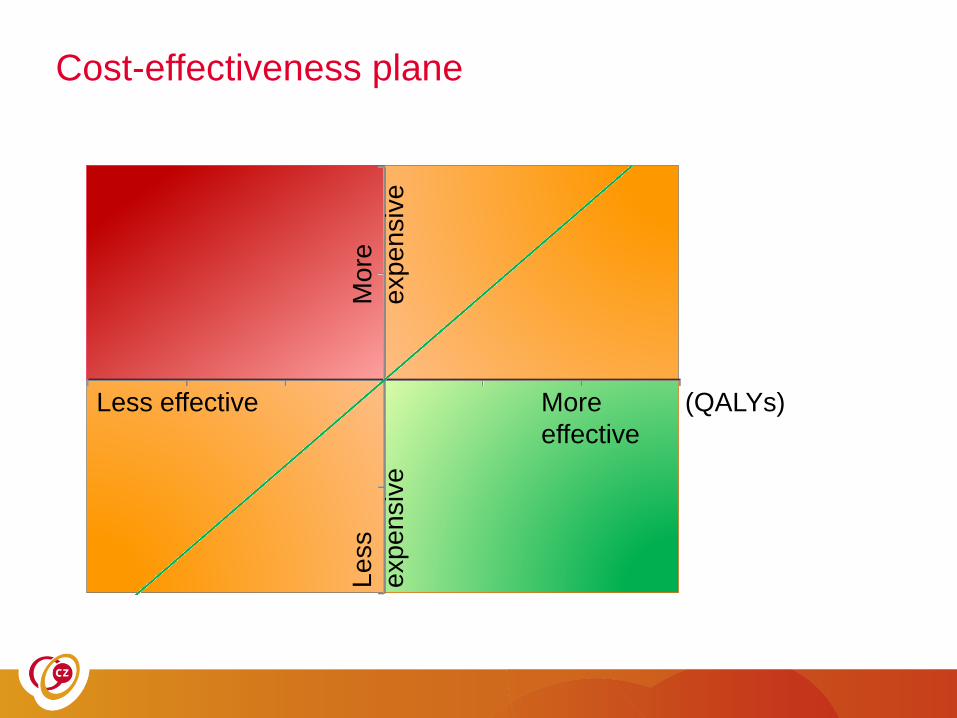
Cost-effectiveness plane
More
effective
Less effective
Mo
re
exp
en
siv
e
Le
ss
exp
en
siv
e(QALYs)
18
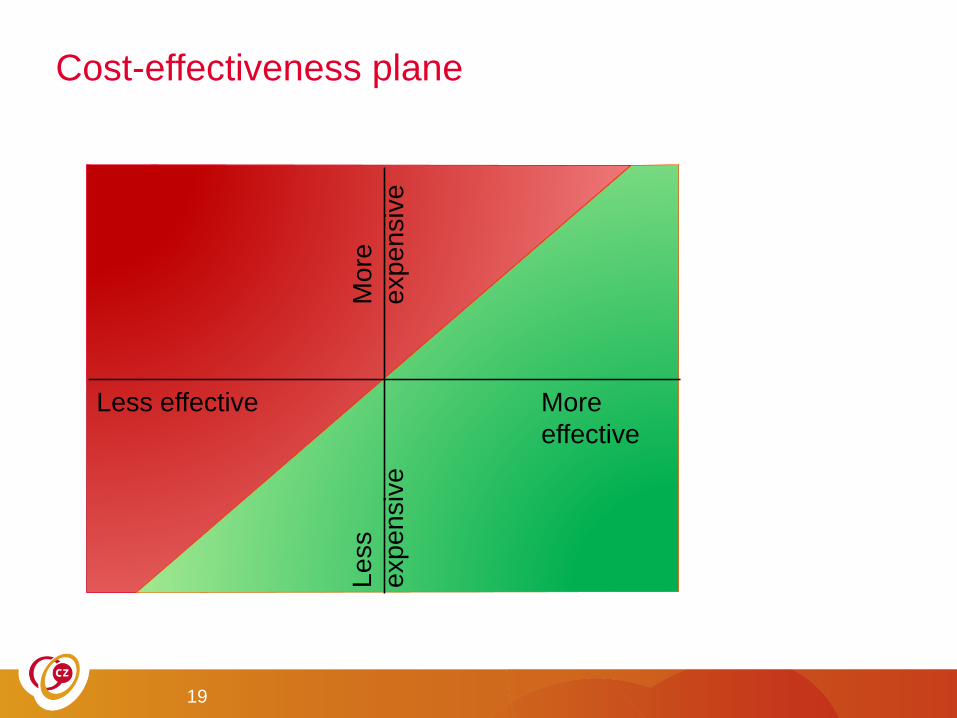
Cost-effectiveness plane
More
effective
Less effective
Mo
re
exp
en
siv
e
Le
ss
exp
en
siv
e
19
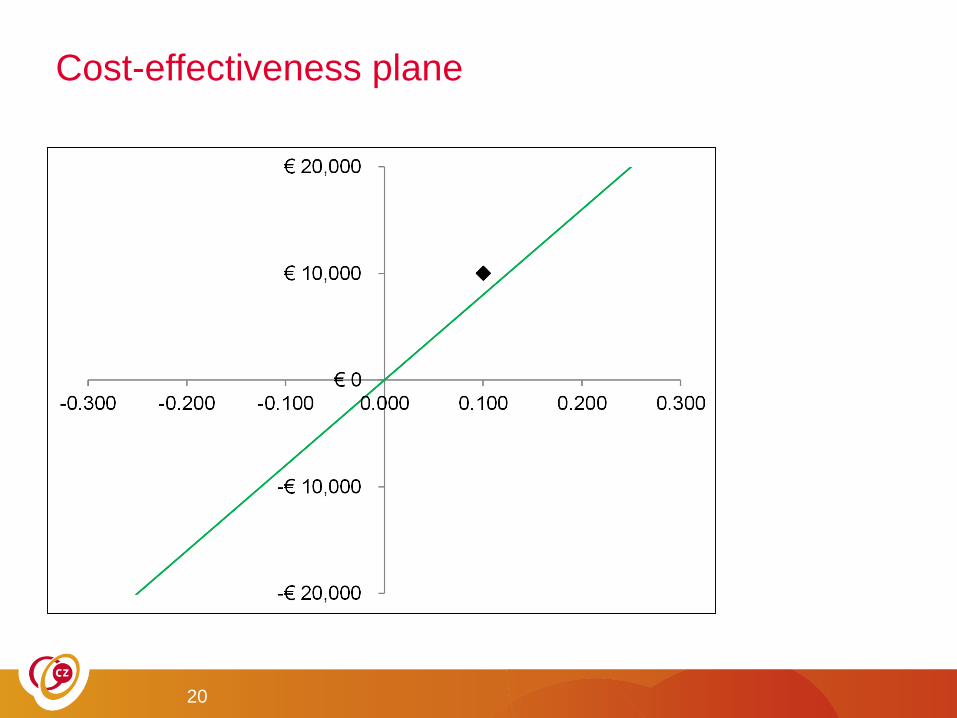
Cost-effectiveness plane
20
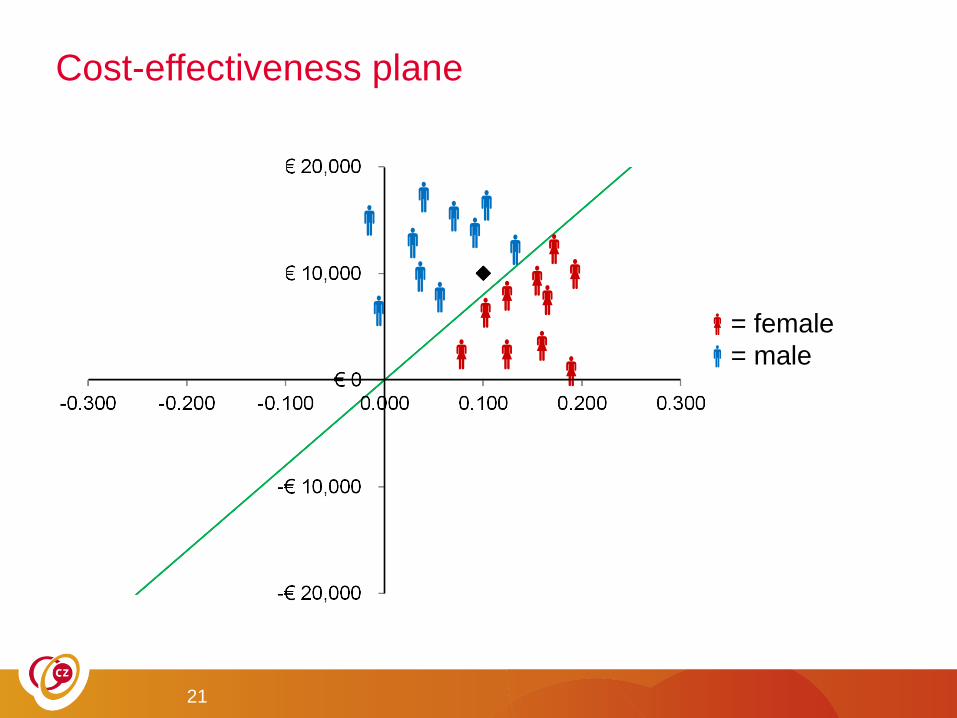
Cost-effectiveness plane
= female
= male
21
Health economic evaluation
• Reimbursement decisions
