Patient prioritization in disease specifictreatment budgets
Lauren E. Cipriano
Jeremy D. Goldhaber-Fiebert

Funding, Disclosure, Acknowledgments
• Funding• Natural Sciences and Engineering Research Council of Canada
• No conflicts to disclose
• Thank you to Eldon Spackman for comments on an early draft

The usual story
• ICER =∆ Cost
∆QALY
• ICER > 𝜆 Not cost-effective
• ICER ≤ 𝜆 Is cost-effective…
…now how will we find the $ to buy it…
Tota
l Hea
lth
Sys
tem
Bu
dge
t
Cost-saving
0-10K/QALY
10-20K/QALY
20-30K/QALY
30-40K/QALY
40-50K/QALY
Budget

The usual story
• ICER =∆ Cost
∆QALY
• ICER > 𝜆 Not cost-effective
• ICER ≤ 𝜆 Is cost-effective…
…now how will we find the $ to buy it…
Tota
l Hea
lth
Sys
tem
Bu
dge
t
Budget

The usual story
• ICER =∆ Cost
∆QALY
• ICER > 𝜆 Not cost-effective
• ICER ≤ 𝜆 Is cost-effective…
…now how will we find the $ to buy it…
Tota
l Hea
lth
Sys
tem
Bu
dge
t
Budget

Tota
l Hea
lth
Sys
tem
Bu
dge
tThe usual story
• ICER =∆ Cost
∆QALY
• ICER > 𝜆 Not cost-effective
• ICER ≤ 𝜆 Is cost-effective…
…now how will we find the $ to buy it…
BudgetMay take years to divest
Budget impact may be
temporary

Restricted capacity disease specific treatment budgets
• AIDS Drug Assistance Programs (ADAPs)• Established in 1987 for low-income and under-insured
• Exclusively provides funding for HIV treatment
• Discretionary US federal and state funding
• Budget shortfalls• More restrictive eligibility (income, disease severity)
• Cost sharing
• Reduce number of medications available
• Waiting lists (2008-2013)• First-come first-served or Priority based on disease severity
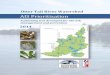
Treatment is cost effective for everyone: Who should go first?

F0 F1 F2 F3 F440-4445-4950-5455-5960-6465-6970-7475-79
Hepatitis C treatment is cost effective
$20,000 – $25,000 per QALY gained
$25,000 – 50,000 per QALY gained$50,000 –100,000 per QALY gained
<$20,000 per QALY gained
Treating 20% of the treatment eligible population = $20-25 billion annually (25% of Medicare Part D)

The research question
• Treatment is ‘cost-effective’ for everyone but budget impact is overwhelming
• At least for a transitional phase, policy is to restrict access to manage budget impact… but, who should be prioritized for treatment?
•Should patient subgroups be prioritized on ICERs?

Stage 1 Stage 2
𝒑𝟏 𝒑𝟐
𝑩𝟏 𝑩𝟐 > 𝟎≫
𝒓𝟏 𝒓𝟐≥
Incr. net monetary benefit(Treat now vs. never)
Period reward, if wait
𝑵Number of people 𝑵
Dead(not trt elig.)
Two time periods (now and later) with N treatments available at each period,who should get treatment first?
TheModel

Time 1 Time 2
Lower ICER goes first 𝐵1 + 𝑟2 1 − 𝑝2 𝐵2𝛿 1 − 𝑝2 𝐵2
Higher ICER goes first 𝐵2 + 𝑟1 1 − 𝑝1 𝐵1 + 𝑝1𝐵2𝛿 1 − 𝑝1 𝐵1 + 𝑝1𝐵2
Total Treatments
2𝑁 − 𝑝2𝑁
2𝑁
Lower ICER goes first
Higher ICER goes first
> ?
𝐵1 + 𝑟2 + 𝛿 1 − 𝑝2 𝐵2 > 𝐵2 + 𝑟1 + 𝛿 1 − 𝑝1 𝐵1 + 𝑝1𝐵2

