Brit. 7. Ophthat. (1976) 6o, 583
Optic nerve metastasis from a mediastinal carcinoid tumour
MARTIN L. FISHMAN AND SUSAN ROSENTHAL*From the Clinical Branch, National Eye Institute and the Medicine Branch*, National Cancer Institute,National Institutes of Health, Bethesda, Maryland, USA
Carcinoid tumours arise from the enterochromaffincells of tissues derived from primitive entoderm(Gosset and Masson, 1914). They have beendescribed in the gastrointestinal tract, pulmonarybronchus, biliary system, pancreas, ovary, testis,and parotid gland (Peskin and Kaplan, I969). Ocularmetastases from these tumours have occurred, butin every case have originated from bronchial car-cinoids (Southren, 1960; Ricketts, Price, andThomas, 1955; Rosenbluth, Laval, and Weil, I960;Font and Kaufer, i963; Honrubia, Davis, Moore,and Elliott, I972; Fu, McWilliams, Stratford, andKay, 1974; Bell, Bullock, and Albert, 1975).An unusual mediastinal tumour, with features
most consistent with a carcinoid neoplasm, hasrecently been described (Rosai and Higa, 1972).We present such a case in which clinical symptomsdeveloped from metastases to the optic nerve. Thisis the first case of ocular metastasis from mediastinalcarcinoid and the only case, of which we are aware,of carcinoid metastatic to the optic nerve.
Material and methodsCASE REPORT
A 25-year-old White man was found to have hilar andmediastinal adenopathy in October 1974, after a historyof recent weight loss, pleuritic chest pain, and pneu-monia. Bronchoscopy and endobronchial brush biopsywere normal. A scalene lymph node biopsy and bonemarrow examination showed metastatic tumour and thepatient was referred to the National Cancer Institutefor evaluation. No history of flushing, cyanosis, diarrhoea,abdominal cramping, or lacrimation was elicited.Physical examination revealed enlarged supraclavicularlymph nodes. Haematological and blood chemicalevaluations were within normal limits, and urinary5-hydroxy-3-indoleacetic acid levels were normal.Scalene lymph node and bone-marrow specimens werereviewed (see below) and a diagnosis of mediastinalcarcinoid tumour was made based on the pathologicaland clinical findings.
Treatment was begun with cyclophosphamide andvincristine and a partial response was noted. By February1975, however, symptoms recurred, hepatic metastases
Address for reprints: Clinical Branch, National Eye Institute,National Inistitutes of Health, Bethesda, Maryland 20014 USA,
were demonstrated, and pulmonary tomograms showedfurther mediastinal widening. An enlarged scalene lymphnode was biopsied for electron microscopical examination,and the patient was given palliative radiation therapy tothe mediastinum followed by adriamycin chemotherapy.By May 1975 osteoblastic metastases were noted in theskull, ribs, and vertebrae and inguinal lymphadenopathydeveloped.
In July 1975, the patient noted blurred vision in theright eye. An examination revealed normal pupillaryresponses, full ocular motility, and no evidence ofproptosis. The vision is reported to have been normalat this time, although an ophthalmologist was notconsulted. Re-examination three weeks later showed dischaemorrhages and exudates to be present in the righteye. The vision in the right eye decreased rapidly tohand movements, and the patient died of severe res-piratory difficulties four weeks after the onset of visualsymptoms. The left eye was normal throughout thepatient's illness.
Histopathological findingsLYMPH NODE BIOPSY
The lymph node was replaced almost totally bydense sheets of moderate size cells, arranged inparallel and anastomosing bands with occasionalperivascular palisading. Multiple mitoses werepresent. The cells had scanty cytoplasm, with largenuclei, finely distributed chromatin, and incon-spicuous nucleoli. Modest variation in the size andshape of individual cell nuclei was noted. Stains forneurosecretory granules were equivocal for argen-taffin granules (Fontana's stain) but positive forargyrophilic granules (Bodian's silver stain).
Electron microscopical examination of glutaralde-hyde fixed tissue revealed the presence of membraneenclosed circular and oval neurosecretory granuleswithin the cytoplasm of the tumour cells. Thesecontained a central core of homogeneous, electrondense material, surrounded by a small, electronlucent space (Fig. i). The cells tended to be ar-ranged around small central limina into which a fewmicrovilli projected. Many displayed prominentpseudopods and interdigitations. The cytoplasmcontained dilated endoplasmic reticulum, abundantmitochondria, prominent Golgi apparatus, lipiddroplets, and fibrils. Both dark and light cell types
on October 6, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.60.8.583 on 1 A
ugust 1976. Dow
nloaded from