• Implies valuing the worth of a QALY
• Example nivolumab for metastatic lung cancer in NL
• Gain: 3 months
• €134,000 per QALY gained
• Budget impact €200 million per year
• Dutch Health care institute: too expensive (Dec 2015)
• Minister of Health (Schippers) agreed
• Dutch Cancer Society: impermissible to restrict access for financial
reasons (Dec 2015)
22
23
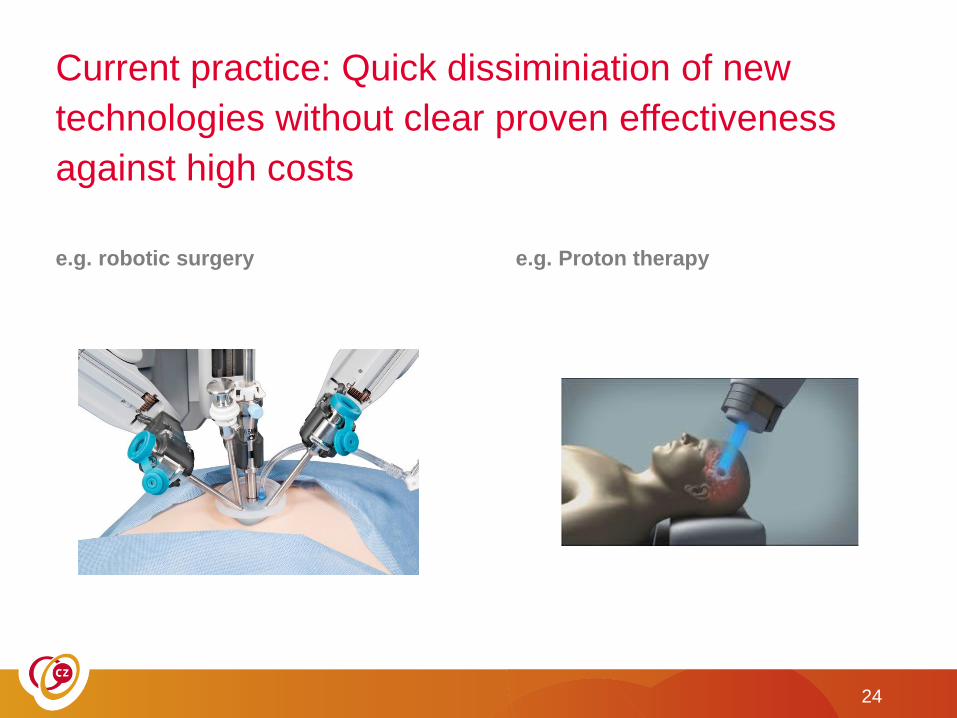
Current practice: Quick dissiminiation of new
technologies without clear proven effectiveness
