Overdose: A major preventable cause of
death in Eastern Europe and Central Asia
Shona Schonning

Founded in 1997, Secretariat in Vilnius, Lithuania
260 members: GOs, NGOs, drug user organizations
Exchange news, information, skills (over 700 people get email listserve)
Generate, identify new knowledge (research)
Build partnerships
Support advocacy initiatives
Provide technical assistance (through the Harm Reduction Knowledge Hub and through the Civil Society Action Team (CSAT)
Eurasian Harm Reduction Network (EHRN)

Eurasian Harm Reduction NetworkPROGRAM AREASNetworking and information workHarm Reduction Knowledge HubAdvocacy and policy workSpecial programs (including CSAT on GFATM and
civil society role)
PRIORITY TOPICS drug policy, overdose, opioid substitution therapy,
stigma and discrimination

In Western Europe:
OD is the number 1 of death of opiate injectors where data is collected systematically
OD is the number 2 cause of death of youth in Europe
So what’s up in Eastern Europe?
Overdose

Countries studied: Latvia, Kyrgystan, Romania, Russia and Tajikistan
Information gathered on:
Epidemiology
Services
Knowledge & skills,
Local & national policy
Overdose in Eastern Europe and Central Asia

Epidemiology
Data available was minimal, unreliable and likely to underestimate due to:
Poor data collection
Limited access to toxicological resources
Stigma
Concern about police involvement
Drug user surveys done in Russia and Latvia provided useful information

Barriers to good data
Not a priority
Not understood as preventable
No responsible agency
Requires medical examiner / forensic infrastructure
Requires identification of overdose as indicator or reportable cause of death
Requires consistent definition of overdose death
Social stigma (+/- registry)
Financial consideration of providers and families

Country Estimated number of IDU
Expected number of ODs
Expected number of OD deaths
Kyrgystan 25,000 5000 200
Latvia 10,000 2000 80
Romania 25,000 5000 200
Russia 355,568* 71,114 2844 (9354 recorded)
Tajikistan 33,000 6,600 264
Estimates
* Number of officially registered drug users
Based on:• 20% of IDU experience OD within a year• 4 out of 100 OD result in death

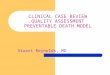
Cause of death among people living with AIDS in Russia where over 80% of PLHIV are IDU
N.N Ladnaya of the Federal AIDS Center of the Russian Federation made on November 1, 2007

OD death can be reduced!
Distributing nalaxone reduces overdose deathto drug users (through HR programs and
pharmacies)to emergency services (ambulances & hospitals)
Access to addiction treatment including OST programs have strong impact
Safer injection rooms
The good news about OD:

Cost-benefit~10-20% of naloxone prescriptions are used in
overdoseX
~4% of opiate overdoses result in death=
~0.4-0.8% of naloxone kits may result in a life saved that would otherwise be lost
at a price of $3 per 2 naloxone vials in each kit $375-750 per life saved (excluding
program costs)

Services
Hospital-based care was accessible but limited byDistanceAmbulance availabilityLimited nalaxone availabilityFear of police
Few (but very successful) pilot programs to distribute nalaxone to drug users & their communities
OST available only on pilot level and still prohibited in Russia and Tajikistan

NGO Volunter distributes nalaxone to
Hospitals
Emergency services
Drug users and their family & friends
Good practices in Khorog, Tadjikistan

Opiate ODs by EMS in Khorog Tajikistan
165
65
21
139 133
4
29 29
00
20
40
60
80
100
120
140
160
180
2006 2007
Heorin overdose
Reached by Naloxone
Fatality

Opiate ODs in ER, Khorog Tajikistan
38
23
6
54
51
1
9 9
0
0
10
20
30
40
50
60
2006 2007
Heroin Overdose
Reached by Naloxon
Fatality

OD prevention program of Russian Harm Reduction Network“There were three of us shooting up at a friend’s place. One guy
overdosed. I had nalaxon on me given to me by the project staff. After giving him an injection of nalaxon he got to his feet abruptly and didn’t even realize what had happened to him. Thanks to nalaxon his life was saved. Now I always have nalaxone with me and I am really gratful to the harm reduction program for educating me.” - Client in Biysk
“ Two weeks after we started the project people having heard about a miraculous medication and the vials went like hot cakes at the next outreach session.” – project staff in Samara
“It goes without say that we should continue this work” – outreach worker” – Naberezhni Chelni
outreach worker

Policy
Often not seen as a priority: rarely addressed in policy documents
Not clear which agency is responsible
In Tajikistan it is addressed in national policy documents
Latvia considering addressing OD in their HIV program
EU Action Plan on Drugs calls for OD programming
Contradictory laws about reporting to police
No laws to protect witnesses from police

POLICYPrioritize OD Identify responsible agencyUse EU policy to advocate for national response
SERVICESNalaxone access (peer-driven & EMS)Scale-up of access to addiction care including OST
RESEARCH
FUNDING (for advocacy & services)
Recommendations
Recommended