584 British 7ournal of Ophthalmology
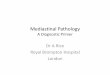
FIG. I Pseudopods of tumour cells containing mitochondrion and multiple circular secretory granules, characterized bya uniform electron dense central core with a small electron lucetnt space surrounded by a membrane (arrow). X 25 000
were noted (Bensch, Gordon, and Miller, I965)(Fig. 2).
GENERAL NECROPSY FINDINGS
Metastatic carcinoid tumour was present in thelungs, epicardium, mediastinum, axillary lymphnodes, liver adrenal glands, abdominal lymphnodes, colon, peripancreatic tissue, and vertebrae.No evidence of a bronchial or gastrointestinalprimary was found, and the site of the tumour wasbelieved to be the mediastinum.
OCULAR FINDINGS
The eyes were normal externally except for anenlarged right optic nerve (7 I mm diameter,compared with 4-6 mm in the left eye), with anormal optic nerve sheath and a patent subarachnoidspace. The anterior segment of the right eye wasnormal, but the right disc was raised with super-ficial haemorrhages on its surface and a pale
appearance of the disc tissue obscured the emergingretinal vessels. Scattered peripheral retinal haemor-rhages were also present. The left eye was normal.
Microscopically, the anterior segment of theright eye was normal. Papilloedema of the right discwas present with peripapillary exudates andhaemorrhages. Almost the entire retrolaminar opticnerve was replaced by fairly uniform, basophiliccells with scanty cytoplasm (Figs 3, 4). These weredensely packed, separated by multiple fine fibro-vascular trabeculae, with a tendency towardspalisading and rosette formation (Figs 5, 6).Several large areas of necrosis were present withinthe tumour. Stains for argyrophilic granules wereequivocal, while argentaffin stains were negative.Electron microscopical examination of the opticnerve revealed cells similar to those in the examinedlymph node.
DiscussionPrevious reports of ocular metastasel from carcinoid
on October 6, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.60.8.583 on 1 A
ugust 1976. Dow
nloaded from

Optic nerve metastasis 585
FIG. 2 Tumour cells with both 'light' (L) and 'dark' (D) cytoplasm, displaying multiple pseudopods (double arrowv).Cystoplasm contains neurosecretory granules (single arrow) and lipid droplets (broad arrow). x 4000
tumours have been limited to bronchial carcinoids,which have involved either the choroid (Southren,I960; Ricketts and others, I955; Rosenbluth andothers, 1960; Font and Kaufer, I963; Fu andothers, 1974; Bell and others, 1975) or orbit(Honrubia and others, 1972). Over 95 per cent ofcarcinoid tumours arise in the gastrointestinal tract,usually the small intestine or appendix, with theremaining 5 per cent taking their origin from othersites (Pesking and Kaplan, I969). While thegastrointestinal tumours characteristically have alow malignant potential with very slow growth andlate metastases, bronchial carcinoids have beenfound to metastasize in IO to I5 per cent of cases(Tolis, Fry, Head, and Shields, 1972) thus account-ing for their occasional association with ocularmetastases.
Rosai and Higa (I972) have recently presented acomprehensive description of primary carcinoidtumours of the mediastinum. In the cases sum-marized, all the patients were adults and most
(I4 to i6) were male. None of the patients de-veloped the carcinoid syndrome (Sjoerdsma andMelmon, I964). Many presented with minimalsymptoms, and tumour progression occurred slowly.A more aggressive form of this tumour, alsoarising in the mediastinum but associated withmultiple endocrine adenomatosis (Rosai, Higa, andDavie, 1972), was described in three additionalcases. Metastases occurred to bone, gastrointestinaltract, lung, lymph nodes, and adrenal glands andcaused death in each of the patients. Ocular meta-stases were not described. The present case thushas features characteristic of both types ofmediastinal carcinoid tumours.
Mediastinal carcinoids, as described by Rosai andothers (I972) and exemplified by the present case,have histological features similar to carcinoidtumours of other tissues. A useful subclassificationof these neoplasms by their embryonic site of origin(Williams and Sandler, I963) emphasizes the differ-ences of foregut, midgut, and hindgut carcinoids.
on October 6, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.60.8.583 on 1 A
ugust 1976. Dow
nloaded from

tic secretory granules of these foregut tumours aresmall, round, electron dense deposits, surroundedby a clear zone and a unit membrane (Hage, 1973;Black, i968). Carcinoid tumours of midgut andhindgut origin present somewhat different character-istics, as summarized in the Table. The histologicalpattern, argyrophilic staining, and ultrastructuralfindings of small, round uniform secretory granulesin the present and similar cases (Broderick, 1973;Manes and Taylor, I973) would support a foregutderivation.
p'' ,.
FIG. 3 The retrolaminar optic nerve is almost totallyreplaced by tumour cells. Papilloedema is present, andthere is an area of necrosis within tumour (arrow).Haematoxylin and eosin. x IO
Those of foregut origin (bronchus, pancreas,
stomach, and mediastinum) tend to have a trabecularpattern and reduce silver only in the presence of anexogenous reducing agent (positive argyrophilicstaining, negative argentaffin stain). The characteris-
FIG. 4 A cross-section of optic nerve shows normal nerve
tissue present only peripherally (arrovJ). Haematoxylinand eosin. x 14
Table Carcinoid tumour characteristics according to gut derivation
Foregut Midgut Hindgut
Tissue Lung, pancreas, stomach, Small intestine, ascending colon Descending colon, rectummediastinum
Histology Trabecular Classical 'nests' TrabecularArgyrophil Positive Positive NegativeArgentaffin Usually negative Positive Often negativeGranule ultrastructure Uniform, small, round Pleomorphic, large uniform or Rounded, variable density
dense central cores; rounded,variable size and density
Metastases Common Rare Common
Modified from Williams, 1963; Hage, 1973; Black, I968
586 British Journal of Ophthalmology
La:
on October 6, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.60.8.583 on 1 A
ugust 1976. Dow
nloaded from