against high costs
e.g. robotic surgery e.g. Proton therapy
24
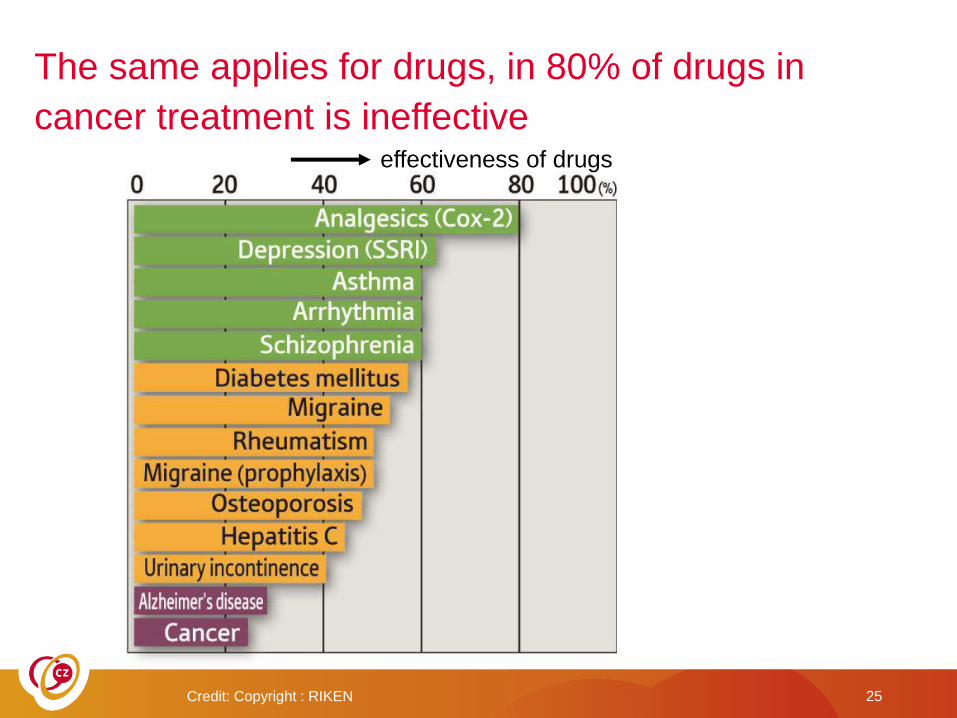
Credit: Copyright : RIKEN 25
effectiveness of drugs
The same applies for drugs, in 80% of drugs in
cancer treatment is ineffective

As a consequence….
Unnecessary treatment related side effects
Wast of health care! inefficient!
26
Every patient is unique, however….
27
The average patient doesn’t exist !
Guidelines are based on the
average patient, but…..
28
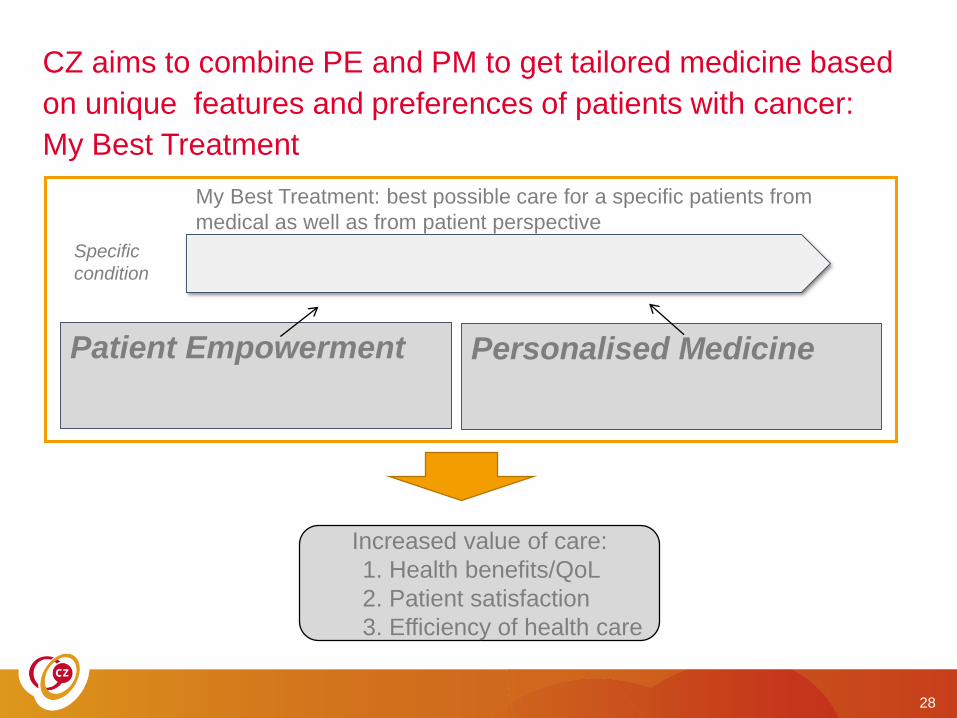