Lower ICER goes first
Higher ICER goes first
>
(𝐵1−𝐵2)(1 − 𝛿) − (𝑟1 − 𝑟2) + 𝛿 𝑝1 𝐵1 − 𝐵2 − 𝑝2𝐵2 >0
+ve, small𝛿 ≈ 1
Benefit lost when Stage 1 Stage 2 (because of delay)
-ve, smallBenefit lost when Stage 2 Dead(because of delay)

𝐵1 − 𝐵2𝐵2
>𝑝2𝑝1
Ratio of the progression probabilities
Relative gain in INMB
from treating at Stage 1
Priority to lower ICER• Large difference in ICERs
• Low rate of out of Stage 2• People are unlikely to become
treatment ineligible
• High rate of out of Stage 1• Fleeting opportunity for early
high-impact intervention
>

𝐵1 − 𝐵2𝐵2
<𝑝2𝑝1
Priority to higher ICER!• Small difference in ICERs
• High rate of out of Stage 2• People are going to become
ineligible for cost-effective treatment!
• Low rate of out of Stage 1• Slowly progressing disease
• People can wait for treatment with little health consequence
Ratio of the progression probabilities
Relative gain in INMB
from treating at Stage 1
<

What if you had (much) less than N treatments available each period?
• Prioritize lower ICER when
(𝐵1−𝐵2)(1 − 𝛿) − (𝑟1 − 𝑟2) + 𝛿 𝑝1 𝐵1 − 𝐵2 − 𝑝2𝐵2 >0
If the de-prioritized group will have long treatment delay,Large difference in ICER Prioritize lower ICER

Does it make a difference in real life?Priority on ICER
Optimize on NMB
F0 F1 F2 F3 F4
40-44 6 5 3 0 0
45-49 6 4 2 0 0
50-54 6 5 3 0 0
55-59 7 6 3 0 0
60-64 7 5 4 1 0
65-69 7 6 4 1 2
70-74 7 6 7 5 8
75-79 7 7 7 6 8
F0 F1 F2 F3 F4
40-44 5 0 0 0 0
45-49 5 0 0 0 0
50-54 5 0 0 0 1
55-59 7 0 1 1 3
60-64 8 2 3 2 4
65-69 9 5 5 5 7
70-74 9 7 7 6 8
75-79 9 8 8 8 8
ICER Opt.
Within 5 years
Within 10 years
ESLD and cancer
ICER Opt.
QALYs

Another way to think about it
• The mutually exclusive collectively exhaustive set of decision alternatives is a complete set of times until each subgroup will be prioritized
F0 F1 F2 F3 F440-44 6 5 3 0 0
45-49 6 4 2 0 0
50-54 6 5 3 0 0
55-59 7 6 3 0 0
60-64 7 5 4 1 0
65-69 7 6 4 1 2
70-74 7 6 7 5 8
75-79 7 7 7 6 8

All immediately
Severityonly
F0 F1 F2 F3 F4
40-44 5 3 3 1 0
45-49 5 3 3 1 0
50-54 5 3 3 1 0
55-59 5 3 3 1 0
60-64 5 3 3 1 0
65-69 5 3 3 1 0
70-74 5 3 3 1 0
75-79 5 3 3 1 0

Severityonly
All immediately

Severityonly
All immediately
Priority on ICER
Maximizes NMB s.t. Annual Treatment Budget
ICER
Optimize on NMB
F0 F1 F2 F3 F4
40-44 3 3 0 0 0
45-49 3 0 0 0 0
50-54 4 0 0 0 0
55-59 4 0 0 0 0
60-64 4 2 0 0 0
65-69 4 3 2 1 1
70-74 4 3 2 3 2
75-79 4 3 3 3 3
F0 F1 F2 F3 F4
40-44 0 0 0 0 0
45-49 1 0 0 0 0
50-54 2 0 0 0 0
55-59 2 0 0 0 0
60-64 4 0 0 0 1
65-69 5 2 2 2 3
70-74 5 3 3 3 4
75-79 5 4 4 4 4

Conclusion
• Health care budgets should not always be allocated in order of ICER
• How long will the wait be? Consequences of waiting?
• Maximizing NMB for all individuals s.t. the annual budget constraint incorporates • relative benefit of treatment
• consequences of waiting
• time until resources available to expand treatment access
Recommended