Optic nerve mnetastasis 587
While the origin of mediastinal carcinoid ,tumours is not clear, it has been suggested that thethymus may give rise to this tumour. Cells similarto the Kultschitsky cell of the intestine have beenfound in the thymus of some animals (Reggiani,1946; Toro, Olah, Rohlich, and Viragh, 1969),argyrophilic cells have been found in humanthymus (Rosai and Higa, I972), and neurosecretorygranules have been reported in human thymus byelectron microscopical examination (Koss, 1970).
Treatment for carcinoid tumours has beenprimarily surgical with chemotherapy reserved forthose cases in which widespread metastases have gd,. Pbeen presented (Davis, Moertel, and McIlrath, -1973). Although radiotherapy has been used to treat
iX6l~~~~~A
Vt S 1 eastse frmteetmus,te r sal
8tt;t;j 5 4 4 kl % g ~~~~~radioresistant (Martin, 1970). Enucleation has thusrXJb* * ~~~~~~~~~~~been advocated for progressive intraocular
si<i tw"* * * * ~~~~~metastases (Bell and others, 1975).
sv+tXt 3 D 4 8 ~~Summary||#Sb5(t>#t4v !>JkJ*j r s A 25-year-old man with a rapidly progressivew=*;-k0^ 24|F*4eb 5 rgS ~metastatic carcinoid tumour arising in the medias-giWWi_%wv s * <: N*} * s tinum developed a metastasis to the optic nerve.>S--t1 -K> 4*t;w+ ; ^ ~~This is the first instance in the literature of ant*"Fqm e tj--" }* ~~~~ocular metastasis from this variant of carcinoid
§ tt ^t ....... Ji>k8t 00.* tumour. The ocular pathology, ultrastructure, andFIG. 5 The tumour cells are divided by fibrovascular recent information on the derivation of this tumour,strands. Haemotoxylin and eosin. x 350 believed to originate in the thymus, are presented.
References
BELL, R. W., BULLOCK, J. D., and ALBERT, D. M. (1975) Brit. 3Y. Ophthal., 49, I55BENSCH, K. G., GORDON, G. B., and MILLER, L. R. (I965) Cancer (Philad.), I8, 592B3LACK, W. C. (x968) Lab. Invest., I19, 473
on October 6, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.60.8.583 on 1 A
ugust 1976. Dow
nloaded from

588 British Journal of Ophthalmology
BRODERICK, P. A. (1973) 7. thorac. cardiovasc. Surg., 65, 134DAVIS, Z., MOERTEL, C. G., and MICILRATH, D. C. (1973) Surg. Gvnec. Obstet., 137, 637FONT, R. L., and KAUFER, G. (I963) Amer. _r. Ophthal., 62, 723FU, Y. S., MCWILLIAMS, N. B., STRATFORD, T. P., and KAY, S. (1974) Cancer (Philad.), 33, 707GOSSET, A., and MASSON, P. (1914) Presse mid., 22, 237HAGE, E. (973) Virchows. Arch. path. Anat., 36I, I2IHONRUBIA, F. M., DAVIS, W. H., MOORE, M. K., and ELLIOTT, K. J. (I972) Amer. J. Ophthal., 72, I I I8KOSS, L. G. (1970) 59th Annual Meeting of the International Academy of Pathology, St Louis, MO, Io MarchMANES, J. L., and TAYLOR, H. B. (1973) Arch. Path., 95, 252MARTIN, R. G. (1970) Cancer (Philad.), 26, 547PESKIN, G. W., and KAPLAN, E. L. (I969) Surg. Clin. N. Amer., 49, 137REGGIANI, M. (1946) Boll. Soc. ital. Biol. sper., 22, io8RICKETTS, M. M., PRICE, T., and THOMAS, M. (1955) Amer. J. Ophthal., 39, 33ROSAI, j., and HIGA, E. (1972) Cancer (Philad.), 29, Io6i
and DAVIE, J. (1972) Ibid., 29, 1075ROSENBLUTH, J., LAVAL, j., and WEIL, J. V. (I960) Arch. Ophthal., 63, 47SJOERDSMA, A., and MELMON, K. L. (I964) Gastroenterology, 47, 104SOUTHREN, A. L. (I960) 7. clin. Endocr., 20, 298TOLIS, G. A., FRY, W. A., HEAD, L., and SHIELDS, T. W. (I972) Surg. Gvnec. Obstet., 134, 6oITOR6, I., OLAH, I., ROHLICH, P., and VIRAGH, S. (I969) Anat. Rec., I65, 329
WILLIAMS, E. D., and SANDLER, M. (I963) Lancet, I, 238
on October 6, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.60.8.583 on 1 A
ugust 1976. Dow
nloaded from
Recommended