CZ aims to combine PE and PM to get tailored medicine based
on unique features and preferences of patients with cancer:
My Best Treatment
Patient Empowerment Personalised Medicine
Specific
condition
My Best Treatment: best possible care for a specific patients from
medical as well as from patient perspective
Increased value of care:
1. Health benefits/QoL
2. Patient satisfaction
3. Efficiency of health care
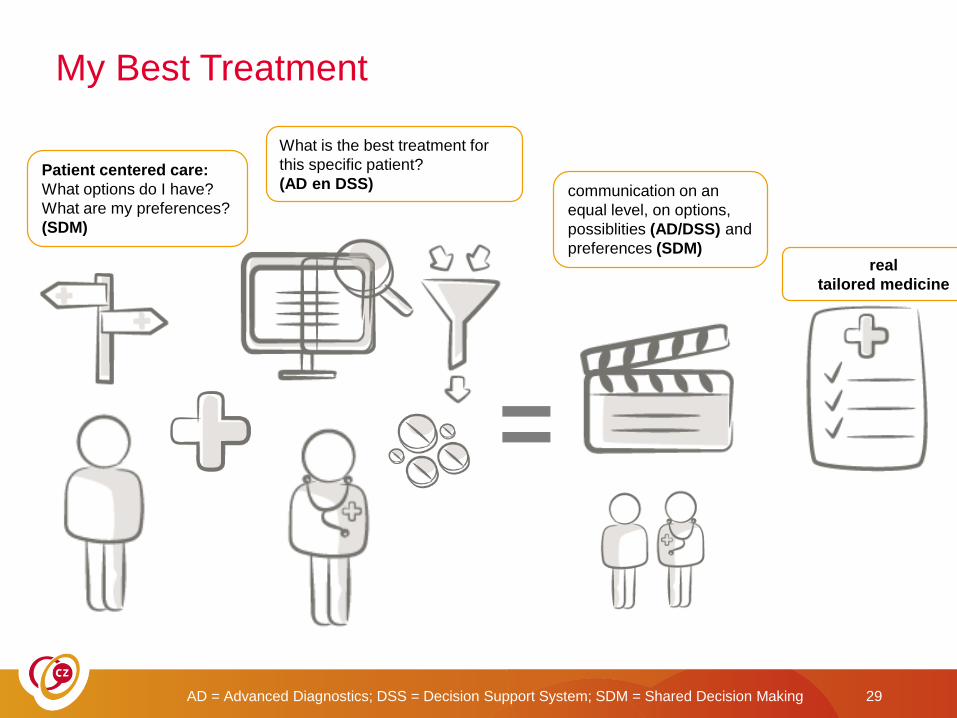
My Best Treatment
AD = Advanced Diagnostics; DSS = Decision Support System; SDM = Shared Decision Making 29
Patient centered care:
What options do I have?
What are my preferences?
(SDM)
What is the best treatment for
this specific patient?
(AD en DSS)
real
tailored medicine
communication on an
equal level, on options,
possiblities (AD/DSS) and
preferences (SDM)
=
30
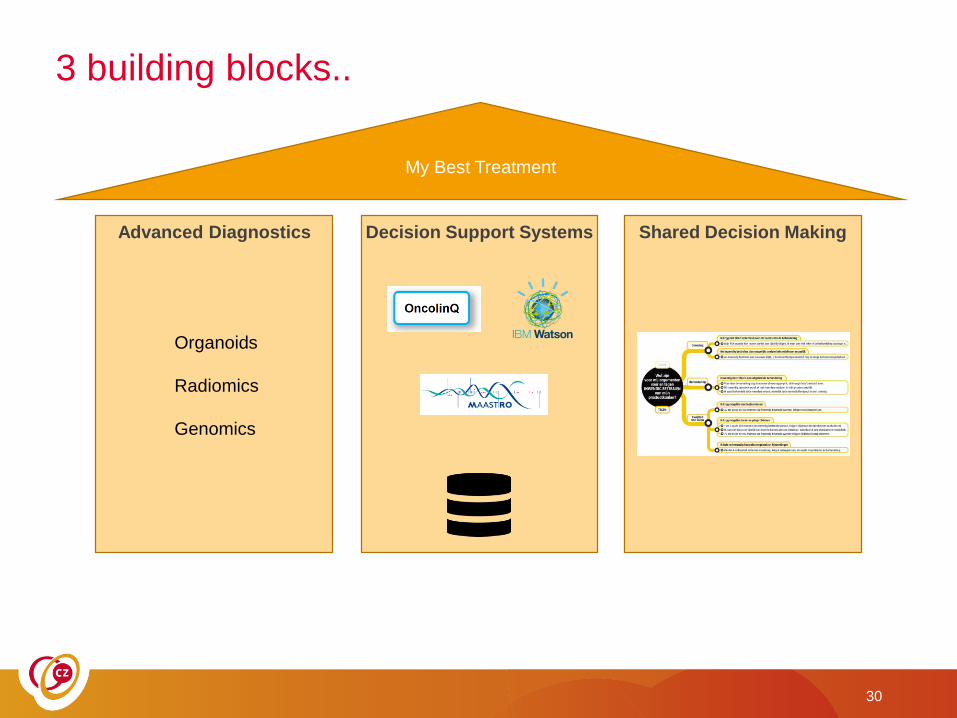
My Best Treatment
Advanced Diagnostics Decision Support Systems Shared Decision Making
Organoids
Radiomics
Genomics
3 building blocks..

31
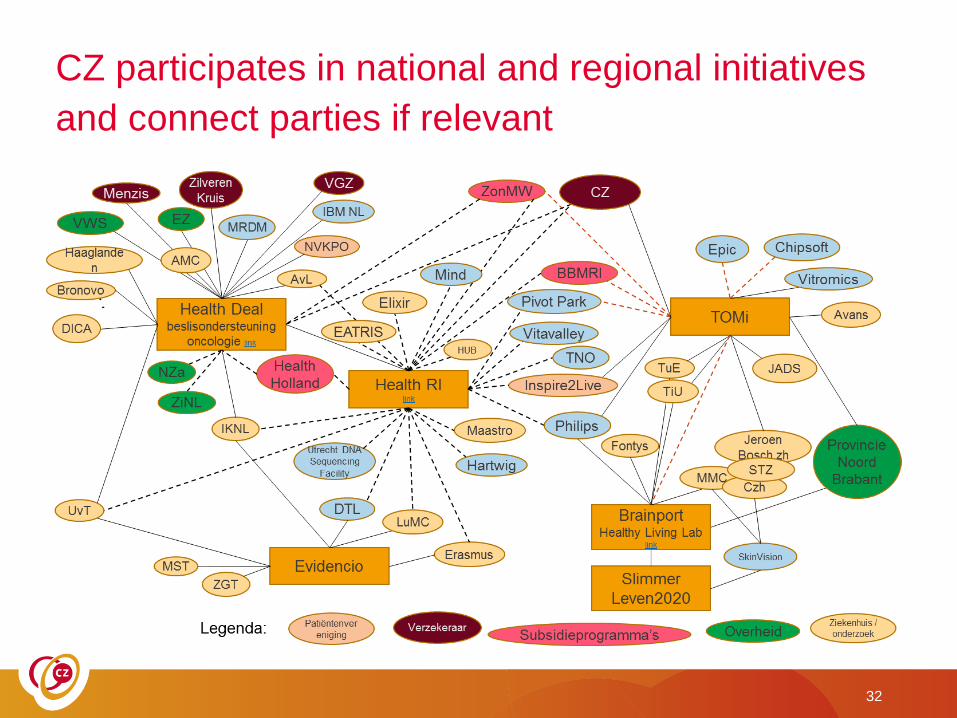
32
CZ participates in national and regional initiatives
and connect parties if relevant

CZ initiate's and support projects that contributes
to the implementation of My Best Treatment in
health care, e.g.:• 2014
• 2016
• 2017 - Exploration of ‘quick wins’: what is already available and how to adopt it quickly in health care?
- Several initiatives in preparation
33
Zorgpad moet patiënt helpen beslissen
5 juli 2016
Zorgverzekeraar CZ, Tilburg University, het Elisabeth-TweeSteden Ziekenhuis (ETZ),
MAASTRO clinic en VU Medisch Centrum werken samen om een verbeterd zorgpad
voor patiënten met longkanker te ontwikkelen. Het doel van dit zorgpad, My Best
Treatment, is om de behandeluitkomsten voor een patiënt te voorspellen en vervolgens
samen met hem de meest geschikte behandelmethode te bepalen.
Recommended